
Abstract
The North American continent comprises a diverse array of individuals. Although the majority of them prescribe to the beliefs and treatments of Western biomedicine, a substantial number also practice diverse approaches to health. This article summarizes the basic tenets of major non-Western approaches to health, including the main beliefs and treatments. It bases this discussion in the context of health disparities, the existence of which presents a major problem for health care in America, and with an eye toward aiding the development of cultural competence for clinicians and health care providers nationwide.
For most people living in the United States of America, basic indicators of good health include the absence of disease, injury, or illness; a slow pulse; or the ability to do many physical exercises. All these represent only one general way of being healthy, the one supported by Western medicine. Many of the 304 million Americans have different answers to questions about health and are not similarly healthy.1-3 For example, death rates for African Americans are significantly higher than those of Americans overall for heart disease, cancer, diabetes, HIV, and homicide. 4 Corresponding to such differences, the United States health care system has been making active attempts to broaden approaches toward health care in order to fulfill the needs of the diverse population 5 and advance cultural competence. 6 There are critical cultural variations in the conceptualization, perception, health-seeking behaviors, assessment, diagnosis, and treatment of abnormal behaviors and physical sickness. In this article, I first review the major approaches to health across cultures, including some major nontraditional health care practices. I then focus on the role of acculturation and health, with an emphasis on Latinos and Asian Americans.
In general, health care, mental health, and disease incidence vary significantly across cultural groups.
Defining Culture
Culture can be broadly defined as “a unique meaning and information system, shared by a group and transmitted across generations, that allows the group to meet basic needs of survival, by coordinating social behavior to achieve a viable existence, to transmit successful social behaviors, to pursue happiness and well-being, and to derive meaning from life.” 7 Culture includes ethnicity, race, religion, age, sex, family values, the region of the country, and many other features. Aspects of the specific culture we belong to correspondingly influence each of our health behaviors.
The most often discussed types of culture are race and ethnicity, but two of the most important aspects that define cultural groups, and relate to health, are socioeconomic status (SES) and sex. 8 SES is related to a higher occurrence of most chronic and infectious disorders and to higher rates of nearly all major causes of mortality and morbidity. 9 In regard to sex, men and women differ on a variety of health-related factors, such as their need for health information. 10 This often interacts with other elements of culture. For example, heavy drinking among Korean American men is believed to be associated with Korean traditions, such as Poke-Tang, because they encourage men to drink but not women. 11
Gender is a social/cultural construct that is learned by being placed within the context of each unique society, 12 and gender differences exist within cultural groups. In the Latino community, for example, there are differences in relation to health-seeking behavior, especially substance use.13-18 In Mexican border samples, high acculturation was associated with heavier episodic drinking for women; however, a lower prevalence of abuse and dependence existed for men who were more assimilated, and those that were less acculturated were 7 to 11 times more likely to abuse or become dependent on alcohol. 13 Latino adults who immigrated during an older age are less likely to smoke cigarettes or engage in binge drinking than US-born peers, but this finding was more significant for women. 15
Health Disparities
Considering cultural variations in approaches to health provide useful ammunition in the fight against existing health disparities—“differences in health that are not only unnecessary and avoidable, but in addition, are considered unfair and unjust.” 19 There are many examples of disparities: for example, the infant death rate among African Americans is still more than double that of European Americans, and heart disease death rates are more than 40% higher for African Americans than for European Americans. 20 The suicide rate among American Indians is 2.2 times higher than the national average, and those living below the poverty level are significantly more depressed than those with a higher SES. 21 In general, health care, mental health, and disease incidence vary significantly across cultural groups.
The fact that there are differences in health behaviors and health in general has not escaped the notice of the American government, funding agencies, or psychologists. The American Psychological Association (APA) has worked hard toward “the elimination of racial and ethnic disparities in health access.” 22 The federal government has also created cultural competency standards (www.thinkculturalhealth.org/), with corresponding training resources designed to help health care practitioners better serve patients from diverse populations. The field of nursing has been particularly active in this regard and sees developing cultural competency as an explicit way to eliminate health disparities.6,23 The review in the rest of this article is aimed at helping a broader field of health professionals enhance their knowledge of not just cultural groups, but more important, the approaches.
Cultural Variations in Approaches to Health
In most of the countries around the globe, health is understood using either the Western evidence-based medical approach or traditional indigenous approaches. 24 Western biomedicine is one of the most dominant forms of health care in the world today, and hallmarks of this approach are an increasing reliance on technology and the use of complex scientific procedures for the diagnosis and treatment of illness. In stark contrast are the beliefs of traditional Chinese medicine (TCM) and Curanderismo.
Traditional Chinese Medicine
TCM is used to treat more people than any other form of medicine. However, even in North America, there are a large number of TCM schools and practitioners. In fact, acupuncture, one form of TCM, is covered by most health insurance policies. Two main systems categorize the forces identified in TCM that influence health and well-being: yin and yang and the 5 phases. According to one Chinese philosophy, all life and the entire universe originated from a single unified source called Tao. In TCM, health is the balance of the yin and yang, the 2 complementary forces in the universe. Yin and yang are mutually interdependent, constantly interactive, and potentially interchangeable forces. A healthy individual has a balanced amount of yin and yang. If a person is sick, his or her forces are out of balance. 25
The yin and yang are often translated into hot and cold (2 clear opposites), referring to qualities and not temperatures. To be healthy, what you eat and drink and the way you live your life should have equal amounts of hot qualities and cold ones. Balancing hot and cold is a critical element of many different cultures (eg, Chinese, Indian, and even Mexican), although the foods that constitute each may vary across cultures. Some “hot” foods include beef, garlic, ginger, and alcohol. Some “cold” foods include honey, most greens, potatoes, and some fruits (eg, melons and pears). The 5 phases or elemental activities refer to specific active forces and illustrate the intricate associations that the ancient Chinese saw between human beings and nature. Energy or qi, another critical aspect of TCM, moves within the body in the same pattern as it does in nature, with each season and different foods helping optimize energy flow within the body. The 5 elements of wood, fire, earth, metal, and water each link to a season of the year, a specific organ, and a specific food. What you eat correspondingly can influence your different organs and your well-being in general. 25
There is a growing body of research being conducted on different TCMs. Some empirical studies suggest that TCMs are no more effective than Western medicines. For example, 620 cocaine-dependent patients took part in a randomized clinical trial where one-third of the participants received acupuncture. The acupuncture group did not show significant reduction in drug use. 26 There is a larger body of work supporting TCMs, though much of the research validating TCM was done without the use of robust Western scientific methodology. Part of the problem is that testing TCMs involves special challenges. 27 How do you provide a comparative control condition or placebo when you are testing acupuncture? Much of the research conducted on TCM in America analyzes the constituents of herbs used in treatment, and many such studies show that the active ingredients of the herbs facilitate cures. 28 The growing evidence notwithstanding, it will be some time before TCM is accepted widely.
Mexican American/Latino Health Beliefs
Curanderismo is the Mexican American folk-healing system that often coexists side by side with Western biomedicine. Coming from the Spanish verb curar meaning “to heal,” curanderos are full-time healers. The curandero’s office is in the community, often in the healer’s own home. There are no appointments, forms, or fees, and you pay whatever you believe the healer deserves. This form of healing relies heavily on the patient’s faith and belief systems and uses everyday herbs, fruits, eggs, and oils. In studies beginning as early as 1959, researchers first focused on Mexican American cultural illnesses, such as mal de ojo (sickness from admiring a baby too much). More recent work focuses on the healers themselves, their beliefs, training processes, and processes for treatment. 29 Surveys of Mexican Americans show that even among highly assimilated Mexican Americans, traditional and indigenous practices still persist.
The Mexican American cultural framework acknowledges the existence of 2 sources of illness, one natural and one supernatural. When the natural and supernatural worlds exist in harmony, optimal health is achieved. Disharmony between these realms breeds illness. Beyond this supernatural balance component, the curandero’s concept of the cause of illness parallels that of Western biomedicine. Like biomedical practitioners, curanderos believe that germs and other natural factors can cause illness. However, curanderos also believe that there are supernatural causes to illness in addition to natural factors. If an evil spirit, a witch, or a sorcerer causes an illness, then only a supernatural solution will be sufficient for a cure. Illness can also be caused if a person’s energy field is weakened or disrupted. Whether it is diabetes, alcoholism, or cancer, if a spirit caused it, supernatural intervention is the only thing that can cure it.
Curanderos use 3 levels of treatment depending on the source of the illness: material, spiritual, and mental. 29 Working on the material level, curanderos use things found in any house (eggs, lemons, garlic, and ribbons) and religious symbols (a crucifix, water, oils, and incense). These material things often are designed to either emit or absorb vibrating energy that repairs the energy field around a person. Ceremonies include prayers, ritual sweepings, or cleansings. 30 The spiritual level of treatment often includes the curandero entering a trance, leaving his or her body, and playing the role of a medium. This spiritual treatment allows a spirit to commandeer the curandero’s body, facilitating a cure in the patient. On some occasions, the spirit will prescribe simple herbal remedies (via the curandero). On other occasions, the spirit will perform further rituals. The mental level of treatment relies on the power held by the individual curandero, rather than on spirits or materials. Some illnesses (eg, physical) often are treated by herbs alone, 31 and psychological problems may be treated by a combination of all these types of treatments.
In a manner akin to that of health psychologists, curanderos explicitly focus on social, psychological, and biological problems. 29 The difference is that they add a focus on spiritual problems as well. From a social perspective, the community where the curanderos work recognizes and accepts what the curandero is trying to achieve. The social world is important to the curanderos, who evaluate the patient’s direct and extended support system. The patient’s moods and feelings are weighed together with any physical symptoms. Finally, there is always a ritual petition to God and other spiritual beings to help with the healing process.
For most Mexican Americans, the choice between curanderismo and Western biomedicine is an either/or proposition. Some individuals use both systems, and some stay completely away from Western hospitals as much as they can or because they do not have enough money to use them. Acculturated and higher social class Mexican Americans tend to rely exclusively on Western biomedicine. The existence of this strong cultural and historical folk medicine and the large numbers of its adherents make this approach to illness an important alternative style for us to consider in our study of the psychology of health.
There are limited empirical studies of the effects of curanderismo, though there are many different accounts of the practices available in health and medical journals.32,33 More and more medical journals are publishing articles on this form of healing,34,35 but little has been found in mainstream health psychology. The uses of curanderismo have been associated with negative health outcomes that are more often seen in print. For example, there was a report of a case of a young child who had to be hospitalized for isopropyl alcohol toxicity caused by the use of a curanderismo treatment of espanto (evil spirits). 36
Other Cultural Approaches to Health
African American folk medicine
In addition to the 2 basic approaches to health, there are also a wealth of other belief systems. One group of beliefs not discussed as often as those above is African American beliefs. For many members of this cultural group, health beliefs reflect cultural roots that include elements of African healing, medicine of the Civil War South, European medical and anatomical folklore, West Indies voodoo religion, fundamentalist Christianity, and other belief systems.
African American communities have become very diverse, especially with the recent arrival of people from Haiti and other Caribbean countries and Africa. Similar to the American Indians, many people of African descent also hold a strong connection to nature. There are many geographical variations in folk medicine in Africa. For example, in the southern region of Africa (eg, Zimbabwe and Swaziland), many people relied heavily on inyangas (traditional herbalists). Even today in Africa, hospitals and modern medicines are invariably the last resort in illness. Some traditional Africans seeks relief in the herbal lore of the ancestors and consult the inyanga, who is in charge of the physical health of the people. 37 When bewitchment is suspected, which happens frequently among the traditional people of Africa, or if there is a personal family crisis or love or financial problem, the patient is taken to a sangoma (spiritual diviner or spiritual/traditional healer), who is believed to have spiritual powers and is able to work with the ancestral spirits or spirit guides. 37 The sangoma uses various methods such as “throwing the bones” (amathambo, also known by other names depending on the cultural group) or going into a spiritual trance to consult the ancestral spirits or spirit guides to find the diagnosis or cure for the problem, be it bewitchment, love, or any other problem. Depending on the response from the higher source, a decision will be made on what herbs and mixes (intelezis) should be used and in what manner (eg, orally or burning). If more powerful medicine is needed, numerous “magical rites” can or will be performed according to rituals handed down from sangoma to sangoma. 37 In South Africa, there are more than 70, 000 sangomas or spiritual healers who dispense herbal medicines and even issue medical certificates to employees for purposes of sick leave.
Many African Americans believe in a form of folk medicine that incorporates and mirrors aspects of voodou (the often seen spelling voodoo is not accurate), which is a type of religion derived from some of the world’s oldest known religions that have been present in Africa since the beginning of human civilization. 38 Today, voudoo is a legitimate religion in a number of areas of the world. In some parts of the United States, the remnants are stronger than in others. Some African American communities in isolated areas, such as the coast and islands of North Carolina, survived intact well into the 20th century. Here, Gullah culture involving belief in herbalism, spiritualism, and black magic thrived. 39 What was called voodou in other parts of the country was called the root (meaning charm). Although shamanistic rituals and voodou rites may seem to be ineffectual ways to cure according to Western science, the rituals have meaning to those who believe in them and should not be ignored or ridiculed.
American Indian health beliefs
Many elements of the American Indian belief system and the approach to health are somewhat consistent with elements of curanderismo and TCM and provide a strong contrast to Western biomedicine. Although different tribes have different variations on the basic beliefs, 4 practices are common to most 40 : the use of herbal remedies, ritual purification or purging, symbolic rituals and ceremonies, and the involvement of healers, also referred to as medicine men, medicine women, or shamans (though the latter is primarily used for the healers of northern Europe). 41 Native Americans have used and benefited from these practices for at least 10, 000 years and possibly much longer.
Similar to the ancient Chinese, American Indians believed that human beings and the natural world are closely intertwined. The fate of humankind and the fate of the trees, the mountains, the sky, and the oceans are all linked. The Navajos call this “walking in beauty,” a worldview in which everything in life is connected and influences everything else. In this system, sickness is a result of things falling out of balance and of losing one’s way in the path of beauty. 42 Animals are sacred, the winds are sacred, and trees and plants, bugs, and rocks are sacred. Every human and every object corresponds to a presence in the spirit world, and these spirits promote health or cause illness. Spiritual rejuvenation and the achievement of a general sense of physical, emotional, and communal harmony are at the heart of Native American medicine. Shamans coordinate American Indian medicine and inherit the ability to communicate with spirits in much the same way that Mexican American curanderos do. Shamans spend much of their day listening to their patients, asking about their family and their behaviors and beliefs, and making connections between the patient’s life and their illness. Shamans do not treat spirits as metaphors or prayers as a way to trick a body into healing. Shamans treat spirits as real entities, respecting them as they would any other intelligent being or living person.
Ritual and ceremony play a major role in American Indian medicine. One of the most potent and frequent ceremonies is the sweat lodge. 43 Medicine men hold lodges or “sweats” for different reasons. Sometimes a sweat purifies the people present; at other times, a sweat is dedicated to someone with cancer or another terminal illness. The ceremony takes place in a sweat lodge where hot stones raise the temperature leading to profuse perspiration, which is thought to detoxify the body. Because of the darkness and the heat, participants often experience hallucinations that connect to spirit guides or provide insight into personal conditions.
Other ceremonies are also used. For example, the Lakota and Navajo use the medicine wheel, the sacred hoop, and the sing, which is a community healing ceremony lasting from 2 to 9 days and guided by a highly skilled specialist called a singer. Many healers also use dancing, sand painting, chanting, drumming (which places a person’s spirit into alignment with the heartbeat of Mother Earth), and feathers and rattles to remove blockages and stagnations of energy that may be contributing to ill health. Sometimes sacred stones are rubbed over the part of the person’s body suspected to be diseased. Although many American Indians prefer to consult a conventional medical doctor for conditions that require antibiotics or surgery, herbal remedies continue to play a substantial role in the treatment of various physical, emotional, and spiritual ailments. The herbs prescribed vary from tribe to tribe, depending on the ailment and what herbs are available in a particular area. Some shamans suggest that the herbs be eaten directly. Others suggest taking them mixed with water (like an herbal tea) or even with food. Healers burn herbs such as sage, sweet grass, or cedar (called a smudge) in almost every ceremony and let the restorative smoke drift over the patient.
Ayurveda: Indian health beliefs
Ayurveda, a traditional Indian holistic system of medicine was developed by Charaka.44,45 Charaka described 4 causative factors in mental illness: (1) diet (incompatible, vitiated, and unclean food); (2) disrespect to Gods, elders, and teachers; (3) mental shock caused by emotions such as excessive fear and joy; and (4) faulty bodily activity. Thus, Ayurveda considers a biopsychosocial approach in formulating causative factors in mental disorders. Charaka, while emphasizing the need for harmony between body, mind, and soul, focused on preventive, curative, and promotive aspects of mental health. The use of plants and herbal remedies plays a major part in Ayurvedic medicine. About 600 different medicinal plants are mentioned in the core Ayurvedic texts. Western drug companies have used a number of plants originally used in India to cure diseases. For example, psyllium seed is used for bowel problems, and other plants are used to reduce blood pressure, control diarrhea, and lessen the risk of liver or heart problems. A substance called forskolin, isolated from the Coleus forskohlii plant, has been used in Ayurveda for treating heart disease, and its use has now been empirically validated by Western biomedicine. 3
TCM and Ayurveda share many basic similarities. Ayurvedic science also uses the notion of basic elements: 5 great elements form the basis of the universe. Earth represents the solid state; water, the liquid state; air, the gaseous state; fire, the power to change the state of any substance; and ether, simultaneously the source of all matter and the space in which it exists. Achieving the right balance of these elements in the body is critical to maintaining a healthy state. These elements also combine to form 3 major forces (doshas) that influence physiological functions critical to healthy living 46 : the Vata dosha, Pitta dosha, and Kapha dosha. Similar to the meridians in TCM, the existence of these forces is demonstrated more by inference and results of their hypothesized effects than by physical observation. Vata, Pitta, and Kapha are also associated with specific body type characteristics. 46
Culture and Mental Health
Culture influences how individuals manifest symptoms, communicate their symptoms, cope with psychological challenges, and their willingness to seek treatment. 2 Understanding the role of culture in mental health is crucial to comprehensive and accurate diagnoses and treatment of illnesses. Even the US Surgeon General has recognized the importance of both a patient’s culture and that of the health care provider in mental health treatment, service use, and diagnosis. 47 A number of frameworks have been used to understand cultural influences on mental health, including the sociobiological, ecocultural, and biopsychosocial perspectives. 2 Another perspective that has become increasingly important in our postmodern world, with much migration and resettlement, is multiculturalism. It literally means many cultural views. It is a view that emphasizes importance, equality, and acceptance for all cultural groups within a society and supports a strong desire to increase awareness about all groups to the benefit of the society as a whole. 48
Overall epidemiological, clinical, and other studies suggest a “moderate but not unlimited impact of cultural factors” on mental health. 49 This implies that accurate evaluation and diagnoses of psychological disorders within the bounds of culture is crucial for appropriate and effective treatment and intervention. 50 However, in spite of efforts in the field of counseling/clinical psychology to include or emphasize cultural influences on psychopathology in our traditional training programs, we are still limited in the depth and breadth of material available.
Culture influences the client as well as the therapist. One needs to also focus on a wide range of processes—conceptualization, perception, health-seeking behaviors, assessment, diagnosis, and treatment—in the context of cultural variations. We need to consider issues related to reliability, validity, and standardization of commonly used psychological assessment instruments among different cultural groups and the role of factors such as religion and stress as they relate to culture. It is also important to look at a bigger picture, focusing on psychotherapy in a culturally diverse world and international perspectives on mental health. 24 Even specific disorders, such as eating disorders, mood disorders, anxiety disorders, posttraumatic stress disorder, and psychotic disorders, vary by culture. 2 There are cultural differences and/or similarities in the symptoms reported as well as the possibility of misdiagnosing mental illness among people who focus on specific symptoms (eg, somatic) and less on others for varying reasons.
The Role of Acculturation
Although different cultural groups may have different approaches to understanding health and each approach has its own treatments and related health behaviors as described above, the extent to which a person will practice the health behaviors of their cultural group will vary with their own acculturation level. In the last part of this article, I examine how acculturation affects the health behaviors of the largest North American minority group, Latino/Hispanic Americans.
Acculturation is commonly defined as a phenomenon that results when 2 or more cultures come into continuous contact that can often result in not only individual changes but also changes at the sociocultural level. 51 In general, those who integrate (are a part of both their heritage culture and the larger society) are better adapted than those who orient themselves to one or the other culture or to neither culture.52,53 The most commonly used measures to examine acculturation assess cultural identity, language preferences, place of origin, media preferences, and social networks. Some studies use a combination of scales. For example, the Acculturation Rating Scale for Mexican Americans (ARTHMA-II) and Multi-group Ethnic Identity Measure (MIEM) are both used when the combination would better capture ethnic identity in relation to acculturation. 54
The Latino and Hispanic population are often the center point of research examining acculturation and health within the United States.55,56 In relation to perceived health, studies show that highly acculturated Mexican American Hispanics more frequently reported poor/fair health or poorer health outcomes.57-59 Minority/Immigrant status was also associated with lower reported health for both Hispanic and African American immigrants. 60 In relation to mental health, Latino clients who reported higher levels of ethnic identity also reported more negative pre– and post–psychological outcome evaluations. 54
In contrast to reported health outcomes, whether someone seeks out healthy behaviors or forms healthy habits is related to their level of acculturation.15,59,61-64 Within the Latino/Hispanic sample, Mexican and Puerto Rican Americans were less likely to seek help from mental health services, and acculturation predicted the differences. 61
Differences increase with a focus on immigration status. Adult women immigrants reported more healthy behaviors than US-born women. 16 In contrast, another study found that women aged 55 years and older reported more healthy behaviors (eg, exercising and avoid smoking) and less age-denial behaviors (eg, coloring hair and using wrinkle remover cosmetics, tummy tucks, and face lifts) than women within the same age range. 17 Within the United States Mexico border communities, those who reported higher levels of acculturation experienced a decline in some of their health-seeking behaviors, whereas the less acculturated participants reported healthier food intakes such as less fat, cholesterol, and sodium intake and consumption of more fruits and vegetables. 63 Hispanic adults who reported lower levels of acculturation also reported better diets but displayed a greater risk of having poor hypercholesterolemia control than those who were more acculturated because the acculturated adults reported more physical activity. 62 It was found that US-born Mexican Americans tend to sleep less per night; however stress levels and smoking status also contributed to the lack of sleep. 65
In relation to cancer screenings, Latinos who were not born in the United States were less likely to have reported having a mammogram and cervical cancer screening than US-born women. 66 HIV-positive and highly acculturated Latinos were more likely to engage in negative coping styles, which were associated with risky sexual behavior, cigarette smoking, alcohol use, and greater nonadherence with HIV medication. 59 Avoiding excessive substance use is a health-seeking behavior that influences the health outcomes of many women and men of different ethnic backgrounds within the United States. 67
Substance use for Latino/Hispanic Americans is often also related to their level of acculturation.13,64,68,69 Two variables that influence the relationship between substance use and acculturation are age and social factors.64,68-70 For example, parent–child acculturation differences can increase the likelihood that the adolescent will use substances such as, alcohol, marijuana, and cigarettes; however, Hispanics with a US orientation were more likely to use all 3 of these substances, whereas those of Hispanic orientation were more likely to just use alcohol, which could imply different cultural norms based on their level of acculturation. 64 Both family and peer relationships were found to mediate the association between acculturation and substance use for adolescents.68,69 Within a qualitative study, Hispanic/Latino adolescents reported that they believed that high alcohol consumption is based on individual characteristics and peer influence rather than acculturation level. 70 Acculturation stress was rated higher for Latino adolescents with greater parental conflict, and more substance abuse behaviors were also present. 68 Based on a sample from Florida, Mexican and Puerto Rican adolescents who primarily spoke English at home reported higher levels of substance use and were more likely to associate with deviant peers, to live with families with higher tolerance of substance use, and live in communities with perceived greater drug and firearm use. 68 Perceived parental monitoring and parent–child communication were also found to be related to less use of cigarettes, alcohol, and marijuana for Hispanic adolescents. 71
Recommendations for Clinicians and Health Care Workers
There are clearly many different cultural approaches to health, and it is of great importance for health care workers and the administrations that support them to be culturally aware. Table 1 provides a summary of key recommendations for health care administrators. Many clinicians and health care workers may not have received the necessary instructions to be culturally competent, but there are some easy ways to be prepared. Perhaps the most helpful model of cultural competence is the Purnell Model 72 of cultural competence. The model posits 12 main cultural domains that a clinician should be aware of and attempt to learn about for each client. Table 2 illustrates the main domains and provides sample questions for the clinician to use to gain cultural competence. Note that cultural diversity spans every aspect of life, and the 12 domains and questions to understand each are designed to help a clinician get an understanding of cultural diversity. There are other useful resources for the interested reader that provide in-depth summaries of key characteristics of a variety of cultures and provide a single-stop shop for learning about different cultural approaches.72,73
Recommendations for Fostering Cultural Sensitivity in Health Care Organizations and Clinics a .
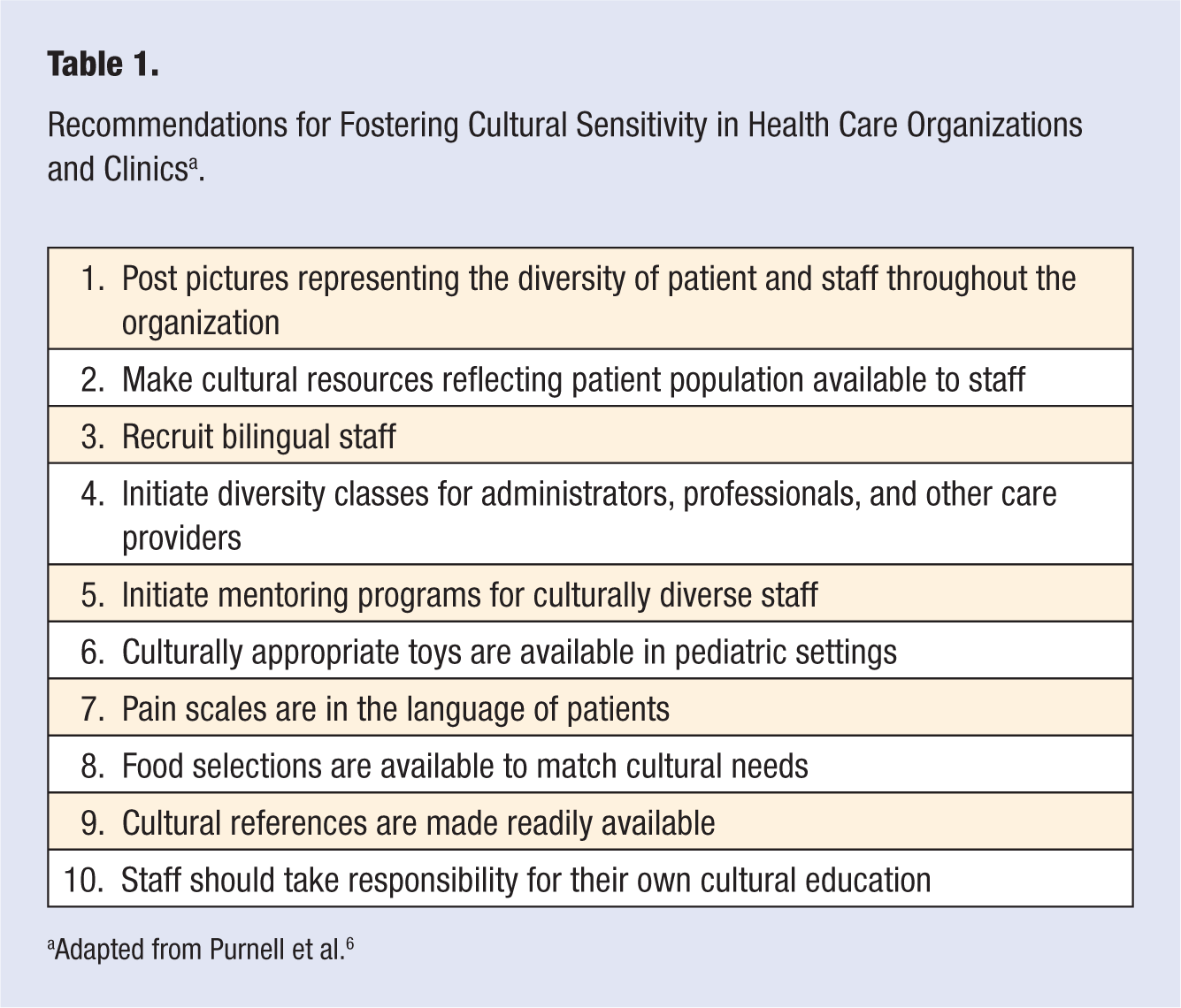
Adapted from Purnell et al. 6
Key Cultural Domains From the Purnell Model of Cultural Competence With Sample Questions to Ask to Determine Each a .
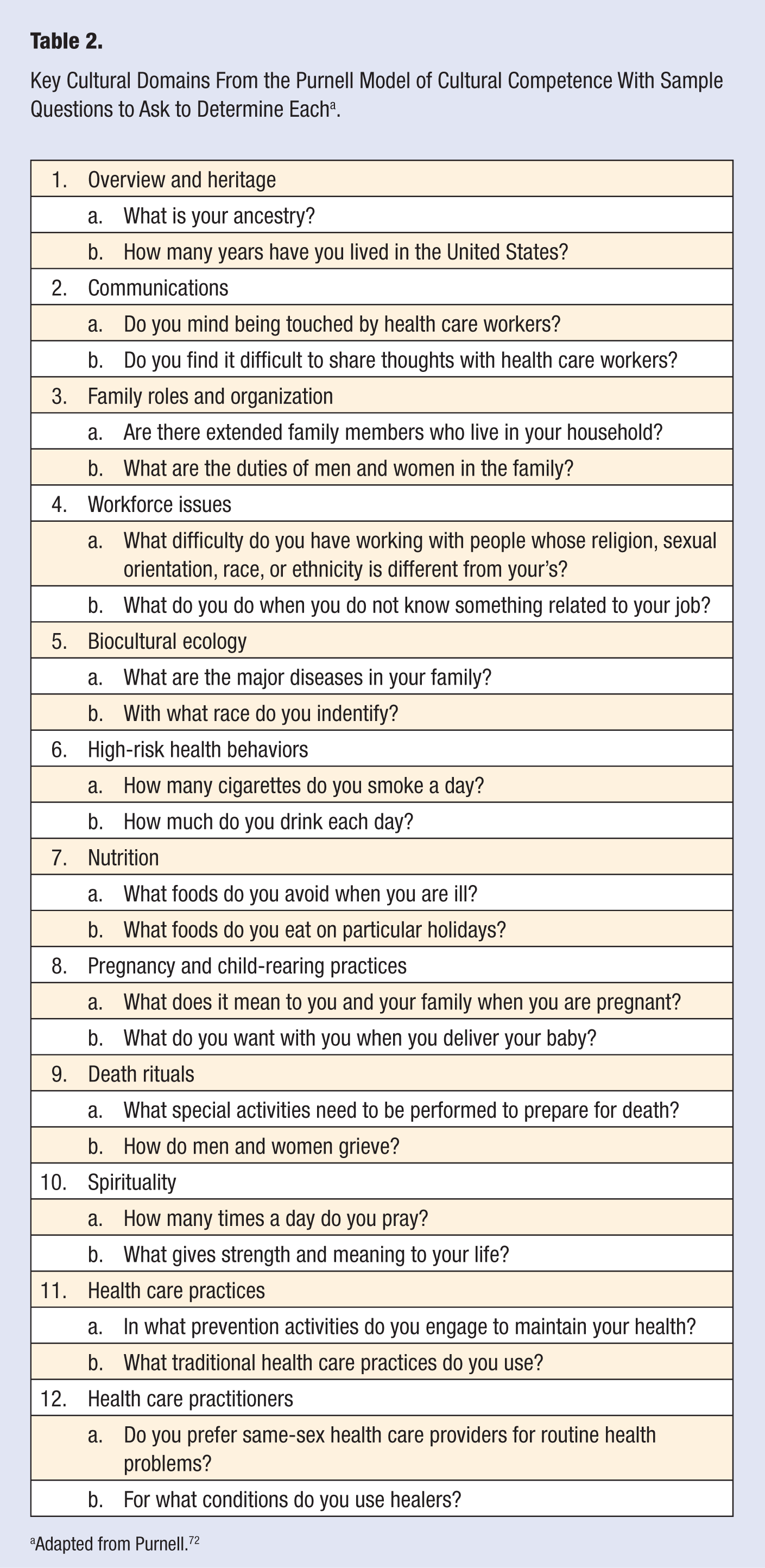
Adapted from Purnell. 72
In conclusion, it is important to acknowledge that many cultural variations exist within ethnic communities. Knowing how different cultural groups approach health and having a better understanding of how factors, such as acculturation, are important, and this can help clinicians, health care workers, and others with an interest in how lifestyle decisions are made be more culturally competent. The efforts to increase cultural competency in the treatment of mental and physical health6,23,74 are promising, but the wider health care arena needs to pay attention to the causes of health disparities and the role played by multicultural approaches to health. We need a better connection between health care and the community, so individuals can seek out treatments that best fit their cultural needs 75 and the manifold health disparities can be reduced.