
Abstract
Ultraviolet radiation (UVR) has many interactions with the skin, which are explored in detail in this review. Both ultraviolet A (UVA) and ultraviolet B (UVB) wavelengths are absorbed by chromophores in the skin, resulting in important biologic effects. Exposure to UVR can result in sunburn, immediate and delayed skin pigmentation, photoaging, and immunosuppression. In addition, exposure to UVA and UVB is an important risk factor for melanoma, squamous cell carcinoma, and basal cell carcinoma. Because endogenous vitamin D synthesis requires UVB, concerns have been raised about the possibility that photoprotection might contribute to vitamin D deficiency; however, vitamin D supplementation is a safer and more reliable method for maintaining adequate vitamin D levels than UVR exposure. Protection from UVR is critical and involves several factors. These elements include sun avoidance during peak hours of UVR exposure (10
Interactions between ultraviolet radiation (UVR) and the skin are complex and manifold. Certain issues associated with the relationship between UVR and the skin, such as vitamin D deficiency, indoor tanning, sunscreen labeling changes, and the effects of UVR on melanoma incidence, have recently been topics of interest in the media and in medical journals. Other topics, such as nonmelanoma skin cancer, have not garnered as much recent media attention but remain of importance given their common clinical occurrence. This review summarizes many of the most frequently encountered effects of UVR on the skin, including sunburn, pigment alteration, immunosuppression, and nonmelanoma and melanoma skin cancers. The relationship between UVR and vitamin D levels is also reviewed. Last, methods of sun protection and the hazards of indoor tanning are discussed.
The response of skin to UVR [ultraviolet radiation] varies in patients with different skin colors. . . . Skin type I is the lightest in color and is most susceptible to UV-induced erythema, whereas skin type VI is the darkest and least sensitive to sunburn.
Ultraviolet Radiation and Chromophores
Ultraviolet radiation is divided into 3 categories based on wavelength: UVC (270-290 nm), UVB (290-320 nm), and UVA (320-400 nm). UVA is further subdivided into UVA2 (320-340 nm) and UVA1 (340-400 nm). Although all the 3 types of UVR are emitted by the sun, only UVA and UVB reach the earth’s surface, because UVC is absorbed by nitrogen and oxygen molecules in the ozone. At the earth’s surface, UVA is present in much higher quantities than UVB (20:1), and because of its longer wavelength, UVA can penetrate more deeply into the skin than UVB. 1 In addition, unlike UVB, most UVA is not filtered by window glass.
For UVR to have a biological effect on the skin, it must be absorbed by molecules in the skin called chromophores. There are many chromophores in the skin, and each absorbs a specific spectrum of electromagnetic wavelengths. Studies have demonstrated that DNA is a major chromophore in human skin for erythema induced by UVB and short UVA wavelengths.2-4
The response of skin to UVR varies in patients with different skin colors. Dermatologists frequently classify patients into 1 of 6 skin type categories based on the Fitzpatrick scale. Skin type I is the lightest in color and is most susceptible to UV-induced erythema, whereas skin type VI is the darkest and least sensitive to sunburn. The Fitzpatrick skin types are summarized in Table 1. 5
Fitzpatrick Skin Types.
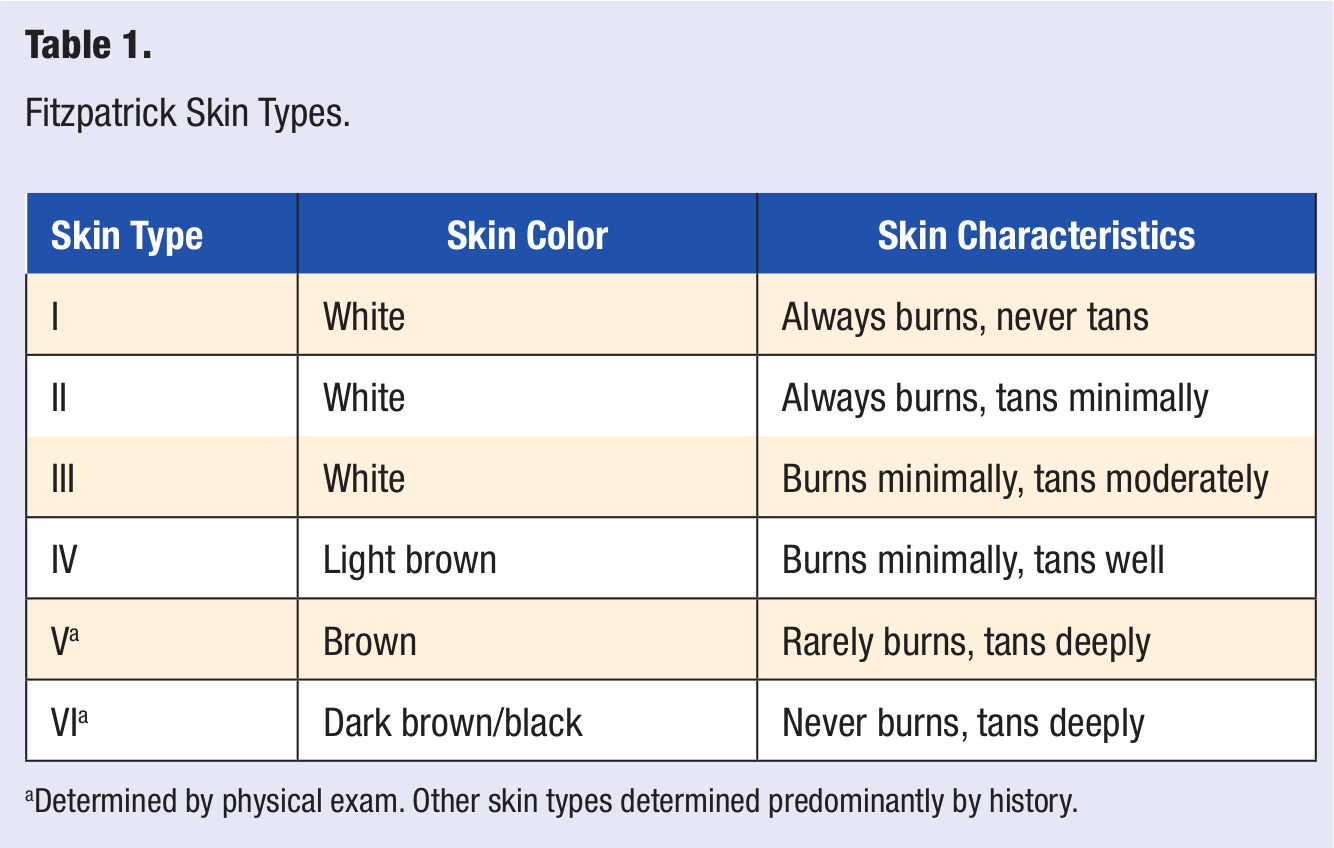
Determined by physical exam. Other skin types determined predominantly by history.
Sunburn
Sunburn manifests clinically as erythema, which is often followed by desquamation. Edema and blisters may occur with more severe sunburns. Erythema typically develops approximately 3 to 5 hours after exposure to the sun, peaks in 12 to 24 hours, and gradually fades over several days. 6 However, in individuals with fair skin, immediate erythema may be observed after UVB exposure, and the erythema can last up to 2 weeks. 3 It is known that the intensity of erythema resulting from exposure to UVR in the UVA and UVB range (290-400 nm) depends on wavelength, with shorter wavelengths producing erythema more effectively. UVA is separated into UVA2 (320-340 nm) and UVA1 (340-400 nm) because, due to its shorter wavelength, the biologic properties of UVA2 (such as effectiveness at producing erythema) are closer to those of UVB (290-320 nm). Because of the inverse relationship between wavelength and the intensity of erythema generated, solar UVB is the primary cause of sunburn, with UVA2 contributing to a lesser extent. In fact, it has been shown that UVB is 1000 times more erythemogenic than UVA. 7
Absorption of UVB by DNA in the skin leads to cyclopyrimidine dimers and pyrimidine pyrimidone photoproducts, which ultimately results in an inflammatory response consisting of vasodilation and increased vascular permeability. 8 UVB also causes erythema by increasing prostaglandin E2 synthesis and nitric oxide production. 9 Other inflammatory mediators thought to play a role in the sunburn reaction include lipoxygenase products; cytokines, such as tumor necrosis factor–α; adhesion molecules; reactive oxygen radicals; and mast cell–derived mediators, including histamine. 10
The most studied medications for sunburn symptoms are nonsteroidal anti-inflammatory drugs (NSAIDs) and topical corticosteroids. Both are mechanistically attractive options because of their anti-inflammatory properties, but studies of these medications have not demonstrated convincing evidence of substantial clinical benefits for sunburn prevention or treatment. Oral and topical NSAIDs have shown mild effectiveness in the prevention and treatment of UVB-induced erythema in clinical trials, 10 but the NSAIDs were started before or immediately after UVB exposure in almost all the studies, which limits the clinical applicability. One interesting double-blind randomized controlled trial showed a statistically significant decrease in pain and erythema in the treatment group relative to controls when diclofenac sodium 0.1% gel was administered 6 and 10 hours after exposure to a standardized dose of sunlight, 11 but further studies are needed to confirm this result. Although topical corticosteroids are widely used to treat sunburn, there is minimal evidence in the medical literature to support this practice. Most clinical trials examining the use of topical corticosteroids after UVB exposure have shown minimal or no clinical improvement in the sunburn reaction.6,10 In one controlled clinical trial, twice daily application of moderate potency topical corticosteroids starting 6 hours after UVB exposure and continued for up to 1 week did result in clinical improvement that was statistically significant on days 4 and 5. 12 Given the weak data supporting the clinical effectiveness of topical corticosteroids and NSAIDs in patients with sunburn, symptomatic treatment with conservative therapies such as cool compresses and soothing emollients is frequently the most appropriate management option.
Skin Pigmentation
Exposure to UVR can cause both transient pigment changes and longer lasting delayed tanning. Immediate pigment darkening, which occurs with exposure to UVA and some short wavelengths of visible light, has a grayish color and occurs immediately after UVA exposure, lasting 10 to 20 minutes. 3 With higher doses of UVA, persistent pigment darkening occurs, which appears darker brown in color and lasts from 2 to 24 hours. Both immediate and persistent pigment darkening are due to oxidation of preexisting melanin and melanin precursors and metabolites.
Delayed tanning, which begins approximately 72 hours after UVR exposure, occurs with exposure to both UVA and UVB. 3 With delayed tanning, the number and activity of melanocytes are increased. More specifically, there is increased melanocyte tyrosinase activity (rate-limiting enzyme in melanin synthesis), elongation and branching of melanocytes, increased size and number of melanocytes, and increased transfer of melanosomes from melanocytes to keratinocytes. It should be noted that UVB-induced tanning is always preceded by erythema, whereas perceptible erythema may not always occur before UVA-induced tanning. A common misconception is that obtaining a tan helps protect against sunburn.13,14 However, tanning provides minimal photoprotection. On average, a UVB-induced tan affords a sun protection factor (SPF) of 3, and a visually identical UVA-induced tan results in an SPF of 1.4. 15 Another frequent misconception is that tanning is safe as long as no sunburning occurs, but because UV-induced DNA damage is part of the molecular mechanism of tanning, “safe tanning” is an oxymoron.14,16
Ultraviolet Radiation and Skin Cancer Pathogenesis
In 1992, UVR from the sun was classified as a carcinogen by the International Agency for Research on Cancer. 17 DNA is a chromophore for UVB radiation, and absorption of UVR by DNA results in DNA damage. Absorption of UVB by DNA results in the formation of 2 types of photoproducts. Cyclobutane pyrimidine dimers result from covalent binding of carbon atoms at the C5 and C6 positions of adjacent pyrimidines, and pyrimidine 6-4 pyrimidone photoproducts are formed by covalent binding between the C6 ad C4 positions of adjacent pyrimidines. 18 Ideally, these photoproducts are repaired by cells, but when not repaired, C to T and CC to TT mutations occur. These mutations, which are known as the UV fingerprint mutations, are an initial step in the pathway to skin cancer.
The mechanisms underlying UVA-induced carcinogenesis are not as well understood. Unlike UVB, UVA is not well-absorbed by DNA, 19 but skin exposure to UVA generates reactive oxygen species, which results in production of the guanine oxidation product 8-oxo-7 8-dihydroguanine in much larger amounts than oligonucleotide strand breaks and oxidized pyrimidine bases. 20 8-Oxo-7, 8-dihydroguanine is one of the major promutagenic DNA lesions resulting from oxidative damage from a variety of sources and can result in G to T and C to A mutations.19,21 As with UVB, exposure to UVA also results in the formation of cyclobutane pyrimidine dimers, which likely also play an important role in UVA-induced carcinogenesis. 22
Notably, UVR can cause mutations directly in the p53 tumor suppressor gene. UV fingerprint p53 mutations are very common in basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) and are observed less frequently in melanoma.17,23
Immunosuppression
Ultraviolet radiation not only causes skin cancer by direct damage to DNA but also facilitates the growth of skin cancers by inducing a state of immunosuppression. Absorption of UVA and UVB by chromophores results in immune suppression via multiple pathways.24,25 Langerhans cells, the primary antigen-presenting cells in the skin, show a decrease in number as well as function in response to UVR. 25 When exposed to antigen, UV-irradiated Langerhans cells activate Th2 cells preferentially, resulting in activation of suppressor T cells and suppression of the immune response. Stimulation of the production of various cytokines, such as interleukin (IL)-1, IL-10, and TNF-α, and inhibition of cytokines, such as IL-12, also contributes to the immune suppression seen with UVR. In addition, UVR causes isomerization of urocanic acid to its cis isoform, which is an immune suppressant. Numerous other cells and molecules likely play a role in the multiple pathways of immune modulation induced by UVR. 24
Melanoma
Whereas the overall incidence of cancers tracked by the major cancer registries in the United States has decreased in the past several decades, numerous studies demonstrate a rapid increase in the incidence of melanoma over this time period.26-29 Based on estimates from the Surveillance, Epidemiology, and End Results database, there was an increase of more than 600% in the incidence of melanoma between 1950 and 2000. 30 The annual incidence of melanoma in the United States increased from 6.8 per 100 000 people in 1973 to 20.1 per 100 000 people in 2003 to 2007. 27 Over the past 2 decades, young women have shown the most pronounced increase in melanoma incidence. 31 The lifetime risk of melanoma has recently been estimated at 2.67% (1 in 37) for men and 1.79% (1 in 56) for women. 27 Incidence of melanoma increases with age, but almost one third of cases are in patients below 50 years of age. 32
Cutaneous melanoma classically presents as a pigmented lesion that exhibits features of the “ABCD” rule: asymmetry, border irregularity, color variegation, and diameter greater than 6 mm. Evolution of a pigmented lesion over time is also a feature that may be worrisome for melanoma. However, some melanomas, particularly nodular, desmoplastic, and amelanotic melanomas, may not show these classic features and can present a diagnostic challenge. Unlike nonmelanoma skin cancers, which very rarely metastasize, up to one fifth of melanoma patients develop metastatic melanoma, which is often eventually fatal. 33 Based on the American Cancer Society estimates for the year 2010, approximately 68, 130 people in the United States were diagnosed with melanoma, and 8700 died of the disease. 29
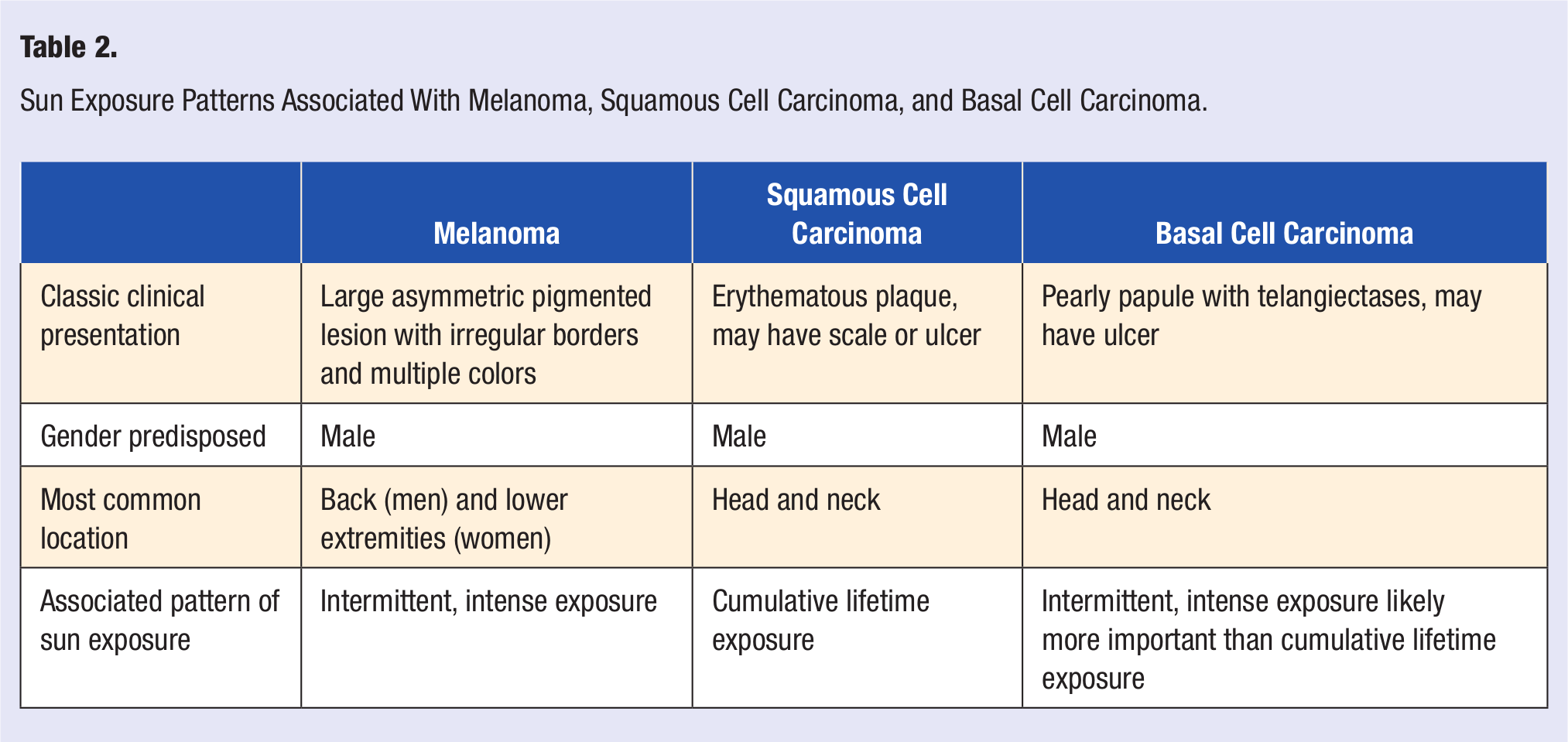
Ultraviolet radiation plays an important but complex role in the development of melanoma, and the nature of this role continues to be defined (Table 2). The incidence of melanoma in a particular geographic location correlates positively with the average amount of UVR. 27 Intermittent intense exposure to sunlight, rather than chronic exposure, appears to carry the highest risk for melanoma. 34 Although some studies have focused on childhood sunburns as a risk factor for melanoma, more recent studies indicate that sunburns at any age increase melanoma risk. A 2008 meta-analysis demonstrated an association between the risk of melanoma and increased number of sunburns, irrespective of whether the sunburns occurred in childhood, adolescence, or adulthood. 35 In a multicenter case–control study, more than 5 sunburns was associated with a 2-fold risk of melanoma, regardless of the age at which the sunburns occurred. 36 Recent data indicate that exposure to tanning beds is also associated with an increased risk of melanoma.37,38
Sun Exposure Patterns Associated With Melanoma, Squamous Cell Carcinoma, and Basal Cell Carcinoma.
The precise mechanism whereby a melanocyte is transformed into malignant melanoma remains to be elucidated, but UVR likely plays an important role by causing DNA damage in melanocytes and also possibly through immunosuppression. Certain gene mutations associated with melanoma, including CDKN2A and BRAF, are also important in melanoma pathogenesis. Activating mutations in BRAF, which encodes the serine/threonine protein kinase B-raf, cause constitutive activation of the MAP kinase pathway and are present in approximately 50% of melanomas. 39 Vemurafenib, an inhibitor of the most common BRAF mutant (BRAF V600E [valine at position 600 replaced by glutamine], which accounts for 90% of BRAF mutations in melanoma), was recently approved by the US Food and Drug Administration (FDA) and several regulatory agencies in Europe for the treatment of metastatic melanoma in patients harboring this mutation. Mutations in CDKN2A, which encodes 2 tumor suppressor proteins, p16 and ARF (p14), are associated with familial melanoma. 27 Interestingly, recent studies of melanomas have revealed UV fingerprint mutations in CDKN2A and other probable UVR-induced mutations in BRAF, providing evidence of a direct role for UVR in the mutagenesis of these important genes in melanomas.17,40,41
Squamous Cell Carcinoma
Cutaneous squamous cell carcinoma is a tumor of keratinocytes and is the second most common skin cancer, accounting for approximately 20% of nonmelanoma skin cancers. 42 The most common location for SCC is the head and neck, and 80% of cases occur in patients aged 60 or older. Males are affected more frequently than females. Patients typically present with firm, erythematous papules or plaques that may be smooth, scaly, or ulcerated and may cause bleeding, pain, and pruritus. The 5-year rate of metastasis for SCC is likely approximately 5%,42,43 but estimates of metastatic risk vary widely in the literature, and some subtypes of SCC carry a much higher risk of metastasis than others.44,45 Characteristics of SCC associated with a high risk for metastasis include location on the lip or ear and histopathologic features such as poor tumor differentiation or perineural invasion. 46
Although SCCs may arise de novo, many develop from actinic keratoses, which are considered to be SCC precursors. 45 Actinic keratoses present clinically as rough erythematous macules or papules that are often more easily identified by palpation than visual inspection. An individual actinic keratosis has only a small risk of progression to SCC, but treatment is warranted because it is not possible to determine which actinic keratoses will progress to invasive cancer. Furthermore, some actinic keratoses can be clinically indistinguishable from SCC, and biopsy may be required when a presumed actinic keratosis is not responding to standard treatment. Risk factors for SCC include exposure to UVR, fair skin, various genodermatoses, ionizing radiation, human papillomavirus infection, chronically inflamed skin (such as chronic ulcers), and immunosuppression (especially in the context of organ transplantation). 42 Interestingly, in contrast to the general population, organ transplant patients have more SCCs than basal cell carcinomas.
Exposure to UVR has been well-established as the most common and important cause of SCC. Whereas intermittent intense UVR exposure is associated with an increased risk of melanoma, cumulative lifetime UVR exposure is believed to be the primary determinant of SCC risk. 47 SCCs favor areas on the head and neck that have maximal sun exposure. 48 In addition, studies have demonstrated that SCC risk is higher in patients living closer to the equator, in patients with occupational light exposure, and in patients with higher estimated total cumulative solar exposure.49,50
Basal Cell Carcinoma
Basal cell carcinoma is the most common skin cancer, accounting for approximately 80% of nonmelanoma skin cancers. 42 BCC is also the most common malignant tumor in white populations. 51 Although BCCs may cause significant disfigurement via local tissue destruction, metastatic disease is very rare. The most common BCC subtype, nodular BCC, classically presents as a pearly papule with telangiectases, sometimes associated with a central nonhealing erosion or ulceration. Like SCCs, BCCs are most common on the head and neck of elderly patients, are more common in men than women, and more common in patients with fair skin. UVR, immunosuppression, and various genodermatoses are also risk factors. 52
As with SCC and melanoma, UVR exposure is a well-established risk factor for BCC. However, the pattern of sun exposure responsible for BCC development appears to be more complex than the exposure pattern associated with SCC. 51 Although BCC was classically believed to be associated with cumulative sun exposure like SCC, more recent studies indicate that intense intermittent UVR is the main risk factor for BCC (Table 2). As with SCC, the risk of BCC correlates with proximity to the equator, and BCCs occur most frequently in areas that receive the highest average amount of sun, such as the head and neck. However, BCCs are also associated with number of sunburns and recreational (intermittent) sun exposure during childhood and adolescence.51,53-56
Photoaging
Chronic exposure to UVR accounts for many of the age-associated changes seen in the skin. These changes are termed photoaging and include freckles, lentigines, leather-like coarseness, rhytides, inelasticity, purpura, and yellow-gray discoloration.33,57 Photoaged skin demonstrates changes in dermal connective tissue, with damaged and disorganized collagen fibrils and accumulation of elastic material. 58 This elastic material appears on slides stained with hematoxylin and eosin as basophilic blue-gray material in the upper dermis and is termed solar elastosis.
The dermal connective tissue damage observed in photoaging is mediated by matrix metalloproteinases, enzymes responsible for degradation of collagen and other extracellular matrix proteins in dermal connective tissue. 58 Via multiple molecular mechanisms, UVR causes increased activity of the transcription factor activator protein-1, which controls transcription of matrix metalloproteinases. 59 Both UVB and UVA are involved in the pathogenesis of photoaging, but UVA is believed to play a larger role because, relative to UVB, UVA has a greater average depth of penetration in the dermis and a greater abundance in natural sunlight. 57
Vitamin D
Vitamin D, which has long been known to be essential for skeletal health, has been in the news over the past few years because of reported associations of vitamin D deficiency with a wide variety of medical problems beyond osteoporosis, including malignancy, autoimmune disease, infection, type 2 diabetes, cardiovascular disease, cognitive decline, and even all-cause mortality. 60 Physicians who recommend sun protection are often asked about whether this can adversely affect vitamin D levels. The term “Vitamin D” refers to the 2 fat-soluble prohormones, vitamin D2 (ergocalciferol, made by plants and fungi) and vitamin D3 (cholecalciferol, made by animals and humans). Both forms are used in supplements for humans. The biologically active form of vitamin D is 1,25-dihydroxyvitamin D (1,25-OH-vitamin D), which regulates the transcription of vitamin D–responsive genes. 61 However, the most commonly used test to assess vitamin D levels in patients is serum 25-hydroxyvitamin D (25-OH-vitamin D).
Endogenous synthesis of vitamin D3 in humans takes place in the basal and suprabasal layers of the epidermis, where 7-dehydrocholesterol (pro-vitamin D3) is converted into pre-vitamin D3 by UVB radiation.62,63 Nonenzymatic isomerization of pre-vitamin D3 produces cholecalciferol (vitamin D3), which enters the bloodstream and is carried to the liver by vitamin D binding protein. 62 In the liver, vitamin D3 is hydroxylated by 25-hydroxylase, producing 25-OH-vitamin D (calcidiol). In the final step of vitamin D synthesis, 25-OH-vitamin D is carried by vitamin D binding protein to the kidney where 25-OH-vitamin D is hydroxylated by 1-alpha-hydroxylase, forming the active form of vitamin D, 1,25-OH-vitamin D (calcitriol). Evidence from in vitro studies demonstrates that this final step can also take place in certain nonrenal tissues that express 1-alpha-hydroxylase, such as epidermal keratinocytes. 63
Another source of vitamin D3 is exogenous intake, including dietary intake and oral supplements. Ingested vitamin D3 is converted to active vitamin D via the pathway detailed above, but the first 2 steps are bypassed (see Figure 1), and UVB thus does not play a role in the process. Natural dietary sources of vitamin D3 are limited; fatty fish, including salmon, tuna, and mackerel, and cod liver oil are some of the best sources.62,64 However, in the United States a wide variety of popular food items are fortified with vitamin D, including almost the entire United States milk supply and some brands of breakfast cereals, orange juice, yogurt, and margarine.62,64 Numerous supplements containing vitamin D3 and vitamin D2 are available, but only vitamin D2 is available as a high-dose prescription supplement. 65 It is controversial whether vitamin D3 supplements are more effective at increasing serum 25-OH-vitamin D levels than vitamin D2 supplements. Some studies have shown equivalence of vitamin D2 and D3,66,67 whereas others have demonstrated increased effectiveness of vitamin D3.68,69 Because some data indicate superior efficacy of vitamin D3, some experts recommended vitamin D3 over vitamin D2, especially when dosing is infrequent (less than once weekly), as vitamin D3 has a longer half-life. 70
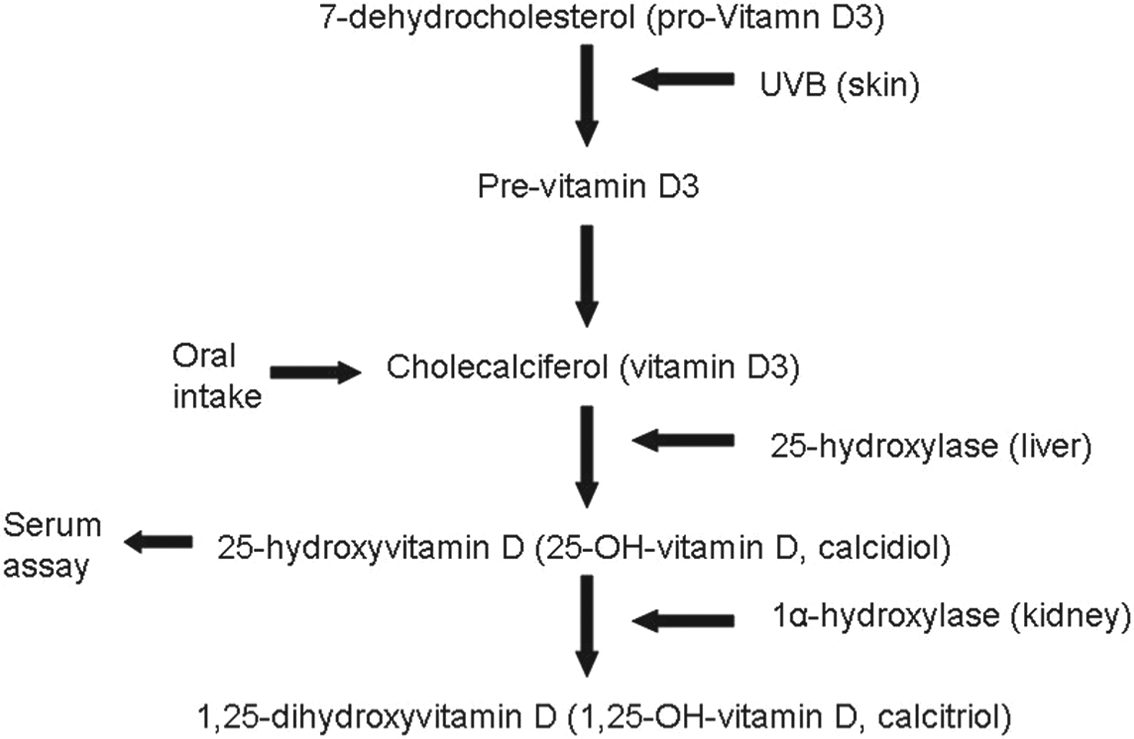
Synthesis of vitamin D.
Institute of Medicine (IOM) committee released a public health report in 2010 detailing the recommended daily allowance (RDA) for vitamin D. The IOM recommendations for nutritional requirements are based on strong scientific evidence for the role of vitamin D in skeletal health, as they concluded that the evidence linking vitamin D to extraskeletal outcomes is inconsistent and not strong enough to influence their recommendations. 71 The RDA for vitamin D is 600 IU/day for healthy people aged 1 to 70 years and 800 IU/day for those aged 71 years and older. These RDAs correspond to a serum 25-OH-vitmain D level of at least 20 mg/mL, which meets the requirements for at least 97.5% of the population. For infants, there is no official RDA, but adequate intake is estimated at 400 IU/day. Per the IOM recommendations, the tolerable upper intake levels are 4000 IU/day for individuals aged 9 and older. All recommendations were based on the assumption of minimal or no sunlight exposure.
Given that endogenous vitamin D synthesis requires UVB irradiation, sunscreen theoretically could block this process, and concern has been raised that widespread recommendations for sunscreen use might lead to vitamin D deficiency. However, a review of the literature revealed that although under very strictly controlled conditions sunscreens can result in significant reduction in the production of vitamin D, normal use of sunscreens does not typically lead to vitamin D insufficiency. 72 The lack of vitamin D deficiency resulting from normal use of sunscreen may be explained by the fact that individuals commonly apply sunscreens at much lower densities than the concentration of 2 mg/cm2 that is mandated for SPF testing and also may not reapply sunscreens as often as recommended.72-74 Furthermore, sunscreen is not usually applied to all exposed skin.72,75
Because of the risk of skin cancer associated with UVR, intentional sun exposure should not be recommended as a means for increasing vitamin D levels. For those who cannot meet the age-appropriate RDA for vitamin D through dietary consumption, oral vitamin D supplements are usually a much safer and more reliable alternative than sun exposure. The median dietary intake of vitamin D in the United States ranges from approximately 272 to 396 IU/day; therefore, most healthy individuals require dietary changes or a supplement to reach the RDA; for instance, a 75-year-old person with a dietary intake of 300 IU/day of vitamin D requires 500 IU/day supplementation to reach the RDA of 800 IU/day. 76 Patients can be reassured that that sun protection does not affect these recommendations, as the IOM RDA guidelines were made with the assumption of minimal to no UVR exposure.
Sunscreen
In the United States, sunscreens are considered over-the-counter medications and are regulated by the FDA. The purpose of sunscreens is to protect against the harmful effects of UVB and UVA irradiation. Ideally, sunscreens should be applied to all sun-exposed skin areas 30 minutes before sun exposure and, when outdoors, reapplied every 2 hours. Sunscreen should ideally be applied at a density of 2 mg/cm2, which is approximately 1 ounce (2 tablespoons) for an average-sized adult. There are 17 sunscreen active ingredients currently approved in the FDA monograph, each of which has different advantages and disadvantages. Many sunscreen products contain multiple active sunscreen ingredients.
Of the 17 US FDA-approved sunscreen ingredients, only 2 are inorganic (physical) filters, and the rest are organic (chemical) filters (see Table 3). 77 The inorganic filters, titanium dioxide and zinc oxide, function by absorbing, scattering, and reflecting UVR. Benefits of these agents include their photostability, low allergenicity, and broad protection against UVA and UVB. 78 Titanium dioxide imparts better UVB protection and has a whiter color, whereas zinc oxide offers better UVA coverage. 79 The main detraction from inorganic filters is that they may appear opaque, which is cosmetically undesirable.
United States FDA-Approved Sunscreen Filters.
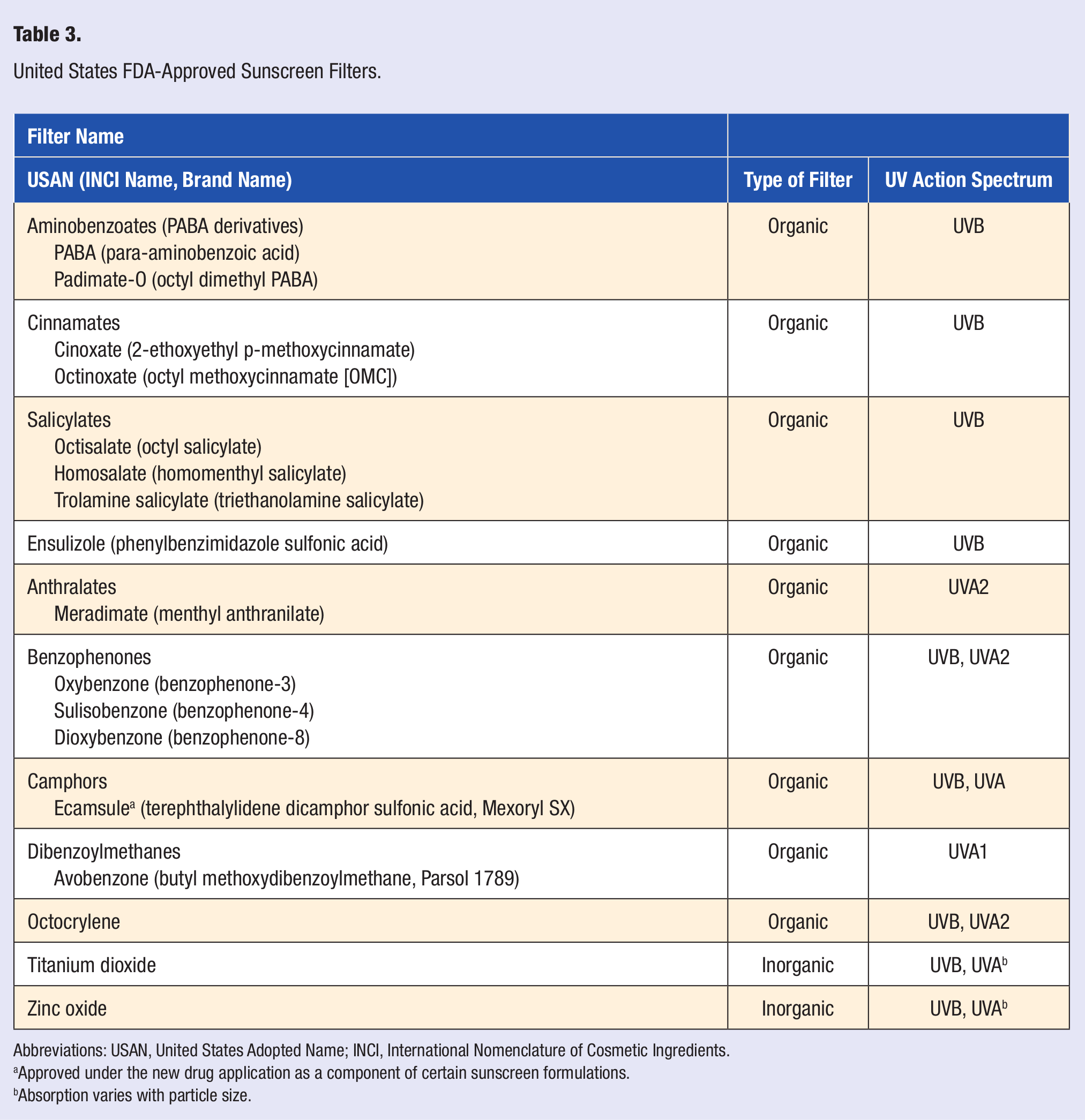
Abbreviations: USAN, United States Adopted Name; INCI, International Nomenclature of Cosmetic Ingredients.
Approved under the new drug application as a component of certain sunscreen formulations.
Absorption varies with particle size.
To improve cosmetic acceptability, many sunscreen products are now manufactured with smaller particles of titanium dioxide and zinc oxide, which results in a more transparent product that blends more readily into the skin. 80 Some of these products contain nanoparticles (<100 nm) of titanium dioxide or zinc oxide, and concerns have been raised about the safety of these products.81,82 These concerns stem from the theoretical possibility that the small size of nanoparticles might enable penetration into the deeper layers of the skin where they could potentially cause toxicity. A few isolated cell experiments have suggested that nanoparticles of zinc oxide and titanium dioxide may cause DNA damage via induction of reactive oxygen species in the presence of UVR. 82 However, in vitro and in vivo studies of nanosized titanium dioxide and zinc oxide have demonstrated that when titanium dioxide and zinc oxide nanoparticles are applied to intact skin, they do not penetrate deeper than the inviable stratum corneum, where there is no potential for cytotoxicity. 81 Therefore, current evidence indicates that sunscreens containing nanoparticles are safe for use on intact skin. Furthermore, nanoparticles of titanium dioxide and zinc oxide can be coated with manganese or other materials to reduce the potential of generating oxygen radicals on exposure to UVR.83,84 Nonetheless, as the incorporation of nanoparticles into sunscreens becomes more prevalent, further data are needed to assess whether nanoparticle application to damaged skin results in deeper skin penetration and potential toxicity.
Organic filters, which work by absorbing UVR, can be divided into UVB filters and UVA filters based on their action spectra. In the United States, octinoxate is the most commonly used UVB filter. 1 Although there are many FDA-approved UVB filters, there are only a handful of organic filters with effective UVA coverage, and most of these UVA filters cover predominately UVA2. Avobenzone is the most effective UVA filter available in the United States and is the only agent with significant coverage in the UVA1 range. 85 However, because of its inherent photolability, avobenzone must be combined with photostabilizing compounds such as octocrylene. 86 See Table 3 for a complete listing of FDA-approved sunscreen filters and their action spectra. 87
One popular UVA filter, oxybenzone, is the most common cause of photoallergic reactions to UV filters. However, considering the widespread use of sunscreens, the true incidence of UV filter–induced photoallergic reactions is low. Concerns have also been expressed about the safety of oxybenzone. These concerns stem from the fact that oxybenzone is absorbed systemically in humans at a rate of 1% to 2% after topical application and that it has been reported to have estrogenic and anti-androgenic activity in in vitro studies and in an animal model.82,88,89 However, human studies of oxybenzone have demonstrated no detectable hormonal disruption with topical use of oxybenzone. 87 Furthermore, to place the animal model in perspective, it was estimated that the average US woman would have to apply oxybenzone daily to 25% of her body surface area for an unrealistic duration of 277.0 years (or 100% of her body surface area for 69.3 years) in order to obtain the concentrations observed in the animal study. 87 The available scientific evidence shows a lack of systemic effects in humans with topical use of oxybenzones, and the FDA currently stands behind the safety of oxybenzone and all other approved UV filters. 77 However, the FDA will continue to monitor oxybenzone for potential systemic effects as new data become available.
The safety of an ingredient present in some sunscreens, retinyl palmitate, has also recently been questioned in the media. Retinoyl palmitate, which is a storage form of retinol (vitamin A) in human skin, is not a UVR filter but is commonly found in sunscreens and other topical products. Although some concerns have been raised that retinoyl palmitate may be carcinogenic, in vitro and animal studies do not show evidence of carcinogenicity, and decades of clinical use of topical products with retinyl palmitate in humans support its safety. 82
Sun protection factor is the widely accepted standard for quantifying the UVB protection of sunscreens. SPF is defined as the ratio of the lowest dose of UVR required to produce erythema on sunscreen-protected skin after application of 2 mg/cm2 of product, compared with the lowest UVR dose needed to produce the same erythema on skin without sunscreen. Patients often ask what SPF is recommended for sun protection. The recommendation by the American Academy of Dermatology is the generous application of sunscreen with a minimum SPF of 30. 90 Whether SPF values higher than 30 offer a benefit compared with SPF-30 sunscreens is controversial. Under laboratory conditions, the additional absorption of UVR by SPF-30+ sunscreens is minimal; for instance, SPF-15 sunscreens absorb 93.3% of the UVR, whereas SPF-30 sunscreens absorb 96.7%, and SPF-60 sunscreens absorb 98.3%. 91 Some have argued that because consumers do not apply adequate amounts of sunscreen, the effective SPF is much lower than the labeled SPF, and high SPF values therefore have substantial clinical benefit. 77 In 2011, the FDA proposed a maximum label of SPF-50+ after concluding that there are insufficient data to support the contention that SPF values above 50 produce additional clinical benefit. In response, a recent study was published demonstrating SPF-70 and SPF-100 sunscreens do offer clinical benefit in comparison with SPF-30 and SPF-50 sunscreens when the sunscreens are applied at the inadequate density of 0.5 mg/cm2.73,90 Given that individuals usually apply sunscreen at densities of 0.5 to 1 mg/cm2 rather than at the recommended 2 mg/cm2,73,90 this study likely has real-world applicability.
In summary, if sunscreen is applied at the recommended density of 2 mg/cm2, there appears to be minimal additional benefit to using sunscreens above SPF-30. However, recent data indicate that SPF-70 and SPF-100 sunscreens may offer superior protection relative to SPF-30 and SPF-50 sunscreens when sunscreen is applied at the inadequate density used by the average person. 90 The final FDA recommendations remain to be determined, but there is concern that allowing SPF labels higher than 50 may engender a false sense of security in sunscreen users, encouraging them to spend more time in the sun and ultimately resulting in more UVR-related skin damage. 77
UVA protection in sunscreen is also critical. Sunscreens labeled broad spectrum have both UVA and UVB coverage. In the United States for many years, sunscreens with any UVA filters could be labeled broad spectrum, and there was no way for consumers to know whether the UVA coverage of a given product was adequate. In June 2011, the FDA released a final rule on sunscreen labeling and effectiveness testing (the “final rule”) that addresses this issue. Any sunscreen that is labeled as broad spectrum must have a critical wavelength of greater than or equal to 370 nm, which indicates that it has adequate UVA coverage. 77 The critical wavelength is the wavelength below which 90% of the total area under the absorbance curve resides. It is important to understand that as UVB absorption (which correlates with SPF) increases, UVA absorption must increase proportionately to maintain a critical wavelength of 370 nm. Therefore, a sunscreen with a higher SPF must meet a higher minimum standard for UVA absorption before it can be labeled as broad spectrum. This allows consumers to more easily compare sunscreen products in terms that are already familiar to the general public; consumers simply can select a product based on the SPF, provided the sunscreen is broad spectrum. The FDA requires that all broad spectrum sunscreen products distributed after the final rule goes into effect (June 2012) display the words “Broad Spectrum” and “SPF” in the same font size and color and on the same line or adjacent to each other to emphasize the importance of broad spectrum coverage.
The FDA final rule has several other provisions. Products that claim to be water-resistant must be labeled as “water resistant (40 minutes)” or “water resistant (80 minutes)” based on standardized water resistance testing. 77 The misleading claims “water proof,” “sweat proof,” and “sun block” are no longer allowed. Another change is that broad spectrum sunscreens with SPF-15 or greater can display the following claim in the “Drug Facts” box on the back of the product package: “If used as directed with other sun protection measures, (sunscreens) decrease the risk of skin cancer and early skin aging caused by the sun.” The final rule also calls for more specific instructions about how to appropriately apply sunscreens.
There are several outstanding issues that are still being debated. The FDA has proposed capping the maximum SPF at 50+ but is currently still seeking additional comments about this proposal. 77 Another issue that is being considered is which sunscreen dosage forms can be marketed as sunscreens. The FDA has proposed that oils, lotions, creams, gels, butters, pastes, and ointments be considered satisfactory sunscreen dosing forms whereas wipes, towelettes, powders, body washes, and shampoos should not be marketed as sunscreens. Whether spray forms of sunscreens should be eligible for marketing as sunscreens is still being debated.
Sunscreen labels recommend that parents ask a physician about the use of sunscreen on infants below 6 months of age. In comparison with adults, infants have a higher body surface area-to-mass ratio, and there may also be differences in absorption, metabolism, and excretion of sunscreen products in young infants relative to adults. 92 In addition, sunscreens are not tested on young infants. For these reasons, sun avoidance and protective clothing are recommended as the preferred method of sun protection in infants below 6 months of age. However, both the American Academy of Dermatology and the American Academy of Pediatrics recommend the use of sunscreen for infants in this age range on small exposed areas of the body as an alternative method of photoprotection when full protection cannot be provided by protective clothing and sun avoidance. When selecting a sunscreen for infants and toddlers, inorganic filters are typically preferred as these have a lower potential for skin and eye irritation.
Other Methods of Sun Protection
When counseling patients about sun protection, physicians frequently recommend sunscreen use but often fail to discuss other methods of sun protection.
93
Sun avoidance is the most effective method of sun protection, although complete avoidance is obviously not practical. Minimizing sun exposure between 10
Clothing that causes scattering of UVR can provide effective protection against the sun, but the protection against UVB is greater than that against UVA. The UV protection provided by clothing is quantified by the UV protection factor (UPF), which is analogous to the SPF of sunscreen. UPF is determined as follows: (a) transmission of UVR through fabric is measured with a spectrophotometer and (b) UPF is calculated using a formula that combines the UV transmission data with 2 weighting factor values, solar spectral irradiance and erythema effectiveness, at each UV wavelength. 94 Because UVB is primarily responsible for the erythema response, similar to SPF, UPF is more heavily affected by the UVB component than the UVA component of the UVR spectrum.
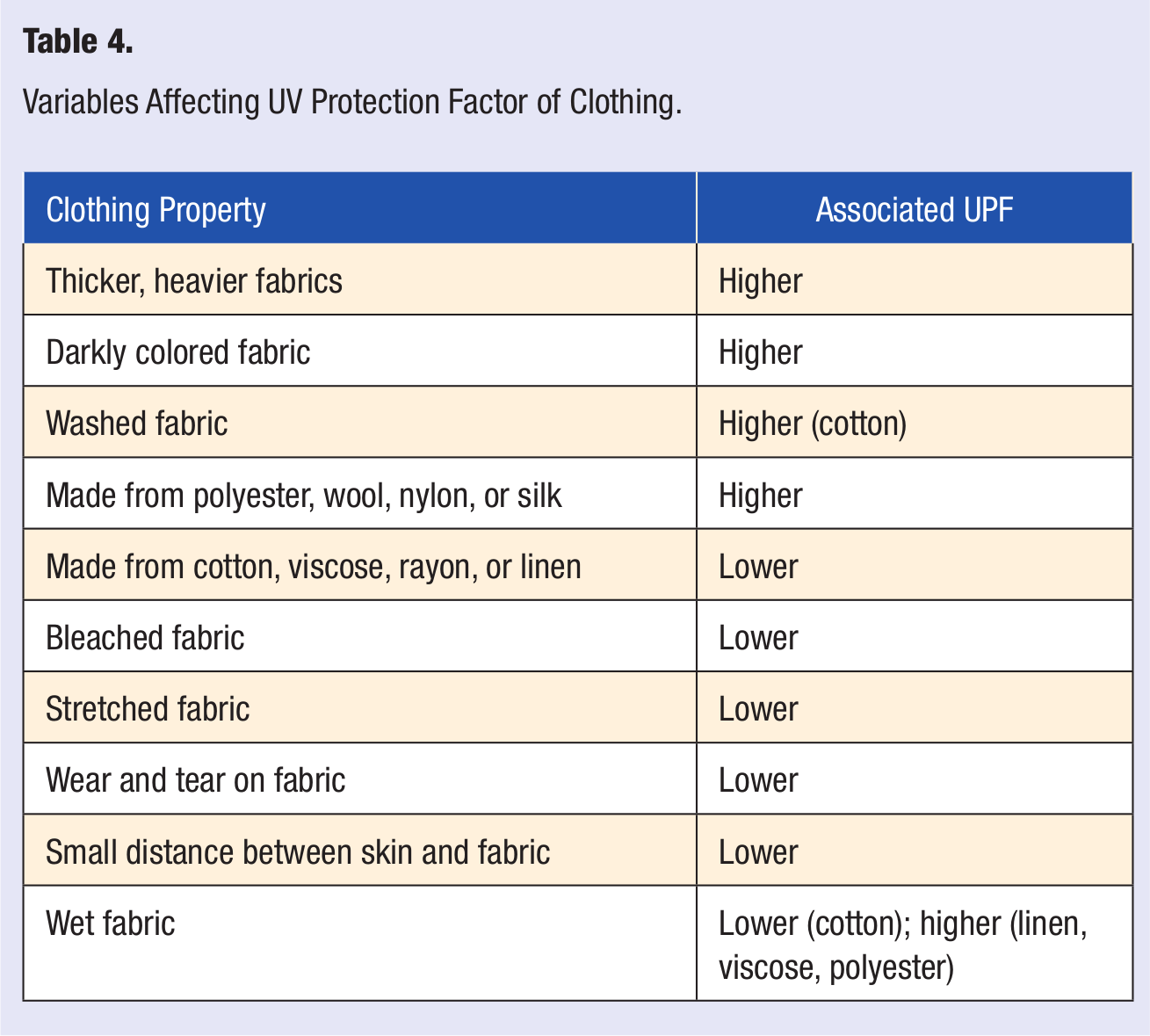
UPF is influenced by multiple variables, which are summarized in Table 4. 95 In general, thicker, heavier fabrics and more tightly woven fabrics have a higher UPF. With respect to specific materials, polyester typically provides the highest UPF, followed by wool, nylon, and silk. Cotton, viscose, rayon, and linen have a lower UPF. Unbleached fabrics have a higher UPF than bleached textiles, and darkly colored fabrics have a higher UPF than lighter fabrics. For cotton clothing, washing causes an increase in UPF because of shrinkage of the porosity of the fabric. Reduced UPF occurs with stretching of fabrics, wear and tear on fabrics, and when there is a small distance between skin and fabric. Water has a variable effect on UPF; wetness decreases the UPF of cotton but increases the UPF of linen, viscose, and polyester. To increase the UPF of clothing, fabrics can be chemically treated with UV absorbers and optical whiteners during the manufacturing process. 96 Commercially available laundry products containing UV absorbers Rit® SunGuardTM, which contains TinosorbTM FD are also very effective in increasing UPF.94,96,97 As the wide variety of factors involved in determination of UPF can be difficult to remember, one simple strategy is to advise patients to wear polyester clothing as opposed to cotton when spending time in the sun. For patients who prefer cotton, cotton clothing marketed as sun-protective (owing to pretreatment with UV absorbers) and use of laundry products containing UV absorbers are practical alternatives. Wide-brimmed hats (>7.5 cm), which provide better sun protection for the head and neck than hats with smaller brims, should also be recommended. 1
Variables Affecting UV Protection Factor of Clothing.
Another important component of sun protection, which may be neglected by dermatologists who focus on the skin, is eye protection. The cornea and lens absorb UVR in people of all ages, whereas the retina absorbs UVR predominantly in children because lens opacities that develop with age protect the retina in adults. 98 Chronic UVR exposure is a risk factor for many ocular diseases, including cortical cataracts, pterygium, SCC of the cornea and conjunctiva, conjunctival melanoma, and possibly uveal melanoma. Acute UVR exposure can also cause multiple ocular problems, including photokeratitis and photoconjunctivitis.
Sunglasses can be effective at protecting the eyes from UVR, although some lenses transmit much more UVR than others. There is a standard guideline in the United States that categorizes the different types of sunglasses according to the degree of shading and the UV absorption profile, but this standard is voluntary, so it can sometimes be difficult to find a pair of sunglasses with adequate protection. 99 Ideally, consumers should seek glasses that block as much UV radiation as possible while allowing the transmission of visible light.
UVR exposure of the eye has several important differences from exposure of the skin. Because the eye is shielded by the eyelids and brow ridges and because looking at direct light causes squinting, reflection (off grass, sand, ground, water, or snow) and scattering (for instance, from patchy cloud cover) are the most important sources of UV exposure. It is therefore critical that the eyes be protected from all directions, but most sunglasses are designed for fashion and comfort, so the lateral and inferior borders of the eyes are typically poorly shielded. 99 Tight-fitting sunglasses with a wrap-around design provide better protection than small, flat lenses worn away from the eye. UV-blocking contact lenses are also effective at protecting the eyes from UVR. 100 In addition, unlike sunglasses, which often prevent the protective squint mechanism by blocking visible light, UVR-blocking contact lenses do not decrease the squint mechanism. However, unlike sunglasses, contact lenses cannot provide protection for the periocular skin.
In contrast to the relationship between peak sunlight hours and the skin, off-peak hours of sunlight are more dangerous to the eyes than peak hours.
99
During the morning and late afternoon, the UV incident angle is low, allowing the UVR to bypass the defense of the brow ridge and eyelid. Furthermore, the light intensity is weaker during off-peak hours, so protective squinting does not occur. Because sun protection campaigns typically focus on skin protection and advise sun protection mostly between 10
Indoor Tanning
In the United States, indoor tanning is used by almost 30 million people annually, including 2.3 million adolescents. 101 Indoor tanning rates are highest among young females, aged 17 to 30 years. 102 The incidence of both melanoma and nonmelanoma skin cancer in the United States is rapidly increasing, especially in young women.103,104 A recent systematic review specifically linked indoor tanning use with an increased risk of both melanoma and SCC. 105 An even higher relative risk of melanoma was found in those who started using tanning beds before 35 years of age. Although the systematic review did not find an elevated risk of BCC in tanning bed users, a large case–control study did demonstrate an increased risk of both BCC and SCC with use of indoor tanning. 106
In recent years, the dangers of tanning beds have been recognized publicly around the world. The World Health Organization classified tanning beds as a human carcinogen in 2009, and multiple countries have imposed restrictions or bans on the indoor tanning industry, generally targeting minors. 107 In the United States, California and Vermont are the only states with a complete ban on indoor tanning for minors, but 31 states have enacted restrictions, and efforts to increase restrictions are ongoing. 108
To facilitate tanning, indoor tanning devices emit UVR at much higher doses than are found in sunlight. 107 In addition, to minimize erythema, indoor tanning devices also use an increased UVA to UVB ratio relative to natural sunlight. One study quantifying UVR output at 62 indoor tanning locations found much higher mean UVA (192.1 W/m2) and UVB (0.35 W/m2) doses than the UVR in noon sunlight in Washington, DC in the summer. 109 Relative to the noon DC summer sunlight, the mean UVA dose was approximately 4 times as high and the UVB dose was twice as high in the indoor tanning salons. Furthermore, 95% of tanners exceeded the FDA-recommended exposure limits.
Some proponents of indoor tanning argue that tanning beds can have health benefits by increasing vitamin D levels. 107 However, tanning beds emit predominantly UVA, which makes them inefficient at increasing endogenous vitamin D synthesis, as this is a UVB-dependent process. Furthermore, for those at risk for vitamin D deficiency, vitamin D supplements are a much safer and more reliable source of vitamin D than indoor tanning or exposure to natural sunlight.
There is substantial evidence indicating that individuals may become addicted to indoor tanning. UVA exposure can cause an elevation of plasma endogenous opioids, 110 and symptoms of opiate withdrawal occurred when frequent tanners were given the opiate antagonist naltrexone in a randomized controlled trial. 111 A recent study using a modified version of the Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition, Text Revision) (DSM-IV-TR) criteria for substance-related disorders in college students who had used indoor tanning facilities found that 39.3% of tanners met DSM-IV-TR criteria for tanning addiction. 112 In summary, indoor tanning can be an addictive behavior, and it is a well-documented carcinogen with no legitimate health benefits. The dermatology community strongly supports public education campaigns about this issue as well as the ongoing efforts to ban minors from engaging in this dangerous activity. 107
Conclusion
UVR clearly has a broad impact on the skin and has the potential to lead to a myriad problems, including melanoma and nonmelanoma skin cancer, sunburns, immunosuppression, and ocular problems. Other adverse effects of UV exposure include photodermatoses (including polymorphous light eruption, actinic prurigo, chronic actinic dermatitis, solar urticaria, and hydroa vacciniforme), phototoxicity and photoallergy (caused by drugs or chemicals), and photoaging (wrinkling, uneven pigmentation, telangiectases, and other undesirable skin changes). 107 Educating patients about the dangers of UVR and the most effective forms of sun protection is an important task that will most effectively be accomplished through the joint efforts of primary care physicians, dermatologists, and other health care practitioners.