
Abstract
Life events unique to the perinatal period may place a woman at greater risk for decreased physical activity and increased postpartum weight retention (PPWR). Study purposes were to determine a) the relationship between women’s postpartum self-efficacy (SE) to overcome perceived barriers to exercise with current and past pregnancy leisure-time physical activity (LTPA), and b) the relationship between LTPA and PPWR. A Modifiable Activity Questionnaire was used to assess current and past pregnancy LTPA (Met*h/wk) at 20 and 32 weeks gestation and 12 weeks postpartum. Current barriers to LTPA and SE were assessed via the Perceived Barriers Efficacy Questionnaire. Top three barrier values were averaged to obtain an overall SE score for participants (N=30). Pearson correlations were run between LTPA, PPWR and SE scores. ANOVA was used to compare PPWR between women who did and did not meet LTPA guidelines of 7.5 MET*h/wk. The top three barriers to LTPA were time, motivation, and childcare. Positive correlations (p≤0.01) were found between SE levels and LTPA at all time periods of interest. LTPA was inversely related to PPWR. Relationships between SE, LTPA, and PPWR helped validate the need to promote perinatal PA, to aid long term weight management.
‘During the postpartum period, women may initiate lifestyle changes with a renewed focus on weight loss.’
Introduction
Regular leisure time physical activity (LTPA) during the postpartum period has been associated with reduction in excessive weight gain/retention, improved aerobic fitness and insulin sensitivity, maintenance of bone mineral density, and enhanced psychological well-being.1,2 Moderate PA performed by healthy women during pregnancy has been shown to improve cardiovascular function, limit weight gain and retention, improve attitude and mental state, improve overall fitness, and decrease labor duration and complications.1,3 Because of its documented positive impact on health, LTPA is rarely contraindicated during healthy pregnancies and is usually beneficial for the maternal-fetal unit.1,3,4 PA does not appear to have adverse effects on breast milk volume and composition or infant growth.1,5 Therefore, the PA guidelines for Americans are 150 minutes of moderate-intensity PA per week (7.5 MET h/wk) for all pregnant women. 1
During the postpartum period, women may initiate lifestyle changes with a renewed focus on weight loss. Conversely, life events unique to pregnancy (eg, acute sickness, fatigue, and weight gain) and the postpartum period (eg, family obligations and child care) may place a woman at risk for decreased LTPA that may result in higher postpartum weight retention (PPWR). Weight retained from a pregnancy can remain indefinitely and may increase a woman’s risk of becoming overweight or obese.6-8
PA self-efficacy (SE) may influence a woman’s choice to engage in perinatal LTPA. SE is a person’s belief in his/her ability to succeed in tasks that occur in his/her life to obtain a specific outcome. 9 The strength of an individual woman’s SE for LTPA will determine what activities she will attempt, how much effort she will expend, and how well she will persist in her quest to adopt a physically active lifestyle. 10
Barrier efficacy involves a person’s belief in his/her ability to overcome barriers that inhibit participation in certain aspects of his/her life. 11 Investigators who have focused on barriers have demonstrated this form of efficacy to be consistent with the prediction of exercise behavior. 10
Because pregnancy and the postpartum period are times of marked lifestyle changes, it is important to bolster a woman’s PA SE during these critical time points. Perceived barriers may influence a woman’s LTPA intentions as well as participation. 12 Determining barriers that might be most important and how a woman deals with them could assist researchers and PA specialists with the creation of appropriate intervention programs for the perinatal period and beyond, where PPWR is of great concern. In addition, determining whether LTPA during pregnancy may also influence future intentions and a woman’s PA participation after childbirth may be important to intervention success.
The purposes of this study were to determine (a) the relationship between postpartum SE to overcome perceived barriers to exercise and current and past-pregnancy LTPA and (b) the relationship between LTPA and PPWR.
Materials and Methods
Our sample was taken from 56 women who participated in a study designed to determine the reliability and validity of 3 commonly used LTPA measurement modalities during pregnancy.13,14 Six years postpartum, participants were contacted to participate in the current study. Permission to recontact the women had been obtained as part of the original consent process. We used e-mail, telephone calls, and letters to contact 41 of the original 56 participants believed to still live in the area. In all, 31 women were located and contacted. All but 1 agreed to participate.
All measures were collected in the Human Energy Research Laboratory at Michigan State University. A stadiometer was used to measure participant height to the nearest 0.1 cm. A beam balance was used to measure participant weight to the nearest 0.1 kg. Current body mass index (BMI) was calculated from height and weight measures (kg m−2). PPWR was calculated in 2 ways. First, estimated prepregnancy weight (recalled at follow-up) was subtracted from current measured weight (PPWR-1). Second, weight at 20 weeks of gestation (measured as part of the original study) was subtracted from current measured weight (PPWR-2).
A Perceived Barriers Efficacy Questionnaire (PBEQ), an open-ended survey, was used to assess current barriers to LTPA and the participant’s sense of SE to overcome them. 15 The PBEQ used an individual approach to assess barrier efficacy. 16 Participants were first required to list their own perceived barriers to current PA behavior. Each was then asked to assign an efficacy rating for overcoming each barrier. Efficacy ratings ranged from 0% to 100% confidence, in 10-unit intervals, with 0 meaning no confidence and 100 meaning total confidence in overcoming a chosen barrier. 10 After an efficacy rating was provided for each barrier listed by the participant, her top 3 were ranked from first (meaning most) to third (meaning least) important barrier. A total barrier efficacy score was then calculated for each participant by averaging the scores of the top 3 ranked barriers, then converted to a total percentage efficacy score ranging from 0% to 100%. Because of the open-ended format of the PBEQ as well as the fact that each participant was queried for her individual perceived barriers, participant A’s top 3 barriers may differ from participant B’s and so on.
The women used the Modifiable Activity Questionnaire (MAQ) to recall current LTPA behavior as well as activity performed during their original study pregnancy that occurred 6 years earlier. The MAQ is a recall questionnaire designed for easy modification to maximize a researcher’s ability to assess PA in different populations.17,18 This questionnaire has been used to assess historical as well as recent (eg, past week) PA levels. The MAQ can be designed to collect information regarding mode, intensity, duration, and frequency of both leisure-time and occupational activity. The MAQ was shown recently to be a valid tool for assessing recent (last week) LTPA as well as PA performed at 20 weeks and 32 weeks of gestation and 12 weeks postpartum during a pregnancy 6 years earlier. 19
For each time period of interest, participants were asked to circle all activities (from a predetermined list generated from pilot studies) in which they had participated during leisure time. Frequencies, in days per week, and duration, in hours per bout, were established for each chosen activity. PA duration values ranged from 0 to >1 hour. Minutes of PA were converted to values in hours (30 minutes = 0.5 hours). MET values for all listed activities were determined using the compendium for physical activities developed by Ainsworth et al. 20 Energy expenditure during LTPA was quantified as MET h/wk for each time period of interest (20 and 32 weeks of gestation, 12 weeks postpartum, and current).
Because percentage barrier efficacy scores were not normally distributed, a median split was used to group women with low, versus high efficacy in overcoming their perceived barriers to performing LTPA. A 2 (efficacy condition) × 5 (time periods) ANOVA was utilized to determine whether LTPA before pregnancy, at 20 and 32 weeks of gestation, at 12 weeks postpartum, and currently differed according to percentage efficacy scores. ANOVA was also used to determine whether PPWR-1 and PPWR-2 differed according to women’s percentage efficacy. Finally, Pearson correlation coefficients were used to analyze the relationships between LTPA at each time point and both indices of PPWR. A 2-sided α level of P < .05 was used to determine statistical significance.
Results
Participants’ descriptive characteristics were as follows: mean age = 36.2 ± 5.0 years, height = 165.9 ± 6.9 cm, and current BMI = 23.7 ± 4.2. A total of 25 (80%) of the 30 study participants were primiparous when part of the original study. Average PPWR values were 2.7 ± 5.2 kg (PPWR-1) and −2.0 ± 5.0 kg (PPWR-2).
Results of all frequencies for all listed barriers to exercise are displayed in Table 1. The top 3 barriers, with subsequent frequencies were as follows: the most common barrier listed by the participants was time (22), followed by motivation (7), and then child care (6). The average participant percentage efficacy score was 65.6% (±24.5), whereas the median score was 74.1%.
Listed Current Barriers to Physical Activity in Rank Order.
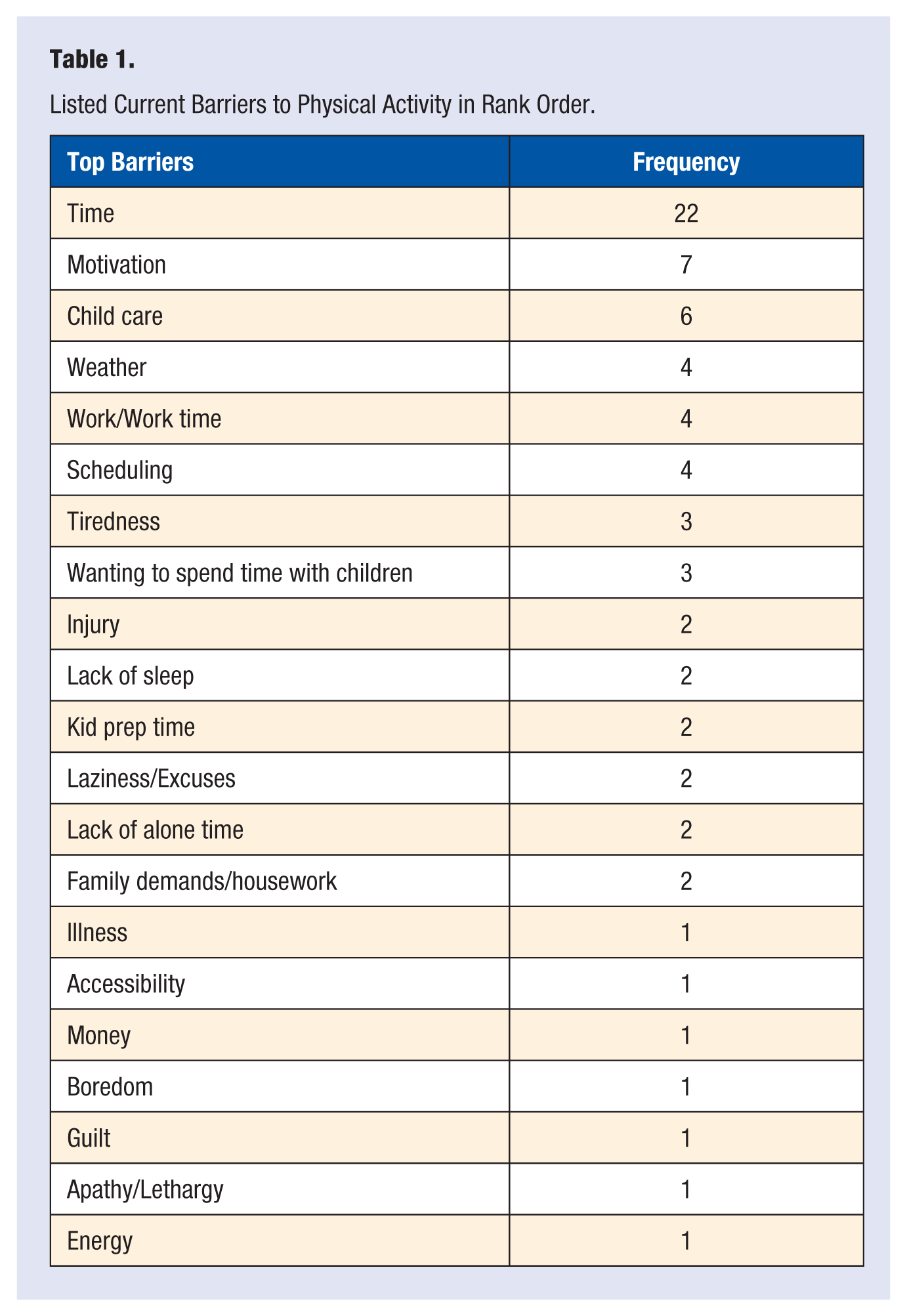
Table 2 shows LTPA at all time points as a function of efficacy groups. Results showed LTPA to be significantly greater (F = 8.09; P < .008) in women classified as having high efficacy in their ability to overcome perceived barriers to PA at all time points. Moreover, women with high efficacy were more likely to perform LTPA at or above recommended minimum levels. Likewise, women in the high-efficacy groups were more likely to have less PPWR (PPWR-1: F = 7.83, P < .009; PPWR-2: F = 10.97, P < .002) than those classified as having low efficacy (Table 3).
LTPA During and After Pregnancy According to Percentage Efficacy Classification.
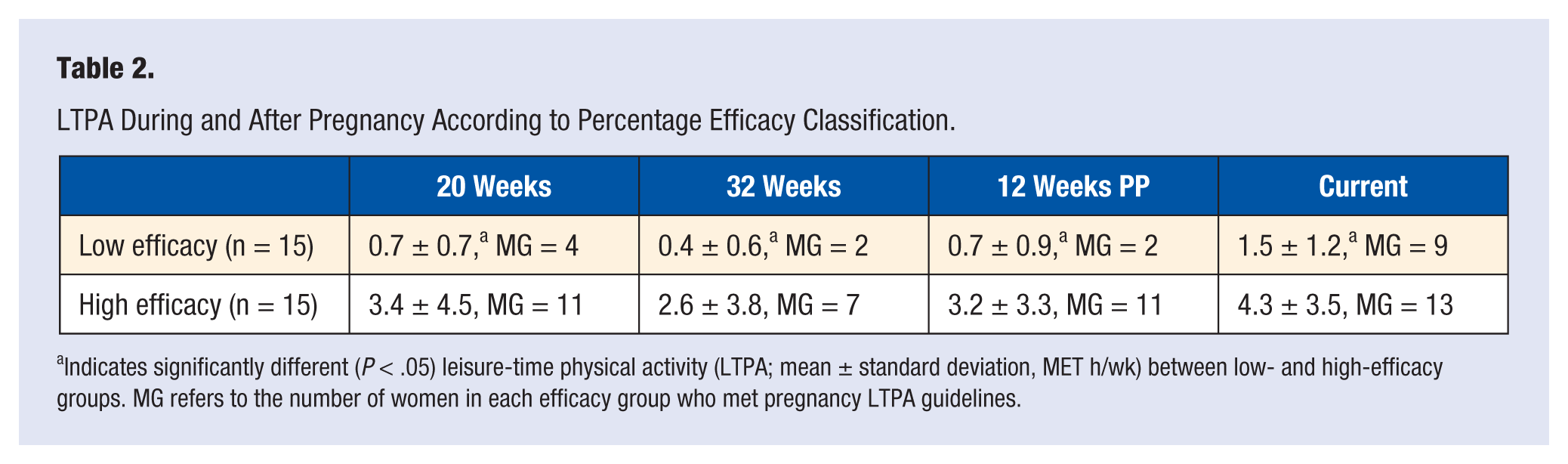
Indicates significantly different (P < .05) leisure-time physical activity (LTPA; mean ± standard deviation, MET h/wk) between low- and high-efficacy groups. MG refers to the number of women in each efficacy group who met pregnancy LTPA guidelines.
PPWR According to Percentage Efficacy Classification.
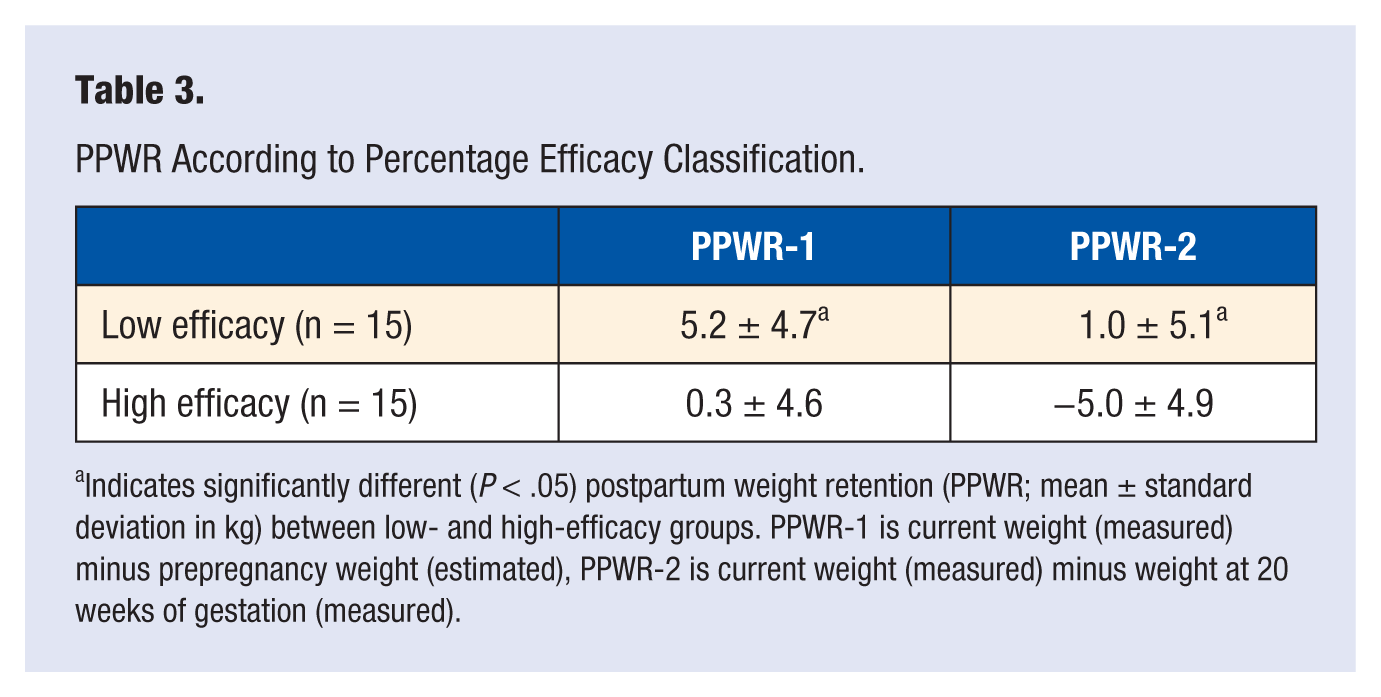
Indicates significantly different (P < .05) postpartum weight retention (PPWR; mean ± standard deviation in kg) between low- and high-efficacy groups. PPWR-1 is current weight (measured) minus prepregnancy weight (estimated), PPWR-2 is current weight (measured) minus weight at 20 weeks of gestation (measured).
Results of Pearson correlations showed that PPWR was significantly and inversely related (P < .05) to pregnancy, postpartum, and current LTPA values (Table 4). Significant correlations were moderate or greater, ranging from r = −0.42 to −0.62 during pregnancy and after delivery.
Correlations (r) Between LTPA and PPWR During and After Pregnancy (n = 30).
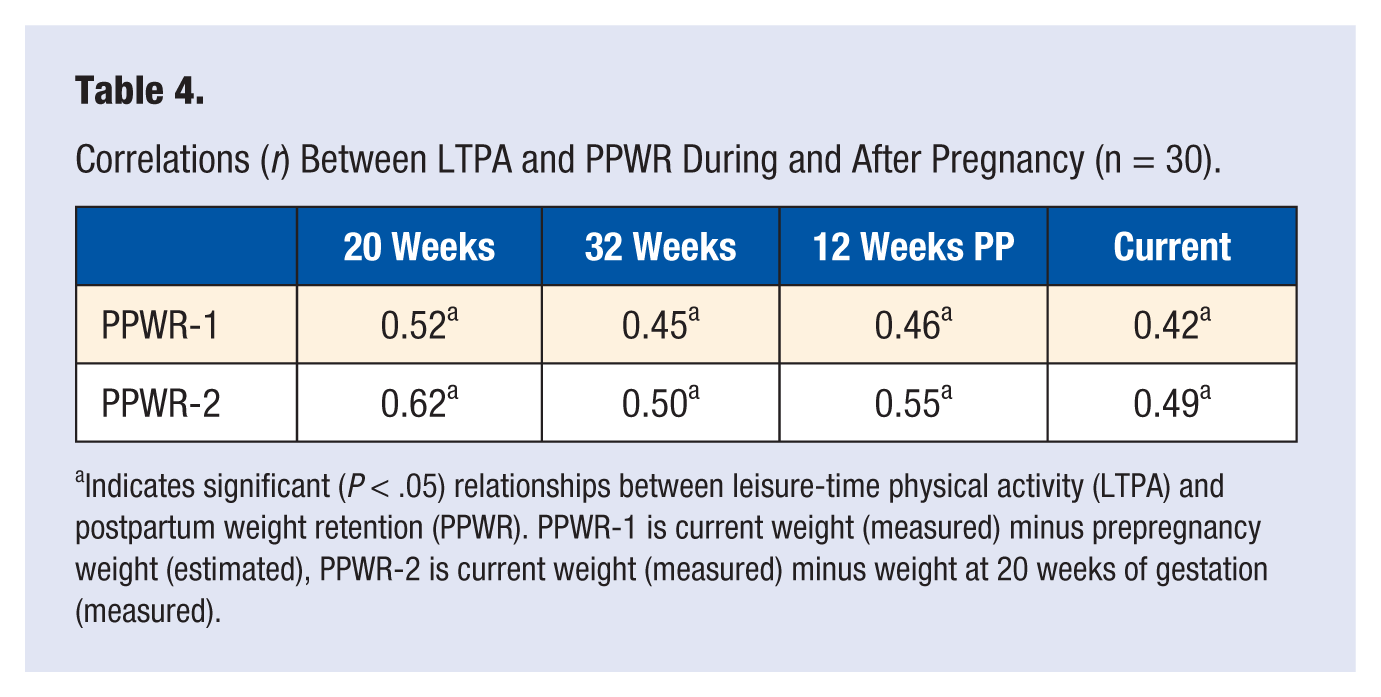
Indicates significant (P < .05) relationships between leisure-time physical activity (LTPA) and postpartum weight retention (PPWR). PPWR-1 is current weight (measured) minus prepregnancy weight (estimated), PPWR-2 is current weight (measured) minus weight at 20 weeks of gestation (measured).
Discussion
The purposes of this study were to determine the relationship between a woman’s SE to overcome perceived barriers to LTPA during pregnancy and to relate her activity levels to PPWR, which is a unique contribution of this investigation. For the sample overall, PPWR averaged 2.7 kg (±5.2 kg), ranging from −8.4 to 14.9 kg. The mean PPWR in this sample is higher than that found in other studies (0.9 and 1.51 kg); the range is similar to that found in 1 similar study (−12.5 to 26.5 kg). 21 We used 2 values as proxies for PPWR to ensure that the outcomes would be true representations of PPWR and other factors associated with the perinatal period. The first value was estimated using recalled prepregnancy weight values and current postpartum weight, whereas the second value used measured weight at 20 weeks of gestation as a surrogate for prepregnancy weight. The fact that both estimates led to similar results adds to the validity of our findings.
Barriers to LTPA found in this study are displayed in Table 1. Lack of time was the top barrier in this investigation, which was similar to others’ findings and showed much higher frequencies than any other barrier listed. Top barriers listed in this study (lack of time, motivation, and child care) are similar to those found by other investigators.15,22-24
The survey tools used in this investigation (MAQ and PBEQ) have been used and validated in previous studies, giving credibility to both LTPA and percentage confidence data.15,19 Cramp and Bray 22 also used the MAQ to assess recalled PA to study exercise SE and barriers to LPTA among postnatal women. The Cramp and Bray study was, in total, much larger than this investigation, but at the only time point shared by both studies (12 weeks postpartum), participant numbers were similar to ours (n = 31).
Participants in the Beilock et al 15 study were former athletes who were asked to list barriers to training for competition during the postpartum period, whereas we queried our participants about barriers to LTPA in general and not for competition. Though a few participants in the present investigation may have competed from time to time in road races, a majority of the sample was not overly competitive. Unlike the current investigation, Beilock et al did not assess percentage efficacy in overcoming barriers to LTPA; therefore, direct comparison of the 2 studies is not possible.
In 2004, Downs and Hausenblas 23 investigated women’s beliefs and behaviors during pregnancy and postpartum. The investigators’ main findings were that women believed that LTPA during pregnancy can improve mood and that physical discomfort obstructed pregnancy LTPA; the women also believed that postpartum LTPA controlled weight gain. Downs and Hausenblas concluded that spouse/family support was most influential on LTPA during pregnancy and in the postpartum period and that women exercised more before they were pregnant than during pregnancy and postpartum. The goals of that investigation and this one were similar, but different measurement tools for LTPA and SE were used. Because Downs and Hausenblas used different measurement tools and they did not compare efficacy in participating in LTPA with current or recalled LTPA values, direct comparison with our results is not possible.
We found no studies that compared both actual and recalled LTPA with current barriers to PA. However, Godin et al 25 investigated the factors influencing intentions of pregnant women to exercise after giving birth. Their results showed that intention to exercise was strongly correlated with attitude toward the act, exercise habit, and perceived barriers to exercise.
The finding that LTPA during pregnancy and the postpartum period was inversely related to a woman’s PPWR is encouraging and supported by previous research. 26 Even with the benefits associated with perinatal LTPA, research has shown that it is a time (especially the postpartum period) of decreased LTPA.27-29 Lifestyle changes associated with parenthood have been shown to be the main predictors of postpartum LTPA.26,28,29 Results of this investigation confirm that barriers to perinatal LTPA are consistent, giving health care providers and fitness professionals valid information from which to help pregnant and postpartum women remain active during the perinatal period. In addition, it is reassuring to know that women who reported the highest efficacy for overcoming barriers were more likely to perform recommended levels of LTPA during pregnancy and the postpartum period.
Studies have shown that most women visit their health care provider regularly during pregnancy, but the clinician was not the person with the most influence regarding LTPA, even though they have the opportunity to provide PA counseling and support. 23 In conjunction, a study investigating health care provider knowledge, beliefs, and practices toward pregnancy LTPA concluded that even though most of the beliefs were positive, not all the clinicians were aware of or followed current LTPA guidelines. 30 A renewed focus of health care providers on perinatal LTPA and an enhanced symbiotic relationship with knowledgeable local fitness professionals using the Exercise is Medicine program offered by the American College of Sports Medicine or other referral mechanisms could positively affect perinatal as well as long-term maternal health.
Limitations of this longitudinal study include the small sample size and homogeneous participant population as well as self-reported recall by study participants, all of which may explain some of the discrepancies between our outcomes and those of other studies. Study designs and measurement of PA and barriers also differed, which may explain some of the discrepant findings.
Conclusions
This investigation showed that most women will retain weight during the postpartum period, but women who were active within the current recommended LTPA guidelines retained less weight 6 years postpartum than those who were not. In addition, this follow-up also showed a relationship between past-pregnancy PA and PPWR. We conclude, therefore, that LTPA during pregnancy and the postpartum period may help decrease long-term weight retention related to pregnancy. The existence of this relationship could greatly add to the value of promoting recommended amounts of PA during pregnancy. Long-term weight management may be aided if women remain, or become, physically active during pregnancy and in the postpartum period. Health care providers and fitness professionals need to be aware of current LTPA guidelines as well as the common barriers to perinatal LTPA in order pass on proper information to their patients and clients.
Footnotes
Acknowledgements
The authors would like to acknowledge the study participants for their cooperation with this study.
Authors’ Note
This article was presented at the American College of Sports Medicine national meeting in 2008.