
Abstract
Research suggests that patient-centered culturally sensitive health care may be an important precursor to patient satisfaction and treatment adherence. Data from this study are a subset from the data collected for the Patient-Centered Culturally Sensitive Health Care and Health Promotion Research Project. The present study was designed to (a) explore the relationship between patients’ perceived patient-centered cultural sensitivity of their health care sites (ie, the physical and social environment and clinic policies) and their self-reported adherence to treatment and (b) investigate whether this relationship is mediated by satisfaction with health care experienced. Participants consisted of a low-income, culturally diverse sample of 1581 patients from 67 health care sites across the United States. A significant positive relationship between patients’ perceived patient-centered cultural sensitivity of their health care sites and their self-reported treatment adherence to a prescribed regimen was observed. Patient satisfaction with care partially mediated the relationship between these 2 variables. Assessing the level of patient-centered cultural sensitivity patients perceive in their health care sites might provide guidance to health care administrators as to how to make their sites more culturally sensitive from the perspective of patients. This, in turn, might increase patients’ treatment adherence, leading to improved health outcomes.
Keywords
Patient-centered culturally sensitive health care (PC-CSHC) has been identified as a best-practice approach for improving treatment adherence and, consequently, health outcomes.
Poor treatment adherence (ie, the willingness and ability of patients to actively follow the recommendations of their health care providers) is a significant concern in the United States.1,2 Research has consistently demonstrated that inadequate treatment adherence leads to higher rates of morbidity and mortality and also to increased health care costs.3 -5
Patient-centered culturally sensitive health care (PC-CSHC) has been identified as a best-practice approach for improving treatment adherence and, consequently, health outcomes.1,6,7 Tucker and colleagues 8 used the term patient-centered culturally sensitive health care to describe health care systems that display patient-desired, modifiable provider and staff behaviors and attitudes, and health care site environment characteristics and policies that culturally diverse patients identified as indicators of respect for their culture and that enable these patients to feel comfortable with, trusting of, respected during, and trusting of the health care they receive. Research has consistently shown that the higher the patient perceived patient-centered cultural sensitivity of health care providers, the higher the treatment adherence of patients.9,10
Health care literature on cultural sensitivity has mostly centered on the impact of provider behaviors and attitudes on patient satisfaction and treatment adherence.6,11,12 Yet, other studies have reported positive associations between cultural sensitivity of the health care physical environment and policies and positive patient outcomes such as satisfaction with care and treatment adherence.13,14 The implementation of culturally sensitive practices at an organizational level can aid with the deinstitutionalization of racism in health care practices. 15 Furthermore, a review of the relevant literature reveals that increased cultural sensitivity at the organizational (systemic) level (eg, extended clinic hours, flexibility with appointment times, short waiting times) positively affects patient–provider communication, patient satisfaction, and patient treatment adherence.16 -19 Additionally, plenty of anecdotal evidence indicates that barriers to cultural competence and sensitivity at the organizational/systemic level (eg, limited site hours or prolonged waiting-times) create a disconnection between health care organizations and the diverse patient populations they serve. 20
No known research has explored the associations between levels of patient-identified indicators of cultural sensitivity in health care site environments and policies (ie, patient-centered cultural sensitivity indicators) and positive patient outcomes (eg, patient satisfaction and treatment adherence). Patients are the most ideal experts regarding what they perceive as culturally sensitive. The high rates of treatment nonadherence speak to the need to develop interventions that empower patients to actively participate in their health care by providing feedback to their health care sites on what makes them feel comfortable, trusting, and respected. Incorporating these indicators in patients’ health care may lead to higher patient satisfaction and higher engagement in health-promoting behaviors.
Present Study Hypothesis and Research Question
The present study examines the associations among patients’ perceived patient-centered cultural sensitivity of their health care sites, patient satisfaction with care, and treatment adherence in a nationwide sample of culturally diverse patients in the United States (ie, patients who are from racially/ethnically and economically diverse backgrounds). Based on the relevant literature, the specific hypothesis is that there will be a significant positive relationship between patients’ perceived patient-centered cultural sensitivity of their health care sites and patients’ self-reported level of treatment adherence. A significant relationship between these variables could provide additional support for assessing the levels of patient-centered cultural sensitivity patients perceive in their health care sites and, if necessary, adjusting these levels to meet the needs of culturally diverse patients. Additionally, the research question set forth in this study is: Does patient satisfaction with care mediate the relationship between patients’ perceived patient-centered cultural sensitivity of their health care sites and patients’ self-reported level of treatment adherence?
Method
Participants
The participant data for the present study are a subset of data collected as part of the first phase (Phase I) of a larger national Patient-Centered Culturally Sensitive Health Care and Health Promotion Research Project (C.M. Tucker, Principal Investigator). Specifically, the main objectives of this first phase of the larger national study were to (a) establish the reliability and validity of the pilot versions of the Tucker-Culturally Sensitive Health Care Inventory (T-CSHCI), including the T-CSHCCEI-PF (used in this study), and (b) identify provider and office staff as well as clinic environment characteristics that are most important to culturally diverse adult patients. For Phase I of this national study, adult patient participants (N = 1725) were recruited from 67 health care sites across the United States that volunteered to participate in response to a written invitation. To be enrolled in the project, participants had to (a) be at least 18 years old, (b) have been patients at one of the health care sites for at least 1 year, (c) be able to communicate either verbally or in writing in Spanish or English, and (d) sign an informed consent form that documented agreement to participate in the study.
Of the 67 participating health care sites recruited, 71.4% were community health care centers/clinics, 5.4% were hospitals, 7.1% were health departments, 12.5% were private practices, and 3.6% were other types of sites (eg, half way houses for rehabilitation). With regard to location, 50.0% of the sites were situated in the west, 30.0% in the south, 10% in the midwest, and 5.0% in the northeast. A small percentage (5.0%) was in unreported geographic locations.
For the mediation analyses in this study, listwise deletion subsample was used. This subsample included any adults participating in the larger national study who had no missing data on any of the investigated variables in this study. Of the adults included in this subsample (N = 1581), 32.4% were male and 65.3% were female. This gender composition is a good reflection of prior research studies with patients who use health care sites. Specifically, in such studies, women as compared to men are more likely to regularly visit a health care provider, use medical services, and have a usual source of health care.21 -24
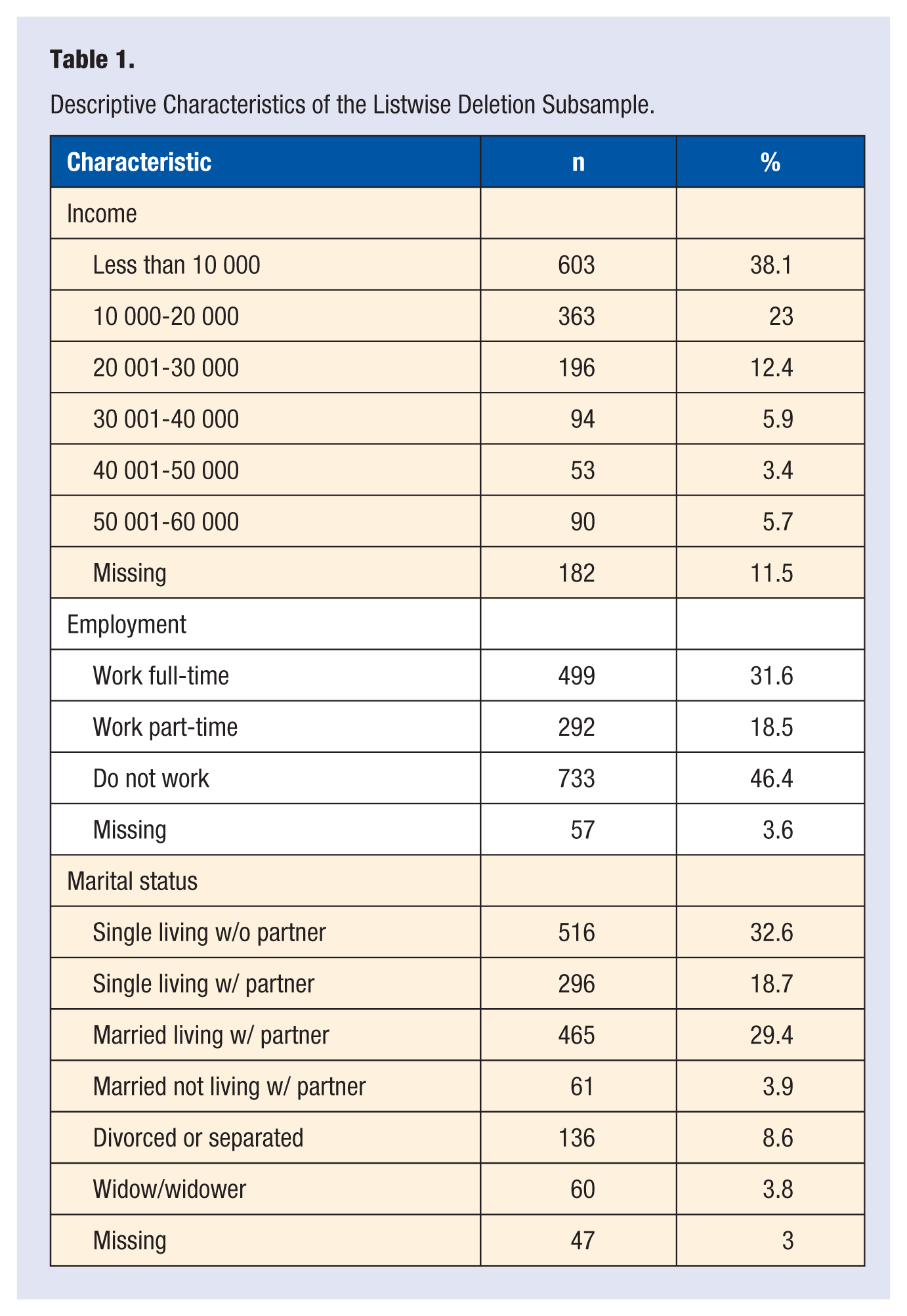
In the listwise subsample, the percentage of participants per age group investigated is as follows: 18-24 (17.0%), 25-34 (20.4%), 35-44 (21.2%), 45-54 (22.9%), 55-64 (12.6%), and 65+ years (4.7%). A few (1.3%) participants did not report their age. Race/ethnicity composition of the subsample was as follows: 20.0% African American/Black, 32.5% White/European American, 3.8% American Indian/Native American, 3.2% Asian/Asian American/Pacific Islander, 31.0% Hispanic/Hispanic American/Latino, and 3.4% Other. Race/ethnicity was not reported by 6.1% of the participants. Additional demographic information for the subsample is provided in Table 1.
Descriptive Characteristics of the Listwise Deletion Subsample.
Instruments
In the larger national study, patient participants anonymously completed a research participation packet that included (a) 2 copies of the Informed Consent Form—one for the participant to keep and one for the researchers to keep and (b) an assessment battery consisting of 12 brief questionnaires. Four of these questionnaires will be used to examine the variables of interest in the present study: (a) the Patient Demographic Data Questionnaire, (b) the Tucker Culturally Sensitive Health Care Clinic Environment Inventory–Patient Form (T-CSHCCEI-PF), (c) the Patient Satisfaction Questionnaire–Short Form (PSQ-18), and (d) the General Adherence Measure (GAM). Each of these measures is described in the following sections.
Participants had a choice of completing the assessment packet in Spanish or English since all patient measures had been translated into Spanish, independently back-translated into English by experienced translators, and then verified by certified translators to confirm translation reliability. The assessment battery was at an eighth-grade reading level.
Patient Data Demographic Questionnaire
This instrument was constructed by the principal investigator for the national study and her research team to collect participants’ demographic information. The questionnaire includes questions regarding participants’ gender, age, marital status, race/ethnicity, level of education, employment status, generation status, and household income.
Tucker Culturally Sensitive Health Care Clinic Environment Inventory–Patient Form
This 25-item self-report measure was designed by the principal investigator of the larger national study to assess patients’ perceived levels of patient-centered cultural sensitivity in the physical environment and policies of their health care centers. The instructions on the T-CSHCCEI-PF 25 are used with the provided 4-point Likert-type scale (on which 1 = Strongly disagree and 4 = Strongly agree) to rate one’s level of agreement that a series of health care site characteristics and policies exist at their health care site (ie, health care center or office). Sample items from this inventory include the following: “My health care center or office has affordable services” and “My health care center or office has brochures available in English and Spanish.” Research shows the T-CSHCCEI-PF is a reliable and valid inventory for culturally diverse patients to provide feedback to the administrators at their health care centers regarding the degree to which these centers have characteristics that are reflective of patient-centered culturally sensitive health care. 26
Patient Satisfaction Questionnaire–Short Form
This 18-item scale 27 was developed to measure 7 different dimensions of patient satisfaction with medical care. There is no total score. For the present study, only the 2-item general satisfaction subscale of the PSQ-18 was used because it most clearly measures overall patient satisfaction with their health care sites. The 2 items in this subscale are “The medical care I have been receiving is just about perfect” and “I am dissatisfied with some things about the medical care I receive” (the latter item is reverse-scored). Respondents rate the items on a 5-point Likert-type scale (1 = Strongly disagree to 5 = Strongly agree). Higher scores indicate higher patient satisfaction with the health care experienced. The general satisfaction subscale has been found to have acceptable internal consistency reliability (Cronbach’s α = .75). 27 Marshall and Hays, 27 coauthors of the PSQ-18-SF, conclude this questionnaire is appropriate for use in situations when, due to time constraints, use of its more extensive 50-item counterpart (PSQ-III) would not be feasible.
General Adherence Measure
This 5-item measure of treatment adherence assesses patients’ tendency to follow medical recommendations from their health care providers in the past 12 months. 28 Items are rated on a 4-point Likert-type scale (on which 1 = None of the time and 4 = All of the time). Sample items include the following: “I had a hard time doing what my provider suggested I do” or “I followed my provider’s suggestions exactly.” Two of the items on the scale (1 and 3) are reversed scored. A general adherence score can be computed by averaging the ratings on all (5) items on the GAM. Higher scores indicate higher adherence to treatment. Internal consistency reliability for this scale is acceptable (Cronbach’s α = .81), with a 2-year stability of .41. 28
Procedure
Data for the present study are a subset from the data collected during Phase I of the larger national study (ie, Patient-Centered Culturally Sensitive Health Care and Health Promotion Research Project). Permission to conduct the national study, from which the data for the present study were derived, was received from the institutional review board at the University of Florida. Data for the larger national study (and thus the present study) were conducted using a 3-step procedure.
Step 1: Recruitment of National Health Care Sites
Health care sites to be research sites were identified using 2 strategies: (a) a National Health Care Site List method and (b) a Co-Investigators and Collaborators Method. The National Health Care List Method of identifying and recruiting research site study participants involved having the research team at University of Florida complete Web searches to identify potential participating sites and compiling a database from the results of the Web searches. The second method involved having the co-investigators for the national study telephone representatives/colleagues from various organizations that provide health care services to specific populations (eg, the Commission on Minority Health) for the purpose of asking them to be research collaborators. Specifically, the representatives/colleagues invited to be research collaborators were asked to help with recruitment efforts by identifying potential participating sites throughout the United States.
The potential study sites identified through the methods listed above were located in the Midwest, Northeast, South, and West regions of the United States, in particular regions that were mostly populated by racial/ethnic minorities and low-income individuals. Sites were sent an invitation letter that (a) explained the purpose and objectives of the study; (b) described potential benefits of participating in the study; (c) invited providers, staff, and patients at these sites to participate in the study; (d) described potential benefits of participating in the study; and (e) provided the research team’s contact information to express interest in participation in the study or ask for more information about the study. Additionally, members of the research team contacted the sites that expressed interested in participating to provide more details about the study and answer any pertinent questions. The research team and on-site administrators at the different sites worked collaboratively to obtain approval for each specific site to participate in the study.
Step 2: Recruitment of On-Site Data Collection Coordinators and Data Collectors
In Step 2, on-site administrators at each site identified a staff person to be a Data Collection Coordinator (DCC), whose primary role was to coordinate and assist with data collection. The research team mailed the DCCs at each site a box with the following recruitment and participation materials: (a) information packets for the DDD and Data Collectors, which included scripts for recruiting participants; (b) a Health Care Site Demographic and Health Data Questionnaire, used to collect overall demographic information on the patients and staff at each site; (c) flyers for recruiting participants; (d) Patient Recruitment Logs, to keep track of the recruited patient participants; and (e) research participation packets for each participant, which included 2 informed consent forms (ICFs), assessment batteries (one in Spanish and one in English), 2 envelopes to separately return the ICF and completed questionnaires, and a cover letter describing the study and providing instructions on how to complete the questionnaires. DCCs also received 2 boxes with prepaid FedEx return labels for storing and then mailing back the participation materials to the designated member of the research team that conducted the national study. DCCs had an opportunity to review all the study recruitment and participation materials and then meet with the research team to go over them.
The DCCs were asked to recruit 2 individuals at each site (eg, community members, office staff members, and/or graduate or undergraduate students) to be Data Collectors (DCs), whose primary responsibility in the study was to recruit participants and collect their data. The DCCs and research team members discussed with DCs study materials and DCs’ roles and responsibilities in the study. Afterwards, DCs took a verbal knowledge test, with the DCCs, to make sure that they understood and remembered study data collection procedures. DCCs reviewed test results with DCs. DCs who did not get 9/10 questions correct had an opportunity to retake the test.
Both DCCs and DCs were trained in study procedures in accordance with the national study’s research protocol (including patient confidentiality), which had been approved by University of Florida’s institutional review board. The research team continued to provide weekly structured support to both DCs and DCCs at the clinics; sites also had a phone number they could contact in case they had questions.
Step 3: Recruitment of Patient Participants
Data Collectors recruited patient participants by handing them the patient recruitment flyers or by posting these flyers in waiting rooms at the health care sites. DCs also used the snowballing technique of asking participants to recruit additional patients for the study. Patients who expressed interest in participating and met the inclusion criteria were each given a research participation packet by the DC. As instructed in the cover letter within each participation packet and as instructed by the DC, each participant (a) read and signed the informed consent form, (b) answered questionnaires in the assessment battery without placing their names on these questionnaires, (c) signed a Payment Release Form that included the name and address where they wished to have their compensation for study participation mailed, and (d) returned to the DC all questionnaires in one envelope and all materials that contained their personal information in the other envelope (to protect participant confidentiality).
The DCs returned all envelopes (ie, 2 envelopes per participant) to the DCC at their clinic; the DCCs, in turn, placed these envelopes in the data storage/mailing boxes. When filled, these boxes were mailed back to a designated member of the research team conducting the national study. All data were processed in accordance with the ethical standards of the aforementioned institutional review board.
All participants were mailed a money order for $15 for their participation in the national study. For their study participation, each DCC was mailed a $50 money order, and each DC was mailed a money order of an amount based on an $8 rate per hour for a maximum of 4 hours per 4 weeks (the estimated duration of the study at each site). Consequently, each DCC received a maximum of $128 for study participation. The total study implementation period was 8 months long. All participants were compensated within 6 weeks following the end of the study at their specific health care sites.
Results
To determine if the national study data sample (N = 1725) and partial data subsample used in this study (N = 1581) significantly differed with regard to gender, age, race/ethnicity, and/or education level, χ2 analyses were conducted., Results of these analyses revealed a significant difference in age between the 2 samples, χ2(5) = 14.68, P < .05, with a slightly higher representation of 55+ year olds in the incomplete data set. There was also a significant difference in level of education between the 2 samples, χ2(5) = 13.53, P < .05, with a slightly higher representation of college-educated participants in the complete data sample. There were no significant differences between the 2 subsamples with regard to gender or race/ethnicity (P < .05).
Descriptive Data for the Major Variables
The mediation analyses employed in this study is parametric in nature and thus requires data to be normally distributed. Therefore, the variables of interest were examined to assess basic distributional properties and to determine if normality assumptions were met. This initial examination indicated that skewness and kurtosis were significant for all variables (ie, patients’ perceived patient-centered cultural sensitivity of their health care sites [CSHCCI], general patient satisfaction with health care [Satisfaction], and self-reported adherence to a prescribed treatment regimen [Adherence]). Given the large sample size, there was substantial power to detect even small deviations from normality. However, to facilitate analyses with the assumption of multivariate normality (mediation), a Blom transformation was used to normalize the distribution of all variables 29 ; this reduced skewness and kurtosis of the investigated variables to an acceptable level.
Hypothesis Testing
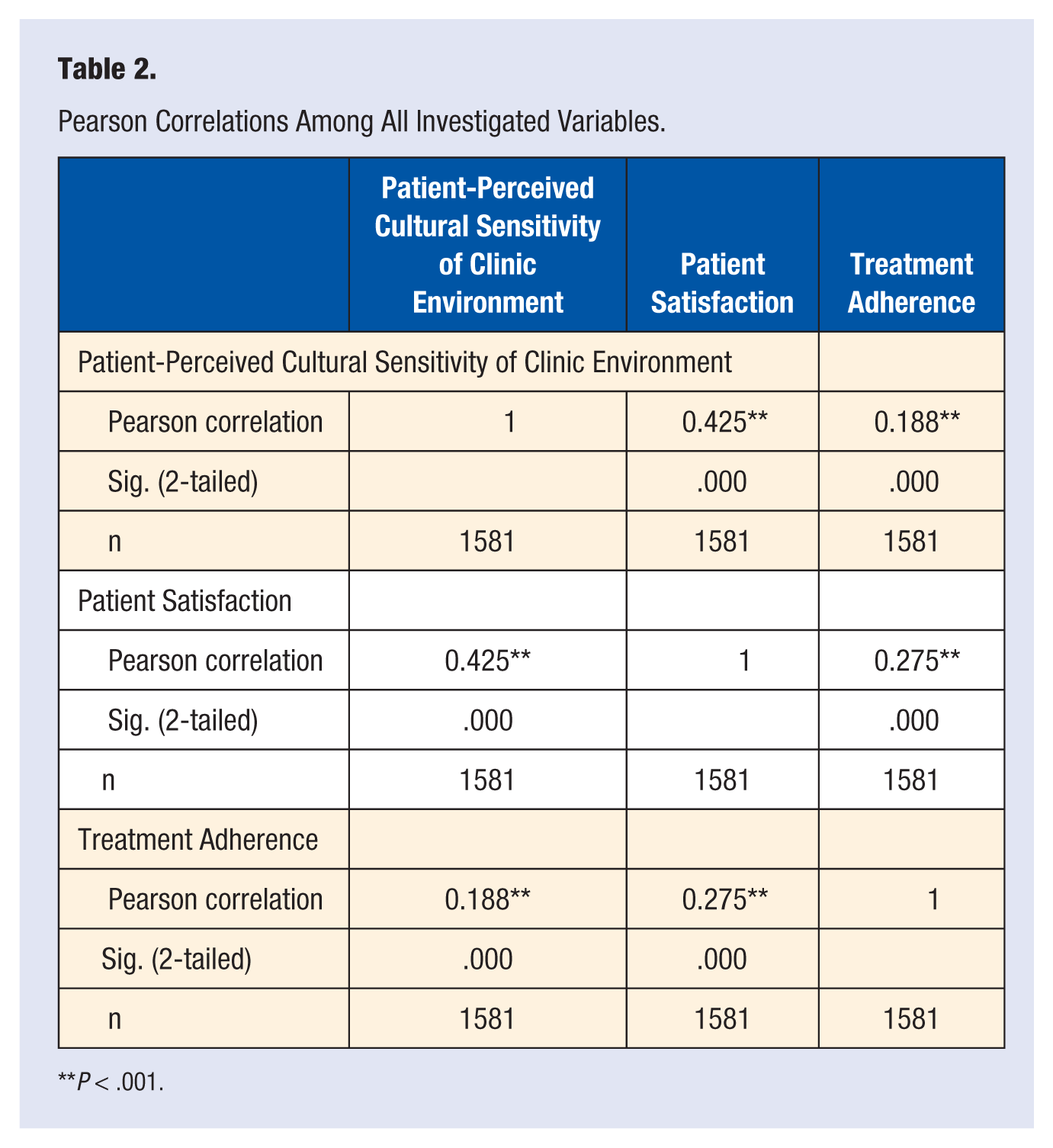
A Pearson correlation analysis was conducted to assess whether there was significant positive relationship between patients’ perceived patient-centered cultural sensitivity of their health care sites (CSHCCI) and their self-reported treatment adherence (Adherence), as hypothesized. Results showed a low but significant positive correlation between CSHCCI and Adherence, r = .19, P < .001. These findings provide support for the main hypothesis of this study.
Research Question
A variable may be considered a mediator to the extent to which it carries the influence of a given independent variable (IV) to a given dependent variable (DV). Generally speaking, mediation can be said to occur when (a) the IV is significantly associated with the outcome variable (DV) in the absence of the mediator, (b) the IV significantly affects the mediator, (c) the mediator has a unique effect on the outcome variable, and (d) the effect of the IV on the DV shrinks on the addition of the mediator to the model.30,31
In addition to the analysis conducted to test the correlation between CSHCCI and Adherence, Pearson correlation analyses were conducted to test the association between CSHCCI and general patient satisfaction (Satisfaction), and the association between Satisfaction and Adherence. Results indicate that patients who report higher CSHCCI also report higher levels of Satisfaction (r = .43, P < .001). Furthermore, patients who report higher levels of Satisfaction also report higher levels of Adherence (r = .28, P < .001; see Table 2).
Pearson Correlations Among All Investigated Variables.
P < .001.
Based on the results from the aforementioned correlation analyses, a mediation analysis was conducted using Preacher and Hayes’s SPSS Indirect macro. 32 This macro estimates the path coefficients in a multiple mediator model and generates bootstrap confidence intervals (percentile, bias-corrected, and bias-corrected and accelerated) for total and specific indirect effects of X (in this study, CSHCCI) on Y (in this study, Adherence) through a proposed mediator (in this study, Satisfaction). 32 This macro is far superior to SOBEL, as it allows for more than one mediator and adjusts all paths for the potential influence of covariates not proposed to be mediators in the model. CSHCCI predicts Adherence, t = 7.46, P < .001, and also Satisfaction, t = 17.61, P < .001. The mediator (Satisfaction) has a unique effect on Adherence, t = 8.99, P < .001. Finally, the effect of CSHCCI on Adherence shrinks when the mediator (Satisfaction) is introduced, t = 3.35, P < .001, but it remains significant, which indicates partial mediation. This model explains 81% of the variance in Adherence, P < .001 (see Figure 1).
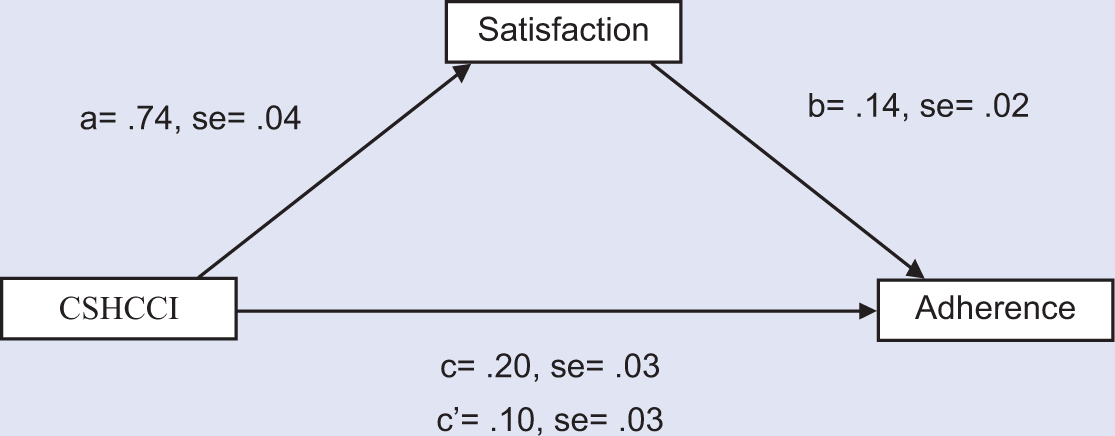
Schematic of the Mediation Model Tested in This Study.
Discussion
This study was conducted in response to international calls for further understanding of the factors that influence patient treatment adherence. The relationships among patients’ perceived patient-centered cultural sensitivity of their health care centers (ie, the physical and social environment and clinic policies), satisfaction with their care, and self-reported levels of treatment adherence were explored. This study is unique in that the measure employed to assess patient-centered cultural sensitivity of health care environments (T-CSHCCEI-PF) consists of items that a national sample of culturally diverse patients identified as indicators of patient-centered cultural sensitivity; in other words, the items in the measure consist of health care center physical environment characteristics and policies that enable culturally diverse patients to feel comfortable with, respected during, and trusting of the health care they experience. 8
Prior to the present study, there was little empirical evidence linking patient-perceived indicators of organizational/systemic cultural sensitivity with satisfaction with care and treatment adherence. Consistent with the hypothesis set forth in this study, results from this study indicate that patients’ perceived patient-centered cultural sensitivity of their health care sites is significantly related to patients’ self-reported level of treatment adherence. These findings are also consistent with previous research indicating that overall provision of culturally sensitive health care directly affects understanding of treatment and treatment adherence.15,33,34
Results from investigating the research question set forth in this study indicate that the relationship between patients’ perceived patient-centered cultural sensitivity of their health care sites and self-reported treatment adherence is partially mediated by patient satisfaction with health care. Specifically, it was found that the more patient-centered cultural sensitivity patients perceived in their health care sites, the more satisfied they were with the health care they received; and the more satisfied they were with the health care received, the more they adhered to their treatment regimens. Although the relationships between organizational cultural sensitivity and patient satisfaction and between patient satisfaction and treatment adherence had been investigated before, the introduction of satisfaction with care as a mediator between organizational cultural sensitivity and treatment adherence is novel to the health care literature.
Implications
While treatment adherence is a behavioral problem observed at the patient level, the contributors to treatment adherence/nonadherence far exceed patient characteristics. The evidence in this study indicating that patient-perceived cultural sensitivity of health care centers is directly associated with treatment adherence has several implications.
The first implication is that interventions that promote patient-centered culturally sensitive physical environment characteristics and policies in health care sites might be key to increasing treatment adherence of patients at these health care sites, which in turn might promote positive health outcomes among these patients. According to the World Health Organization, 35 “Increasing the effectiveness of adherence interventions may have a far greater impact on the health of the population than any improvement in specific medical treatments.” Access to medication is clearly not the only precursor to successful disease management.
Another implication of the present study is that assessing the level of patient-centered cultural sensitivity patients perceive in their health care sites might provide guidance to health care administrators as to how to make their sites more culturally sensitive from the perspective of patients. The success of patient-centered health care interventions is organized around empowering patients to be active participants and decision-makers in their health care. 36 Regular assessment of sites’ patient-centered cultural sensitivity requires empowering patients to routinely provide these data. Enabling participants to provide administrators with feedback on the level of patient-centered cultural sensitivity they perceive in their sites might be helpful to ensure that patients receive care that is high quality and that helps them feel comfortable, trusting, and respected.
Limitations
Despite the importance and methodological strengths of this study, its results must be interpreted with caution given its limitations. The first limitation of this study is the fact study participants were not randomly selected. This study had a volunteer, arbitrarily selected patient sample. Study researchers made efforts to include low-income, racial/ethnic minority patients as such patients are typically not adequately included in health care quality and outcomes research. Yet low-income and racial/ethnic minority patients have been documented to receive lower-quality health care.
The second limitation of the present study is that this sample was limited to individuals who were already receiving health care at the health care sites involved in this study. Patients who did not receive regular health care or were dissatisfied enough with the care received to not return to the sites may not have been adequately represented in this sample. This may further limit the generalizability of this study’s results.
The third limitation of this study is that participating health care sites were not randomly selected; instead, the participating sites volunteered to participate in this study in response to a participation invitation that was sent based on multiple site recruitment strategies including snowballing (ie, having participating sites inviting other nearby sites to be study participants). Given the difficulty involved in recruiting health care sites to be research participants, use of multiple recruitment strategies as done in the present study is not unusual. Health care site recruitment in the present study and in similar studies is difficult because of lack of familiarity with research procedures and goals among health care site administrators and staff, lack of time and/or knowledge to respond to research requests and/or to obtain research approval at their health care site, and concerns about the impact of research proposed on site–patient relationships. 37
A final limitation of this study is that all measures were self-reports. Some of the potential problems that come with using self-report measures include (a) partial/random completion of questionnaires by patients in order to receive financial compensation and (b) provision of “socially desirable” responses by patients. However, data collection for this study was conducted in an anonymous way to encourage participants to provide honest answers. Furthermore, self-report instruments have been found reliable in health care quality research in the past. 38
Future Directions
Despite its limitations, this study suggests that patients’ perceived patient-centered cultural sensitivity of health care sites is positively linked to their treatment adherence and that this linkage partially occurs through their satisfaction with health care experienced. Support is provided for future research similar to the present study with randomly selected health care sites and randomly selected patients from within these clinics. Support is also provided for future research studies that include patient objective health outcome data that are not difficult to obtain such HbA1c levels.