
Abstract
Photosensitivity is a condition that occurs when sunlight or artificial forms of radiation interact with a medication to produce an adverse cutaneous drug eruption. This adverse reaction may increase the incidence of skin cancer and can be prevented with proper counseling. There are 2 major types of photosensitivity: phototoxic reactions, which occur when an individual is exposed to both high doses of medication and radiation, and photoallergic reactions, which require an immune-mediated response. Several classes of drugs are commonly implicated in photosensitivity reactions, including tetracyclines, floroquinolones, sulfonamides, diuretics, phenothiazine antipsychotics, and nonsteroidal anti-inflammatory drugs. This review will discuss photosensitivity reactions, the most commonly reported photosensitizing agents, and treatment and prevention measures for the condition.
Photosensitivity is a condition that occurs when sunlight or artificial forms of radiation interact with a medication to produce an adverse cutaneous drug eruption. Clinical Pharmacology, a drug information database, reports more than 300 drugs associated with photosensitivity. 1 Photosensitive drug reactions make up about 8% of all reported cutaneous adverse drug events. 2 This adverse drug reaction is particularly important because it has the potential to increase the incidence of skin cancer and can be prevented with proper patient counseling. This article will describe photosensitivity reactions and discuss the most commonly implicated photosensitizing medications.
This adverse drug reaction [photosensitive drug reaction] is particularly important because it has the potential to increase the incidence of skin cancer and can be prevented with proper patient counseling.
Adverse Photosensitivity Reactions
Drug-induced photosensitivity reactions can occur through 2 different mechanisms: phototoxic reactions and photoallergic reactions. It is difficult, and sometimes impossible, to determine which type of reaction caused the cutaneous change. However, regardless of the type of reaction, treatment for the condition is the same.
Phototoxic reactions are the most common type of drug-induced photosensitivity. In a phototoxic reaction, ultraviolet radiation converts drug within the skin to a toxic substance. There are no immunologic mechanisms involved. Phototoxic reactions occur in everyone exposed to both high doses of medication and radiation at appropriate wavelengths. 3
Phototoxic reactions occur more rapidly than photoallergic reactions. 4 A phototoxic reaction produces an immediate exaggerated sunburn with edema, a burning sensation, and erythema. The cutaneous changes generally occur only on areas of skin exposed to sunlight.
Photoallergy reactions are less common than phototoxic reactions. They are also less predictable as they do not occur in all individuals exposed to the drug and radiation. Photoallergic reactions require an immune-mediated response. In photoallergic reactions, ultraviolet radiation causes a drug to become an antigen, which subsequently triggers an allergic response to sunlight.
Unlike phototoxic reactions, which occur only on sun-exposed skin sites, photoallergy reactions can cause cutaneous changes in unexposed areas. 5 Clinically, patients with photoallergic reactions present with cutaneous changes that are more eczematous in nature than phototoxic reactions. Additionally, unlike the rapid response seen in phototoxic reactions, photoallergy reactions generally do not appear until 24 to 72 hours after exposure to the sun. 6
Diagnosis
Diagnosing drug-induced photosensitivity in the practice setting relies predominantly on a detailed clinical history. However, there are 2 tests that exist to aid in diagnosis and may even assist in distinguishing phototoxic reactions from photoallergic reactions.
Phototesting works by exposing an individual to artificial radiation on 2 separate occasions, once while taking the suspected photosensitizing medication and once while not taking the medication. When minimal erythema is noted, the dose of artificial radiation is documented and compared between exposures. If the dose of artificial radiation necessary to cause erythema is less while taking the medication than while off the medication, drug-induced photosensitivity is indicated.
Photopatch testing can also be used to diagnose drug-induced photosensitivity. In photopatch testing, 2 topical applications of the suspected medication are placed on an individual’s back. After 24 hours, one of the patch sites is radiated below the dose known to cause minimal erythema. This low dose of radiation is less likely to cause phototoxic reactions and more likely to implicate photoallergic reactions. Patches are compared 24 hours after radiation. If only the irradiated site has erythema, this is suggestive of drug-induced photosensitivity. If both sites display erythema, it is suggestive of allergic contact dermatitis from the medication.
Incidence
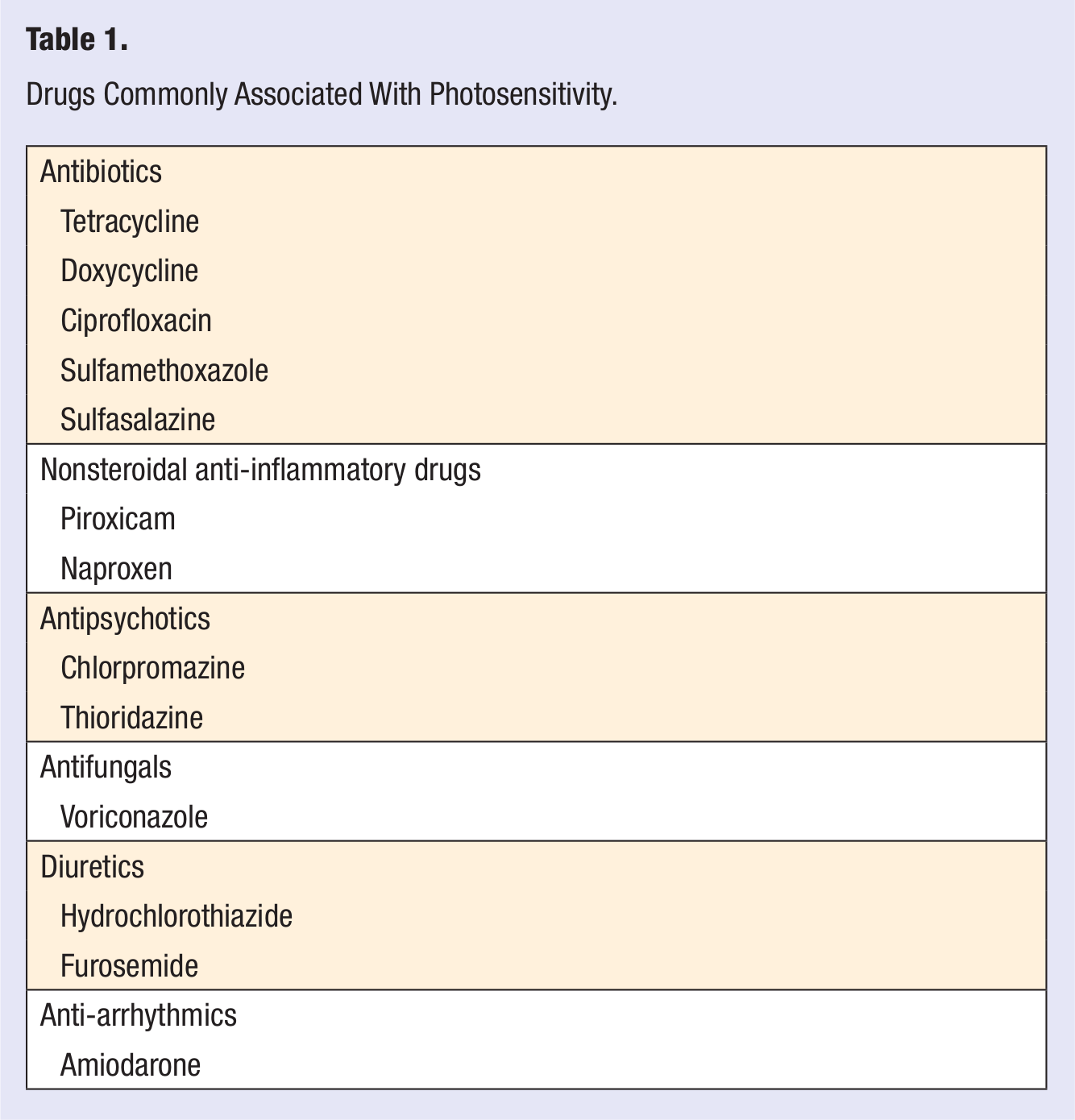
The incidence of drug-induced photosensitivity is difficult to determine and could be underestimated. Among the reasons for this is the difficulty in distinguishing a mild drug-induced photosensitivity reaction from a mild sunburn. There are also problems with the reporting system for adverse drug events. The first being significant underreporting. 7 Adverse drug events are more likely to be reported for drugs new to the market but less so for those that have been on the market for some time, especially those known to cause photosensitivity. For this review, drugs considered major culprits are those that have been more frequently reported to cause drug-induced photosensitivity in the literature and those considered potent photosensitizers by expert opinion.3,8,9 Drugs considered major culprits of photosensitivity are listed in Table 1. Medications implicated in photosensitivity but no longer in use therapeutically, topical agents, and medications whose mechanism of action rely on photosensitivity (ie, psoralens) are not included in this review.
Drugs Commonly Associated With Photosensitivity.
Photosensitizing Agents
Several agents used to treat infectious disease have been implicated in photosensitivity. Among the various classes of antimicrobials, tetracycline, sulfonamides, and floroquinolone antibiotics seem to be the most potent photosensitizers. 9 Within the tetracycline class, tetracycline and doxycycline are considered photosensitizing, while minocycline is not generally associated with cutaneous photosensitivity. 10 Ciprofloxacin is the floroquinolone with the greatest reported potential for photosensitivity, while levofloxacin and moxifloxacin have low phototoxic potential.11,12 Among the sulfonamides, sulfasalazine and sulfamethoxazole are most often implicated in photosensitivity. 8 Although sulfasalazine is used to treat ulcerative colitis and rheumatoid arthritis, it consists of mesalamine (a salicylate) and sulfapyridine (a sulfa antibiotic) and thus included here. In the antifungal class, voriconazole is the major culprit of photosensitivity, predominantly manifesting as a phototoxic reaction. 13
Nearly all nonsteroidal anti-inflammatory drugs (NSAIDs) have been shown to cause inflammation when combined with ultraviolet radiation. 14 However, not all NSAIDs require routine counseling and prevention from photosensitivity. Piroxicam has the most reported photosensitivity within the class, and naproxen is also frequently implicated. 8 Ibuprofen has only 1 documented report of photosensitivity and is generally not considered a culprit drug. 15
Several antipsychotic medications cause photosensitivity, most commonly the phenothiazine antipsychotics chlorpromazine and thioridazine. Both agents cause immediate photosensitivity reactions, confirmed by photopatch testing. In addition to immediate photosensitivity, long-term administration of either agent has been shown to cause a gray-colored hyperpigmentation distributed in areas exposed to sunlight. 16
Cardiac drugs have also been shown to cause photosensitivity. Amiodarone is a well-documented photosensitizing agent. Immediate reactions with burning, tingling, and erythema have occurred as well the distinctive blue-gray photodistributed hyperpigmentation associated with long-term use. 17 Diuretics are also commonly implicated in photosensitivity, particularly the thiazide diuretic hydrochlorothiazide and the loop diuretic furosemide.18,19 Hydrochlorothiazide has been found to cause chronic eczematous photosensitivity that can last months to years after discontinuation of the drug. 20 Photosensitivity with furosemide treatment generally occurs with very high doses of medication. 19
Management
Many drug-induced photosensitivity responses can be avoided with proper preventive measures. Patients should be counseled about increased sun-sensitivity when a known potent photosensitizing agent is prescribed. Avoidance of sun and tanning beds, protective clothing (eg, long sleeve shirt, hat, sunglasses), and the use of sunscreen may all decrease the incidence of this adverse effect.
Treatment of drug-induced photosensitivity includes the discontinuation of the causative agent and avoidance of sun exposure. If the reaction is mild, soothing creams and gels can be used to help with the burning sensation. Pain associated with mild reactions typically subsides within 24 to 48 hours of onset. Depending on the severity of the eruption, topical or systemic corticosteroids can be used. If discontinuing or substituting the offending agent is not an option, preventive measures (as described previously) should be discussed and implemented.
Conclusion
Although many agents are associated with photosensitivity, only a few warrant routine counseling and preventive measures. Medications considered potent photosensitizers include tetracycline, doxycycline, ciprofloxacin, sulfasalazine, sulfamethoxazole, voriconazole, piroxicam, naproxen, chlorpromazine, thioridazine, amiodarone, hydrochlorothiazide, and furosemide. Prevention of photosensitivity reactions includes avoidance of ultraviolet radiation and the use of sunscreen and other protective clothing. Treatment of drug-induced photosensitivity involves discontinuation of the offending agent, avoidance of sun exposure, and corticosteroids if needed.