
Abstract
Nonadherence to antineoplastics is a growing concern because of the increasing number of novel oral targeted anticancer therapies. Many of these agents are administered on a chronic continuous schedule for an indefinite period of time where adherence is crucial to achieve optimal disease control and prolong survival. Many factors are known to contribute to medication nonadherence. Prevention, early detection, and management of adverse drug reactions associated with oral targeted therapies require close vigilance. Knowing how to prevent and manage adverse drug reactions will help clinicians develop strategies to promote patient adherence to oral anticancer treatment regimens. Optimal adherence requires a dynamic patient-provider alliance through education, communication, ongoing monitoring, and follow-up.
Introduction
Cancer is the leading cause of death in the United States among men and women younger than 85 years of age. 1 It accounted for 23% of all deaths in 2007, the most recent year for which data are available. The 5-year survival rate is expected to improve with the increasing use of targeted anticancer therapy. 2
Even though the new oral targeted therapies offer enormous benefit, one of the biggest challenges is improving patient adherence to therapy at home.
Advances in the understanding of molecular biology and carcinogenesis have led to the development and approval of novel oral anticancer agents, which has shifted the responsibility of drug administration to the patient in the community setting instead of a supervised clinical setting.3,4 The new oral anticancer agents, also called targeted therapeutic agents, include small-molecule inhibitors that target intracellular signaling effectors and pathways that regulate cancer cell proliferation, apoptosis, angiogenesis, invasion, and metastasis. 5 These “smart drugs” can focus on inhibiting interactions taking place on the cell surface or inside the cancer cell, thereby leading to cell death.
An increasing number of oral targeted agents are in development and undergoing phase I and II trials. They are expected to be available for clinical use in future years. An estimated one quarter of the 400 antineoplastic agents are currently in the pipeline as oral drugs according to the 2008 Task Force Report of the National Comprehensive Cancer Network. 6 With Federal Drug Administration (FDA) approval, the expected availability of oral antineoplastic agents will rise from 10% in 2008 to 25% in 2015.
Part 1: Medication Adherence and Oral Antineoplastics
Adherence rates average 50% for long-term drug treatment of chronic conditions according to a 2003 report by the World Health Organization (WHO) and is even lower in the developing world. 7 The Cochrane group on Medication Adherence also reported similar low adherence rates, thereby potentially compromising the effectiveness of the therapy. 8
A higher adherence rate is expected in life-threatening and serious diseases such as cancer.9,10 Data are scarce regarding oral antineoplastic medication adherence in cancer patients, particularly those with malignancies other than breast cancer. It was believed that most patients with cancer would take drugs as prescribed because of the nature of the disease, but that has not been the case. The limited available evidence suggests that adherence to oral antineoplastic agents is quite variable and ranges from 20% to 100%.
There is no consensual standard for what determines satisfactory versus poor adherence in cancer pharmacotherapy.10,11 A greater than 90% adherence rate is considered adequate in clinical trials with oral targeted therapies to observe a complete molecular response. Further investigations are needed to determine the optimal adherence rate associated with dose-related response of the individual targeted therapies.
Adherence is defined as the extent to which individuals take medication for as long as it is prescribed by their physician in the correct dose (taking the prescribed number of pills or daily dose) and at the correct time (taking pills within a prescribed period or with special considerations such as food).12,13 Adherence to a medication regimen is dependent on a set of intentional behaviors that include filling the prescription; timely administration of the correct drug, dose, frequency, and interval by the oral route; and persisting with taking the medication as long as it is required. Despite the advantages of oral targeted therapies, they do pose challenges such as uncertainty of adherence.
Barriers to Adherence
The majority of patients prefer oral anticancer to parenteral therapy.14-16 As more patients choose oral antineoplastics—affording them more convenient, noninvasive treatment options; a reduction in the number of regularly scheduled office or clinic visits; and less time with physicians— providers have difficulty in monitoring patient medication adherence. Potentially fewer office visits may influence adherence according to the National Comprehensive Cancer Network Taskforce Report on Oral Chemotherapy. 6 Even though the new oral targeted therapies offer enormous benefit, one of the biggest challenges is improving patient adherence to therapy at home. 17
Much effort has been expended to understand the barriers to medication adherence in chronic disease, and many variables have been identified.18,19 Therefore, different approaches will be needed to improve adherence, particularly in cancer patients.
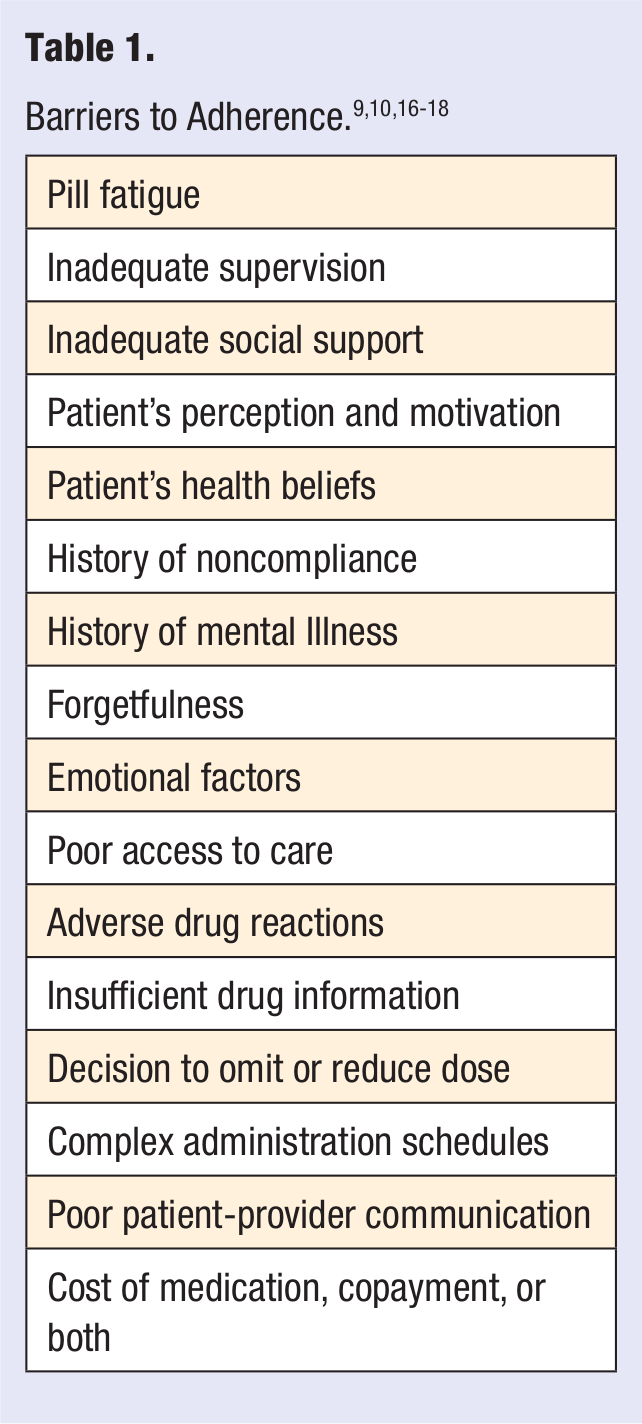
Patients may be nonadherent for nonintentional reasons, such as forgetfulness or pill fatigue associated with chronic administration or intentional reasons such as a lack of belief in the medication or believing that the cost of the medication and related side effects outweigh its benefits.20,21 A list of barriers to adherence is provided in Table 1. Intentional nonadherence is considered a behavioral issue, and nonintentional nonadherence is “process oriented.”
Health care providers should be aware that some cancer patients adjust their dose without informing them. Taking more than the prescribed dose of oral anticancer medication because of perceived ineffectiveness or the belief that “more is better” can lead to a substantial increase in toxicity.22,23 Conversely, cancer patients may decrease the dose or omit doses because of a fear of adverse effects as a result of taking the drug.
Another important consideration is medication costs related to targeted therapies. The requirement by many drug insurance companies to use mail order or specialty pharmacies or designated specialty networks in order to obtain network pharmacy benefit coverage may result in a delay in receiving the medication.24,25 Although Medicare D plans provide coverage for oral targeted therapies, patients are caught in the “doughnut hole” when they lose drug coverage through the gap, paying much out-of-pocket money for these costly drugs. Patients too young to qualify for Medicare also face increased out-of-pocket expenses and high copayments. 26 Patients may reduce their dose or temporarily stop taking expensive oral anticancer drugs to delay the need for refills and avoid high costs and copayments.
Consequences of Nonadherence
Medication nonadherence can lead to disease progression and even premature death, adverse drug events, additional prescriptions, changes in dose and regimen, unnecessary hospitalizations and diagnostic testing, and increased health care costs.27-31 Nonadherence accounts for approximately 11% of hospitalizations in older adults. In 1 report, 32 patients who filled fewer than 70% of their anticancer prescriptions (eg, tamoxifen) had an increased risk of death from breast cancer. In the United States, poor adherence has been estimated to cost approximately $177 billion annually, of which $47 billion is attributable to drug-related hospitalizations and an additional $2000 in medical costs each year per patient for physician visits in total direct and indirect health care costs, according to a report by the National Council on Patient Information and Education. 33
Improving Adherence to Oral Antineoplastics
Signs and predictors of nonadherence include missed appointments, unfilled prescriptions, toxicity, lack of belief in the benefits of treatment, depression, cognitive impairment, treatment of asymptomatic disease, lack of insight into the illness, poor provider-patient relationship, and lack of adequate social support.34-37 Patients who develop negative views regarding their care may miss appointment visits. Lack of timely follow-up with their physicians may also lead to nonadherence. Physicians may deem treatment failure when a patient presents with the equivalent degree of disease severity or greater degree since his or her time of initial presentation, whereas, in fact, the patient has not been taking the treatment drug as prescribed.
Providers are also limited by the lack of a gold-standard measurement for assessing medication adherence.9,10,18,38 There are different ways to measure adherence, but they have their own limitations as well. Most significant is the patient history where patients self-report their medication intake. Limitations to the history taking could include patients falsifying information to prove themselves “good patients” and reporting complete medication adherence, whereas in fact they are nonadherent and clinically getting worse.
Continuous dose monitoring and direct observations are used, but because patients know that they are being observed, there is a possibility of the “Hawthorne effect,” 39 where patients change their behavior because they are under observation. Although pill counts, returning empty bottles, and self-report diaries during clinical trials are also ways of establishing medication adherence, there is a probability that patients might manipulate the number of pills before their next clinical appointment.
One way to more accurately assess adherence is the use of “smart bottles” or microelectronic monitoring systems (MEMSs). A study by Lee et al 40 investigated medication adherence in lymphoma patients using MEMS, where the light entry in the prescription bottle detects the act of opening it and records the time of opening. The authors point out that the process of opening bottles does not guarantee the ingestion of pills. Another suggestion could be to monitor insurance and pharmacy records, but this method does not determine how well the patient is taking the medicine. 9
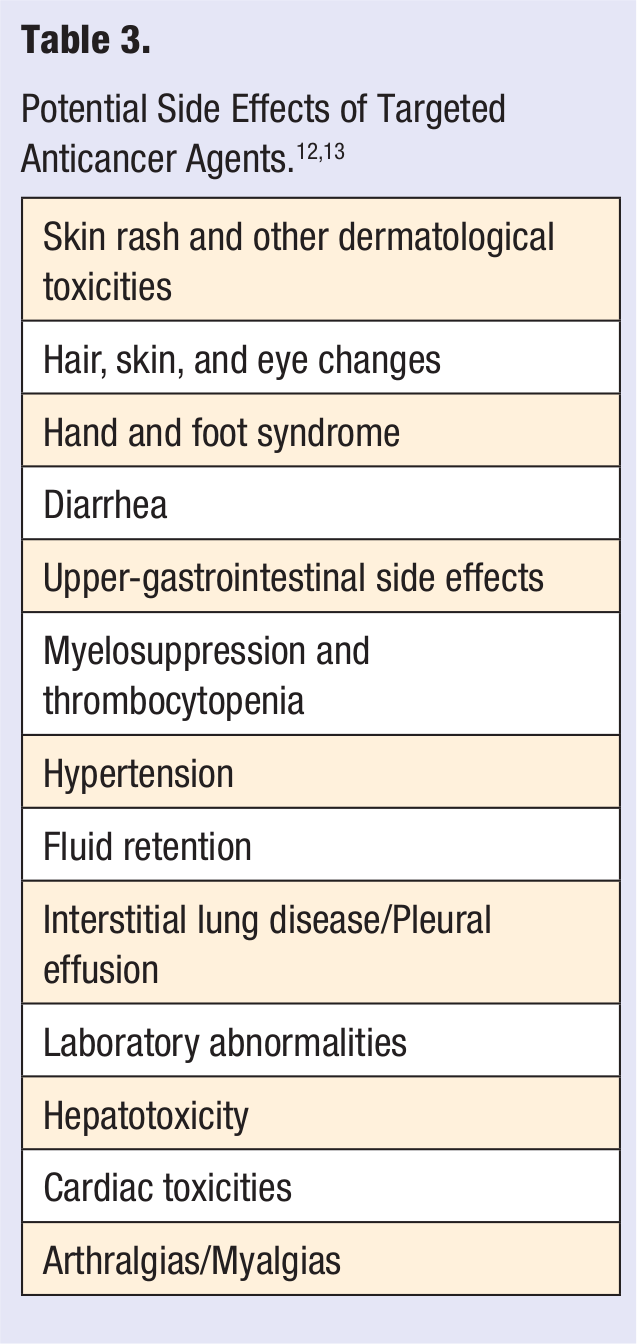
An objective approach could be to establish a multidisciplinary approach by physicians, nurses, pharmacists, nutritionists, and social workers to adherence education and management.41,42,43 Studies have shown that a multidisciplinary approach to medication taking behavior is necessary for patient adherence to be sustained. An action plan with 10 recommendations released by the National Council on Patient Information and Education calls for raising awareness of medication adherence as a critical health care issue and mounting a coordinated, multidisciplinary campaign to improve adherence. 33 Multiple strategies and repetitive interventions suggested to improve medication adherence behavior among those with cancer are provided in Table 2. The extent of nonadherence in cancer patients as a result of adverse effects related to targeted therapies needs investigation. Educating patients about potential adverse drug reactions, their detection, and management prior to starting oral targeted therapies is recommended (Table 3). Further studies are needed to determine the success of this intervention by physicians, pharmacists, and nurses in cancer patients.
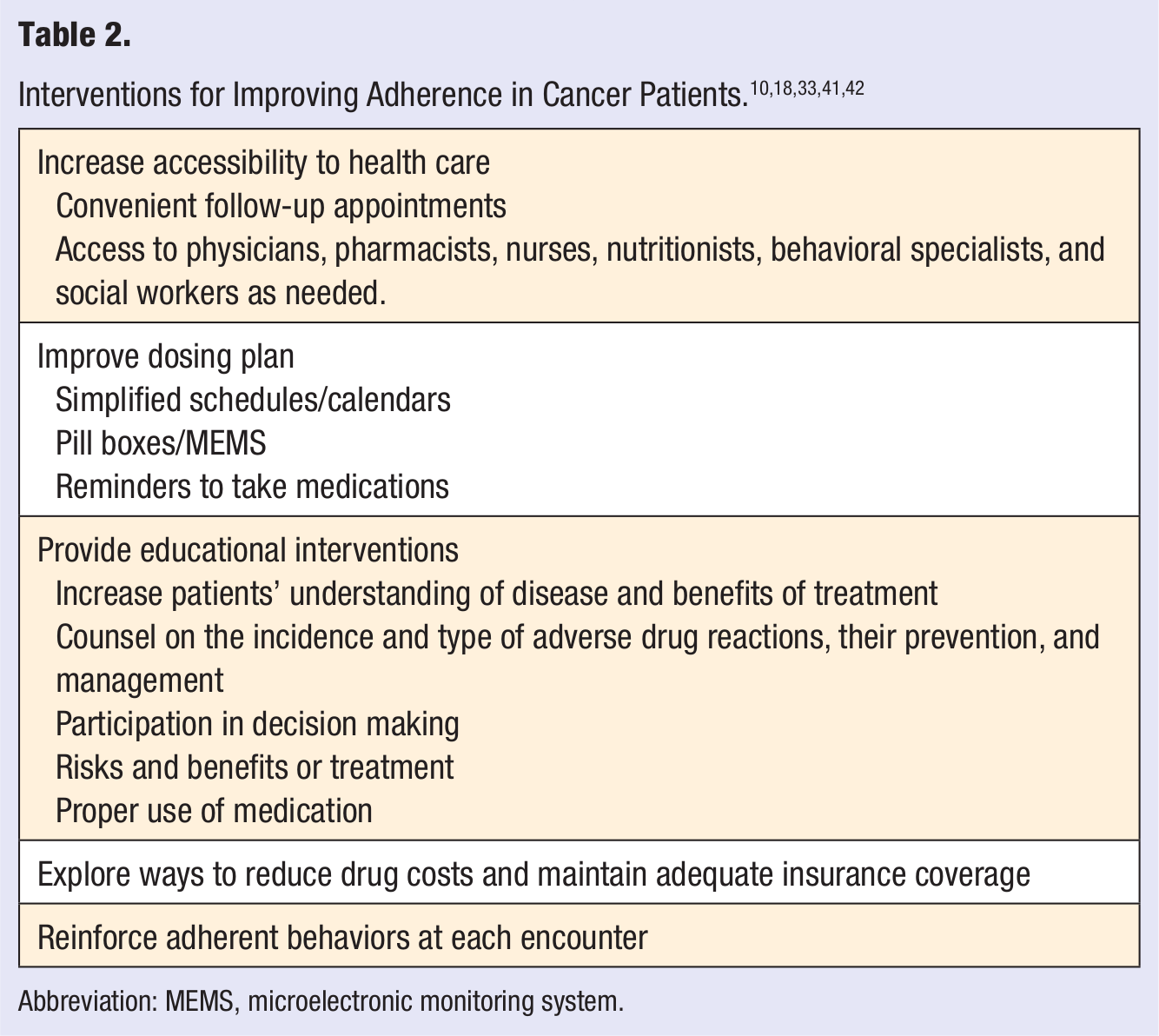
Abbreviation: MEMS, microelectronic monitoring system.
Another consideration of oral targeted therapy is variable absorption that may be dependent on meal time and unpredictable or incomplete bioavailability, making medication adherence critical. 44 Taking medication with regard to meals is an important consideration that may determine effectiveness and/or toxicity. With targeted therapies, there is no consistency about taking the medication with food or on an empty stomach, and each drug has its own recommendation. Patients should be educated about the optimal time to take their oral antineoplastic medication daily (Table 4).45-57
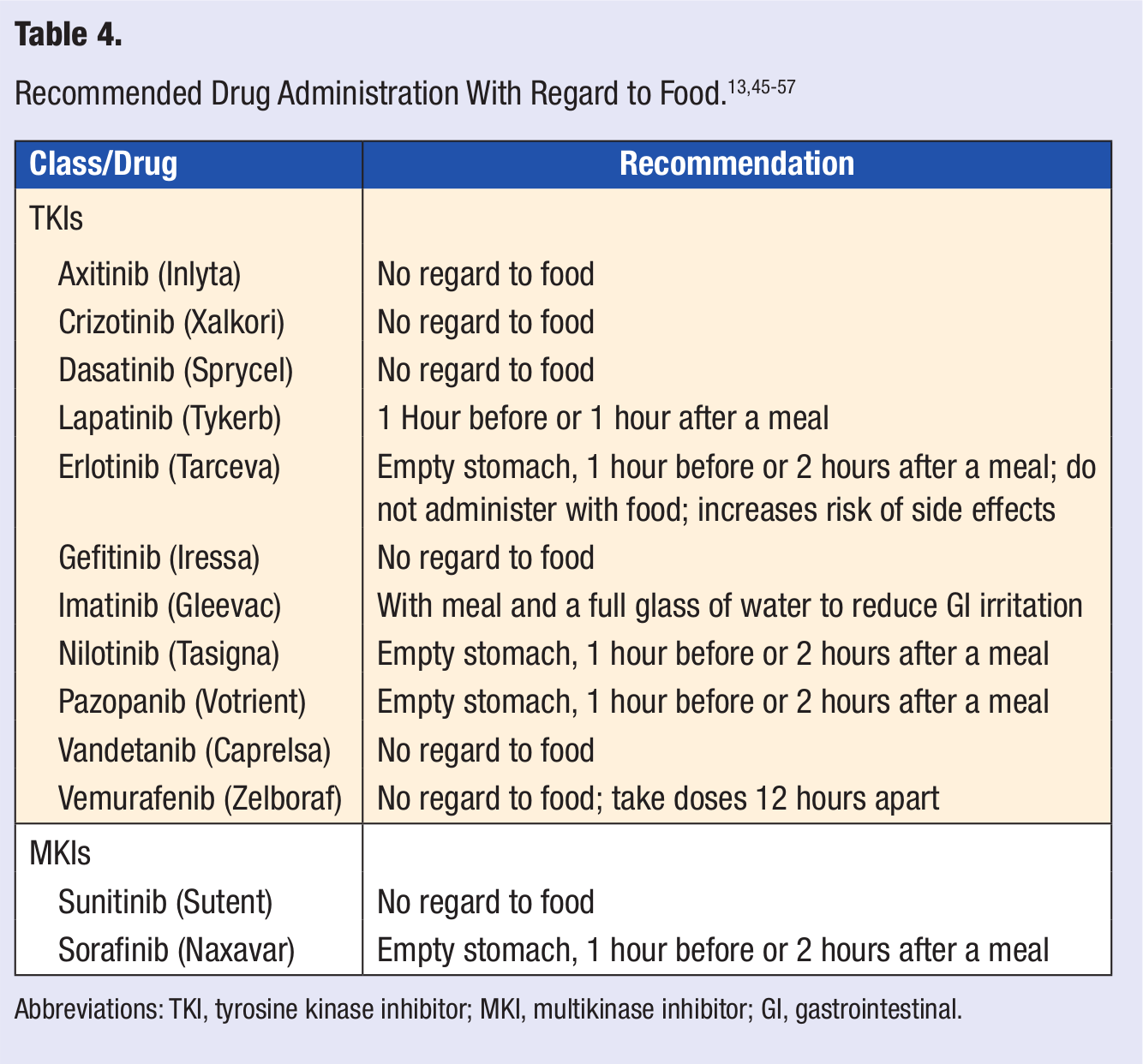
Abbreviations: TKI, tyrosine kinase inhibitor; MKI, multikinase inhibitor; GI, gastrointestinal.
Part 2: Newer Targeted Therapies
The signal transduction inhibitors are targeted to components of intracellular signaling pathways such as protein kinases and include the class of drugs called tyrosine kinase inhibitors (TKIs) and multitargeted small-molecule TKIs or multikinase inhibitors (MKIs; Table 5).58,59 Most of these agents do not cure disease. Rather, they prolong disease progression and improve survival rate.
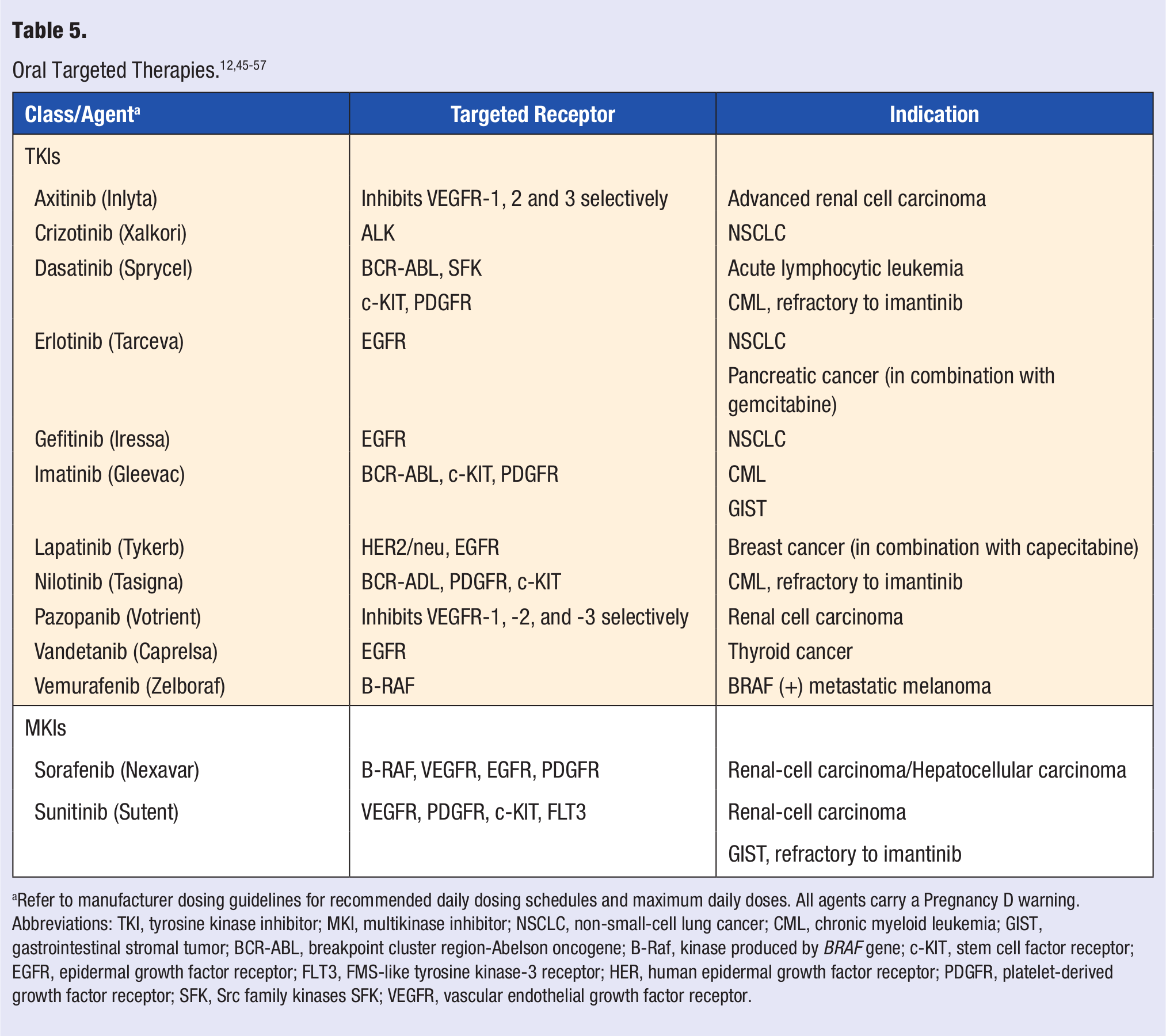
Refer to manufacturer dosing guidelines for recommended daily dosing schedules and maximum daily doses. All agents carry a Pregnancy D warning.
Abbreviations: TKI, tyrosine kinase inhibitor; MKI, multikinase inhibitor; NSCLC, non-small-cell lung cancer; CML, chronic myeloid leukemia; GIST, gastrointestinal stromal tumor; BCR-ABL, breakpoint cluster region-Abelson oncogene; B-Raf, kinase produced by BRAF gene; c-KIT, stem cell factor receptor; EGFR, epidermal growth factor receptor; FLT3, FMS-like tyrosine kinase-3 receptor; HER, human epidermal growth factor receptor; PDGFR, platelet-derived growth factor receptor; SFK, Src family kinases SFK; VEGFR, vascular endothelial growth factor receptor.
Because targeted therapy is associated with high antitumor activity, lower systemic toxicity, or both, dosing regimens are designed to produce prolonged exposure to these agents, sometimes for an indefinite period of time. 60 Some tumor cells may develop tyrosine kinase resistance to selected therapy.61,62 Optimal doses have not been established in this setting; however, dose escalation of TKIs may overcome resistance, making it vital that patients adhere to changes in their dosing schedule. Therapeutic drug monitoring or monitoring serum drug levels is not recommended, and titration of dose is usually based on signs of toxicity.
Drug-Drug Interactions
Many of these small-molecule inhibitors are metabolized by the small bowel and/or cytochrome P450 (CYP 450) hepatic enzymes.63,64 All available TKIs and MKIs are substrates for CYP450 enzymes and are subject to clinically significant drug interactions with potent CYP3A4 enzyme inducers or inhibitors such as amiodarone, anticonvulsants, azole antifungals, dexamethasone, isoniazid, macrolide antibiotics, nefazodone, protease inhibitors, rifampin, St John’s wort, and verapamil.45-57 Patients taking TKIs and MKIs should undergo careful medication review and may require dosage modification when these drugs are coadministered with potent CYP450 enzyme inducers or inhibitors. Additionally, the TKI imatinib inhibits CYP2D6, and nilotinib inhibits 2C8, 2C9, and 2D6. Warfarin is a substrate of both 3A4 and 2C9 and should be used with caution and monitored carefully in the presence of these agents. Warfarin dose adjustments may be necessary to avoid toxicity. Inclusive lists of clinically significant drug interactions and specific dose adjustments for each drug should be investigated by the prescribing clinicians.
Several of these oral agents, particularly TKIs that are epidermal growth factor receptor inhibitors (EGFRIs) and the MKIs are associated with prominent, and sometimes clinically significant, dose-limiting dermatological reactions that may result in nonadherence.65-67 Even though targeted therapies produce their anticancer effect by hindering the development of rapidly proliferating cancer cells, healthy cells that regenerate quickly may also be affected.68,69 These include mucosal, intestinal, and hair cells as well as bone marrow. Adverse effects such as diarrhea, nausea, vomiting, mucositis, alopecia, and myelosuppression may develop. The overall risk of cardiotoxicity such as QT interval prolongation and heart failure associated with targeted therapies is generally low but may occasionally be significant and lead to drug discontinuation. Prospective monitoring of cardiac function is advisable with their use. 70 Table 6 includes a list of some of the commonly occurring side effects associated with targeted therapies.
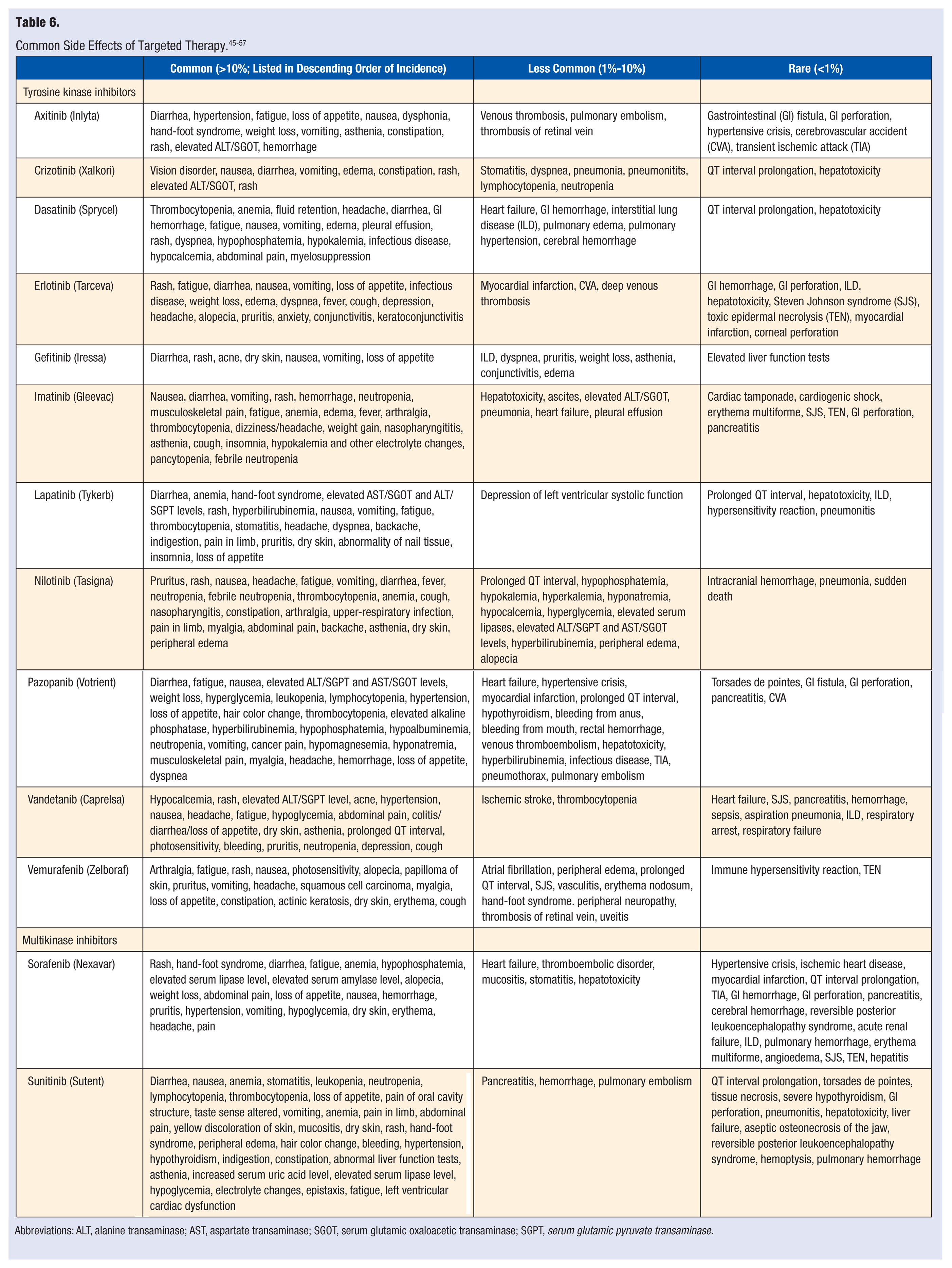
Abbreviations: ALT, alanine transaminase; AST, aspartate transaminase; SGOT, serum glutamic oxaloacetic transaminase; SGPT, serum glutamic pyruvate transaminase.
Multikinase Inhibitors
The adverse drug effects of the MKIs, sunitinib and sorafenib, have been described in several phase-III studies. The most bothersome reported adverse effects are cutaneous reactions—namely, palmar-plantar erythrodysesthesia, also known as hand-foot syndrome. Other common adverse effects linked to MKIs are rash, diarrhea, fatigue, nausea, and alopecia.71-73 Rarer and potentially more serious effects of MKIs include cardiac toxicity, gastrointestinal perforation, and hypothyroidism. Hypertension and a decrease in left-ventricular ejection fraction are concerns with the use of MKIs. Hypothyroidism, most commonly associated with sunitinib, is also a potentially serious adverse effect, which requires periodic monitoring of the thyroid-stimulating hormone level. 74
Tyrosine Kinase Inhibitors
TKIs, just like MKIs, include drugs in the class that have similar adverse effects. TKIs have the potential to cause rash, and this is more likely to occur with EGFR inhibitors (dastininb, erlotinib, imatinib, lapatinib, nilotinib, and vadetanib).56,71,75 Rash is most commonly reported with erlotinib (49%-75%, all grades, of which 5%-8% may be severe). 46 Diarrhea is also commonly reported with TKIs. 76 Additionally, each agent in this class has its own set of distinctive adverse effects. Dasatinib, which is more potent than the other agents in its class, can cause myelosuppression, edema, nausea, vomiting, and anorexia. However, dasatinib-associated QT interval prolongation and hepatotoxicity are the most dangerous. ECG monitoring is recommended to detect dangerous QT interval changes. Liver transaminases should be routinely monitored. Imatinib, nilotinib, and sunitinib have also been associated with QT interval prolongation.48,77 Severe congestive heart failure and left-ventricular dysfunction have been reported in patients taking imatinib. Gefitinib 47 is least associated with QT interval prolongation. FDA labeling for gefitinib (Iressa) limits the indication to cancer patients who, in the opinion of their treating physician, are currently benefiting or have previously benefited from gefitinib treatment. New patients should not be given gefitinib because a large study demonstrated that it did not improve survival. The latest additions to the TKI class—pazopanib, 55 vandetanib, 56 and vemurafenib 57 —may also cause QT interval prolongation.
Imatinib and nilotinib can cause myelosuppression, whereas imatinib can also cause hypokalemia, muscle cramps, and fatigue, and nilotinib can cause hyperglycemia and edema. 76 Basic metabolic panel monitoring of electrolytes is required during therapy with these agents and also with other TKIs, dasatinib and pazopanib, and the MKIs, which can lead to various electrolyte changes.49,51.52,55 Conjunctivitis has been reported with erlotinib. 46
Gastrointestinal perforation represents a rare but serious and potentially fatal adverse effect associated with MKIs and some TKIs. 68 A safety warning by the manufacturers of erlotinib, imatinib, and axitinib has been issued about their association with gastrointestinal perforation (<1%).46,48,53 The manufacturer of pazopanib 55 also reported gastrointestinal perforation or fistula in 5 patients, which was fatal in 2 patients. The manufacturer of erlotinib 46 also warns of rare cases of Stevens-Johnson syndrome and corneal perforation that have also been reported with the drug (<.01%). Stevens-Johnson syndrome has also been reported with sorafenib, imatinib, vandetanib, and vemurafenib.48,52,56,57
Part 3: Common Adverse Drug Reactions and Their Management
Skin Toxicities and Management
EGFR inhibitor–related dermatological toxicities are most bothersome and include skin rash (Table 7), superinfection of skin, pruritis, xerosis, and fissures.
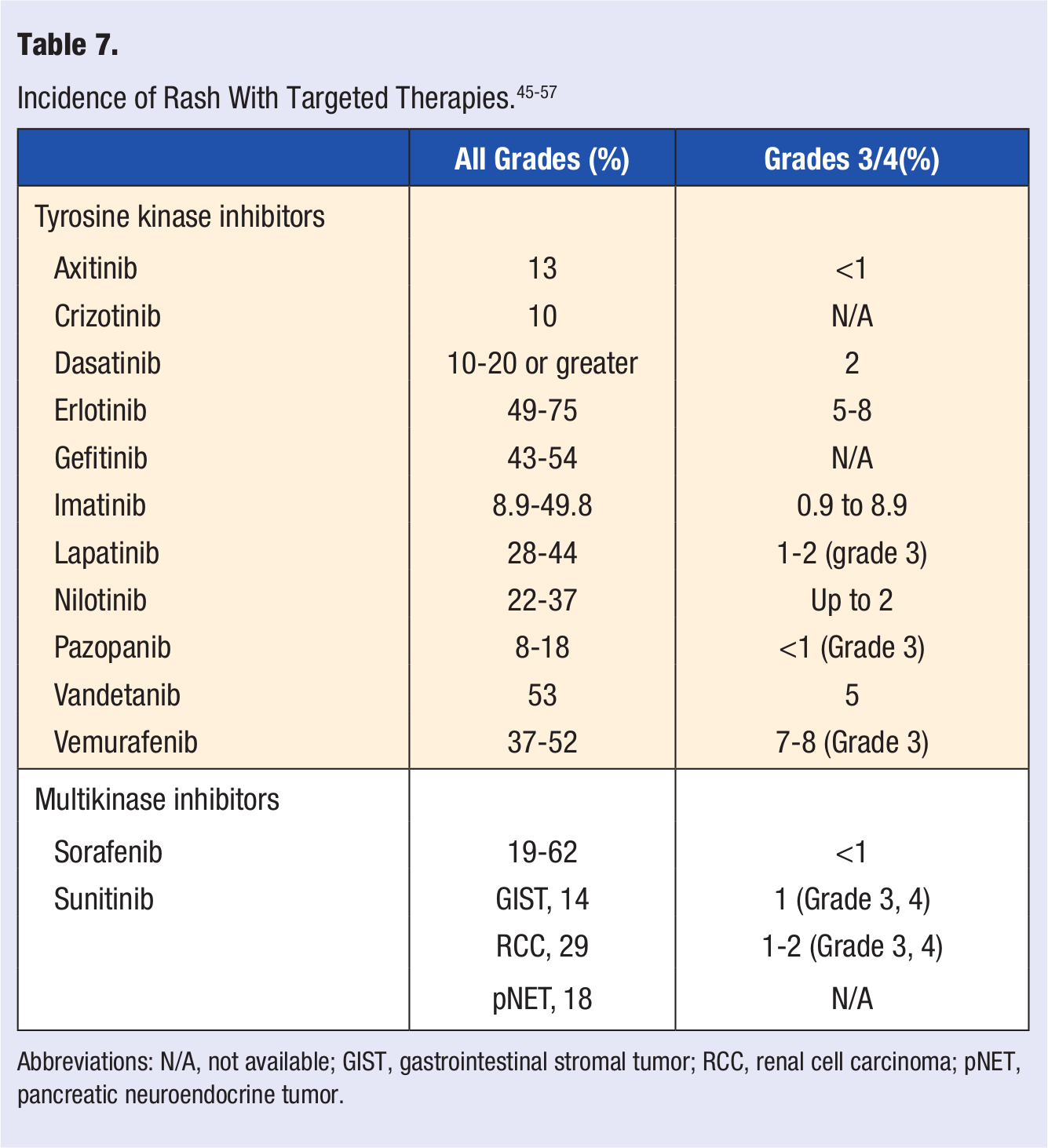
Abbreviations: N/A, not available; GIST, gastrointestinal stromal tumor; RCC, renal cell carcinoma; pNET, pancreatic neuroendocrine tumor.
Skin rash is considered a potential marker for drug activity and clinical outcome of EGFRIs. 78 Patients should be educated to report any sort of rash to the physician. There is a consistent positive correlation between the severity of rash and antitumor activity.
The skin eruption consists of a dry, erythematosus, papulopustular rash, typically without comedones, occurring from inhibition of EGFR in basal keratinocytes, resulting in follicular degeneration and destruction. 67 The rash is usually seen with drugs that target EGFR receptors but is not limited to them exclusively. The rash is dose dependent, with or without pruritis, and usually begins within 8 to 10 days after initiation of treatment and becomes more intense at week 2. During weeks 4 to 6, the rash peaks, and it decreases in severity after weeks 6 to 8. Erythema and hyperpigmentation develop in the affected areas and may last for months to years. It occurs mainly on the face, trunk, and extremities, sparing the palms and soles. Scaling of the interfollicular skin may also be present. Only in the most severe cases is EGFRI therapy stopped. One way to control bothersome rash is to counsel patients to take EGFRIs on an empty stomach because food increases their bioavailability and dose-related side effects such as rash.
A grading scale for rash according to severity is used to determine if the dose should be reduced or the drug stopped. 76 Severity of adverse events is based on the National Cancer Institute-Common Technology Criteria for Adverse Events grading scale. 79 A scale of 1 to 5 is used with grade 1 rash being localized and grade 5 rash being death.
A grade 1 reaction is asymptomatic not affecting activities of daily living (ADL) nor change in treatment. 80 Grade 2 is acneiform rash involving <50% of body surface area. In fact, maintaining a grade 2 skin rash is optimal to ensure antitumor activity. Once the acneiform rash worsens and covers more than 50% of the body, it is considered severe or grade 3. A grade 4 rash is considered severe, life threatening, and disabling, with ulcerations, exfoliations, and bullae.
Specific treatment protocols to prevent and manage EGFRI rash vary widely throughout different centers that use these agents in their clinics. Nonetheless, some basic principles may apply. A multinational, interdisciplinary panel of experts in oncology supportive care recently developed consensus guidelines for EGFRI-related dermatological toxicities. 81 Because of a lack of randomized control clinical trials with control groups, most of the recommendations were based on pertinent studies and case reports in conjunction with expert opinion and consensus on presented findings.
Inflammatory chemokines have been shown to be released in vitro after EGFRI administration. 81 The acneiform lesions caused by EGFRIs are completely different from acne. Nonetheless, antiacne medications such as oral minocycline and doxycycline along with anti-inflammatory topical steroids have been shown to be effective in the prevention and treatment of EGFRI rash in descriptive studies. Systemic steroids are not recommended.
For prevention, the recommended dose of minocycline, 100 mg daily, or doxycycline, 100 mg twice daily for 6 weeks, may be prescribed at the initiation of EGFRI therapy. 81 Minocycline is less photosensitizing, and doxycycline is safer in patients with renal impairment. Hydrocortisone 1% topical cream along with a moisturizer and a sunscreen block should also be applied twice daily. However, topical benzoyl peroxide and retinoid are not used because they can dry the skin even more and enhance burning and irritation.
For treatment, systemic minocycline or doxycycline may be prescribed for 6 weeks. 81 Medium- to high-potency topical steroids such as alclometasone 0.05% cream or flucinonide 0.05% cream, along with a topical antibiotic, clindamycin 1%, are also recommended. The agents should be applied to the affected areas twice daily. The EGFRI should be continued while grade 1 or 2 rash is being treated. 82
Both grade 3 and 4 rash are managed with a dose reduction or interruption of EGFRI therapy while treatment with oral antiacne medications and topical steroids and topical clindamycin continues. 81 If superinfection occurs, hospitalization may be required to provide supportive care with appropriate intravenous antibiotics. Finally, oral isoretinoin therapy with low doses (20-30 mg daily) is only recommended when all other measures to treat rash fail because it may exacerbate xerosis and paronychia associated with EGFRI use. It is used with extreme caution and only considered in patients who have a positive antitumor response necessitating continuation of EGFRI therapy.
EGFRIs can cause xerosis as a result of abnormal keratinocyte differentiation that debase stratum corneum with diminution of loricrin, a protein responsible for scaffolding epidermis.68,81 Dry skin can lead to inflammation known as xerotic dermatitis. There are no randomized controlled trials, but case and cohort studies indicate that preventive techniques such as avoidance of hot showers and use of moderate warm water for bathing work. For mild to moderate xerosis, extreme temperatures are to be avoided. Use of thick moisturizing creams without fragrances containing urea, colloidal oatmeal, or petroleum are recommended. For severe xerosis and inflammation, topical steroid creams are applied locally. For scaly xerosis, ammonium lactate 12% or lactic acid 10% topical cream may be applied to the affected area twice daily.
Fissures related to EGFRIs are reported to occur in the hands and feet. 81 Recommendations are based on case studies, observations, expert opinion, and studies in noncancer patients regarding treatment-related fissures. For prevention, protective footwear and avoidance of friction at susceptible sites such as toes, heels, soles, fingernails, knuckles, and palms are recommended. Bleach soaks can also be used to prevent infection. The treatment of fissures includes thick moisturizing or zinc oxide creams. Cyanoacrylate and liquid glues can also be used to seal cracks to prevent infection. Zinc oxide, steroid tapes, hydrocolloid dressing, and topical antibiotics are also used to treat fissures.
Pruritis can occur with papulopustular rash and also as a result of dry skin (xerosis). 81 Prevention measures include gentle skin care. Medium- to high-potency topical steroid creams such as triamcinolone acetonide 0.025%, desonide 0.05%, fluticasone 0.05%, and alclometasone 0.05% may be used. If bothersome, a systemic antihistamine may be considered after determining the risks and benefits of therapy. A second-generation systemic antihistamine such as loratadine has been shown to be effective and is preferred for daytime use. At night, first-generation antihistamines, such as diphenhydramine or hydroxyzine, may be used because of their sedative effects. Antihistamines are not recommended in elderly patients. Second-line pruritis treatment with systemic gabapentin or pregabalin may be tried, although randomized controlled studies are lacking. These agents were found to be effective in the treatment of EGFRI rash in small case series.
Over-the-counter topical menthol solutions may alleviate rash and itch associated with pruritis because of their cooling effect. 81 Even though over-the-counter topical anesthetic and antihistamine products such as pramoxine and doxepin, respectively, have been suggested to relieve pruritis in the general population, it is not known whether these agents will effectively manage EGFRI rash. Furthermore, topical antihistamines are skin sensitizers and should not be used long term in order to avoid secondary contact dermatitis.
Hair, Nail, and Eye Changes and Management
Hair changes may be seen with long-term administration of TKIs.71,81 It includes hypertrichosis (hirsutism), trichomegaly (abnormally long, curly eyelashes), thinning of the hair, and both scarring and nonscarring alopecia.
Facial hypertrichosis and trichomegaly appear after 1 to 2 months of treatment and persist as along as targeted therapy is continued. 81 Treatment of facial hypertrichosis may include the use of a topical eflornithine cream. Laser hair removal can be tried, but eflornithine combined with laser has better efficacy. Nonscarring alopecia may occur after 2 to 3 months of TKI treatment and usually presents in frontal patterns or patches. Alopecia may resolve spontaneously or after TKI discontinuation.
There is no specific recommendation for the prevention of alopecia. For nonscarring alopecia, topical minoxidil 2% solution for women or 5% solution for men applied twice daily has been effective in the general population; however, higher incidences of pruritis and hypertrichosis have been reported with higher strengths of minoxidil. 81 Caution is advised if these products are considered during EGFRI therapy. Overlapping skin toxicities with topical minoxidil in patients receiving EGFRIs may occur and needs further investigation. For scarring alopecia, topical hydrocortisone 0.2% and steroid shampoos are recommended to reduce inflammation.
The long-term use of EGFRIs may result in hypertrichosis and trichomegaly that may irritate the cornea. 81 Thick, curly, or misdirected lashes should be taken out to prevent corneal abrasions. Clipping of eyelashes every 2 to 4 weeks is recommended. They should not be bleached or plucked out. Recurrent misdirected lashes causing discomfort and irritation can be treated with diathermy by an ophthalmologist.
MKIs are known to lead to changes in hair color. Sunitinib may cause depigmentation and graying of hair, which generally appears after 5 to 6 weeks of treatment and is reversible after treatment discontinuation. 82 Sunitinib-induced hair depigmentation may be to the result of a blockade of stem cell factor or suppression of c-Kit signaling.
EGFRIs ay also cause paronychias or painful erythema, and pus around the nail beds of the finger and toes can occur. The nails become more delicate and tend to grow more slowly. Few recommendations to prevent paronychia are available. They include avoiding skin immersion in water, application of petroleum jelly to periungal areas frequently. Warm soaks with diluted bleach may help prevent the condition. 81 Treatment includes use of corticosteroid and calcineurin inhibitor (eg, pimecrolimus) topical creams. A systemic biotin supplement is suggested for brittle nails. Weekly cauterization with silver nitrate, electrodissection, and nail avulsion are used to eliminate excessive granulation tissue. If superinfection is suspected, the causative organism should be determined by culture and sensitivity testing and appropriate antibiotic treatment begun. In case of recurrent topical fungal infections of the toenails, patients should be asked to dispose of old slippers and shoes. Also, chemotherapy-related neuropathy can cause trauma and subsequent paronychia, so patients should be encouraged to use well-fitted shoes and sandals.
Hand-Foot Syndrome and Management
Hand-foot syndrome reaction (HFSR) is a significant problem associated with the TKIs axitinib, lapatinib, and also vemurafenib57,83 and the MKIs, sorafenib and sunitinib.84,85 It appears to be dose related with sorafenib but not sunitinib. HFSR is most common with lapatinib in combination with capecitabine and has an incidence of 53% (all grades), of which 12% is grade 3 (Table 8). 45
Incidence of Hand-Foot Syndrome With Targeted Therapies.
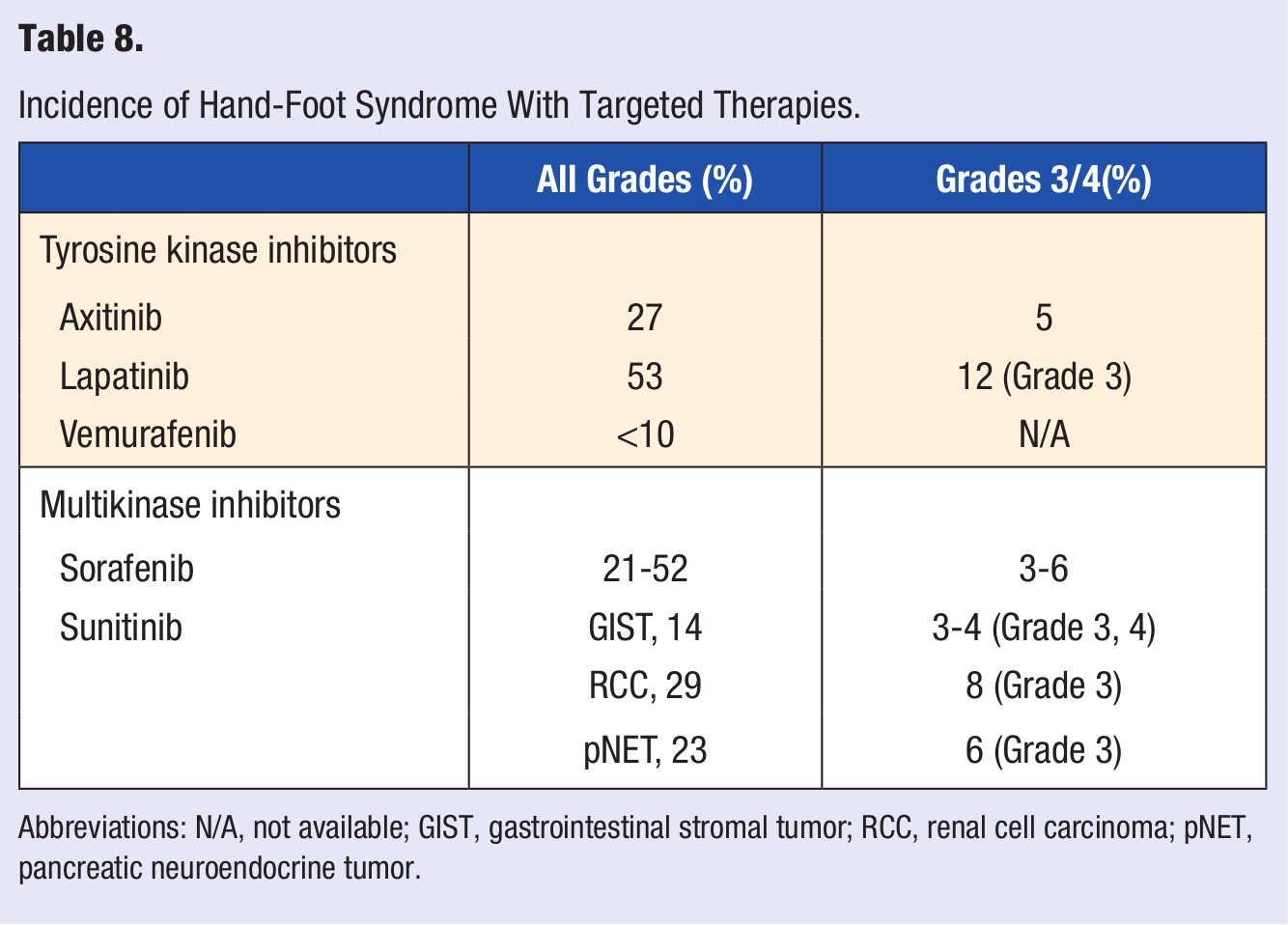
Abbreviations: N/A, not available; GIST, gastrointestinal stromal tumor; RCC, renal cell carcinoma; pNET, pancreatic neuroendocrine tumor.
The onset of HFSR usually occurs 2 to 12 days after initiation of therapy and may progress 3 to 4 days later into symmetrical edema and erythema of the palms and soles.84,85 Symptoms usually precede lesions and may include paresthesias, tingling, burning, and painful sensations on the palms and soles as well as decreased tolerance to contact with hot objects. The lesions are localized and tender and appear as blisters or hyperkeratosis in areas of trauma or friction on the soles of the feet and palms of the hand and sometimes on the elbows as well. The hyperkeratosis typically presents as yellowish, painful, hyperkeratotic plaques localized to the pressure sole areas (heels and metatarsals).
Grade 1 reaction presents with numbness, dysesthesia, paresthesia, tingling, painless swelling or erythema, and/or discomfort of the hands or feet not disrupting normal activities.68,86 Grade 2 reaction manifests as painful erythema and swelling of the hands or feet and/or discomfort affecting ADL. Grade 3 reaction develops as moist desquamation, ulceration, blistering or severe pain in hands or feet, or severe discomfort, preventing performance of ADL.
Prospective data for the prevention, assessment, and management of HFSR is lacking. Symptomatic management strategies and dose-reduction recommendations have been used.68,86 An effective way to manage HFSR on the palms and soles of the feet is the 3C approach: control calluses, comfort with cushions, and cover with moisturizing cream. Prevention includes removal of preexisting hyperkeratotic areas and calluses through a manicure and/or pedicure before treatment begins. Nonpharmacological interventions include advising patients to avoid undue pressure on or rubbing of the skin and to avoid blood vessel dilation induced by hot showers or sun exposure. An orthotic device is encouraged for patients with signs of abnormal weight bearing; also, constrictive footwear, excessive friction on the skin when applying lotions, massages, or performing everyday tasks such as typing or using handheld electronic devices should be avoided. Vigorous exercise that places undue stress on the palms and/or soles of the feet should also be avoided, particularly during the first month of therapy. Patients should be counseled to wear shoes with padded insoles to reduce pressure on the feet and to wear thick cotton gloves or socks to prevent injury and keep the palms and soles dry.
For mild (grade 1) symptoms, dose modification of the offending agent is not necessary. 86 For symptomatic relief, topical petrolatum-lanolin–based ointments, emollients, aloe vera lotion, and moisturizing creams may alleviate discomfort. Keratolytics, such as 20% to 40% urea-containing creams or lotions applied twice daily may be helpful. For grade 2 HFSR, treatment should continue as for grade 1 HFSR, with the addition of a topical corticosteroid to the erythematous areas twice daily. Long-term use of topical steroids should be avoided because they may increase the chance of infection. Topical analgesics such as lidocaine 2% may alleviate discomfort. If necessary, the dose of the offending agent should be reduced by 50% until the reaction reaches grade 0 to 1, then full dosing should be resumed. For severe (grade 3) symptoms, treatment should be provided as for grade 1 or 2 HFSR, with temporary discontinuation of the offending drug for at least 7 days until the grade of severity is reduced to 0 or 1. Treatment should be resumed at 50% of the usual dose. If toxicity does not recur, dose escalation can be attempted.
Diarrhea and Management
Dose-related diarrhea is also a common adverse effect of orally administered TKIs and MKIs (Table 9).87,88 It constitutes a significant problem, may be life threatening, and is unlikely to resolve on its own. It leads to decreased quality of life and increased emotional distress. The severity of diarrhea is graded on a scale of 1 to 4. Symptoms usually appear gradually within 7 to 10 days after starting TKI therapy. All other etiologies of diarrhea should be ruled out first before instituting pharmacological therapy. Grade 1 and 2 diarrhea indicate an increase in daily stool frequency of less than 4 and 4 to 6 stools, respectively. Grade 3 diarrhea indicates more than or equal to 7 stools per day, and grade 4 is diarrhea with hemodynamic compromise.
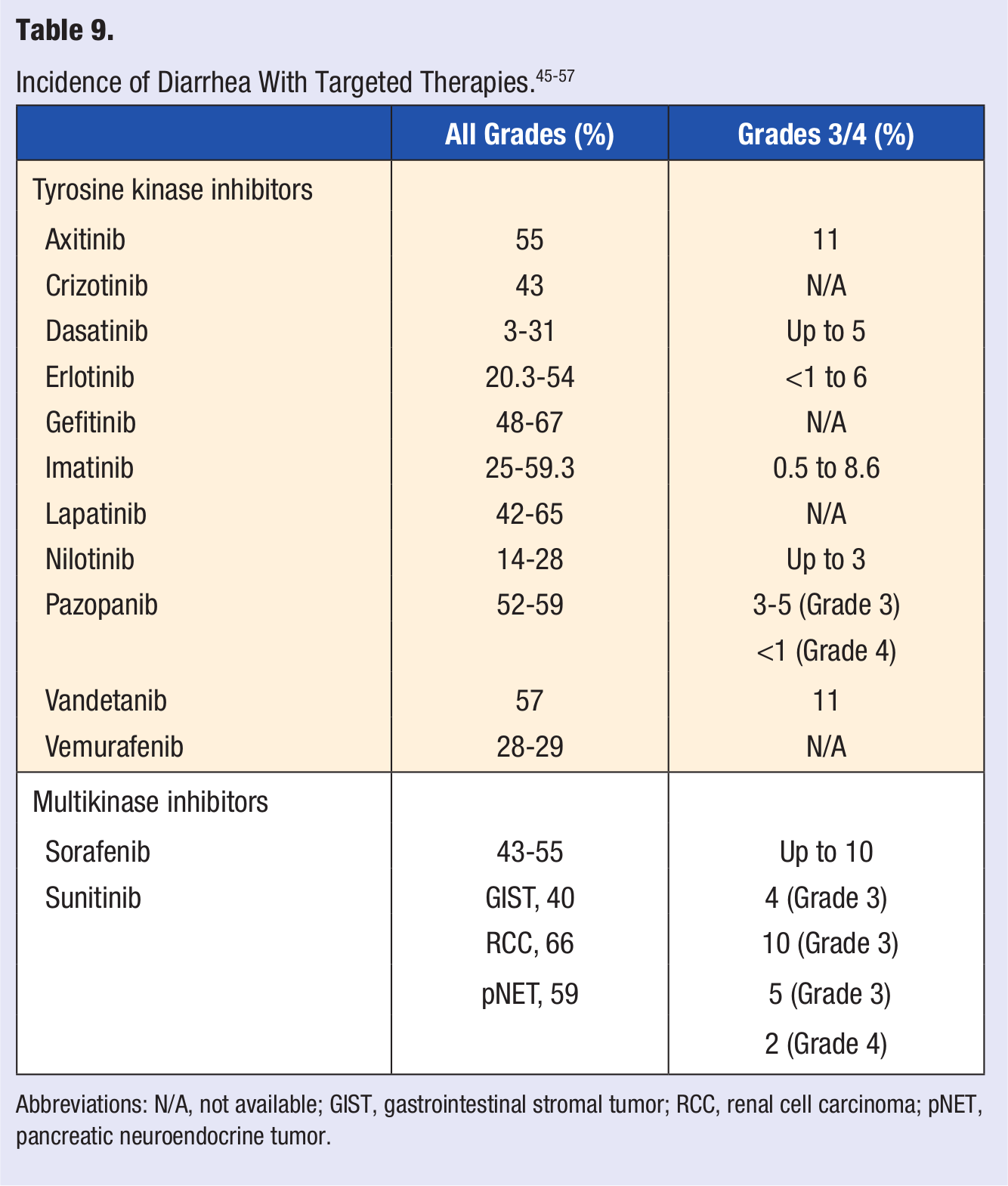
Abbreviations: N/A, not available; GIST, gastrointestinal stromal tumor; RCC, renal cell carcinoma; pNET, pancreatic neuroendocrine tumor.
Although specific guidelines for diarrhea are lacking, general management strategies include dietary counseling, dehydration management, pharmacological treatment, and dose reduction of the targeted therapy. Patients should be counseled to increase fluid intake (eg, water, sports drinks, diluted fruit juice, and broth) and keep a diary to note the frequency and severity of diarrhea and report them. Foods that may lead to diarrhea include caffeinated, carbonated, or heavily sugared and alcoholic beverages; fruit juices with pulp; high-fiber and high-fat foods; hot or heavily spiced foods; and dairy products and should be avoided. To slow gastrointestinal motility, a BRAT diet (bananas, rice, applesauce, and toast) can be used. Management 74 of grade 1 diarrhea includes adjusting diet and low-dose loperamide, whereas, for grade 2, high-dose loperamide is recommended. Severe grade 3 and 4 diarrhea require stopping the offending drug until symptoms resolve, with a dose reduction after interruption. 89 Uncontrolled diarrhea can lead to severe dehydration and electrolyte imbalances requiring hospitalization for intravenous fluid and electrolyte replacement. For nonresolving grade 3 and 4 or complicated diarrhea, loperamide should be discontinued, and more aggressive management with a second-line antidiarrheal agent, octreotide, along with intravenous fluid/electrolyte replacement and antibiotics should be instituted until diarrhea is controlled.
Upper-Gastrointestinal Side Effects and Management
A bothersome side effect of targeted therapy could be painful inflammation of the mucous membranes of the whole digestive tract, known as mucositis; that of oral mucous membranes is called stomatitis. These painful lesions, although not life threatening, may interfere with the ability to chew or swallow and result in taste changes or loss of appetite. 90
Mucositis occurs with the MKIs, sorafenib and sunitinib. EGFR inhibitors, lapatinib and erlotinib, that target HER2 have also been associated with stomatitis when the agents are given in combination with chemotherapy.90-92 Management options include palliative care such as mouth care consisting of salt and/or baking soda gargles, topical analgesia (lidocaine), and systemic analgesics. Patients should be counseled to eat lukewarm, nonirritating foods, avoid alcohol-containing mouthwashes, and brush with a soft toothbrush. Switching to plastic cutlery may help. Dose interruption or dose reduction of the offending agent may be considered in severe cases of mucositis.
Another recognized adverse effect of targeted therapy is nausea and vomiting. Patients may complain of uncomfortable, unpleasant feelings in the back of the throat or in the stomach that may or may not result in vomiting, which usually limits appetite, and are rated as a high concern for patients.92,93 Patients should be advised to stay well hydrated and to eat small amounts during the day. To prevent nausea and vomiting, patients should be asked to avoid strong odors; not to lie flat after eating; to avoid sweet, salty, fatty, spicy and heavy foods as well as citrus and tomatoes; and not to exercise after eating. They should also limit sights, sounds, and smells that precipitate vomiting.
The best way for patients to manage nausea and vomiting is staying hydrated, eating before getting too hungry, and eating bland food at cold or at room temperatures. Counsel patients to seek fresh air when possible. 63 They should try peppermint or ginger tea, sports beverages, ice chips or popsicles and apply cool compresses to the forehead, neck, and wrists. Keeping a diary to identify triggers may help. Listening to music, using relaxation techniques, pressure point biofeedback, and aromatherapy may also help. Antiemetic medications such as ondansetron may be prescribed. A trial of hypnosis or acupuncture may also be considered in selected patients who have debilitating symptoms. If nausea and vomiting continue, lowering the dose of treatment medication may help.
Myelosuppression and Management
Myelosuppression effects of neutropenia and thrombocytopenia are 2 important adverse effects to monitor while patients are on TKIs.94,95 Myelosuppression may also result from active disease, concurrent medications, or comorbid conditions. Complete blood count should be monitored with differential and hemoglobin every 1 to 2 weeks for 2 months, then monthly, to rule out evidence of myelosuppression. For grade 3 or 4 toxicity, withholding the causative drug usually reverses myelosuppression within several days. The drug can be reintroduced without dose reduction. If myelosuppression recurs, the dose can be reduced. Infections should be managed promptly. Neutropenia is usually seen with TKIs that target the BCR-ABL (breakpoint cluster region-Abelson oncogene) fusion protein found in leukemia. Therefore, it is only a concern with dasatinib, imatinib, and nilotinib.
Clinical trials have shown a higher frequency of neutropenia in patients with more advanced leukemia.94,95 This effect is most likely a result of the disease rather than a result of the drug’s direct cytotoxic effect on neutrophil progenitor cells. Additionally, phase I studies with imatinib observed a dose-related relationship with neutropenia; therefore, patients should expect close monitoring of their white blood cell count to be used to adjust their dose if necessary. The greatest concern with neutropenia is infection. Inform patients to report symptoms of fatigue, low energy levels, inability to do regular activities, shortness of breath, or chest pain with activity. Other symptoms to monitor include fever and shaking chills, dizziness or fainting, redness or swelling of skin or open wounds, or respiratory symptoms such as cough or sinus congestion. Counsel patients about thorough hand washing to reduce contact exposure, avoiding crowds, and potential contagion use of a face mask as instructed. In severe cases, hematopoietic growth factors or colony stimulating factors, such as granulocyte colony stimulating factor and granulocyte-macrophage colony stimulating factor may be indicated.
If anemia develops, treatment may include iron, folate, or vitamin B12 replacement therapy. Energy-sparing activities and a reduced dose of the antineoplastic may control symptoms. Thrombocytopenia is another serious side effect of therapy. 96 Platelet count less than 50 000/mm3 is considered grade 3 and 4 thrombocytopenia. Interrupting the dose until the platelet count is ≥50 000/mm3 is recommended. Gingival bleeding is most commonly caused by thrombocytopenia. Bleeding usually resolves rapidly as platelet counts increase following the hematological nadir. Patients may need a platelet transfusion at signs of bruising or bleeding or before any necessary invasive procedure. Patients should be counseled to report any frequent or large bruises, blood in the urine or stool, spontaneous nosebleeds, small red or purple spots on the body, or bleeding that does not stop with pressure. To reduce the risk of bleeding, patients should be informed that they should not take aspirin or nonsteroidal anti-inflammatory drugs unless instructed and to avoid activities that can cause bruising or bleeding such as contact sports and heavy lifting.
Hypertension and Management
MKIs are known to cause hypertension. The mechanism of action associated with MKI-induced hypertension is not completely known. It may be a result of abnormal endothelial function from Raf kinase inhibition and angiogenesis as a result of inhibition.97,98 The incidence of hypertension with sorafenib is 9% to 17%, grades 3 and 4, 3%; and for sunitinib, it is 15% to 34%, grade 3, 0% to 13%.51,52 A risk factor for cardiac toxicity is uncontrolled hypertension.86,91,97,98 Before starting these agents, a baseline blood pressure of less than 140/90 mm Hg is recommended. Patients should be counseled to routinely monitor their blood pressure at home and report any changes as soon as they occur. Hypertension usually occurs within the first 6 weeks after initiation of therapy. Blood pressure should be monitored weekly during the first 6 weeks of treatment. Interruption and/or dose reduction should be considered for persistent hypertension. Permanent discontinuation of MKIs is rare. Standard antihypertensive agents can be prescribed for uncontrolled hypertension. However, antihypertensive agents that are strong enzyme inhibitors, with the potential for CYP3A4 drug-drug interaction (eg, diltiazem and verapamil), should be avoided with MKIs.
The newest TKI approved in 2012, axitinib, 52 is also associated with hypertension. The incidence of hypertension with the drug is 40%, grades 3 and 4, 5%. Hypertension has also been reported with pazopanib 55 and vandetanib. 56
Fluid Retention and Management
The overall incidence of generalized edema is usually <10% and appears to be dose related. All the TKIs are prone to cause edema; however, it is more often seen with crizotinib, dasatinib, erlotinib, imatinib, and nilotinib as well as the MKI, sunitinib.44,58,59 Patients should be instructed to monitor weight daily and report any sudden changes. The addition of a diuretic may be needed for the management of early signs and symptoms of fluid retention and hypertension.
Interstitial Lung Disease (ILD) and Management
Perhaps the most dangerous, potentially fatal, adverse effect associated with the TKIs is ILD. The incidence is less than 1% and has been reported with dasatinib, erlotinib, gefitnib, imatinib, laptinib, and vandetanib.45,47,56,68,99,100 The mechanism for this adverse effect is not clearly understood, but it is thought that tyrosine kinases play an important role in repairing lung damage. Inhibiting their pathway would allow patients to become more susceptible to acute lung injuries. ILD presents with shortness of breath or nagging cough and may also lead to pneumonitis or pulmonary fibrosis.
Patients should be counseled to report the first signs of shortness of breath or cough and to seek medical attention immediately.68,69 In the presence of worsening dyspnea or interstitial infiltrates on radiographic chest X ray, the offending agent should be discontinued and diuretics such as furosemide and spironolactone prescribed. Anecdotal evidence suggests that a course of corticosteroids may be beneficial. If pleural effusions are symptomatic or require supplemental oxygen, a thoracentesis may be indicated. Patients with preexisting lung comorbidities are at increased risk of drug-induced ILD, and careful assessment of clinical respiratory symptoms and radiographic findings should be performed in the first 1 to 2 months of treatment.
Laboratory Abnormalities and Management
All the following agents may lead to clinically significant laboratory abnormalities: dasatinib, imatinib, lapatinib nilotinib, pazopanib, and vandetanib.45,48-50,55,56 A basic metabolic panel should be evaluated prior to administration of anticancer treatment and periodically during treatment. Electrolytes should be replaced accordingly, especially in patients at risk for or suffering from dehydration, diarrhea, or ECG changes such as QT interval prolongation.
Hepatotoxicity is also a concern specific to the BCR-ABL inhibitors dasatinib, imatinib, and nilotinib. It has also been reported with axitinib, erlotinib, lapatinib, and pazopanib and the MKIs, sunitinib and sorafenib.51,55,69,86 The FDA has added a black box warning for sunitinib and pazopanib regarding the risk of hepatotoxicity. Elevations in bilirubin and other liver function tests have been associated with these drugs in clinical trials. It is important to monitor liver transaminases at baseline and at routine intervals during therapy. Fatalities from drug-induced liver failure have been reported.101,102 Patients should be asked to report any abdominal pain, yellowing of skin, and fatigue. Furthermore, the concomitant use of acetaminophen is generally not recommended because of the increased potential for liver toxicity. Withholding the causative agent may improve liver function test abnormalities and avoid hepatotoxicity.
QT Interval Prolongation and Management
The MKIs and TKIs have been reported to lead to QT interval prolongation.55-57,77,86,103 These agents should be used with caution in patients at risk or taking an antiarrhythmic such as disopyramide, procainamide, quinidine, amiodarone, dofetilide, ibutilide, sotalol, and bepridil. Drugs such as chloroquine, fluoroquinolones, haloperidol, tricyclic antidepressants, selected phenothiazines, and other medications that may lead to QT interval prolongation should be used with caution. An ECG should be performed at baseline, again by 1 week of therapy, then periodically. Discontinuation of the causative agent is recommended.
Arthralgias/Mylagias and Management
Muscle cramps affecting calves, feet, and hands are the most bothersome long-term adverse effects associated with imatinib. 104 Muscle cramps are rarely seen with other TKIs. Incidence of arthralgia has been reported to be as high as 53% to 67% with vemurafenib. 57 Hypophosphatemia and hyperphosphaturia has been reported in some patients with muscle cramping taking imatinib. It is not known if the drug may ultimately affect bone metabolism because no increase in fracture risk has been reported. Monitoring serum calcium, phosphorus, and vitamin D concentrations is recommended. Although there is no definitive treatment, a trial of calcium or magnesium supplements or quinine may be helpful to mitigate muscle cramping.
Part 4: Nonadherence Rates Related to Adverse Drug Reactions With Targeted Therapies
Patients have a right to make their own health care decisions, and if they do not take their medicine as prescribed, this should be an informed decision. They should be educated regarding coping and adjusting with anticancer targeted therapies and knowing and understanding the ramifications of medication nonadherence. 105 Patient-focused education about their therapy such as written take-home information, diaries, guidelines for identifying and reporting side effects, a strategy to manage adverse events, and appropriate treatment interventions and frequent contact with health care providers are especially important in the initial stages of therapy, especially with respect to the identification and management of toxicities, patient education, and patient support. Strategies to improve tolerability of therapy with appropriate side-effect management and easing patients’ concerns about side effects may help improve adherence.
Adverse drug effects have generally been shown to lead to nonadherence in various chronic diseases. 106 Few published studies have focused on the impact of adverse effects associated with targeted therapies on adherence rates. Furthermore, few studies of cancer patients have evaluated the relationship between adherence rate and achievement of the treatment goal. 11 Marin et al 11 conducted a prospective study to determine whether imatinib adherence correlated with the degree of molecular response in patients with chronic myeloid leukemia (CML). An adherence rate of less than or equal to 90% as measured by MEMS was considered nonadherent in the clinical trial. Out of 87 patients, 23 (26.4%)were nonadherent to imatinib. The investigators concluded that patients taking less than 90% (missing 3 doses in a month) of their imatinib doses had an adverse effect on their cytogenic and molecular responses, which could ultimately affect long-term outcomes. The study showed that adherence is the critical factor for achieving complete cytogenetic responses from imatinib in CML. Adherence rates were lower in patients with side effects—asthenia, nausea, muscle cramps, and bone and joint pain—and suggest that common adverse effects of imatinib therapy negatively influence medication adherence.
Out of the 23 nonadherent patients in the Marin trial, 21 were evaluated in a subsequent study by Eliasson et al. 107 The investigators determined the reasons for the patients not adhering to oral therapy with imatinib through in-depth interviews with those taking imatinib for CML. The authors found that the most common intentional reason for patients to decide to miss doses was the hope of minimizing adverse effects (to deal with side effects), whereas the most common unintentional reason to miss doses was forgetfulness. Several patients believed that missing 3 or 4 doses per month (a few doses) was unlikely to affect their response to therapy, especially if they were told that they were doing well and did not exhibit disease symptoms.
In 2011, Timmers et al 108 described a 16-week observational trial in BMC Cancer that is under way to study adherence with respect to erlontinib and the influence of adherence on its effectiveness in patients with non-small-cell lung cancer (NSCLC). The study’s primary objective was to evaluate the relationship between adherence and the plasma concentration of erlotinib and to study the relationship between adverse effects and adherence in patients with NSCLC. The secondary objective of the study was to explore the relationships between patient characteristics, disease characteristics, adverse effects, quality of life, patient beliefs and attitude toward disease and medicines, adherence, and dose adjustments and plasma concentrations of erlotinib in patients with NSCLC.
Interventions to promote oral antineoplastic adherence such as prevention, early detection, and management of common adverse effects associated with the oral targeted therapies have been reviewed. Strategies to promote medication adherence include patient counseling about their medications and adverse drug effect management. Regular access to oncologists, pharmacists, nurses, nutritionists, and social workers and periodic monitoring (pill counts, adherence questionnaires, and disease and laboratory monitoring) has been shown to improve patients’ adherence to medication. Only a small number of studies have investigated the impact of a multidisciplinary approach to oral antineoplastic adherence. This approach has been shown to improve medication adherence to anticancer medications.
Conclusion
Despite the advantages of the newer oral anticancer agents, they pose the problem of uncertainty with regard to adherence and a wide range of adverse drug effects. Adherence to oral targeted therapies can be a challenging commitment for many patients. Prevention, early detection, and optimal management of drug-related adverse effects are important. Minimizing the impact of toxicities on patients’ health should increase the likelihood that they will be able to tolerate additional lines of treatment. An organized, multidisciplinary approach involving physicians, nurses, pharmacists, nutritionists, and social workers to educate patients about their cancer therapy may help them cope with drug-related adverse effects and adhere to targeted therapies.