
Abstract
In recent years, there have been increasing national calls for patient-centered, culturally sensitive health care (PC-CSHC). The impetus for these calls include (a) the reality that health care providers are increasingly having to provide health care to a more culturally diverse patient population without the necessary training to do so effectively, (b) the growing evidence that culturally insensitive health care is a major contributor to the costly health disparities that plague our nation, and (c) the fact that racial/ethnic minorities and individuals with low household incomes are more likely than their non-Hispanic white and higher-income counterparts to experience culturally insensitive health care and dissatisfaction with health care—health care experiences that have been linked to poorer health outcomes. This article (a) presents literature on the definition of PC-CSHC and the need for this care, (b) presents research on assessing and promoting this care, and (c) offers research-informed strategies and future directions for customizing and institutionalizing this care.
Keywords
Cultural competence in health care involves having an understanding of culturally different patient groups and a respect for such groups . . .
Definition of Patient-Centered Culturally Sensitive Health Care (PC-CSHC)
Cultural Sensitivity Versus Cultural Competence
Culturally sensitive health care has been described as health care that effectively responds to the attitudes, feelings, and circumstances of people that share common identifying characteristics (eg, race, religion, language, and socioeconomic status) and health care that patients perceive as being concordant with their cultural values and beliefs. 1 Cultural sensitivity encompasses the related concept of cultural competence, which is often used to describe health care providers (eg, physicians, nurse practitioners, and physician assistants). Cultural competence in health care involves having an understanding of culturally different patient groups and a respect for such groups that ideally results in health care tailored to accommodate cultural differences in health-related values and beliefs.2-5
The major difference between cultural sensitivity and cultural competence in health care is the emphasis of cultural sensitivity on the perceptions and feelings of patients regarding whether or not the health care experienced is responsive to their health-related cultural values and beliefs. Indeed, health care providers may use their acquired knowledge of these cultural values and beliefs in health care delivery in ways that do not optimally convey awareness of this knowledge (ie, in ways in which this knowledge is not perceived by culturally diverse patients).
Patient-Centered Health Care
Because patients, rather than health care researchers and providers, are the true experts on what they need to be satisfied with their health care and to feel that their culture is respected, there has been growing recognition that culturally sensitive health care must be patient-centered.6,7 Patient-centered health care includes the following attributes: (a) respect for patients, (b) collaborative communication strategies, and (c) knowledge sharing between patients and their health care providers. 8 Patient-centered health care has been found to enhance patient-provider communication and improve treatment adherence, which in turn positively affects the health outcomes of patients.8,9
Patient-Centered Culturally Sensitive Health Care
PC-CSHC has been defined as health care that is reflective of culturally diverse patients’ perceptions regarding the health care characteristics that enable these patients to feel comfortable with, trusting of, and respected during the health care process. 6 PC-CSHC is empowerment oriented and conceptualizes the patient-provider relationship as a partnership that centers on the patient’s unique needs.6,10 Tucker et al 11 used a focus group research approach to empower culturally diverse patients (ie, African American, Hispanic/Latino, and non-Hispanic white patients) to identify specific characteristics of culturally sensitive health care (ie, PC-CSHC). Data from this focus group research revealed that such care involves multiple components of the health care delivery system. Specifically, from the perspectives of culturally diverse patients, PC-CSHC involves characteristics and behaviors of health care providers and office staff and the physical characteristics and policies of the health care site environment. This patient perspective is novel when compared with past conceptualizations of cultural sensitivity and cultural competence in health care that tend to focus exclusively on the role of health care providers in the delivery of culturally sensitive health care and not the other components of the health care delivery system.10,12 Yet, often, the terms culturally sensitive health care, culturally competent health care, patient-centered care, and patient-centered culturally sensitive health care are mistakenly used interchangeably. One way of conceptualizing these terms that indicates their differences is presented in Figure 1.
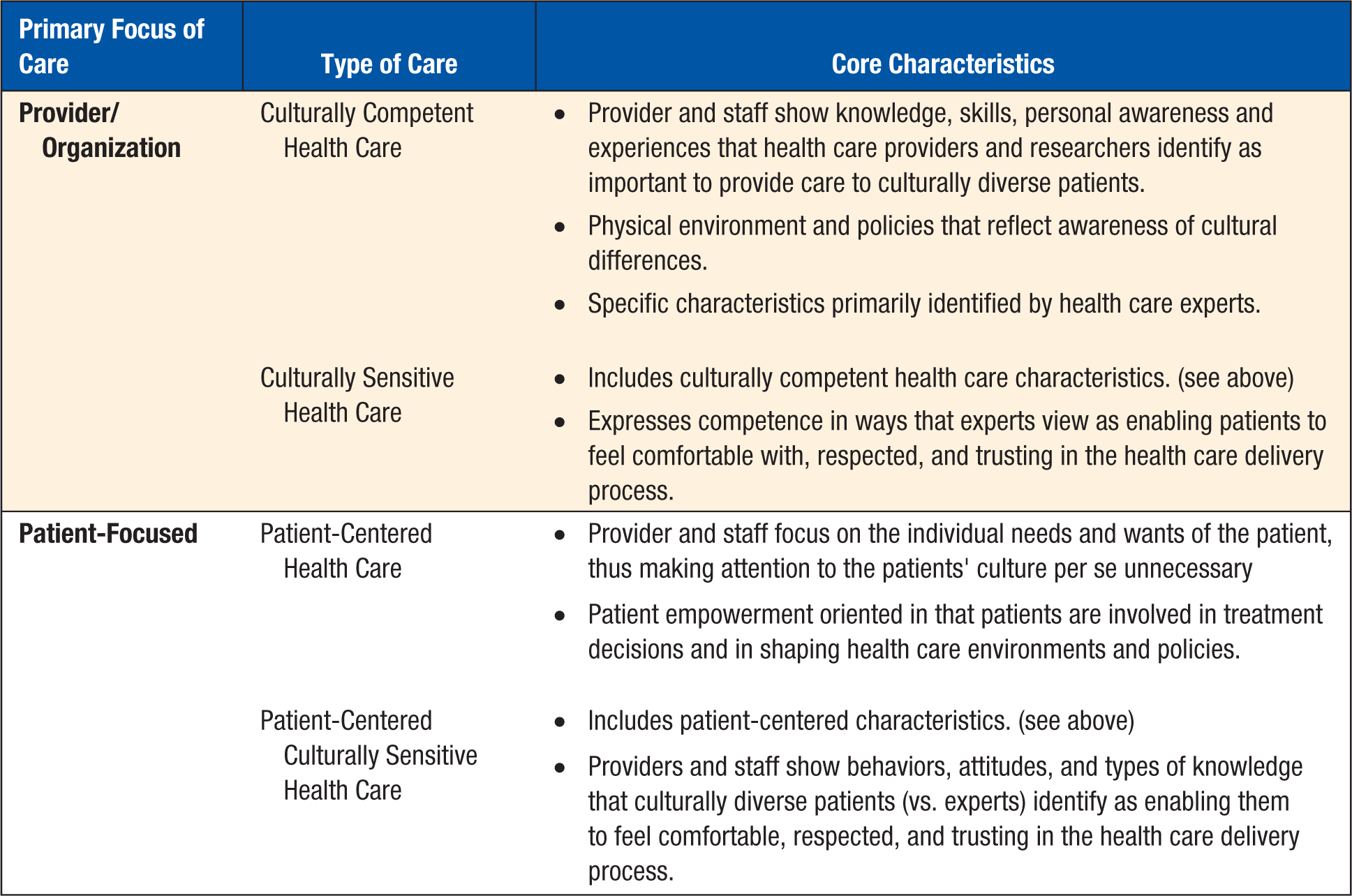
Types of Care.
Literature Indicating the Need for PC-CSHC
There is much agreement that the level of cultural sensitivity in health care that patients experience positively influences their adherence to treatment and, ultimately, their health outcomes.13,14 Low adherence to recommended treatment behaviors among ethnically and racially diverse patients is to some degree a result of the limited levels of culture-related knowledge, skills, experience, and awareness demonstrated by their health care providers. 15 Studies have shown links between cultural sensitivity/competence and patient satisfaction16-18 and cultural sensitivity/competence and improved health outcomes of racial/ethnic minorities.12,19,20 Furthermore, there is some indication that perceived cultural sensitivity of health promotion interventions is positively associated with the effectiveness of these interventions. For example, culturally sensitive health promotion interventions have been found to be effective when implemented with adults who have low levels of literacy 21 and among working class multiethnic employees. 22
Health Disparities
Empirical evidence of the prevalence of race/ethnicity and income-related health disparities among minority populations in the United States is startling. For example, African American and Hispanic populations experience poorer health outcomes related to diabetes, cancer, HIV, and infant mortality when compared with non-Hispanic white populations.23,24 Alarmingly, these health disparities persist after controlling for unhealthy behaviors and inadequate access to health care. 25 Similarly, groups with low household incomes are more negatively affected by health disparities, even when controlling for other demographic variables. 26
Given that treatment nonadherence and poor health outcomes among racial/ethnic minority patients and patients with low household incomes are associated with culturally insensitive health care 27 and that all 3 of these variables are factors contributing to health disparities, 27 disparities in health are a major part of the impetus for national calls for PC-CSHC. Eliminating disparities in health is a part of the overarching goals for Healthy People 2020, thus making health disparities a continued public health priority.27-29
A PC-CSHC Model
The development of evidence-based interventions to promote PC-CSHC has been impeded by the lack of a comprehensive model to provide the foundation for research to inform such interventions. Specifically, there is a recognized need for theoretical models that link perceived cultural sensitivity in health care experienced by patients to the health behaviors (eg, treatment adherence and health promoting behaviors) that affect these patients’ health outcomes/statuses.
Tucker et al 10 proposed a literature-based theoretical model—the PC-CSHC Model—that describes the process by which patients’ experience of PC-CSHC leads to patient health behaviors and outcomes. The PC-CSHC Model makes the following research-based assumptions: (a) culturally sensitive health care delivery is complex and multifaceted and involves patients, health care providers, office staff, and the health care site environment and policies; (b) PC-CSHC can be promoted through targeted trainings that increase patient empowerment and improve the culturally sensitive health care demonstrated by providers and office staff and displayed via the physical environment characteristics and policies of the health care site; (c) this care affects patients’ perceptions regarding the cultural sensitivity of their care from health care providers and, in turn, increases their engagement in health-promoting behaviors and health care satisfaction; (d) health care satisfaction is positively associated with patients’ treatment adherence (ie, dietary and medication adherence); and (e) patient treatment adherence and engagement in health promoting behaviors is directly and positively associated with patients’ health outcomes (eg, BMI, blood pressure, and glucose levels). This model was more recently modified to include physical stress as a variable that influences treatment adherence. 6 Physical stress was included in the model because physical stress indicators, such as headaches, pain in the chest, and tense muscles, tend to more immediately deter health-promoting behaviors such as exercising and dietary and medication adherence than, for example, cognitive stress indicators such as periodically having difficulty concentrating and feeling out of control. Furthermore, physical stress indicators are more reliably quantified by patients than cognitive stress indicators because the latter indicators are often difficult to define for the purpose of measurement among patients. The most recently modified version of the PC-CSHC Model is depicted in Figure 2.
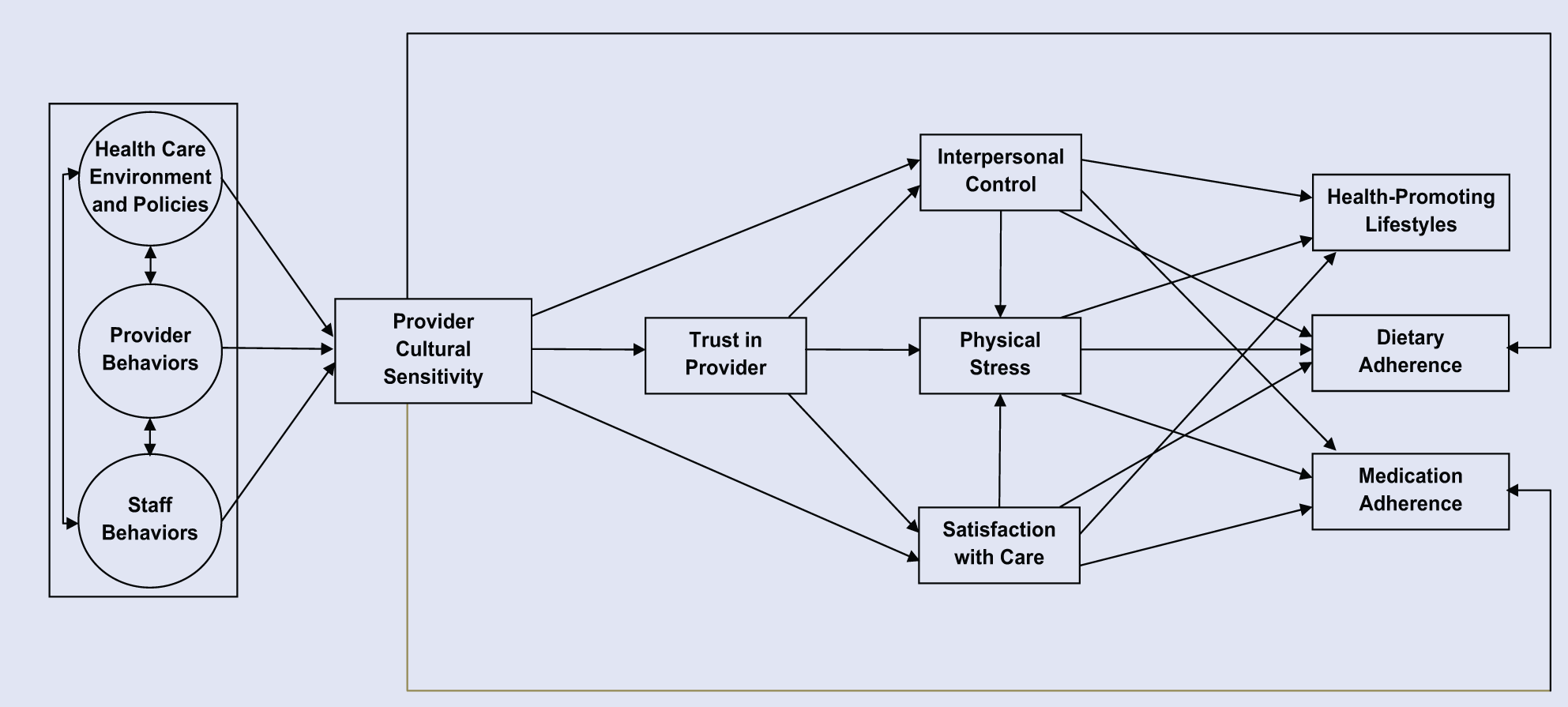
Patient-Centered Culturally Sensitive Health Care (PC-CSHC) Model.
It is noteworthy that the aspect of the PC-CSHC Model that asserts that health care environment and policies and health care staff behaviors as well as provider behaviors affect each other and ultimately influence patient satisfaction is consistent with important aspects of Aday and Andersen’s framework 30 for studying health care access and its relationship to patient/consumer satisfaction. For example, within this framework, health care policies influence the characteristics of the health care delivery system, which in turn influence both utilization of health services and patient/consumer satisfaction with care. Characteristics of the health care system include how the patient is treated at entry into the health care system, including wait time, who the patient sees, and how the patient is treated by medical and other staff in the health care delivery process. The PC-CSHC Model is different from Aday and Andersen’s framework in that the former gives more attention to highly modifiable behaviors of providers and staff and how these behaviors affect the psychological/emotional experiences of patients, patients’ satisfaction with care, and ultimately patients’ health outcomes.
Model Development
Examples of research literature underlying the development of the PC-CSHC Model include research findings indicating that displays of cultural sensitivity by health care providers result in their patients having feelings of comfort with and trust of their providers, both of which enhance patients’ satisfaction with care by their providers22,31 and patients’ sense of interpersonal control in the health care process. 32 The PC-CSHC Model is also informed by research indicating that patients’ satisfaction with provider care and their perceived interpersonal control reduce their level of physical stress when interacting with health care providers and staff, 33 and all 3 of these variables influence patients’ likelihood of following their health care provider’s recommended treatment regimens, which include engagement in a health-promoting lifestyle34,35 and medication and dietary adherence.36,37 Additionally, following recommended treatment regimens directly affects health outcome variables.38,39
Stress is commonly experienced by patients in the health care process as evidenced by the “white coat hypertension” phenomenon (ie, patient blood pressure increases in the presence of a health care provider), 40 and African Americans are at risk for perceived or experienced racism-related stress 41 from, more than likely, unintentional racial bias in the health care process.42,43 Given this, it was deemed particularly important to include physical stress in the PC-CSHC Model. Such stress, as well as other health care circumstances (eg, receiving negative test results), can impede patients’ understanding of treatment recommendations and/or willingness to follow these recommendations, resulting in treatment nonadherence by these patients. Conversely, patients’ satisfaction with their health care and perceived interpersonal control in interactions with their health care providers can contribute to patients experiencing lower stress, and all 3 of these experiences can promote the psychological calmness needed to understand and follow recommended treatment regimens, including health-promoting lifestyle behaviors and medication and diet regimens.
Model Testing
The earlier mentioned most recently modified version of the PC-CSHC Model (as depicted in Figure 2) was empirically tested in a study using patient data from mostly low-income samples of African American patients and non-Hispanic white patients. Results from this study provided support for this model. 6 The specific model-based hypotheses that were tested in the study are as follows: (a) the most proximal and direct impact of provider cultural sensitivity perceived by patients will be on patients’ sense of trust in their provider, satisfaction with the provision of care by their provider, and their sense of interpersonal control; (b) patient satisfaction with provider care and sense of interpersonal control will have indirect effects (through perceived levels of physical stress) on patient treatment adherence (ie, dietary and medication adherence) and engagement in a health-promoting lifestyle; and (c) patient physical stress, satisfaction with provider care, and sense of interpersonal control will also have direct effects on patient treatment adherence and engagement in a health-promoting lifestyle. Because health outcome data were not obtained for the samples used in this test of the PC-CSHC Model, there was no hypothesis regarding the effects of treatment adherence and engagement in a health-promoting lifestyle on health outcomes. 6
Preliminary Pearson correlation analyses were performed to determine the correlations among all investigated variables separately for the African Americans as a group and the non-Hispanic whites as a group. The resulting correlations for each group were at least moderate in effect size at the P < .05 (see Table 1). 6
Correlations Among Variables for the African American and non-Hispanic White Patients. a
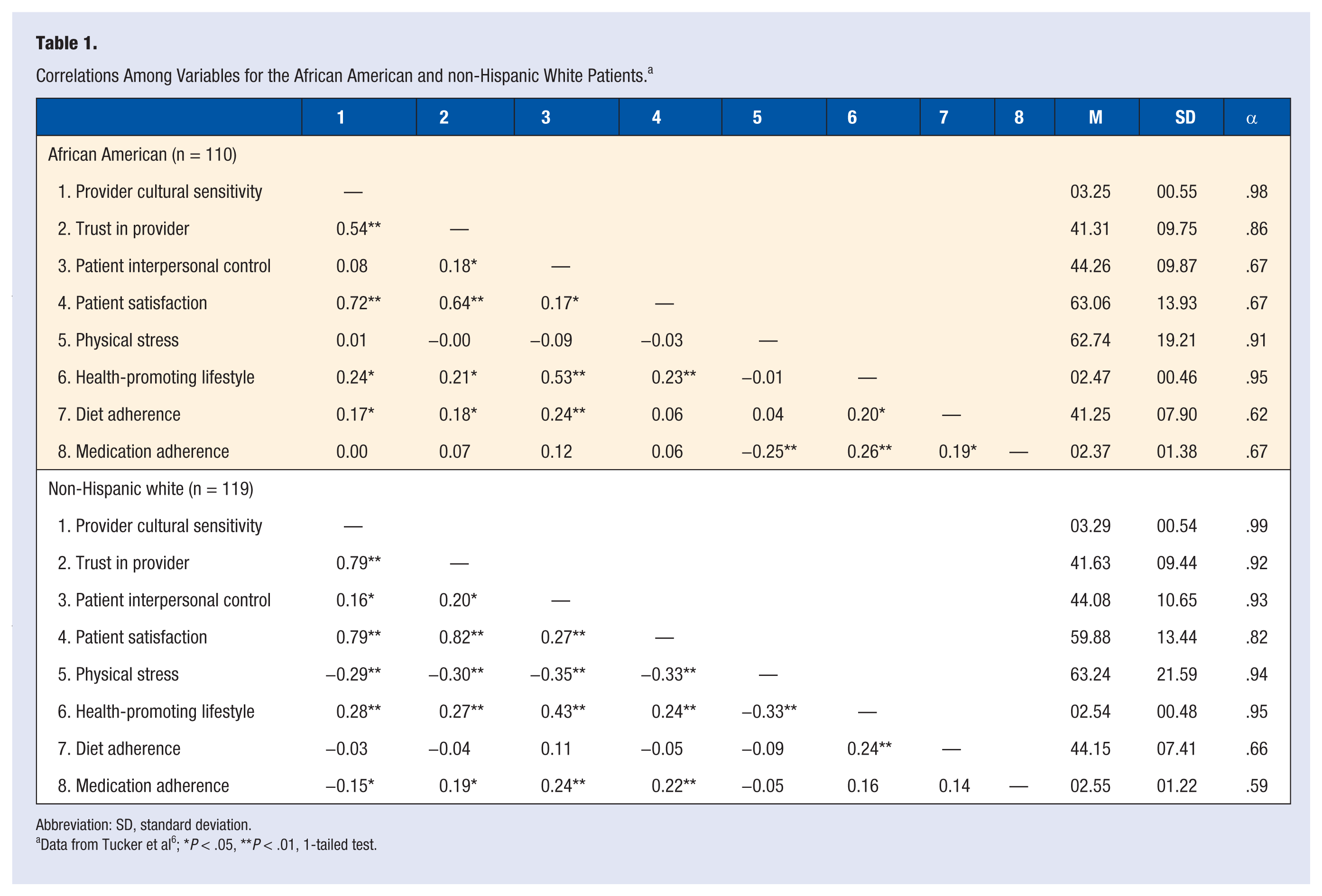
Abbreviation: SD, standard deviation.
Data from Tucker et al 6 ; *P < .05, **P < .01, 1-tailed test.
A 2-group path analysis was used to test the earlier specified model-based hypotheses. This path analysis is described in the article to test the PC-CSHC Model. 6 In sum, it is stated in this article that all coefficients were allowed to be freely estimated across the 2 groups in the path analysis. The invariance of the path model across groups was tested using full-information likelihood estimation. Significance tests were conducted using bootstrapped estimates of standard errors for all effects (ie, direct, indirect, and total effects). Additionally, group differences in effect strength were examined. To do this, 95% confidence intervals were constructed using the standard errors for each group, and the effects from each group were examined for overlap with the confidence interval of the other group.
Findings from the 2-group path analysis to test the earlier specified model-based hypotheses are as follows: (a) patient-perceived provider cultural sensitivity had significant positive direct effects on patients’ sense of trust in their provider and satisfaction with provider care in both racial/ethnic groups (ie, African American and non-Hispanic white patients), but the effect on trust in provider was significantly larger (P < .05) for non-Hispanic whites, and the effect on satisfaction with provider care was significantly larger (P < .05) for African Americans; (b) provider cultural sensitivity had a significant positive direct effect on dietary adherence for African Americans only, and this effect was significantly larger (P < .05) than in non-Hispanic whites; (c) trust in provider had significant direct effects on satisfaction with provider care in both racial/ethnic groups, although the effect was significantly larger (P < .05) for non-Hispanic whites; (d) sense of interpersonal control had a significant negative effect on perceived physical stress for non-Hispanic whites, whereas it had a significant positive effect on dietary adherence for African Americans; (e) sense of interpersonal control had a significant positive direct effect on health-promoting lifestyle in both racial/ethnic groups; however, the effect was significantly larger (P < .05) for African Americans; (f) perceived physical stress had a negative effect on medication adherence but only for African Americans; and (h) patient-perceived provider cultural sensitivity had a significant positive indirect effect on satisfaction with provider care in both racial/ethnic groups, although the effect was significantly larger for non-Hispanic whites than African Americans (P < .05; see Table 2). 6
Direct, Indirect, and Total Effects: Evaluation of Predictor Effects and Race/Ethnic Group Differences. a
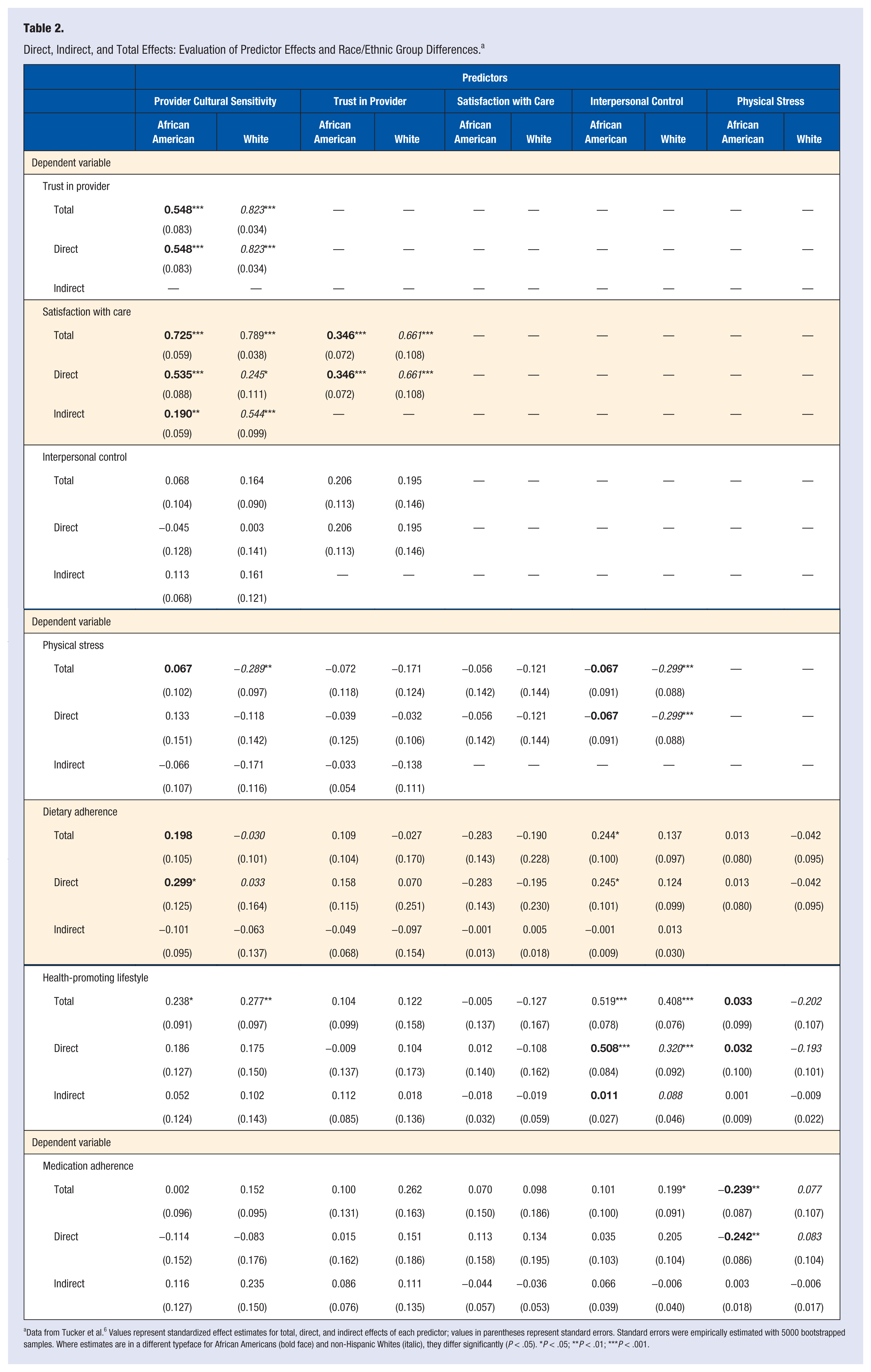
Data from Tucker et al. 6 Values represent standardized effect estimates for total, direct, and indirect effects of each predictor; values in parentheses represent standard errors. Standard errors were empirically estimated with 5000 bootstrapped samples. Where estimates are in a different typeface for African Americans (bold face) and non-Hispanic Whites (italic), they differ significantly (P < .05). *P < .05; **P < .01; ***P < .001.
An important conclusion from these findings is that the PC-CSHC Model should be tested separately with different racial/ethnic minority and other cultural groups because the linkages between patient-perceived provider cultural sensitivity, patient treatment adherence, patient engagement in health-promoting lifestyle, and health outcomes may be different and/or differ in strength by racial/ethnic or cultural group. This conclusion is consistent with the Difference Model research approach, which advocates for separately studying groups that are culturally different on major culture-related variables such as race/ethnicity and income. 44
Measures of PC-CSHC
In 2005, the Agency for Healthcare Research and Quality made a call for standardized and valid measures for evaluating the degree to which health care providers and health care sites were providing culturally sensitive health care. 45 Given that cultural sensitivity is different from cultural competence, as earlier discussed in this article, measures of cultural sensitivity are necessarily different from existing measures of cultural competence. Thus far, research to develop measures of cultural sensitivity, in general, and measures of patient-centered cultural sensitivity in health care, in particular, have been limited. Furthermore, the overwhelming majority of available cultural sensitivity and cultural competence inventories have relied on the views of health care professionals in their development rather than on the views of the true “experts” on cultural sensitivity—culturally diverse patients.10,46
Mirsu-Paun et al 47 claim, with 1 known exception, that the main limitations of instruments designed to measure culturally sensitive or culturally competent health care are that their items (a) are not research based, (b) were developed from the perspective of professional experts rather than the true “experts” (patients), and (c) concentrate on specific knowledge pertaining to racial/ethnic groups, ignoring broader aspects of culturally sensitive health care or specific aspects of the cultural sensitivity of health care sites (eg, health care site hours that accommodate patients in low-status, hourly wage jobs that do not allow paid time off for health care visits). The 1 known exception is a set of measures of PC-CSHC developed by Tucker et al.6,48
Development of the Measures
The research that resulted in the above-mentioned set of measures of PC-CSHC began with a previously discussed focus group study by Tucker et al. 11 This study involved having participants in race/ethnicity-specific focus groups (1 group for African American patients, 1 for non-Hispanic white patients, and 1 for Hispanic patients) identify health care provider and office staff behaviors and health care site characteristics (physical environment characteristics and policies) that they considered indicators of culturally sensitive health care. This approach is patient-centered, in that the focus groups allowed the voices and perspectives of patients to be heard.
Following the focus group study, research was conducted in which the focus group data were used to construct measures of PC-CSHC. 10 In this research, an independent sample of African American, Hispanic, and non-Hispanic white patients rated the importance of the focus group generated items as indicators of cultural sensitivity and made these ratings using a Likert-type scale from 1 to 5, where 1 = not important at all and 5 = very important. Items that were considered important (mean rating of 3 or higher) were retained and used to construct 3 pilot race/ethnic-specific Tucker-Culturally Sensitive Health Care Inventories. The pilot inventory for African American patients and the one for non-Hispanic white patients were found to have more than adequate test-retest and split-half reliabilities (ranging from 0.92 to 0.99) and internal consistency (ranging from 0.71 to 0.96). 49 The small number of Hispanic patients from whom reliability data could be obtained precluded determining reliabilities of the race/ethnicity-specific inventory for Hispanics. 10
Because of the item similarities among the pilot race/ethnicity-specific inventories, these inventories, which were originally divided into 3 subscales (ie, provider attitudes and behaviors, staff attitudes and behaviors, and health care center characteristics), were combined into 1 inventory (no longer race/ethnicity-specific) with the same 3 subscales. Furthermore, each of the 3 subscales was transformed into a separate inventory, thus resulting in the following 3 inventories: (a) the Tucker-Culturally Sensitive Health Care Provider Inventory–Patient Form; (b) the Tucker-Culturally Sensitive Health Care Office Staff Inventory–Patient Form, and (c) the Tucker-Culturally Sensitive Health Care Clinic Environment Inventory–Patient Form. Additionally, the Tucker-Culturally Sensitive Health Care Provider Inventory–Provider Form, which is a self-evaluation version of this inventory for use by health care providers, was created by changing the instructions on this inventory, so that a provider completing it is asked to rate the degree to which the items listed were characteristic of her/him.
Psychometrics of the Measures
Using data from a national study on PC-CSHC at primary care clinics funded by a grant from the Robert Wood Johnson Foundation, Tucker and her colleagues determined that the patient forms of the 3 above-mentioned inventories were reliable and valid. Specifically, results of data analyses revealed the following: (a) for the Tucker-Culturally Sensitive Health Care Provider Inventory–Patient Form, the subscales (based on factor analyses) and their Cronbach’s αs are Competence/Confidence (α = .96), Sensitivity (α = .94), and Respect/Communication (α = .94), and the Cronbach’s alpha for the overall scale is .9750; (b) for the Tucker- Culturally Sensitive Health Care Office Staff Inventory–Patient Form, the subscales and their Cronbach’s αs are Sensitivity/Interpersonal Skill (α = .97) and Professionalism, Punctuality, and Responsiveness (α = .95), and the Cronbach’s α for the overall scale is .97 (C. M. Tucker, unpublished data, 2012); and for the Tucker-Culturally Sensitive Health Care Clinic Environment Inventory–Patient Form, there are no subscales, and the Cronbach’s α for the overall scale is .93. 51 To determine the validity of the subscales and overall scales found in each study, a Pearson correlation analysis was performed to determine the correlations between the scales and the subscales of the Patient Satisfaction Questionnaire–18. 52 Results indicated that all correlations were significant and positive, thus providing support for the validity of each of the 3 inventories.
The reliability and validity of the Tucker-Culturally Sensitive Health Care Provider Inventory–Provider Form, which is a self-evaluation version of this inventory for use by providers, was tested in a study with 217 advanced medical students as participants. 47 Five subscales of this inventory were established, and their Cronbach’s αs are as follows: Patient-Centeredness (α = .94), Interpersonal Skills (α = .84), Disrespect/Disempowerment (α = .75), Competence (α = .72), and Cultural Knowledge/Responsiveness (α = .77). With the exception of the Disrespect/Disempowerment subscale, these subscales had significant positive correlations with the Service Delivery and Practice subscale of the Cultural Competence Self-Assessment Questionnaire–Service Provider Version, 53 thus providing support for the validity of the Tucker-Culturally Sensitive Health Care Provider Inventory–Provider Form. 47
Application of the Measures
The above-mentioned inventories for measuring PC-CSHC are novel in that they consist of items generated by low-income individuals and/or racial/ethnic minority individuals—groups often underrepresented in health care research. Additionally, more culturally diverse groups were involved in establishing the psychometric properties of the inventories, thus making them appropriate for use with culturally diverse patients. These inventories can be used as (a) assessment tools to identify needed areas of health care provider and office staff training and needed environment and policy changes to promote PC-CSHC and (b) measures to assess changes in patient-perceived cultural sensitivity among health care providers and office staff and in health care environments (policies and physical characteristics) that occur in association with interventions to promote PC-CSHC.
Interventions to Promote PC-CSHC
Training of Providers
To date, health care providers are typically offered or required to participate in expert-centered culturally competent health care training but emerge from this training engaging in behaviors and attitudes that culturally diverse patients do not recognize as indicators of cultural competence. 54 This state of affairs suggests that it is important that health care providers engage in training that is primarily based on what culturally diverse patients view as indicators of health care provider and office staff cultural sensitivity. Such training can appropriately be called PC-CSHC training, which involves the following: (a) providing opportunities for culturally diverse patients to identify the indicators of culturally sensitive health care and to assess the levels of occurrence of these indicators at the target health care site(s), (b) requesting and providing incentives for health care providers to self-assess the degree to which they display the patient-identified indicators of culturally sensitive health care that are specific to providers, and (c) using the assessment data from patients and health care providers at the target sites to develop and/or customize the training.
The assessment, feedback, and evaluation process to develop PC-CSHC training must occur at health care sites periodically over time rather than once a year, as is often the case with such training, given that (a) the composition of health care providers, office staff, and patients at any given health care site changes periodically and (b) individual health care providers and organizations vary in their training needs, including training needs over time. The earlier mentioned PC-CSHC inventories can be used in the assessment and evaluation aspects of developing PC-CSHC training.
An important aspect of PC-CSHC training for health care providers is recognition of the importance of patient-centered patient-provider partnerships and knowledge of the characteristics of such partnerships. Most important to these partnerships are patients who are actively involved in identifying their needs, values, and preferences and providers who actively show empathy, compassion, and responsiveness in relation to these assessed patient needs, values, and preferences. 54 These partnerships have been associated with increased patient adherence to treatment, 55 improvements in the health statuses of patients, 56 and reductions in misdiagnosis of patients’ health problems as a result of poor patient-provider communication. 57 Moreover, patients want to be active partners in their health care.58,59
Another important aspect of PC-CSHC training is teaching health care providers, office staff, and administrators at health care sites ways to empower patients, particularly racial/ethnic minority patients, to assume active roles in their health care. Researchers who have studied empowerment of African Americans 60 and Hispanics 54 agree that empowerment of racial/ethnic minorities must include enabling them to experience a sense of intrapersonal and interpersonal control and attending to social, political, economic, and legal factors that influence this perceived control. Promotion of perceived and actual control among patients in general, and racial/ethnic minority patients in particular, involves giving patients opportunities to (a) provide input on health care services and policies, (b) evaluate all aspects of the health care experienced, and (c) ask questions and express concerns about their health and health care and have these questions and concerns respectfully addressed in a timely manner. Such patient control-oriented activities become realities through having patients included on health care site advisory boards and administrative teams—groups that typically control the resources and policies of these health care sites.
In recent years there has been growing recognition that patient empowerment in the health care process will not really occur without health care legislation that supports this empowerment. An example of such legislation is the Patient Protection and Affordable Care Act passed in 2010. 61 This legislation includes many required actions that will enable patient empowerment, including a mandated review of medication/drug labels with the objective of making these labels more understandable, particularly to individuals with low education levels. The ultimate goal of this legislation is empowering the nearly 87 million adult patients with low literacy levels and the 24 million adults with limited English proficiency to make informed decisions and take charge of their own health care. 61
Training of Office Staff
Training of office health care staff members in PC-CSHC is clearly important, given the reported associations between health care office staff members’ cultural sensitivity/competence and positive patient outcomes.7,10,62,63 Furthermore, in a study by Sofaer and Firminger, 7 patients defined cultural sensitivity of office staff as an essential component of patient-centered care. Additionally, Barr and Wanat 62 found in a focus group study that ethnic minority patients often identified lack of cultural sensitivity on the part of nonmedical office staff as a barrier to their care.
As is the case with training providers, training of health care office staff to engage in PC-CSHC should ideally be informed by behaviors and attitudes of office staff that culturally diverse patients have identified as culturally sensitive. Levels of these behaviors and attitudes at a target health care site can be assessed by having patients complete the earlier-mentioned inventory to assess the cultural sensitivity of office staff. Additionally, this inventory can be used to evaluate the patient-perceived impact of training to promote the cultural sensitivity of health care office staff.
Existing research on training health care office staff to engage in PC-CSHC suggests that this training should be similar to that for health care providers but include an emphasis on (a) displaying behaviors and attitudes that reflect a high regard for patient confidentiality, (b) ways to show patients that they have priority over office work (eg, warmly greeting patients immediately on arrival at the check-in desk), (c) keeping patients informed of the wait time before seeing a provider, (d) communicating policies and other information that patients need to know, (e) assisting or arranging assistance for patients who may have difficulty completing required paperwork, and (f) ways to show respect for patients (eg, addressing them as Mr, Mrs, or Dr unless otherwise requested by the patient). 11 However, behaviors and actions targeted in this health care office staff training require support from health care administrators and must be supported by culturally sensitive health care environments and policies.
Health Care Environment and Policy-Focused Intervention
Adaptation of health care site environments and policies to make them more culturally sensitive by the standards of culturally diverse patients has also received considerable empirical support. Research has identified positive associations between increased cultural sensitivity of health care physical environments and policies (ie, patient-centered cultural sensitivity at the organizational/systemic level) and positive patient outcomes, including patient satisfaction and patient treatment adherence.64-67 For example, provision of reader-friendly materials at health care sites has been found to be positively associated with positive patient outcomes.68-70 Additionally, interventions that help patients schedule and keep their appointments (eg, telephone reminders), expand scheduling flexibility, reduce waiting times, and provide a welcoming (spacious, well-furnished, and well-equipped) health care site environment have been found to positively influence treatment adherence.27,65,71-73 Andrulis et al 74 recommends the implementation of culturally sensitive practices at the organizational level as a way to decrease and eventually eliminate racism in health care practices.
In spite of the research positively linking patient-centered culturally sensitive physical environment characteristics and policies at health care sites to patient outcomes, many of these sites still remain culturally insensitive in many ways. For example, there is still a mismatch between existing reading materials at most health care sites in the United States and patients’ actual literacy level. 75 Vaughn et al 75 concluded that health care materials patients have access to are issued at a much higher reading level (average = 9.34) than patients’ average reading level (equal to or less than 5th grade). Other studies have led to similar conclusions.69,70
An important intervention to promote PC-CSHC environments and policies must include training health care site administrators on their importance for positive patient outcomes. The views of culturally diverse patients suggest that such environments and policies include having culturally diverse health care providers and office staff, interpreters for patients who prefer communication in a language other than English, areas for private conversations with the front desk staff, policies about the order in which patients are seen to avoid discrimination in this process, keeping the health care site areas clean and professional looking, and having consistent health care providers over time and health assistance programs that help those with low incomes.11,51 Such environments and policies will more likely occur when using, versus not using, the earlier-mentioned patient-empowerment strategy of involving patients on health care site advisory boards and administrative teams. More research is needed to empirically evidence the impact of such patient-empowerment interventions in health care sites.
Training of Patients
Research has found that patients who are empowered in regard to their health and health care are more successful at preventing/managing disease and navigating the health care system. 76 Patient involvement in programs to educate them about the care they are receiving has been found to be positively associated with positive patient outcomes and increased satisfaction with care in patients of diverse socioeconomic backgrounds.77-80
It is also important to involve patients in patient-empowerment training designed to provide them with skills and knowledge that will enable them to take charge of their health and health care to the degree desired. Such empowerment training is needed, given that disempowerment has been identified as a significant health risk factor, especially for disadvantaged populations like racial/ethnic minorities. 81 Empowerment has been described as an avenue to increase the relevance and quality of medical knowledge 82 and as a “health enhancing process.” 83
Given the powerlessness and intimidation that lower-educated and lower-income patients and many other patients across socioeconomic and education statuses often feel in the health care process, it is important that patient-empowerment training includes (a) teaching patients assertiveness skills, anxiety/stress management skills, interpersonal/communication skills (eg, listening skills), and behavior management skills (eg, skills for giving positive feedback and constructive negative feedback to health care providers and skills for using self-praise) 84 and (b) promoting health literacy (eg, provision of information needed to read and understand medication and food labels, to find and successfully use various available health care and health promotion services, and to be ready for a health care visit, such as making a list of questions to give the provider when she/he begins the clinical encounter).84-87 Patient-empowerment training can be provided by health psychologists and behavioral medicine professionals as well as by other professionals and community health workers trained to provide this training. However, it is important that the trainers include some individuals of the cultural backgrounds represented among the patients being trained. Patient-empowerment training can occur at health care sites; however, it is most ideal for this training to occur in community settings (eg, churches and community centers) because such settings allow patients to obtain this training confidentially.
Customized PC-CSHC
Patients within and across racial/ethnic, gender, and income groups differ to some degree in what they identify as characteristics of PC-CSHC or by the importance of the many common characteristics of this care. 11 For example, some patients may report that this culturally sensitive care involves their providers being direct with them and explaining information in more detail, whereas other patients may report that such care involves providers understanding their culture and not “talking down” to them. Consequently, it is clear that there is a need for “customized” PC-CSHC (ie, individualized patient care), particularly by health care providers when in a clinical encounter with patients. Such care avoids the criticisms by some providers that culturally sensitive/competent health care fosters cultural stereotyping—a criticism that has caused resistance to cultural sensitivity/competence training among some health care providers.
The modified version of the earlier-mentioned inventory for assessing the cultural sensitivity of health care providers (ie, the Tucker-Culturally Sensitive Health Care Provider Inventory) can be used to promote “customized” PC-CSHC. Specifically, this care can be facilitated by modifying the instruction on this inventory from rating the degree to which each of the provider behaviors, attitudes, and types of knowledge on the inventory are descriptive of the patient’s health care provider to rating the degree to which each of these are important to the patient. This modified inventory is referred to as the Provider Cultural Sensitivity Clinical Tool.
The Provider Cultural Sensitivity Clinical Tool can be used to “customize” PC-CSHC by providing the specific provider behaviors, attitudes, and types of knowledge (ie, cultural sensitivity indicators) that matter most to each individual patient. For example, prior to the clinical encounter with each of their patients, health care providers can obtain the cultural sensitivity indicators most important to their patients by having each of them complete the Provider Cultural Sensitivity Clinical Tool. The top 5 patient-specific cultural sensitivity indicators rated as most important on this clinical tool by each patient can be displayed by her/his provider during the clinical encounter with the goal of improving the patient’s perceptions regarding the cultural sensitivity of the provider. The previously discussed research involving mostly African American patients and non-Hispanic white patients with low household incomes to test the PC-CSHC Model provides evidence for how improving patient-perceived cultural sensitivity by providers can lead to increased patient treatment adherence (ie, dietary and medication adherence) and engagement in a health-promoting lifestyle and ultimately improving health outcomes of patients. 6
Conclusion
Public health initiatives to eliminate health disparities and provide equal health care to all patients, regardless of their race, ethnicity, or cultural background, have resulted in national calls for culturally sensitive health care. Furthermore, such care must be patient-centered, given that patients are the true experts on what they need to be satisfied with regarding their health care and what constitutes culturally sensitive health care. 4
The earlier-discussed PC-CSHC Model offers a literature-based framework for understanding patients’ experience of PC-CSHC and for research to determine the process by which this care affects patients’ health outcomes. Indeed, PC-CSHC will not flourish without the needed research showing the linkages between this care and positive patient health outcomes. Such outcomes will help reduce the high cost of health care and the health disparities that plague our nation.
The recently developed assessment inventories to assess levels of PC-CSHC by health care providers and office staff or in physical health care environments and policies have enabled the development of interventions to promote this care, evaluation of the effectiveness of this care, and customization of this care. The novelty of these inventories is that they consist of items that describe this care from the perspectives of culturally diverse patients because these patients are the experts on this care. Research is needed to further establish the reliability and validity of these inventories with different patient populations.
PC-CSHC cannot occur without (a) health care policies that support this care, (b) culturally diverse patients being trained to and given the opportunity to be active, empowered partners in their care, and (c) ongoing training of medical and nursing students, veteran health care providers, and health care office staff and administrators to engage in this care. PC-CSHC will not occur without increased research evidencing its contribution to eliminating health disparities and to reducing the cost of health care for all Americans.
Footnotes
Acknowledgements
Thank you to the Robert Wood Johnson Foundation for providing grant funding to develop the Patient-Centered Culturally Sensitive Health Care (PC-CSHC) Model and the culturally sensitive health care inventories discussed in this article. Copies of the culturally sensitive health care inventories can be requested from Dr Carolyn M. Tucker by e-mail: