
Abstract
The purpose of this review was to summarize findings from epidemiological studies that determined if sedentary behavior was associated with obesity, metabolic risk factors, and cardiorespiratory fitness in children and adolescents. We noted if studies adjusted for moderate-to-vigorous physical activity (MVPA), dietary intakes, and/or sleep duration. Articles were identified through PubMed using the search terms: (sedentary OR sitting OR television) AND (adiposity OR blood pressure OR body mass index OR cardiometabolic OR metabolic risk OR waist circumference). The search was limited to ages 6 to 18 years, humans, and published between January 1, 2008 and September 26, 2012. Cross-sectional and longitudinal studies observed associations between more sedentary behavior, especially screen-based sedentary behavior, and measures of obesity; and most associations were independent of MVPA and dietary intake. Cross-sectional and longitudinal studies reported associations between screen-based sedentary behavior and lower cardiorespiratory fitness, and most associations were independent of MVPA and obesity. Cross-sectional studies observed associations between more screen-based and objectively measured sedentary behavior and lower insulin sensitivity; and most associations were independent of MVPA and obesity. There was little-to-no evidence that sedentary behavior was associated with increased blood pressure and increased blood lipids.
‘Cross-sectional studies cannot determine temporal sequence, but longitudinal studies can provide evidence if sedentary behavior leads to poorer health.‘
Introduction
The growth in electronic media, along with the rise in automotive transport, has encouraged sitting and discouraged ambulation, and at present the majority of waking hours are spent in sedentary behavior. 1 Interestingly, when opportunities to spend time in sedentary behavior were increasing chronic diseases increased in parallel. 2 These data provide a basis for the hypothesis that spending too much time in sedentary behavior is detrimental to health.
Epidemiological studies have tested this hypothesis, and indeed there is evidence that excessive sedentary behavior is associated with poorer health. 3 However, before drawing conclusions based on such associations, it is important to ask if other health behaviors have been taken into account, notably, physical activity levels and dietary intakes. The rationale for doing so is that an association between sedentary behavior and poor health may be explained by less time spent in moderate-to-vigorous physical activity (MVPA) with more time spent in sedentary behavior and/or an increase in caloric intake with more time spent in sedentary behavior.4,5 Importantly, not all epidemiological studies have adjusted for these key covariates and so the results of those studies remain open to interpretation. It is also important to consider the study design when assessing evidence of an association between sedentary behavior and health outcomes. Cross-sectional studies cannot determine temporal sequence, but longitudinal studies can provide evidence if sedentary behavior leads to poorer health.
In this review, we will summarize findings from epidemiological studies that investigated the association between sedentary behavior and health outcomes in children and adolescents. The focus on children and adolescents is particularly important as contemporary children and adolescents spend, on average, in excess of 50% of waking hours in sedentary behavior and the proportion of waking hours spent in sedentary behavior increases as children age.6-8 Such high levels of sedentary behavior may be associated with poorer health and in this review we will summarize findings from epidemiological studies that investigated the association between sedentary behavior and obesity, metabolic risk factors, and aerobic fitness.
Methods
Article Search
Key articles were identified through the PubMed database, using the following search terms: (sedentary OR sitting OR television) AND (adiposity OR blood pressure OR body mass index OR cardiometabolic OR metabolic risk OR waist circumference). The search was limited to humans, aged 6 to 18 years, and published in English between January 1, 2008 and September 26, 2012. A total of 907 articles were found, and after reviewing the titles and abstracts 87 articles were identified that investigated the association between sedentary behavior and health outcomes in youth. Two studies in press were also included in this review, which were not indexed in the PubMed database at the time the search was conducted.9,10 Systematic reviews documenting the association between sedentary behavior and health outcomes in children and adolescents have been published.11,12 Our review adds to this literature by highlighting and discussing the role of MVPA, dietary intakes, and sleep duration on the relationship between sedentary behavior and health outcomes. We did not include multicomponent lifestyle interventions that included a sedentary behavior component, since our focus was strictly on the health outcomes associated with sedentary behavior.
Sedentary Behavior Definition and Measurement
Sedentary behavior refers to activities that require little-to-no additional energy expenditure above resting metabolic rate (ie, 1.0-1.5 metabolic equivalents). 4 A recent review by Atkin et al 13 provides detailed information on the measurement of sedentary behavior in epidemiological studies. Sitting is a common characteristic of sedentary behavior and television viewing is among the most common leisure time sedentary behaviors. Given the latter, self-reported television viewing is frequently used as a measure of sedentary behavior in epidemiological studies. However, studies have also used total time spent in front of electronic screens as a measure of sedentary behavior (eg, sum of time spent watching television, playing video games, and using a computer). Hours per day and hours per week of screen-based sedentary behavior were modeled in some studies14,15 whereas other studies categorized participant into specific screen time groups (eg, [≤2 or >2 h/d], [<1, 1-3, or 3-6 h/d], [<2, 2-4, or >4 h/d]).16-18 Other less common self-reported measures of sedentary behavior used in the studies reviewed include reading, talking on the phone, doing homework, and time spent in motorized transport.19-21
Accelerometers measure total time spent in sedentary behavior, and this objective approach is advantageous, especially for children, as participants are not required to recall their past behavior. There are protocols in place to determine valid accelerometer data, however, protocols do vary between studies (number of days required [minimum of 3 or 4 days]; wear time per day [minimum of 8 or 10 hours per day]; and consecutive zero counts that constitutes non-wear [10 minutes of consecutive zeros or 60 minutes of consecutive zeros]). All studies included in this review used ActiGraph accelerometer models (AM7164 and GTM1), and most studies used a cutpoint of <100 counts per minute (cpm) to define sedentary behavior; other cutpoints used were <200 cpm, <500 cpm, and <1100 cpm.22-25 The choice of accelerometer protocol and the sedentary behavior cutpoint used may influence the association with health outcomes in youth. 26
Tables
The summary tables in this review are organized by health outcome: obesity (Table 1), blood pressure (Table 2), lipids (Table 3), insulin sensitivity (Table 4), clustered metabolic risk (Table 5), fitness (Table 6), and other health outcomes (Table 7). Within each table, the studies are organized by the name of the first author (A-Z), study year (2008-2012), study design (cross sectional [C.S.], case-control [C-C], longitudinal [L], or randomized controlled trial [RCT]), and by measure of sedentary behavior (self-report or accelerometry). Each table has a column that states if there was an association between sedentary behavior and the health outcome (negative, null, or positive); and each table has columns that state if the association remained after adjusting for MVPA, dietary intake, sleep duration, and when appropriate obesity. If any of these covariates were not included in a study, not applicable (N/A) was used to highlight the absence.
Sedentary Behavior and Obesity in Youth.
Abbreviations: Adj, adjusted; BMI, body mass index; C.S., cross-sectional; cpm, counts per minute; DXA, dual-energy X-ray absorptiometry; FM, fat mass; HC, hip circumference; IOTF, International Obesity Task Force; L, longitudinal; N/A, not applicable; PA, physical activity; pctl, percentile; RCT, randomized controlled trial; Slp, sleep; TV, television; WC, waist circumference; WHO, World Health Organization.
Association between sedentary behavior and measures of obesity after adjusting for physical activity, dietary intake, sleep, and obesity.
Modify, interaction between moderate-to-vigorous physical activity and sedentary behavior.
Sedentary Behavior and Blood Pressure in Youth.
Abbreviations: Adj, adjusted; C.S., cross-sectional; cpm, counts per minute; DBP, diastolic blood pressure; L, longitudinal; N/A, not applicable; PA, physical activity; Ob, obesity; pctl, percentile; SBP, systolic blood pressure; Slp, sleep; TV, television.
Association between sedentary behavior and blood pressure after adjusting for physical activity, dietary intake, sleep, and obesity.
Sedentary Behavior and Lipids in Youth.
Abbreviations: Adj, adjusted; C.S., cross-sectional; cpm, counts per minute; HDL-C, high-density lipoprotein cholesterol; L, longitudinal; LDL-C, low-density lipoprotein cholesterol; N/A, not applicable; Ob, obesity; PA, physical activity; Slp, sleep; TV, television.
Association between sedentary behavior and blood lipids after adjusting for physical activity, dietary intake, sleep, and obesity.
Sedentary Behavior and Insulin Sensitivity in Youth.
Abbreviations: Adj, adjusted; C.S., cross-sectional; cpm, counts per minute; HOMA-IR, Homeostatic Model Assessment for Insulin Resistance; N/A, not applicable; Ob, obesity; PA, physical activity; Slp, sleep; TV, television.
Association between sedentary behavior and insulin sensitivity after adjusting for physical activity, dietary intake, sleep, and obesity.
Sedentary Behavior and Clustered Metabolic Risk in Youth.
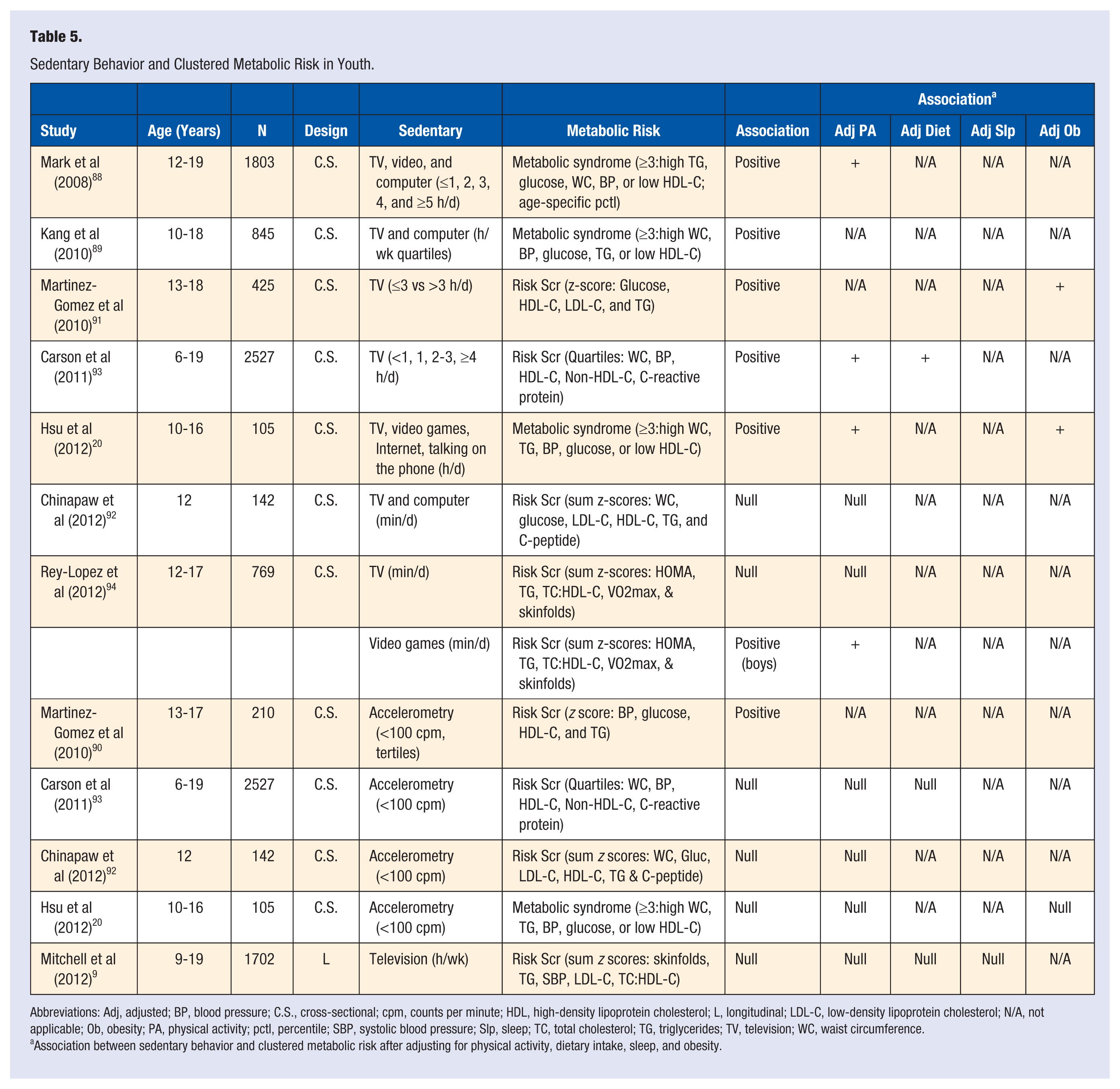
Abbreviations: Adj, adjusted; BP, blood pressure; C.S., cross-sectional; cpm, counts per minute; HDL, high-density lipoprotein cholesterol; L, longitudinal; LDL-C, low-density lipoprotein cholesterol; N/A, not applicable; Ob, obesity; PA, physical activity; pctl, percentile; SBP, systolic blood pressure; Slp, sleep; TC, total cholesterol; TG, triglycerides; TV, television; WC, waist circumference.
Association between sedentary behavior and clustered metabolic risk after adjusting for physical activity, dietary intake, sleep, and obesity.
Sedentary behavior and fitness in youth.
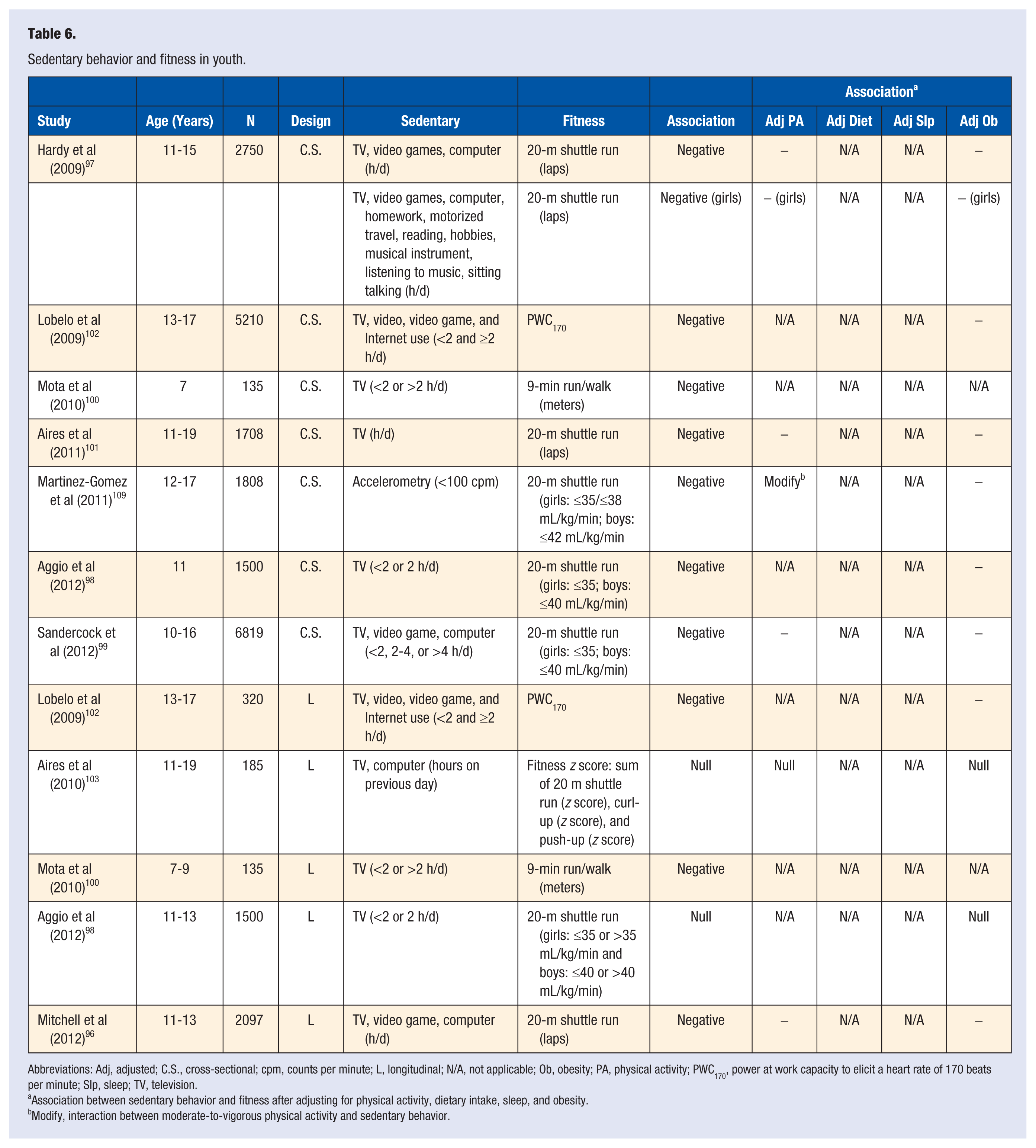
Abbreviations: Adj, adjusted; C.S., cross-sectional; cpm, counts per minute; L, longitudinal; N/A, not applicable; Ob, obesity; PA, physical activity; PWC170, power at work capacity to elicit a heart rate of 170 beats per minute; Slp, sleep; TV, television.
Association between sedentary behavior and fitness after adjusting for physical activity, dietary intake, sleep, and obesity.
Modify, interaction between moderate-to-vigorous physical activity and sedentary behavior.
Sedentary Behavior and Health Outcomes in Youth.
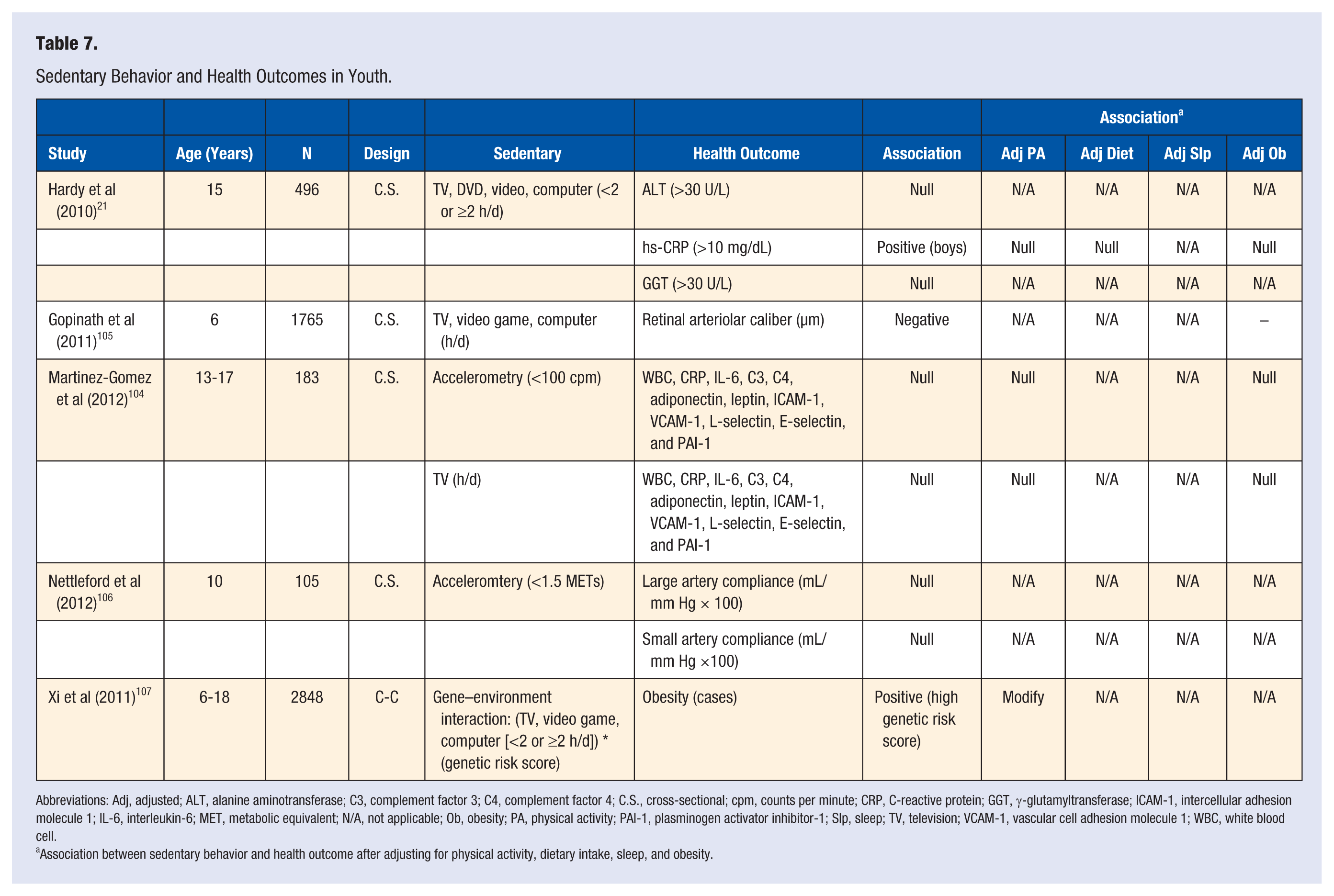
Abbreviations: Adj, adjusted; ALT, alanine aminotransferase; C3, complement factor 3; C4, complement factor 4; C.S., cross-sectional; cpm, counts per minute; CRP, C-reactive protein; GGT, γ-glutamyltransferase; ICAM-1, intercellular adhesion molecule 1; IL-6, interleukin-6; MET, metabolic equivalent; N/A, not applicable; Ob, obesity; PA, physical activity; PAI-1, plasminogen activator inhibitor-1; Slp, sleep; TV, television; VCAM-1, vascular cell adhesion molecule 1; WBC, white blood cell.
Association between sedentary behavior and health outcome after adjusting for physical activity, dietary intake, sleep, and obesity.
Obesity Outcomes
The prevalence of childhood obesity in the United States is 17%. 27 This estimate is based on the proportion of youth with a body mass index (BMI) ≥95th Centers for Disease Control and Prevention growth chart percentile, 28 and a number of studies included in this review used this cutoff to define obesity.16,29-33 However, most studies included used the International Obesity Task Force cutoff 34 to define obesity,15,18,19,35-48 and 2 studies used the World Health Organization reference data to define obesity.17,49 Some studies did not specifically define obesity based on BMI, but defined overweight using Centers for Disease Control and Prevention growth chart data (≥85th BMI percentile).50-58 Electing not to categorize participants into BMI groups, several studies modeled the mean BMI (raw BMI, BMI z score, or BMI percentile),24,59-73 or the median BMI and other percentiles of the BMI distribution.10,74,75
Several studies included in this review measured waist circumference to provide an estimate of abdominal fat mass*; some measured skinfold thickness to provide an estimate of subcutaneous fat mass, or converted skinfold thickness into percent body fat using prediction equations.9,19,38,43,54,60,72 Fat mass was also measured using bioelectrical impedance, densitometry, and dual energy X-ray absorptiometry.22,24,33,67,73,76,77,80,81
Blood Pressure Outcomes
Automated25,78,82 and mercury sphygmomanometers83-85 were used to measure diastolic blood pressure (DBP), mean arterial blood pressure (MABP), and systolic blood pressure (SBP) in studies included in this review. Blood pressure measurements were taken after a period of rest that ranged from 4 minutes 85 to 15 minutes. 83 All blood pressures were expressed in millimeters of mercury (mm Hg). The mean, or median, mm Hg was modeled for each blood pressure measure, except in 3 studies that categorized participants into high and low DBP and SBP groups.21,56,83
Lipid Outcomes
Enzymatic methods (high-density lipoprotein cholesterol [HDL-C], total cholesterol [TC], and triglycerides [TG]) and the Friedwald equation (low-density lipoprotein cholesterol [LDL-C]) were used to measure lipid levels in fasting blood in studies included in this review.9,21,56,78,85 Each lipid was expressed in milligrams per deciliter (mg/dL); and the mean, or median, mg/dL was modeled in each study, except in 2 studies that categorized participants in high and low groups (HDL-C, ≤35 mg/dL or >35 mg/dL; LDL-C, ≤130 mg/dL or >130 mg/dL; TG, ≤130 mg/dL or >130 mg/dL).21,56
Insulin Sensitivity
Insulin sensitivity refers to the degree to which the body responds to circulating insulin. Type 2 diabetics are insulin resistant and one study determined if sedentary behavior differed between type 2 diabetic cases and healthy controls. 86 Three studies estimated insulin sensitivity using the Homeostasis Model for Assessment for Insulin Resistance (HOMA-IR) calculation (HOMA-IR = [fasting glucose × fasting insulin]/22.5).21,23,87 One study performed oral glucose tolerance tests (OGTT), where participants received an oral glucose load (1.75 g/kg), after an overnight fast, and blood was sampled at 30, 60, 90, and 120 minutes after the glucose administration. 87 The Matsuda Index was then calculated to provide a measure of insulin sensitivity (Matsuda Index = 10000/√[(fasting glucose × fasting insulin) × (mean OGTT glucose × mean OGTT insulin)]). 87
Clustered Metabolic Risk
Metabolic syndrome and clustered metabolic risk scores provide an estimate of overall metabolic risk, and 3 studies included in this review investigated metabolic syndrome,20,88,89 and 6 studies investigated clustered metabolic risk scores.9,90-94 For metabolic syndrome, participants were categorized as having metabolic syndrome if at least 3 metabolic risk factors were defined as being high.20,88,89 In those studies, different metabolic risk factors were considered in the definition; and different cutoffs to define high levels of the individual metabolic risk factors were used across studies.20,88,89 For clustered metabolic risk scores, participants are not categorized as having, or not having, metabolic syndrome. Rather, z scores are calculated for the individual metabolic risk factors and the metabolic risk score is the sum of those z scores.9,90-94 However, not all studies included in this review used the same individual metabolic risk factors to calculate clustered metabolic risk scores.
Fitness Outcomes
Submaximal field tests have been established that allow for the measurement of cardiorespiratory fitness (CRF) in epidemiological studies. 95 Five studies included in this review estimated CRF using the 20-m shuttle run field test, where participants completed 20-m laps at an initial pace of 8.5 km/h, with the pace increasing by 0.5 km/h every minute thereafter, and the more laps completed indicates higher CRF.96-101 Using stationary cycles, one study determined the power needed to elicit a heart rate of 170 beats per minute (power at work capacity to elicit a heart rate of 170 beat per minute, PWC170). Greater power needed to achieve a heart rate of 170 beats per minute indicates higher CRF. 102 The 9-minute walk/run test was used in one study to estimate CRF; the more meters covered over 9 minutes indicates higher CRF. 100 One study measured both CRF (20-m shuttle run) and muscular strength (number of push-ups and curl-ups), and created an overall fitness z score. 103
Other Health Outcomes
The associations between sedentary behavior and adipokines, 104 markers of inflammation, 104 markers of nonalcoholic fatty liver disease, 21 retinal vasculature health, 105 and arterial stiffness 106 were investigated in studies included in this review. These health outcomes have not been extensively studied, at this time, and so are listed together under “other health outcomes” for the purpose of this review. One study determined if there was an interaction between obesity susceptibility loci and sedentary behavior with regard to obesity, 107 and this study was also listed under “other health outcomes.”
Results
Sedentary and Obesity (Table 1)
Forty-three cross-sectional studies investigated the association between self-reported sedentary behavior and measures of obesity. Null associations were reported between screen-based sedentary behavior and BMI in 10 studies; † skinfolds in 2 studies;38,61 and waist circumference (WC) in 3 studies.41,62,65 Screen-based sedentary behavior was associated with higher BMI in 33 studies, ‡ thicker skinfolds in 4 studies;19,43,54,60 larger WC in 5 studies;38,43,45,56,79 and higher fat mass in 1 study. 80 Of the 33 studies that found an association between sedentary behavior and higher BMI, 16 adjusted for MVPA, and the associations remained in 15 of those studies. § Of the 4 studies that found an association between sedentary behavior and thicker skinfolds, 3 adjusted for MVPA and the associations remained in all 3 studies.19,43,60 Of the 5 studies that found an association between sedentary behavior and larger WC, 4 adjusted for MVPA and the associations remained in all 4 of those studies.43,45,56,79 Six studies tested if MVPA modified the association between screen-based sedentary behavior and increased BMI.31,35,36,53,63 In those studies, screen-based sedentary behavior was associated with increased BMI only when MVPA was low.31,35,36,53,58,63 In the studies that also adjusted for dietary intakes and/or sleep duration, the cross-sectional associations between screen-based sedentary behavior and BMI and WC remained.14,18,42,44-47,50,60
Seven cross-sectional studies investigated the association between objectively measured sedentary behavior and measures of obesity.22,65,67,76-78,81 Null associations were reported between objectively measured sedentary behavior and BMI in 2 studies;65,76 WC in 3 studies;65,77,78 and fat mass in 2 studies. 78 , 81 Objectively measured sedentary behavior was associated with higher BMI in 1 study, 67 larger WC in 1 study, 76 and higher fat mass in 3 studies.22,67,76 Interestingly, the positive associations between objectively measured sedentary behavior and the measures of obesity became null in the 2 studies that adjusted for MVPA.22,76 The cross-sectional associations between objectively measured sedentary behavior and measures of obesity remained in those studies that adjusted for dietary intake and/or sleep duration.22,76,77,81
Eight longitudinal studies investigated the association between screen-based sedentary behavior and measures of obesity over time.9,10,32,68-72 Null associations between screen-based sedentary behavior and changes in WC, and changes in hip circumference, were reported by Altenberg et al. 72 Screen-based sedentary behavior was associated with greater increases in BMI over time in 6 studies,10,32,68-72 and greater increases in skinfold thickness over time in 2 studies.9,72 Those positive associations remained in 4 longitudinal studies that adjusted for MVPA;9,10,70,71 and those positive associations also remained in 3 longitudinal studies that adjusting for dietary intake and/or sleep duration.9,10,70
Four longitudinal studies investigated the association between objectively measured sedentary behavior and measures of obesity.24,33,73,74 Null associations were reported between objectively measured sedentary behavior and change in BMI in three studies;24,33,73 whereas Mitchell et al 74 reported an association between more objectively measured sedentary behavior and greater increases in BMI from age 9 to 15 years. The positive association in the latter study remained after adjusting for MVPA, dietary intake and sleep duration. 74 Fisher et al 73 reported null associations between objectively measured sedentary behavior and changes in fat mass and waist circumference over time; and Treuth et al 33 reported a null association between objectively measured sedentary behavior and change in percentage fat mass over time. Interestingly, Basterfield et al 24 reported a positive association between objectively measured sedentary behavior and fat mass over time, but that association became null after adjusting for MVPA.
One randomized controlled trial delivered a television reduction intervention, and found that those assigned to the intervention arm had lower BMI z scores compared to the control group at 6 months and 24 months after the start of the intervention. 108 Interestingly, the reduction in television viewing in the intervention group coincided with a reduction in caloric intake. 108
Sedentary Behavior and Blood Pressure (Table 2)
Eight cross-sectional studies investigated the association between screen-based sedentary behavior and blood pressure in youth.21,25,56,62,82-85 Null associations were reported between screen-based sedentary behavior and DBP in 6 studies21,56,62,83-85 and SBP in 4 studies.21,56,83,85 Three studies observed that more screen-based sedentary behavior was associated with increased SBP,62,82,84 and the association remained in one of those studies after adjusting for MVPA. 62 Gopinath et al 82 observed that more screen-based sedentary behavior was associated with higher DBP, and MABP, and those associations remained after adjusting for MVPA and obesity. Interestingly, Gopinath et al 82 also measured time spent reading and observed that more reading was associated with lower SBP, DBP, and MABP; and these associations remained after adjusting for MVPA and obesity.
Ekelund et al 78 objectively measured sedentary behavior and observed a null association between sedentary behavior and SBP. In contrast, Gaya et al 25 observed an increase in SBP with more objectively measured sedentary behavior, and the association remained after adjusting for BMI. Mitchell et al 9 investigated the longitudinal association between television viewing and changes in SBP over time, and observed a null association.
Sedentary Behavior and Lipids (Table 3)
Three cross-sectional studies investigated the association between screen-based sedentary behavior and total cholesterol, LDL-C, HDL-C, and TG.21,56,85 Null associations were observed in all 3 studies,21,56,85 expect for a negative association reported between screen-based sedentary behavior and HDL-C by Byun et al, 56 which remained after adjusting for MVPA.
Ekelund et al 78 investigated the cross-sectional association between objectively measured sedentary behavior and HDL-C and TG, and in that study null associations were observed. Mitchell et al 9 investigated the longitudinal association between television viewing and changes in LDL-C, HDL-C, and TG over time, and observed null associations for each lipid.
Sedentary Behavior and Insulin Sensitivity (Table 4)
Two cross-sectional studies observed associations between more screen-based sedentary behavior and fasting insulin and HOMA-IR.21,87 Henderson et al 87 also observed that more screen-based sedentary behavior was associated with Matsuda Index. The positive associations reported by Henderson et al 87 remained after adjusting for MVPA but became null after adjusting for obesity. The positive associations reported by Hardy et al. remained after adjusting for aerobic fitness, dietary intake, and obesity. 21
Henderson et al 87 observed cross-sectional associations between more objectively measured sedentary behavior and higher fasting insulin, HOMA-IR, and lower Matsuda Index. However, only the fasting insulin and HOMA-IR associations remained after adjusting for MVPA in that study; and only the fasting insulin association remained after adjusting for obesity. 87 Sardinha et al 23 observed a cross-sectional association between more objectively measured sedentary behavior and an increase in HOMA-IR. That association remained after adjusting for MVPA and obesity. 23 In contrast, Ekelund et al 78 reported a positive association between objectively measured sedentary behavior and fasting insulin, but that association was attenuated after adjusting for MVPA.
A case–control study by Lobelo et al 86 investigated if screen-based sedentary behavior was associated with T2DM. No difference in screen-based sedentary behavior was observed between type 2 diabetic cases and controls, and the null association remained after stratifying by obesity status. 86
Sedentary Behavior and Clustered Metabolic Risk (Table 5)
Three cross-sectional studies investigated the association between screen-based sedentary behavior and metabolic syndrome.20,88,89 In all 3 studies more screen-based sedentary behavior was associated with metabolic syndrome.20,88,89 Two of those studies adjusted for MVPA and the positive associations remained in both studies with that adjustment;20,88 and the association remained in the one study that adjusted for obesity. 20 Hsu et al 20 investigated the cross-sectional association between objectively measured sedentary behavior and metabolic syndrome. There was no association between objectively measured sedentary behavior and metabolic syndrome in that study. 20
Five cross-sectional studies investigated the association between screen-based sedentary behavior and metabolic risk scores.43,91-94 Two studies observed that more screen-based sedentary behavior was associated with higher metabolic risk scores.91,93 The positive association remained in one study that adjusted for MVPA and dietary intake 93 ; and remained in one study that adjusted for obesity. 91 Rey-Lopez et al 94 observed that more video game playing was associated with higher metabolic risk scores in boys, and this association remained after adjusting for MVPA; however, Rey-Lopez et al 94 reported null associations between television viewing and metabolic risk score in both boys and girls. Chinapaw et al 92 reported a null association between screen-based sedentary behavior and metabolic risk score.
Three cross-sectional studies investigated the association between objectively measured sedentary behavior and metabolic risk score.90,92,93 Martinez-Gomez et al 90 observed that more objectively measured sedentary behavior was associated with higher metabolic risk scores, but did not adjust for MVPA, dietary intake, sleep duration, or obesity. Null associations were observed between objectively measured sedentary behavior and metabolic risk scores in the remaining two studies.92,93 Mitchell et al 9 investigated the longitudinal association between television viewing and change in metabolic risk score over time, and observed a null association.
Sedentary Behavior and Fitness (Table 6)
Six cross-sectional studies investigated the association between screen-based sedentary behavior and CRF.97-102 In all 6 studies, more screen-based sedentary behavior was associated with lower CRF.97-102 The associations remained in all 6 studies after adjusting for obesity; 3 of the 6 studies adjusted for MVPA, and in those studies the negative association between screen-based sedentary behavior and lower CRF remained.97,99,101 Martinez-Gomez et al 109 observed a cross-sectional association between more objectively measured sedentary behavior and lower CRF, and that association remained after adjusting for obesity. Interestingly, MVPA modified that association, where more objectively measured sedentary behavior was associated with lower CRF when MVPA levels were low. 109
Five longitudinal studies investigated the association between screen-based sedentary behavior and CRF.96,98,100,102,103 Two observed no association between sedentary behavior and change in CRF over time.98,103 Three observed that more screen-based sedentary behavior predicted lower CRF over time.96,100,102 The association remained in 2 studies that adjusted for obesity,96,102 and in the one study that adjusted for MVPA. 96
Sedentary Behavior and Other Health Outcomes (Table 7)
Null associations were observed between sedentary behavior and adipokines; 104 markers of inflammation;21,104 markers of non-alcoholic fatty liver disease; 21 and arterial stiffness. 106 More sedentary behavior was cross-sectionally associated with arteriolar narrowing of the retinal microvasculature, and that association remained after adjusting for BMI. 105 Xi et al 107 observed a cross-sectional interaction between sedentary behavior and obesity-susceptibility loci. Specifically, more sedentary behavior was associated with increased BMI and the increase was greater among those genetically susceptible to obesity. 107
Discussion
Youth spend the majority of their waking hours in sedentary behavior and this may have health consequences. On reviewing the literature, we found evidence that too much sedentary behavior associated with obesity in youth. We found an indication that too much sedentary behavior associated with insulin sensitivity, and an indication that too much sedentary behavior associated with clustered metabolic risk. There was evidence that sedentary behavior was associated with lower CRF in youth; but there was little-to-no evidence that too much sedentary behavior associated with impaired lipid profiles and increased blood pressure in youth. Reasons to explain the associations observed in the studies reviewed are provided below, and possible future research directions are also discussed.
Sedentary Behavior and Obesity
Cross-sectional and longitudinal studies reported associations between sedentary behavior, especially screen-based sedentary behavior, and measures of obesity. The longitudinal findings are important as this indicates a temporal sequence, whereby time spent in sedentary could lead to increases in measures of obesity. A positive energy balance is thought to be the primary mechanism underlying the development of obesity, and spending too much time in sedentary behavior may facilitate a positive energy balance through a reduction in energy expenditure. In some studies the association between sedentary behavior and obesity remained after adjusting for MVPA. ‖ Those findings suggest that substituting sedentary behavior for light-intensity physical activity, to increase energy expenditure, could correct a positive energy balance and reduce the prevalence of obesity. However, in other studies MVPA modified the association between sedentary behavior and obesity,35,36,53,63,69 and in two cross-sectional studies that objectively measured sedentary behavior the association with obesity was attenuated after adjusting for MVPA.22,76 These findings suggest that youth with high levels of sedentary behavior should be encouraged to meet the physical activity guidelines, and that this could sufficiently increase energy expenditure to help correct a positive energy balance. While reduced energy expenditure during sedentary behavior appears to be plausible explanation for the observed associations with obesity, it is not known if specific sedentary behavior guidelines are needed beyond current physical activity guidelines to help prevent childhood obesity from an energy expenditure standpoint.
Spending too much time in sedentary behavior may also facilitate a positive energy balance through an increase in energy intake. Snacking while watching television and exposure to televised food advertisements are 2 mechanisms thought to encourage increased energy intake with more time spent in sedentary behavior. 5 Some studies adjusted for dietary intakes when investigating the association between sedentary behavior and obesity; however, in all of those studies the associations remained. ¶ These findings indicate that the association between sedentary behavior and obesity is not fully explained by increased dietary intakes. However, not all studies used the same measure of dietary intake, and more standardized adjusted for dietary intakes should be adopted in future studies that investigate the association between sedentary behavior and obesity.
Short sleep duration and disrupted circadian rhythms have been associated with obesity.110,111 It is possible that the association between sedentary behavior and obesity in youth is explained, in part, by a reduction in sleep duration that disrupts circadian rhythms. In support, children often watch television in the evening, 112 which potentially increases exposure to light at night and delays the onset of sleep. Few studies included in this review adjusted for sleep duration when investigating the association between sedentary behavior and obesity, and this adjustment should be considered in future studies.
Sedentary Behavior and Metabolic Risk
There was little-to-no evidence that sedentary behavior was associated with increased blood pressure and blood lipids in youth.9,21,56,62,78,82-85 Those findings are in contrast with findings among adults, where associations between sedentary behavior and blood pressure and blood lipids have been reported. 113 It is possible that exposure to high levels of sedentary behavior in youth is of too short a duration to be associated with blood pressure and blood lipids; and long-term exposure to sedentary behavior from childhood into adulthood may be necessary to impair these metabolic risk factors.114,115 It is also possible that sedentary behavior first associates with obesity, and then with hypertension and hyperlipidemia later in adulthood.
There was some cross-sectional evidence that too much sedentary behavior was associated with insulin sensitivity21,23,78,87 and clustered metabolic risk in youth.88-91,93 However, there is a lack of longitudinal studies that have investigated the association between sedentary behavior and insulin sensitivity and clustered metabolic risk, and this is needed to establish temporal precedence. Nonetheless, in some studies the cross-sectional associations between sedentary behavior and those metabolic risk factors remained after adjusting for MVPA.21,23,87,88,93 This indicates that substituting sedentary behavior for light intensity physical activity could improve insulin sensitivity and clustered metabolic risk. Also, in some studies the reported associations between sedentary behavior and insulin sensitivity remained after adjusting for obesity.21,23 This indicates that reducing sedentary behavior could improve insulin sensitivity, independent of changes in fat mass. Few studies adjusted for dietary intake when assessing the association between sedentary behavior and insulin sensitivity and clustered metabolic risk, 21 , 93 so it is not known if poor diet composition with more sedentary behavior explains the association between sedentary behavior and those metabolic risk factors. Also, only one study adjusted for sleep duration, 9 so it is not known if short sleep coinciding with more sedentary behavior explains the association between sedentary behavior and those metabolic risk factors.
Sedentary Behavior and Fitness
Cross-sectional and longitudinal studies reported associations between more sedentary behavior and lower CRF.97-102,109 Importantly, there is evidence that the association between sedentary behavior and lower CRF is independent of MVPA.96,97,99,101 These findings indicate that substituting sedentary behavior for light intensity physical activity could increase CRF levels. However, one study observed that MVPA modified the association between sedentary behavior and CRF, and this finding suggests that those with high levels of sedentary behavior should be encouraged to meet the physical activity guidelines to improve their CRF. 109 More research is needed to determine if specific sedentary behavior guidelines are needed beyond current physical activity guidelines to help improve CRF levels in youth.
Interestingly, the associations between sedentary behavior and lower CRF remained after adjusting for BMI.96-99,101,109 This means that reducing sedentary behavior could increase CRF levels, even if there is no change in BMI. This is important in terms of the fit-fat hypothesis, whereby maintaining moderate-to-high levels of CRF can improve health outcomes, even among those who are obese. 116
Future Research
Studies to date have typically assumed that all sedentary behaviors are equal; especially those that have used accelerometry to objectively measure sedentary behavior. However, certain sedentary behaviors may be more harmful to health than others. For example, Gopinath et al 82 and Sisson et al 55 both demonstrated that reading was not associated with the health outcome under investigation (blood pressure and obesity, respectively), whereas television viewing was associated with the health outcome under study (blood pressure and obesity, respectively). These findings suggest that not all sedentary behaviors are equal in terms of health effects. Although clusters of sedentary behavior have been described among youth, 117 it is not known if certain sedentary behavior patterns are more, or less, likely to be associated with health outcomes in youth. Also, as children age they tend to spend more time in prolonged periods of sedentary behavior, 6 , 7 and it has been shown in adults that more breaks in sedentary behavior are associated with improved metabolic risk profiles, independent of total sedentary behavior; 113 but only one study has investigated the association between breaks and metabolic risk in children and adolescents. 93 Furthermore, the timing of sedentary behavior may be important. Descriptive data among youth show that most television viewing occurs in the evening prior to going to bed, 112 and having a television in the bedroom has been associated with obesity, independent of total television viewing.47,79 It would be worth investigating the timing of sedentary behavior as evening sedentary behavior may have a role in short sleep and disrupted circadian rhythms.
To accommodate time spent in sedentary behavior, it is likely that less time is spent in light intensity physical activity.6,7 If a reduction in energy expenditure with more time spent in sedentary behavior explains, in part, the associations with obesity and lower aerobic fitness in youth, and perhaps impaired metabolic profiles, then substituting sedentary behavior for light intensity physical activity would be expected to improve health outcomes in youth. However, there are few studies that have investigated the health effects of light intensity physical activity. For example, Steele et al. found no association between light intensity physical activity and obesity in youth; and the association between sedentary behavior and obesity in that study became null after adjusting for MVPA. 76 These findings indicate that energy expended through higher intensity physical activity is more important for preventing obesity. However, there is some evidence in adults that light intensity physical activity can improve health outcomes,113,118 and more research in this area is needed, especially among youth.
Xi et al 107 found that screen-based sedentary behavior was associated with increased BMI, and that the association was strongest for those who were genetically susceptible to obesity. This finding provides evidence of a gene–environment interaction, and a similar finding has been reported in a sample of adults. 119 This is an area of research that could be explored further. We have studied the BMI distribution in several studies and a common pattern found was that sedentary behavior was associated with increases in BMI, and the increases were greater at the upper tail of the BMI distribution;10,74 and similar associations were observed by Beyerlein et al. 75 This may provide indirect evidence of a gene-environment interaction, as those at the upper tail of the BMI distribution are more likely to be genetically susceptible to obesity. 120 In addition to obesity, genes contribute to fitness levels and metabolic risk profiles.121,122 and future studies could also determine if gene–environment interactions exist for associations between sedentary behavior and those health outcomes.
Conclusion
Spending too much time in sedentary behavior, especially screen-based sedentary behavior, was associated with obesity and lower aerobic fitness in youth, and these associations were observed in both cross-sectional and longitudinal studies. More time spent in sedentary behavior was cross-sectionally associated with insulin sensitivity and clustered metabolic risk in youth; although, there are no longitudinal studies that support those cross-sectional findings. There was little-to-no evidence that sedentary behavior was associated with increased blood pressure and blood lipids in youth.
Footnotes
Acknowledgements
The author would like to thank Lorraine Dean and Kathleen Sturgeon for commenting on the content of an early draft of the article.
Funding
The author is supported by Award Number F32CA162847 from the National Cancer Institute. The content is solely the responsibility of the author and does not necessarily represent the official views of the National Cancer Institute or the National Institutes of Health.