
Abstract
Integrating effective health behavior change discussions in childhood preventative medical visits is a challenging and important means to support families in the creation and maintenance of healthy habits over the lifespan. The 9-5-2-1-0 model is a tool to identify healthy habits and guide conversation at well-child visits in primary care. Diverse families in a family medicine residency clinic met with a member of the interprofessional team during preventive medical visits between July 2015-March 2020 to discuss current health habits and goal setting. Data were collected at follow up visits to determine whether patients who set goals made progress towards these goals. Seventy two percent of families who met with the team were willing to set a goal at the initial encounter. Of those who set a goal, 53% reported they had partially or fully attained these goals at follow up. The presence of an interpreter did not significantly impact willingness to set a goal, overall goal attainment or add to the length of the intervention. While there are limitations to this study design, the results suggest that an interprofessional 9-5-2-1-0 intervention offers a promising approach for engaging diverse families in health habit conversations and goal setting in primary care.
“Families were most likely to be partially or fully successful with goals around sugar-sweetened beverages and screen time.”
Introduction
Research indicates that maintaining certain healthy habits significantly lowers overall morbidity, death from heart disease, and death from cancer.1-4 Not only do healthy habits impact physical health outcomes, research has shown that they also benefit various mental health and cognitive functioning outcomes across the life course. 5 For example, adolescents with a higher dietary intake quality show increased attention capacity. 6 Youth who participate in physical activity have higher physical self-perceptions, enhanced self-esteem 7 and higher midlife cognitive performance. 8 In addition, frequent and abundant consumption of fruits and vegetables both positively impacts cognitive wellbeing and prevents cognitive decline. 9 In older patients where cognitive decline is prevalent, healthy balanced diets decrease risk of mild cognitive decline and Alzheimer’s disease. 9 Older patients who are more physically active maintain cognition longer than those who are sedentary. 9
Despite these benefits, population adherence to healthy lifestyle recommendations is low, and has significant economic, social, and personal impact on patients and communities. 10 According to the CDC, nearly one third of children ages 1-5 years do not consume any daily fruit and nearly one half do not eat a daily vegetable. 11 According to this same study, over 57% of children ages 1-5 drink at least one sugar-sweetened beverage per week. 11
Urban, resource-limited settings create additional challenges to developing and maintaining healthy lifestyle habits. For example, children in households with food insecurity are less likely to eat a daily fruit or vegetable and are more likely to drink sugar-sweetened beverages. 11 Limited access to fresh fruits and vegetables, safe outdoor green space for physical activity, and readily available sugar-sweetened beverages, make healthy lifestyle options more challenging for families to implement and sustain. Historical inequities, experiences of discrimination, and inequitable access to nutrition education and programming perpetuate gaps in healthy behavior. 12 Weight stigma and bias, as well as limited integration of individual or family social and cultural strengths inhibits the potential impact of programs on lifestyle and health behaviors.
Refugee families, families with non-English Language Preference (NELP) and families with limited income face barriers to navigating programs and accessing culturally appropriate healthy foods as well as safe outdoor and exercise spaces, which in turn impacts lifestyle choices.13-15 Language barriers can provide additional hurdles to health care education and engagement around lifestyle recommendations. NELP patients are less likely to attend well-child visits 16 and have lower healthy literacy levels.17,18 They also are more likely to have social needs, including limited employment, reliance on public benefits, subpar housing, and food insecurity.18,19 Clinicians are less likely to engage in diet and exercise counseling with NELP patients as compared to English speaking patients.20,21
Pediatric well-child checks provide an important opportunity to support children and families in beginning, developing, and sustaining healthy behaviors. Support and education are provided in the context of a long-term patient-provider relationship, an ideal setting for population-level health behavior support. “Let’s Go” or 5-2-1-0 is a CDC approved nutrition and physical activity program originally developed in Maine to support children from birth to age 18 in well-child checks. 22 The program’s central message, “5-2-1-0,” refers to the daily recommendation of 5 fruits and vegetables; 2 h or less of screen time; 1 h or more of physical activity; and 0 sugar-sweetened beverages. Given growing evidence of the importance of sleep for overall health, 23 some programs have added a “9” to the intervention to represent the recommended hours of sleep per night, which comprises the 9-5-2-1-0 program.
The feasibility of health habit assessments and tailored interventions to promote healthy lifestyle in the primary care setting has been studied in the general population24,25 but not across diverse populations. This study aims to evaluate the relationship between a 9-5-2-1-0 intervention, goal setting and goal attainment with diverse populations in the primary care setting. Specifically, are diverse families who engage in the 9-5-2-1-0 intervention willing to set health habit goals and do they successfully attain these goals? We were also interested in whether the use of an interpreter impacted goal setting and goal attainment.
Method
Methods
Population
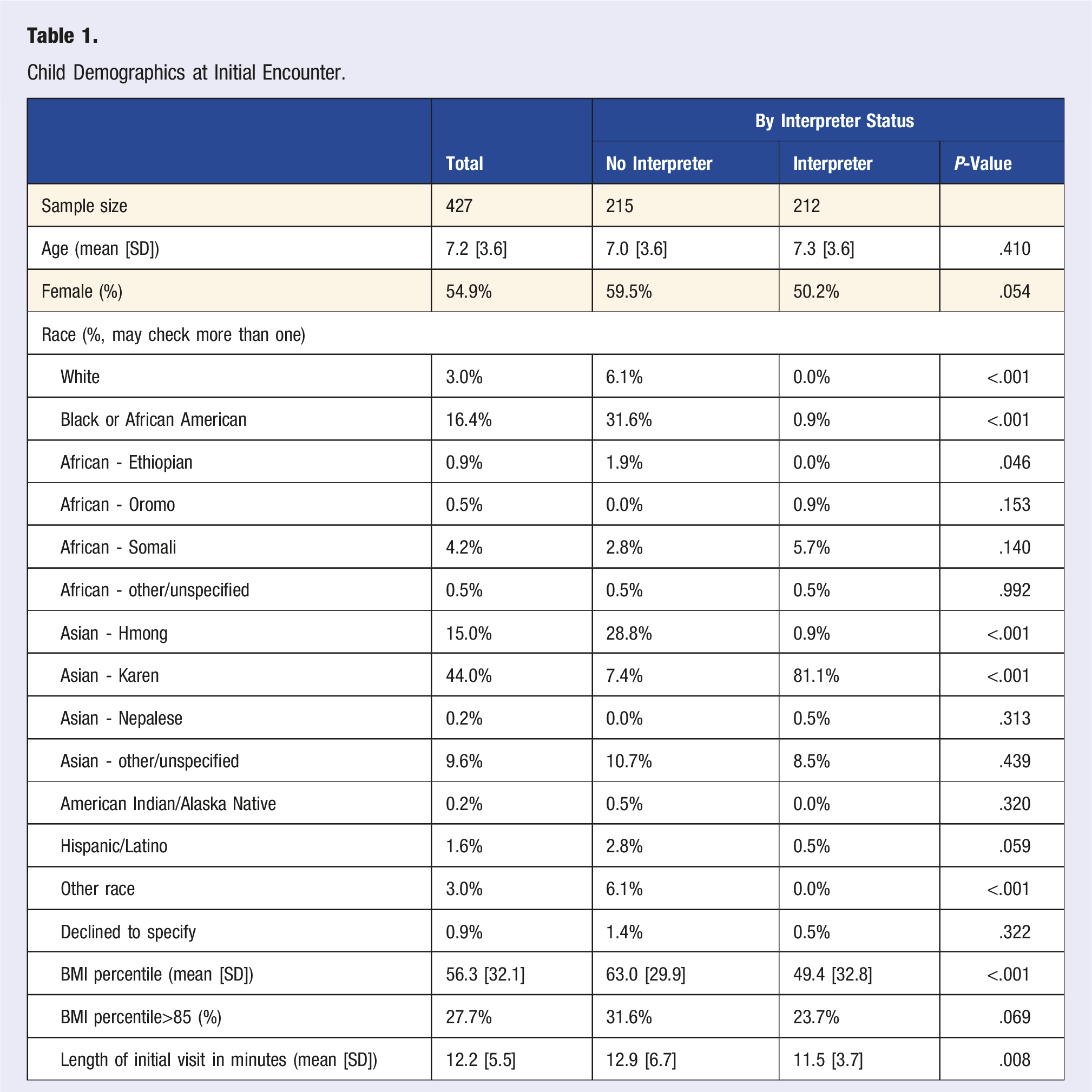
Child Demographics at Initial Encounter.
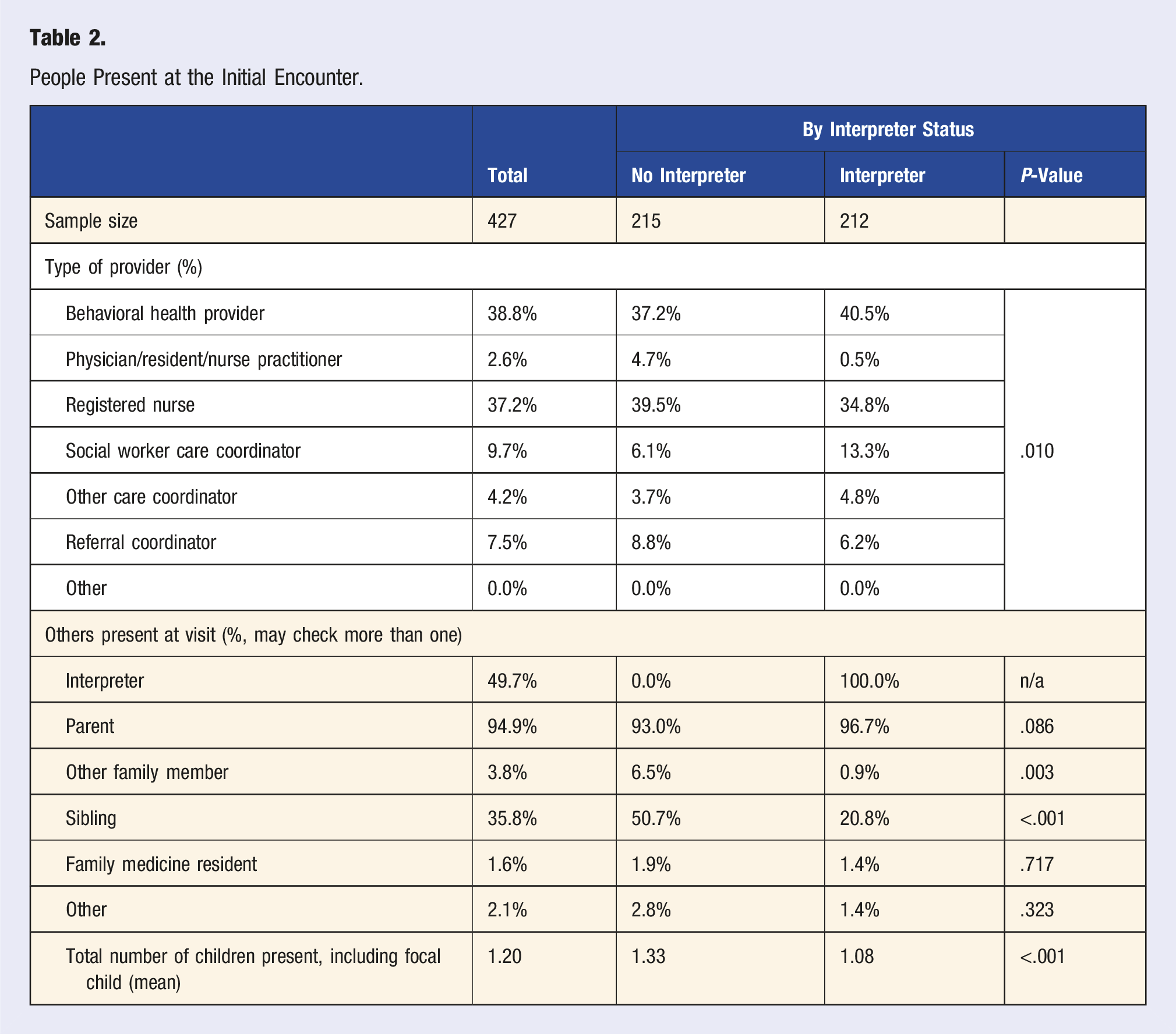
People Present at the Initial Encounter.
Materials
A Lifestyle Risk Screener (LRS) developed by the Minnesota Department of Health (State Health Improvement Program, 2007) was adapted for use in the 9-5-2-1-0 intervention. This instrument collects child-specific data on the following variables: hours of sleep per night, servings of sweets or fried/processed foods per day, servings of fruits and vegetables per day, hours of screen time per day, days of physical activity per week, minutes of physical activity per day, and servings of sugar-sweetened beverages per day.
Procedure
The 9-5-2-1-0 interprofessional team included doctoral level behavioral health clinicians (including the lead author), nurse practitioners, social workers, care coordinators and family medicine residents who all received at minimum a one-hour training session on the 9-5-2-1-0 model and motivational interviewing. Patients and families arriving at the clinic for well-child appointments were asked to complete the LRS during the rooming process. Parents were the reporters for children too young to self-identify behaviors.
Families (child, parent/guardian, siblings, etc.) were seen by a 9-5-2-1-0 provider in the clinic either prior to or following the visit with the primary care physician (PCP) to review reported health habits, provide education on recommendations and engage in conversation informed by motivational interviewing principles to explore a possible goal to set regarding their health habits. Frequently, 9-5-2-1-0 providers shared a hot hand off with the PCP to reinforce any learning/goal setting, but this was not always feasible due to time constraints and workflow. The LRS, as well as 9-5-2-1-0 provider ratings of patient/family stage of change, and goals identified by the family were entered into the electronic medical record (EMR) visit documentation.
Families were asked to meet with the 9-5-2-1-0 provider and complete the LRS at subsequent well-child visits to track progress and offer support for the development and maintenance of health habits over time. This information was again recorded in the EMR. Data from both initial and follow up visit(s) were entered in a REDCap database for storage and analysis. Determination of goal attainment was based on family report of health habits on the LRS at follow up, not family report of goal attainment.
This study was deemed to be a quality improvement project and therefore exempt by the Univeristy of Minnesota IRB.
Statistical Analysis
We computed summary statistics describing the family, provider type and data recorded about healthy habits and goals using SAS Enterprise Guide version 8.3. We also examined the observed differences whether the initial encounter included use of an interpreter. For categorical responses (e.g., type of provider present at the initial visit), we computed the statistical significance by interpreter status using a Pearson Chi-square test. For continuous variables (e.g., number of minutes per day of physical exercise), we computed the significance of differences by group using an ANOVA test.
Results
Demographics at the time of the first encounter are summarized in Table 1. The children’s average age was 7.2 with 55% being female. The sample was racially diverse, including 44% Asian - Karen, 15% Asian - Hmong, and 16% Black or African American. Families who had an interpreter present at this initial encounter were heavily concentrated in the Asian - Karen group relative to low Karen representation when an interpreter was not present (81% vs 7%, P < .001), and the children with an interpreter present had a lower BMI percentile (49 vs 63, P < .001). There were no statistically significant differences in age or sex. 9-5-2-1-0 providers spent on average 12.2 min with each patient/family. Interestingly, visits which required an interpreter were slightly shorter than visits without an interpreter.
Table 2 summarizes the family members and other participants present at the time of the initial encounter. The majority of families were seen by a behavioral health provider (39%) or a registered nurse (37%). Almost all encounters (95%) included a parent, and half (50%) had an interpreter present. The presence of an interpreter was associated with more frequent presence of a behavioral health provider (41% vs 37%) or social worker care coordinator (13% vs 6%), and less frequent presence of a registered nurse (35% vs 40%, P = .010). The presence of an interpreter was also associated with fewer non-parental family members present (1% vs 7%, P = .003), and a reduced probability that siblings were present (21% vs 51%, P < .001).
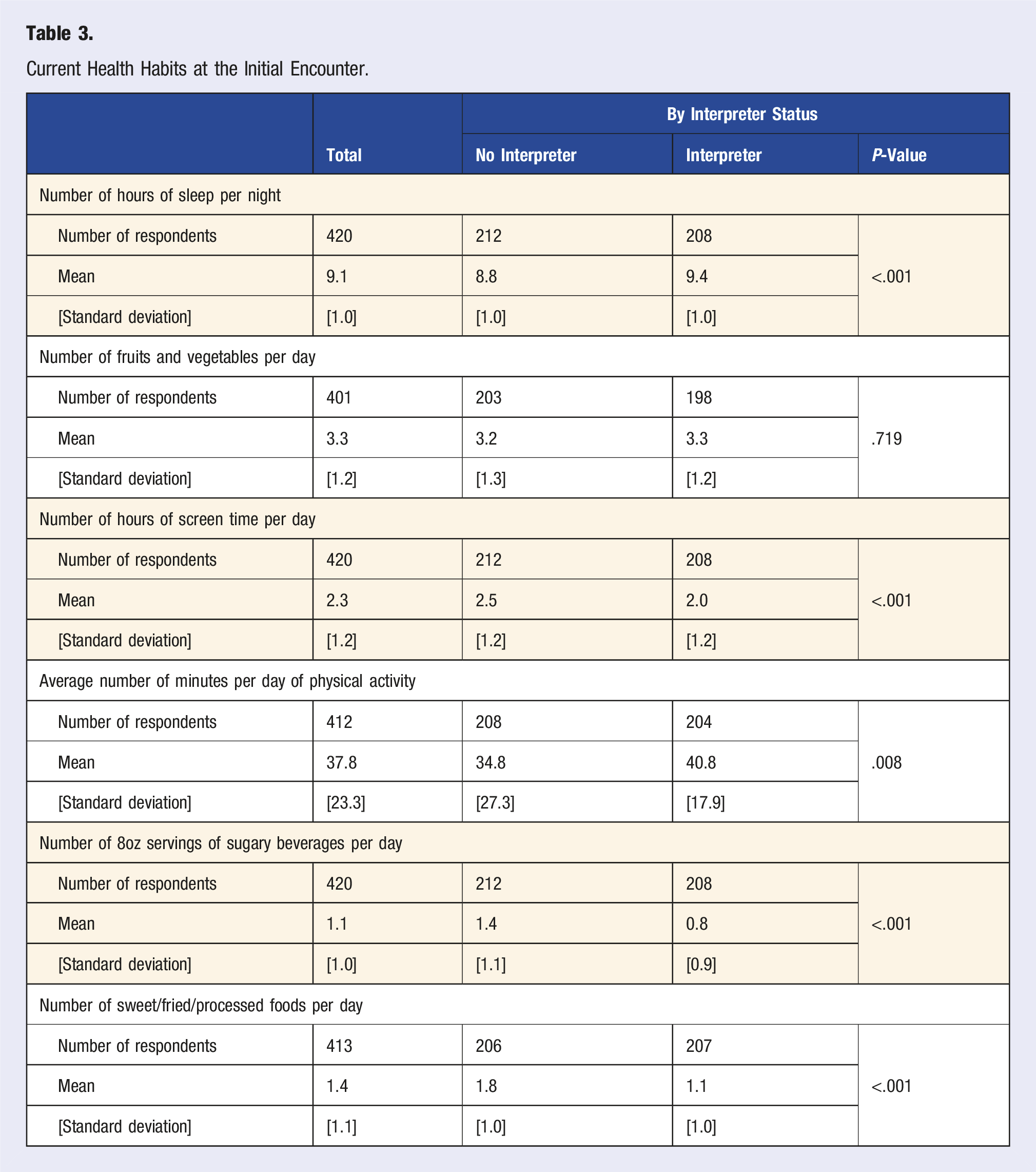
Current Health Habits at the Initial Encounter.
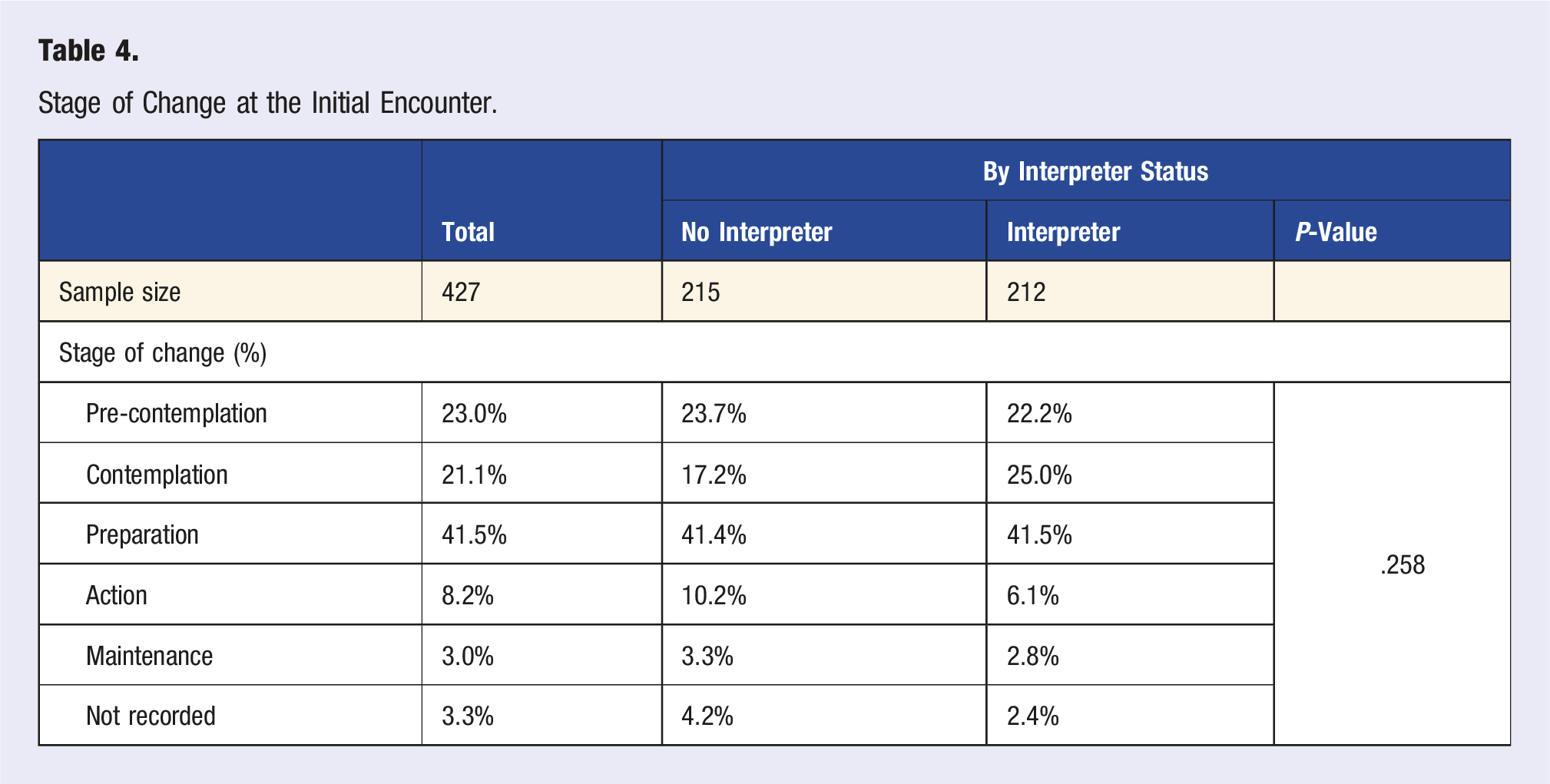
Stage of Change at the Initial Encounter.
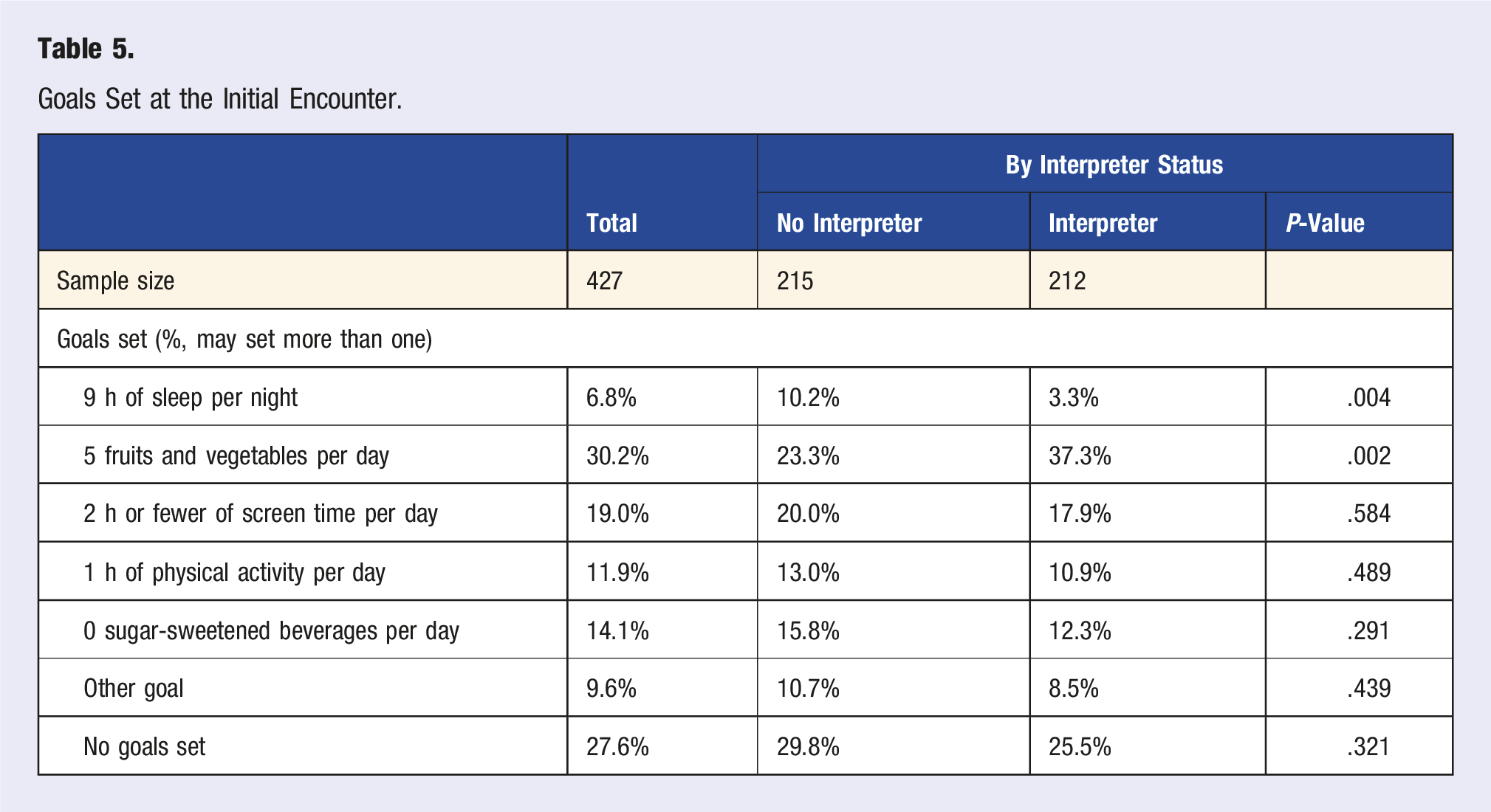
Goals Set at the Initial Encounter.
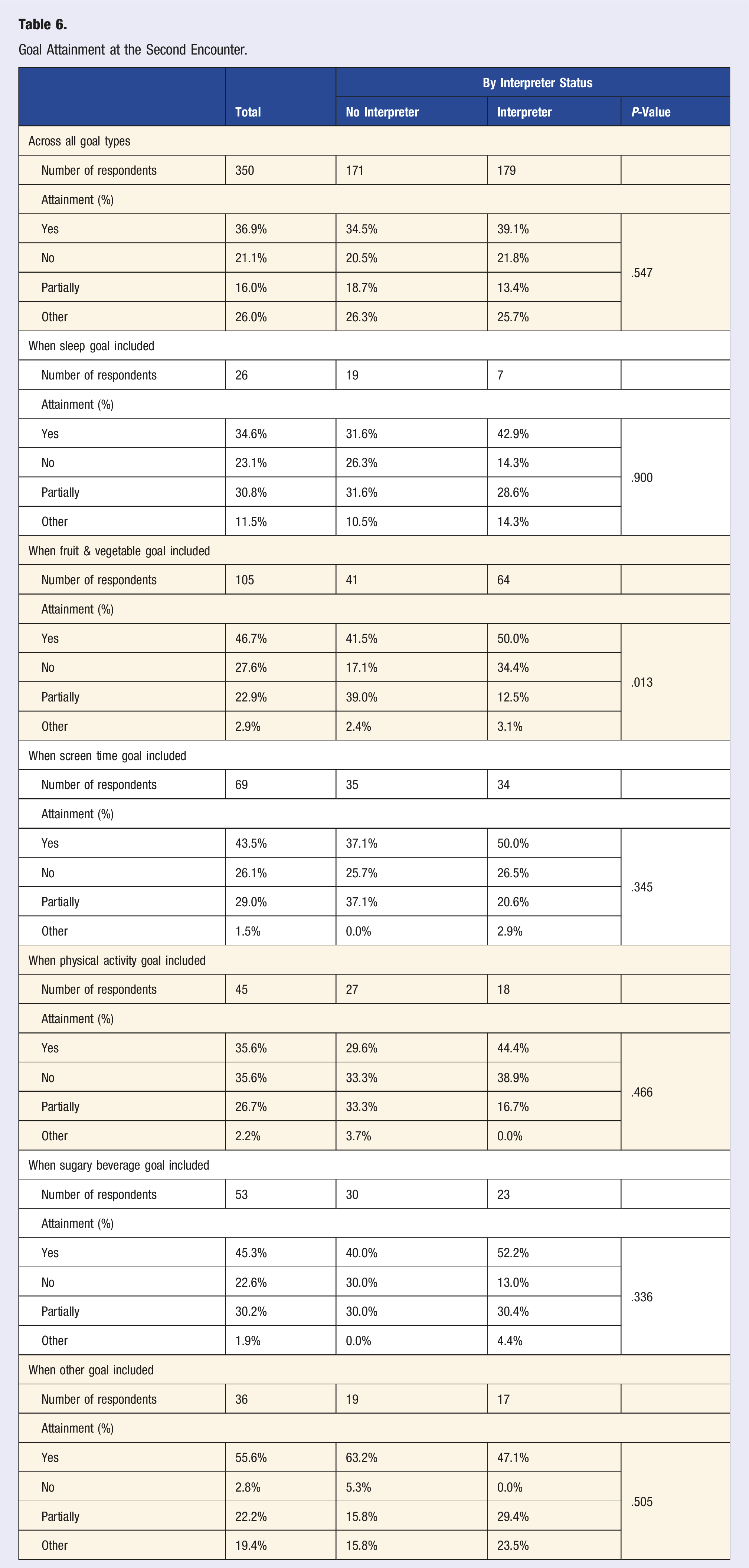
Goal Attainment at the Second Encounter.
Our final sample included 427 families with at least two 9-5-2-1-0 encounters between July 2015 and June 2020, excluding those seen only once during that time frame. Most baseline characteristics (demographics, mix of participants in the visit, current habits, stage of change, goals set) were comparable between our final sample and the excluded families. However, there were some differences that may affect generalizability. Children in excluded families tended to be older (average age 9.1 vs 7.2 years; P < .001), consistent with the wider spacing of recommended wellness visits by age. Most of the remaining differences are plausibly tied to this difference in average age, such as higher initial BMI percentile (60.6 vs 56.3; P = .015), and slightly less sleep at baseline (8.9 vs 9.1 hours; P < .001). A detailed comparison of our sample with excluded families is available from the corresponding author.
Discussion
Given the demands on primary care providers, it is helpful to highlight that short and focused discussions around healthy habits can result in goal attainment and are worth investing in during medical visits. Research indicates that pediatric health education at well-child visits on a variety of topics including nutrition and physical activity can be limited and prone to bias in the pediatric setting secondary to time constraints and other factors. 26 A team based 9-5-2-1-0 intervention, offered in a systematic manner to all children regardless of size, racial background or language preference is a promising model to support children and families in improving and maintaining health habits across the lifespan.
Our study supports the idea that diverse families were willing to engage in conversations around health habits and set goals to improve health habits in the context of well-child visits in primary care. This was true whether the family required an interpreter for the visit or not, suggesting that providers and families can have efficient, productive conversations about health habits even when an interpreter is present.
Our study also found that the majority of families who set goals reported that they fully or partially attained these goals at follow up (53%). There was no overall difference in goal attainment between families who required an interpreter and those who did not. The one exception to this was a somewhat higher success rate for families who required an interpreter and who set a goal of increasing fruit and vegetable consumption. This aligns with previously identified health goals in refugees. 13 This should be encouraging to providers who are evaluating the efficacy and value of primary-care-based conversations with families around health habits. In addition, this finding highlights the important role of interpreters in visits with NELP families, as they are potentially more successful in meeting patient and family health-related needs. While we did not track whether interpreters were physically present in clinic or available via phone or video during the visit, most clinic interpretation was offered in person prior to the pandemic in 2020. It would be interesting to evaluate the relative engagement and efficacy of the intervention comparing in person and virtual interpreters in the future.
The highest attainment at follow up was for goals that were not tied to the 9-5-2-1-0 behaviors (e.g., decreasing sweets or fried, processed and fatty foods, drinking more milk or water, etc.). This may indicate that families are more successful around self-identified, internally motivated habits. This is consistent with a motivational interviewing framework and should inspire providers to elicit patient and family values and perspectives when partnering with families around disease prevention and health promotion.
The literature indicates that new immigrants are likely to endorse better health and healthier habits than the general US population but that their health habits may decline over time with acculturation.27,28 Our study findings were in line with this prior knowledge and found that NELP families were more likely to report healthier baseline habits with the exception of fruit and vegetable consumption. While all families were most likely to choose increasing consumption of fruits and vegetables as a goal (30%) this was even more prevalent for families who required an interpreter (37%). Families with interpreters were also more likely to report success in achieving this goal (50% vs 42%). Given increased likelihood of a parent being present for interpreted visits, this may reflect the importance of parental awareness, involvement and support for the goal.
Interestingly, sleep was the least frequently chosen health behavior goal (7%). This may reflect that families were already closer to the 9 h per night goal and therefore less likely to prioritize this. That said, the second most popular health behavior goal was screen time (19%) and on average most families also reported being relatively close to the goal of 2 h of screen time per day so goal setting may be indicative of perceived control or other values/parental concerns, not just proximity to the goal at baseline.
Families were most likely to be partially or fully successful with goals around sugar-sweetened beverages and screen time. Families were least successful with physical activity goals. This may reflect the relative challenges of these various goals. While it may be relatively simple for parents to stop buying sugary drinks for the home, finding the time and safe space for increased physical activity for their child may be a greater challenge for families living in an apartment or in an unsafe neighborhood. 13 Anecdotally, 9-5-2-1-0 providers often found that school was a significant resource for both fruits and vegetables and a place for physical activity. There may be seasonal fluctuations in health behaviors around the school calendar and summer months when children families do not have the same access to these resources. Many well-child visits take place in the summer when school is still out of session.
While all 9-5-2-1-0 providers were provided with education on motivational interviewing skills, behavioral health providers likely had significantly more experience and practice with this skill set, contributing to higher rates of goal setting and goal attainment for 9-5-2-1-0 encounters facilitated by the behavioral health team. This may indicate that additional training in motivational interviewing and further inclusion of behavioral health providers in primary care teams has potential to increase goal setting and goal attainment around healthy habits.
The 9-5-2-1-0 program emphasizes an opportunity for early lifestyle interventions and health behavior goal setting to improve long-term cardiovascular outcomes, including morbidity and mortality. Future research including incorporation of biometric data, such as blood pressure, blood sugars or lipid levels, and tracking of behavioral change and outcomes across the lifespan will be important to further assess the value of these early interventions.
Limitations
Limitations of this research include reliance on self-report of health habits. We cannot know if families accurately reported health habits or if self-report was influenced by social desirability or poor recall. Our self-report measure was in English and relied on interpreters to translate for NELP patients. Concepts such as “serving size” or “physical activity” may have been interpreted inconsistently.
This study is limited by lack of attention to additional social determinants of health and other contextual variables. Future research would be strengthened by measuring these factors to better understand the interaction between these influences and individual health habits, goal setting behavior and goal attainment.
Our study design was also a limitation, in that the time between the first and second measurement period varied widely. This design limitation presents a challenge in interpreting our data (time intervals ranged from 0.6 to 4.5 years, with a median interval of 1.5 years). Results may have been different if families were assessed at more regular time intervals.
The research is also limited by the lack of a control group. We cannot say if families who received the intervention were more likely to make changes to their health habits than those who did not receive the intervention.
Footnotes
Acknowledgments
We would like to add our sincere gratitude to Sarah Addicks, Michelle Bates, Mary Becker, Mary Earm, Beth Fiebelkorn, Nicole Glumac, Nate Lombardi, Elizabeth Martinez, Deirdre Paulson, Lashana Rodgers, Emily Springer, Marni Tomczyk, Cynthia Trevino, Kristi White, Taylor Wille, Le Yang and Sherri Fong for their contributions to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received no external funding but our clinic did receive some initial support from the Minnesota Department of Health State Health Improvement Project to print 95210 educational materials for our clinic to use with patients.
IRB Protocol
This study (STUDY00017334) was determined exempt by the University of Minnesota Institutional Review Board on March 3, 2023.
Data Availability Statement
Data are not available upon request due to a lack of participant consent to share data outside of the internal study team and regulatory institutions.