
Abstract
Men’s health has been receiving increased attention in health care research and practice because of associated negative outcomes and men’s reluctance to seek help. Religion or religiosity, defined as involvement in an organized, structured community focused on moral code, and spirituality, defined as the subjective, mystical, and holistic interpretation of personal beliefs and behaviors, have been associated with positive health outcomes. Specifically, religion and spirituality mediate an increase in positive health outcomes and a decrease in risk factors through social and existential well-being. However, men seem to be less religious and spiritual compared with women, a potential problem as men may be missing an important pathway to health and wellness. This state-of-the-art review examines the intersections of religion, spirituality, and health and focuses on how religion and spirituality relate specifically to men’s health and health behaviors. Subsequently, 4 health problems with religious and spiritual implications are examined that have been identified in the literature as pertinent to men’s health: (a) prostate cancer screening and coping, (b) HIV/AIDS prevention and coping, (c) addictions, and (d) palliative care. Finally, suggestions are offered for clinicians to incorporate an understanding of religion and spirituality into their patient encounters.
Men’s health has been receiving increased attention in health care research and practice. The health community is working toward a broader conceptualization of men’s health, to identify assets that may increase men’s engagement in positive health behaviors, and to discover new intervention pathways that can improve men’s health and well-being. 1 This review focuses on religion and spirituality as an emergent positive component of men’s health, which health practitioners may be able to draw on in their interventions with male patients. One of the primary points to consider is that religion and spirituality are overlapping, yet distinct, constructs—each with subconstructs with additional definitions.2,3 For the purposes of this article, we define religion or religiosity as an individual’s involvement in an organized community that emphasizes doctrine, adherence to a moral code, and spiritual traditions of the institution.3,4 Spirituality is defined as a subjective, mystical, and holistic interpretation of personal beliefs and behaviors.3,5 Some may connote a value to the terms, but we do not consider one inherently “better” than the other.
The religious makeup of the United States has seen a great deal of change in the past few decades.
At a larger, societal level, religion and spirituality appear to be important to most Americans; approximately 81% identify with a specific religion, 12% with a secular spirituality, 95% believe in god or a higher power (eg, universal spirit), and 14.5 million Americans have practiced yoga (Table 1).6-8 Agnosticism and atheism is comparatively rare, representing a combined 4% of the population. The religious makeup of the United States has seen a great deal of change in the past few decades. The majority of change is a shifting of affiliation. The greatest losses of adherents are seen in the ranks of Protestantism, whereas Catholicism has remained more or less unchanged. The group that has seen the greatest increase is the “religious unaffiliated” category, which includes atheist/agnostic, people who describe religion as not important in their life, and the spiritual but not religious subgroups.6,10
Self-Identified Religious Affiliations, Beliefs, and Practices of Adults Living in the United States a .
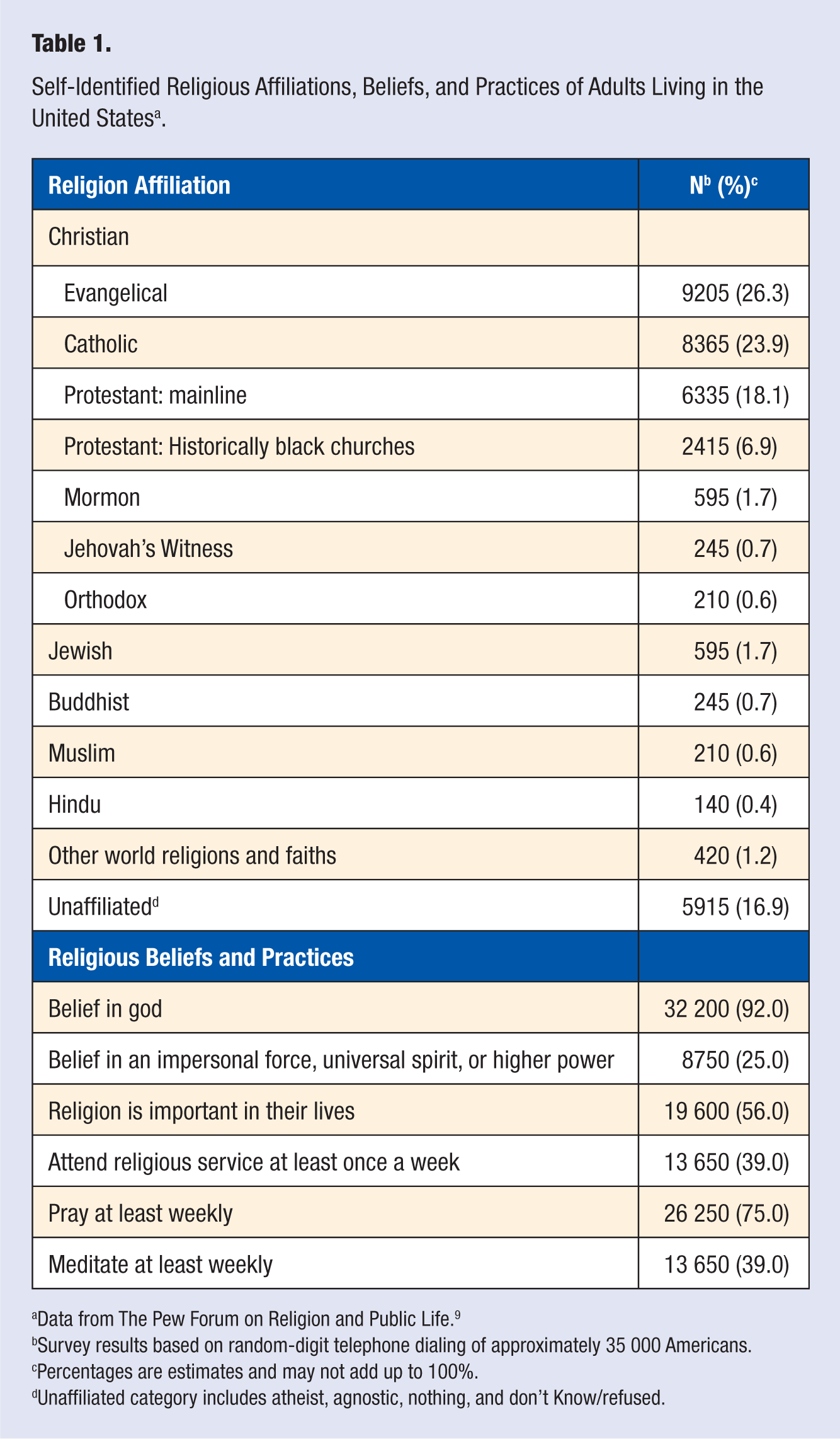
Data from The Pew Forum on Religion and Public Life. 9
Survey results based on random-digit telephone dialing of approximately 35 000 Americans.
Percentages are estimates and may not add up to 100%.
Unaffiliated category includes atheist, agnostic, nothing, and don’t Know/refused.
Religion and Spirituality Among Health Care Professionals
Health practitioners and researchers differ vastly from the general public in their religious and spiritual beliefs. In fact, of all scientists in the biological and medical fields, 32% believe in god and 19% in a universal spirit or higher power. 11 Furthermore, despite recent growth in relevant course offerings (eg, spirituality in medicine), training programs in health-related fields such as medicine and counseling typically do not integrate religious and spiritual competences into their curricula.12-14 Therefore, many health practitioners may be unfamiliar with the recent research in spirituality and health, lack the appropriate training, feel personally disconnected from its importance, and as a result, miss addressing a significant part of the patient’s life.13,15
Religious beliefs can influence patients’ decisions on medical options, prevent or delay disease detection, and cause spiritual-related stress affecting health outcomes. 15 At the same time, religious beliefs have been reported to influence health care providers’ medical decision making. For example, a study of 298 neonatologists found that 30% reported that their religious beliefs influenced their practice, whereas 96.3% reported that they are obliged to present all options to the family. Nearly 95% of neonatologists reported that their religious beliefs play no part in their approval to end life-sustaining treatments. 16 Ethical dilemmas in regard to medical decision making can exist when health care providers, as well as patients/patients’ families, do not share like-minded religious or spiritual beliefs. This conflict of interest is cause for a shared decision-making process that enlists disclosure of all options and a health care provider/patient consensus. 17
Indeed, most health scholarship that focuses on religion and spirituality begins by explaining why the medical, psychological, and various scientific communities historically devalue and do not include religion and spirituality. It is beyond the scope of this article to review all the reasons against the inclusion of religion and spirituality in medicine, but we highlight some of the main arguments and provide citations to seminal articles that offer a more in-depth analysis. In a summary of criticisms and concerns about religion and spirituality as those constructs that relate to health, Miller and Thoresen 18 offer 2 primary contentions. First, religion and spirituality have been associated with adverse health outcomes, studies linking religion and spirituality to positive health outcomes have been plagued with methodological flaws, difficulty defining the constructs, and a potential for harm when practitioners misuse religion and spirituality in practice. Secondly, there are strong historical assumptions that religion and spirituality cannot and should not be studied scientifically. More specifically, religion and spirituality focuses on subjective experiences of faith and of the supernatural, which are largely immeasurable and thus considered antithetical to an objective, scientific perspective. Prominent psychologists such as Sigmund Freud, Albert Ellis, and B. F. Skinner have considered religious and spiritual involvement signs of hysteria, neurosis, and negative psychological health—a view that permeated Western health sciences for much of the 20th century.18,19
Religion and Spirituality as Components of a Healthy Lifestyle
Religion and spirituality remerged in the empirical literature about 20 years ago with new links to positive health outcomes. In 2 recent prominent reviews of the literature, religion and spirituality were found to be associated with both mental health (eg, fewer completed suicides, increased coping with stress, fewer depressive symptoms) and physical health (eg, lower risk of cardiovascular disease, improved recovery from acute care) outcomes.20,21 Additional positive outcomes associated with religion and spirituality include reduced risk to nicotine and substance abuse, reduced risk for psychological externalizing disorders, 22 enhanced coping will serious illness and end-of-life issues 23 if patients garner strength and optimism from their religion and spirituality, 21 medication adherence for serious illness, 24 fulfilling social lifestyle, 25 and overall holistic well-being. 26 Religion and spirituality have been found to be both a mediating factor in well-being and as having a direct effect on health.18,27 Scholars continue to find negative associations between religion and spirituality such as increased risk for psychological internalizing and externalizing disorders 22 and coping with serious illness and life events, if patients feel abandoned by their religion and spirituality.21,28
Although the exact mechanism to explain how and why religion and spirituality are associated with positive health outcomes is yet to be identified, there is compelling research across several disciplines (eg, psychology, nursing, psychiatry) that has identified 2 common explanations for religion/spirituality’s effect on health (Figure 1): (a) religion and spirituality are a protective resource that prevents the development of disease in healthy people and (b) religion and spirituality are a coping resource that buffers the impact of diseases on patients.20,21,29-31 More specifically, a consistent finding is that attending church services protects against death, likely because church attendance elicits the presence of other healthy, more general, mediating factors such as social support, promotion of healthy lifestyle choices, increased positive emotions, a sense of meaning, and self-worth. 21 Other scholars20,31 highlight religion and spirituality as an effective coping behavior in the face of life distress and stress. The use of religion and spirituality as a coping behavior has contributed to a positive worldview, community role models, hope and optimism, a sense of purpose and comfort, feeling blessed and empowered, and decreased loneliness and social isolation.
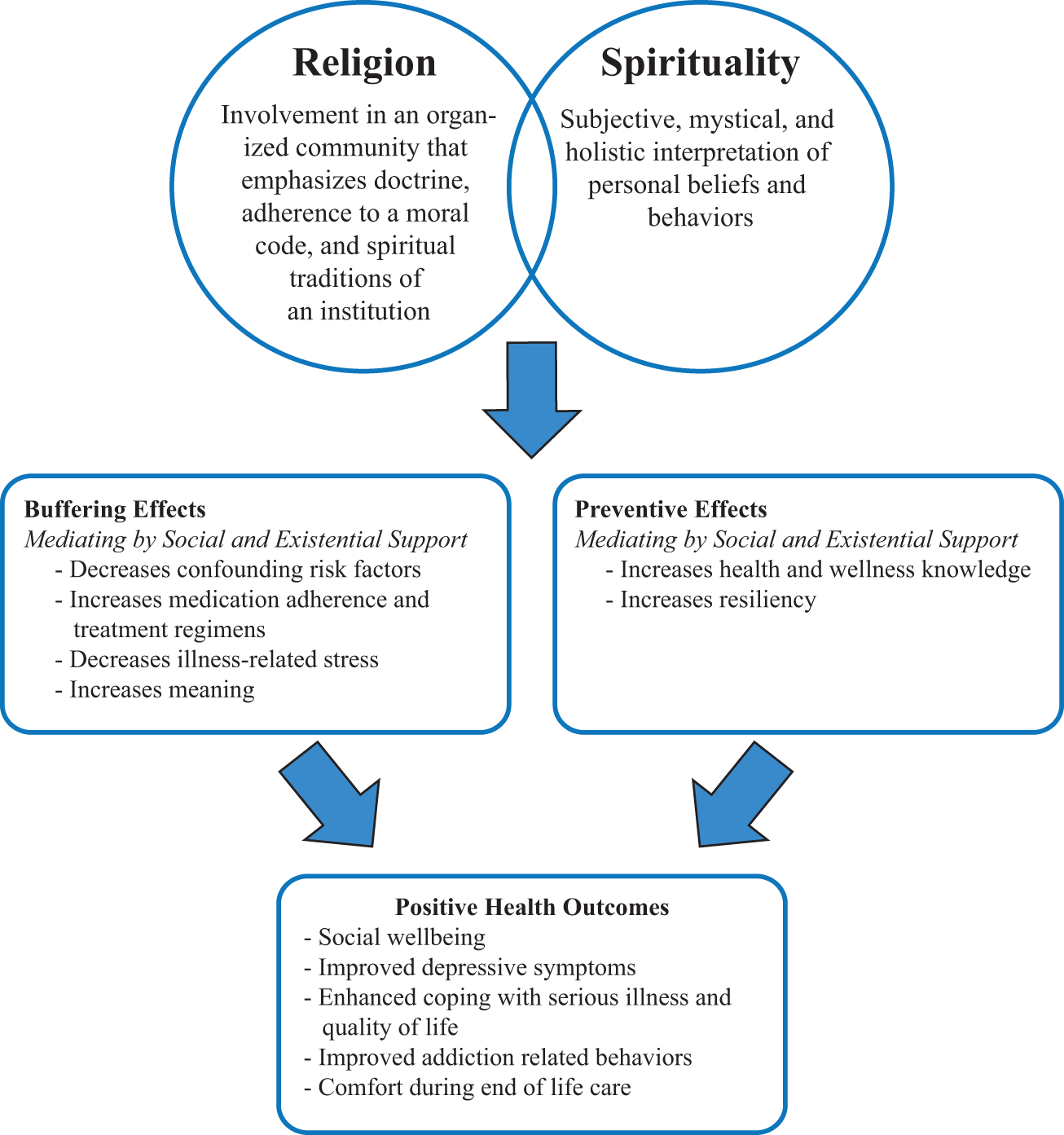
Mediating Effects of Religion and Spirituality on Positive Health Outcomes With Men.
The healthy lifestyle pathway is supported by Reindl-Benjamins and Brown, 32 who reported that, in general, individuals who report religion as important to their lives also reported high use of preventive services such as influenza shots, mammograms, breast self-examinations, prostate screenings, and cholesterol tests. Dyer 29 expanded on the healthy lifestyle choices pathway by describing a few examples from specific religious denominations; Seventh-Day Adventists maintain a healthy diet as part of their religiosity and Mormon women have some of the lowest rates of breast cancer because of common lifestyle behaviors of breast-feeding and low alcohol consumption. Similarly, Hill and Pargament 30 sought to identify pathways that are uniquely inherent to religion and spirituality rather than general mediators; their research found that perceived closeness to god, religion and spirituality as an overarching and central framework to guide life, the uniqueness of religious support across the life span from a community with shared values, and struggles associated with religion and spirituality all helped to explain the associations with both positive and negative health outcomes.
Controversy Surrounding Religion and Spirituality in Health Care
Not surprisingly, 2 “camps” seem present in the current social–psychological–medical scholarship, those that continue to believe that religion and spirituality have no place in scientific endeavors/religious and spiritual activity does not promote health 33 and those that believe that religion and spirituality are important components of holistic health care of individuals and groups. 25 The 2 camps have been discussed as the “Koenig–Sloan controversy” to indicate the 2 primary provocateurs of the debate (Harold G. Koenig, MD, of Duke University as “pro-religion and spirituality” and Richard P. Sloan, PhD, of Columbia University as “anti-religion and spirituality”). 34 The controversy is summarized nicely by Berlinger34(p686): “depending on which article one is reading or which conference one is attending, the connection between spirituality and medicine is clinically proven, presumed, possible, debatable, unproven, unknowable, hazardous, or downright harmful.” Complicating the controversy is the general agreement that religion and spirituality are complex and latent constructs that are difficult to define and measure. 35
Recent scholarship has made progress to operationalize religion and spirituality with reliable and valid measures, identifying empirical support for the use of religion and spirituality in treatment approaches, and placing the discourse in a scientific framework. This review aligns with those efforts by acknowledging that (a) many individuals have religious and spiritual beliefs and experiences, and these may differ from the practitioner; (b) by being aware of the religious and spiritual beliefs and experiences of their patients, health practitioners can better care for them; and (c) health practitioners can draw on empirically based literature when offering interventions from a religious and spiritual perspective to their patients. Competence to respond appropriately to a patient’s religious and spiritual experience has been found to improve treatment efficacy, promote a positive therapeutic relationship, and increase patient wellness. 30
Religion and Spirituality in Men
A comprehensive, analytic review of the extant literature of religion/spirituality related to men is missing, despite the existence of literature reviews focused on religion, spirituality, and health.19-21,30,36-38 A focus on men alone is required because research consistently finds that men are generally less religious than women and men’s construction of their masculinity has a negative correlation with religiosity.35,39-45 Thus, men may be inhibiting their ability to tap into an existing asset to their health, and practitioners may be prone to ignore or “write off” the religious and spiritual experiences of men. Little guidance exists on how health practitioners can explore men’s religious and spiritual lives and draw on that exploration in an intervention strategy. Therefore, the primary purpose of this article is to discuss how religion and spirituality fit into a broader treatment approach in the lifestyle medicine of men’s health and wellness.
According to most empirical data, men are considered less religious than women as measured on several indices, such as weekly attendance at a church service; a belief in a universal or personal god; and affiliation with a religion, daily prayer, and stated importance of religion. 6 Overall, the reasons for the difference between men and women in regard to spirituality and religion are complex, as researchers have identified and debated demographic, social, cultural, and biological factors.35,40 For example, age seems to be a prominent factor as some research has found that younger men are generally less religious than older men.43,45 Other scholars have pointed to the gender role socialization of boys and men, which values self-reliance, risk taking, lack of help seeking, and avoidance of femininity. 46 According to the gender role socialization theory, many men may view religion and spiritual activities as feminine (ie, practiced by women), safe, or a form of help seeking, which would lead to avoidance of spiritual activity and religious involvement. 46 Preliminary research points to biological bases to the gender disparity. For example, Miller and Hoffmann 42 contend that men have an innate predisposition to risky behavior, whereas D’Onofrio et al 47 conclude that women have a genetic component that contributes to church attendance and religiously right social attitudes. In a sample of male twins from Minnesota, research found that religiousness was genetically influenced more so in adulthood than childhood. 48 Although Koenig et al 48 focus on the heritability of religiousness in the aging process, other scholars have attributed older men’s religiousness to sociocultural factors such as men’s acquisition of a feminine worldview, a downplaying of traditional masculinity, and a desire to live a healthier (less risky) lifestyle.43-45,47
Religion, Spirituality, and Men’s Health Behaviors
One of the main problems that have emerged from this research is not necessarily that many men are less religious and spiritual than women are, but that men are missing out on a potentially valuable source of support, coping, and a catalyst for adopting positive health behaviors. The research involving men, religion/spirituality, and their health behaviors is relatively scant, but has begun to focus on 4 major health concerns: (a) prostate cancer screening and coping, (b) HIV/AIDS prevention and coping, (c) addictions, and (d) palliative care. The following section details practical and empirical efforts to integrate religion and spirituality with men’s health behaviors.
Prostate Cancer
Religion and spirituality influence men with prostate cancer via prevention, 49 treatment outcomes, 50 and coping. 51 Preventive intervention strategies with African American men were shown to be more effective if they included a religious or spiritual component and especially effective if the intervention originated from a member of the church. In a study by Holt and colleagues, informed decision making about prostate screenings was improved. 49 Informed decision making at times can involve a shared decision making with the health practitioner to include acknowledgement of personal values. 52 The inclusion of religious and spiritual interventions also increased patient knowledge of options and consequences, and increased the likelihood of getting a screening. 49 The success of religious and spiritual interventions within the African American population seem to be effective because they tend to view their health through a spiritual lens and believe religion and spirituality are important controlling factors for their health. 53 Thus, men who hold religion and spirituality as a high controlling factor in their decision-making process may take into account a connection with a health practitioner on a spiritual level.
Beyond prevention, religion and spirituality is ever-present in the lives of theistic men who are coping with a prostate cancer diagnosis.50,51 This section focuses on religious and spiritual notions from the patient’s perspective and provides empirical support for links to positive health outcomes. Health behaviors that utilize religion and spirituality constructs are praying, receiving support, and general coping; these were the guiding forces for positive health outcomes that include trust in health practitioners, facing a diagnosis, treatment choices, and day-to-day living. 51 Men who had a higher level of spirituality also had an overall higher health-related quality of life and were better adept at coping with their prostate cancer.50,54,55 The more specific subconstruct of intrinsic religion showed a small mediating negative relationship with depression in men with prostate cancer but the relationship with spirituality was much stronger. Intrinsic religiosity and spirituality were associated with the ability to make meaning and find peace in a diagnosis. 54 When a patient places the locus of control in their religious or spiritual beliefs, interventions focusing on trust in from health practitioners are important. By encouraging conversation, expressing compassion, and taking time to actively listen, this trust can be achieved. 51
HIV/AIDS
The Centers for Disease Control and Prevention (CDC) 56 reports that efforts between 1991 and 2006 have succeeded in the prevention of some 350 000 cases of HIV transmissions in the United States, and this has saved an estimated $125 billion in medical costs. Furthermore, the CDC has formally recognized the powerful impact that faith-based interventions have on the prevention of HIV/AIDS. 57 African American and Hispanic Americans have a higher prevalence and are more likely to contract HIV/AIDS. 58 Because Hispanics 59 and African Americans 53 tend to see their health as a spiritual or holistic phenomenon, spiritual or religious interventions with these patients are well suited for prevention. 60 In a review of 4 faith-based HIV/AIDS education programs tailored for African American churches, Francis and Liverpool 61 found that these programs are effective in preventing HIV/AIDS infection. They continued to emphasize the importance of working alongside public health officials, and they encourage a more rigorous program evaluation protocol. Overall, they are effective on a community level as a guide to a healthy lifestyle.
Modern HIV/AIDS antiretroviral medications have drastically improved and have increased the lifespan of infected persons dramatically. Patients still have to deal with health consequences related to their HIV/AIDS infections, and medicine has made a call to investigate lifestyle changes to further improve outcomes. 62 Spiritual growth and religious coping are 2 health behaviors that have received consideration. Spiritual growth measures one’s sense of purpose, connection to something greater, and course toward self-actualization. Religious coping measures the effectiveness of utilizing institutional structures (ie, attending service, speaking with clergy for counsel) to assist them in coping with negative life events, in this case HIV/AIDS. Spiritual growth of HIV infected men has been found to improve health-related quality of life, social functioning, and mental and emotional well-being, 63 whereas religious coping had mixed results depending on the sexual orientation of the man. One study measuring religious coping of HIV/AIDS infected men of all sexual orientations found that coping strategies had a positive impact on depression and buffered against confounding risk factors (increased alcohol, tobacco, and illegal drug use). 64 Conversely, a study of gay and bisexual men found that religious coping increased on HIV positive tests, but engagement in the use of illegal drugs also increased, which was attributed to the gay and bisexual community’s acceptance of drug use as a coping mechanism. 65 Longitudinal spiritual growth had the greatest effect in both populations leading to a reduction of health-related stress 65 and depression. 66 Researchers suggest interventions focusing on existential issues and the integration of healthy worldviews to improve health-related quality of life via spiritual growth.63,64 In addition to improving quality of life, religiosity has been linked to improving medication adherence24,66 and even has been shown to reduce side effects from the medication. 66
Addictions
Gender differences seem to exist in such addictive behaviors as substance use, online viewing of pornography, and gambling.67,68 In the latest survey of addiction treatment facilities, there were more than 1.13 million patients enrolled in a state-approved treatment program and men were approximately twice as likely than were women to be diagnosed as substance dependent. 69 Sexual addiction rates illustrate an even greater gender discrepancy with an estimated 8% of men, opposed to 3% of women, exhibiting compulsive sexual behaviors. 70 Addictive gambling behaviors show similar prevalence rates with 2 times more men diagnosed than women. 71 These addictive behaviors also intersect with men’s spiritual and religious identities and have implications for treatment and clinical conceptualization.68,72,73 For example, some religious belief systems may view addictions as a sin or deviant behavior that is to be punished or repented. Such a macro-level perspective may filter down to individual men who adopt a negative self-image and experience shame and guilt for addictive behavior that many health practitioners consider a medical disease. 74 This section focuses on the intersection between men’s addictive behaviors and spirituality/religion to promote more sensitive treatment and prevention.
Substance addiction
Substance addiction is associated with a wide array of negative biological and psychological outcomes such as depression, HIV/AIDS, hepatitis, blindness, heart disease, seizures, and death from overdose. 75 There are an estimated 10 170 non-faith-based treatment programs and 527 faith-based treatment programs for substance abuse and addiction. 76 However, that comparative data may be misleading as Alcoholics Anonymous, whose mission and steps include a spiritual component, estimates to have 57 905 groups in the United States. 77 Indeed, many health practitioners refer highly religious patients to12-step programs with a spiritual component. 78 With men being less religious than women, 12-step programs with an overt spirituality component may not be the most appropriate referral option. However, research indicates that some men considered a spiritual component to be beneficial to their recovery and a contributor to social support. 79 Particularly for African American men, high religiosity was predictive of treatment completion for substance abuse/addiction. 80 Even men of low religiosity and nonreligious men were found to benefit from spirituality in their substance abuse treatment, if used properly. 81 For example, men found integration of spirituality to be best placed in the maintenance stage of treatment or toward the end of the treatment program, perhaps after initial resistance and defenses to the treatment have subsided. 81 Addiction interventions using Buddhist philosophies and spirituality, such as mindfulness, meditation, and yoga exercises, have been found to facilitate continued sobriety after traditional approaches have ended.82,83 Religion and spirituality may contribute to optimism, support, and resiliency among substance abuse patients. 84 Therefore, a spiritual component to substance addiction treatment may be warranted and contribute to improved care, treatment completion and maintenance, and patient hardiness for many men.
sexually compulsive behavior and internet pornography addiction
Sexual addiction is an overarching term used to describe sexually compulsive behaviors with negative physical, psychological, and social consequences and are acted on despite those negative consequences.70,85 Sexual addiction of various kinds is associated with increased feelings of guilt or shame, depression, anxiety, and increased exposure to sexually transmitted diseases.86,87 Though sexual addiction is a readily accepted term clinically and in the literature, the American Psychiatric Association has yet to acknowledge a formal diagnosis,70,88 and some 8% of men demonstrate negative health behaviors consistent with the accepted definition of sexual addiction. 70 One prominent example of sexual compulsive behavior is Internet pornography addiction. Internet pornography is a billion-dollar business, increasing the accessibility of material to fulfill sexual compulsions. 89 Although not all men addicted to pornography see themselves as having a problem, men suffering from sexual addiction often view women, other men, and themselves in maladaptive ways. For example, Carnes 85 describes 4 negative beliefs common in sexually addicted men:
Self-image: “I am basically a bad, unworthy person”
Relationships: “No one would love me as I am”
Needs: “My needs are never going to be met if I have to rely on others”
Sexuality: “Sex is my most important need.”
Some men are able to view pornography without negative emotional and cognitive consequences, whereas other men experience emotional and cognitive turmoil, which has been attributed to a lack of control over unwanted sexual thoughts and addictive behaviors that are contrary to their personal values and beliefs. 90 For patients struggling with a sexual addiction, spirituality can be a cause of psychological conflict 91 and a source of recovery.85,89 Religious views about sexuality may also magnify stigmatization about sexual addictions and serve as an additional barrier to men’s difficulties with help seeking.92,93
The empirical literature focusing on sexual addiction, men, and spirituality is based primarily on samples of participants identifying as Christians. For Christian men, sexual addiction is counter to beliefs about the sanctity of marriage and may contribute to conflict with their spouse and family. 94 Christian college-aged men, who are not married but are challenged with the religious tenets that promote sexual abstinence prior to marriage, masturbation and pornography viewing may be behaviors used to satisfy intimate needs and change affective states. 95 Christian men at college, particularly those attending evangelical universities, appear to develop sexual addictions at higher rates than non-Christian men but may also be over diagnosed because of the religious context. 91
A combination of behavioral therapy and medication (selective serotonin reuptake inhibitors [SSRIs], Naltrexone) appears to be effective in treating sexual addictions with spiritual/religious men.86,95 Behavioral therapy, which focuses on replacing maladaptive behaviors with adaptive behaviors, is enhanced with “spiritual strengthening.” Spiritual strengthening refers to spiritual direction and work to improve one’s acceptance of meaning, values, and beliefs. 89 Although many health practitioners may be competent in behavioral therapy, providing men with spiritual strengthening may be uncomfortable. As a result, referring patients to a spiritual/religious leader may be warranted. Group therapy has found success because of the nature of disclosure and the ability to gain trust among individuals with similar compulsions. 96 Aversion therapy, stimulus satiation, and degradation recovery has also found a good deal of success. 97 Treatment from health practitioners, be it psychological or pharmacological in nature, will be more powerful with a focus on changing beliefs and affect, as well as a spiritual strengthening congruent with their preexisting spiritual notions.
Gambling addiction
Gambling addiction is associated with a decline in quality of life, mental health, an increase in co-occurring addictions and psychiatric disorders, relationship problems, and occurs at higher rates in men as opposed to women.68,87,98 Problem and pathological gambling among men is observed at similar levels across races in some studies, but at higher rates in African American men in other studies, which has been attributed to a combination of men’s poor help-seeking behaviors and health services that are less attractive to minority men.1,67 Hodge et al 99 found that among their prominently Hispanic sample, 3 distinct religious and spiritual lifestyle subgroups were formed: Nonreligious/nonspiritual, spiritual and religious, and spiritual but not religious. Consistent with their hypothesis, the spiritual and religious group demonstrated the least amount of gambling behaviors and the spiritual but not religious group demonstrated the greatest amount of gambling behaviors. Hoffmann 100 found that religious service attendance decreased gambling behaviors, which adds support to the mediating effects of a religious community/social support as a protective factor.99,100
Gamblers Anonymous is a well-known support group. Gamblers Anonymous places less emphasis on spirituality than other 12-step programs (eg, Alcoholic Anonymous), because problem gamblers often hold irrational beliefs focusing on supernatural wishes to win big, stack odds in their favor, and get lucky. 101 Studies by both Ferentzy et al 101 and Hodge et al 99 point to the idea that spirituality may work as a risk factor with problem gambling behaviors. A randomized clinical trial involving cognitive behavioral therapy and the 12-step program Gamblers Anonymous showed no significant differences in gambling outcomes between the 2 treatments, but did show that both approaches succeed in significant reduction of gambling behaviors. 102 Along with cognitive behavioral therapy and Gamblers Anonymous, brief intervention strategies such as motivational interviewing, have proven to be an effective complementary treatment with gambling disorders and can assist increased positive health outcomes in both men and women.67,102
Palliative Care
Addressing religion/spirituality is important to palliative care because end-of-life issues inevitability bring about increased awareness of existential issues, issues of mortality, and what comes after life here on earth (eg, heaven/hell, reincarnation).103,104 Similar to other lines of research, health practitioners tend to place less importance on spiritual interventions within palliative care compared with patients, which may be because of the lack of empirical evidence supporting spiritual interventions and assessments.105,106 Preliminary research indicates that religious coping has been shown to improve resiliency and increase the likelihood of patients receiving life-prolonging medical interventions while undergoing end-of-life treatment. 107
Many intersections of gender, sexual orientation, religious affiliation, and ethnicity emerged in research regarding palliative care with men. Gay men overwhelmingly preferred relieving pain to life-prolonging medical interventions. 108 Duffy et al 109 looked at the ethnic differences in men and how that translated to end-of-life preferences in care. For example, Arab Muslims did not cite the importance of spiritual concerns, whereas Arab Christians felt spiritual concerns to be very important. African American Christians and Hispanic men shared similar negative feelings about doctors and medical interventions but were not opposed to medical help with ending their life. Caucasian men who identified as highly religious wanted to know the prognosis and preferred to end their life in their own home. 109
Many ethical concerns have surrounded the issue of spiritual or religiously based decisions in end-of-life care, but the aim remains to maintain individualized patient-centered approaches to ameliorating a person’s last days.110,111 When health practitioners are consulting with patients in palliative or end-of-life care, practitioner/patient interactions are important. Many times the onus is on the practitioner to respond appropriately to the patient’s religious or spiritual concerns. By listening to a patient’s beliefs, a practitioner can discuss concerns and address religiously based end-of-life decisions to provide informed treatment and improved comfort. 112
Clinical Recommendations
Intervening with men to improve their health and increase their engagement in positive health behaviors is difficult given social constructions of masculinity and traditional masculine gender-role socialization.1,113 Integrating religion/spirituality into interventions may also be difficult because men have been found to be less religious than women and avoid religion/spiritual activities in order to be more masculine.46,114 However, improving men’s health and increasing their engagement in health behaviors may require men to engage in nonstereotyped masculine behavior. 114 Further, some helpful strategies to integrate religion/spirituality into interventions that enhance health and well-being have been identified in the empirical literature. Thus, health practitioners are encouraged to implement some of these strategies, which are described below, with their male patients in order to tap into a new pathway intended to help men live healthier lifestyles.
Health practitioner self-awareness has been identified as a natural starting point for religious/spiritual interventions with patients.115,116 Engaging in self-reflection and self-awareness-raising helps health practitioners to know and understand their own beliefs and values related to religion and spirituality, which facilitates a nonjudgmental approach with the diversity of religious/spiritual beliefs of patients and keeps the approach patient centered.
115
Second, health practitioners are able to gain a better understanding of their patients’ religious and spiritual beliefs by conducting a “Spiritual Assessment” or gathering a “Spiritual History.”38,115-117 According to Koenig,
117
gathering a spiritual history from your patient entails asking your patient 5 simple questions:
(1) Do your religious or spiritual beliefs provide comfort and support or do they cause stress? (2) How would these beliefs influence your medical decisions if you become really sick? (3) Do you have any beliefs that might interfere or conflict with your medical care? (4) Are you a member of a religious or spiritual community and is it supportive? (5) Do you have any spiritual needs that someone should address?
A spiritual history allows a health practitioner to gain valuable information that may be a catalyst for additional interventions. Furthermore, a spiritual history is an opportunity for patients to be heard and validated about their religious/spiritual beliefs 19 and to inform the health practitioner if a referral to a religious/spiritual healer (eg, rabbi, priest, clergy) would be helpful to the patients.19,54
In a spiritual history/assessment with male patients, it is important for health practitioners to also assess a man’s conformity to traditional masculine norms. Simply asking, “How would you describe yourself as a man?” would help gauge if the male patient would be resistant to discussing religion and spirituality (ie, more traditional men, more resistant). With less resistant male patients, introducing overt spiritual/religious interventions such as prayer, meditation, mindfulness exercises may be received with gratitude.115,118 With more resistant male patients, health practitioners may find remaining nonconfrontational while educating men about the health benefits of religion/spirituality to facilitate patient buy-in. Cecero et al 119 found that men are more inclined to focus on building a secure relationship with god in times of trial as their coping mechanism rather than overt signs of religiosity. Therefore, health practitioners may facilitate internal spiritual/religious strength with men rather than suggesting an external activity (eg, attending a religious service). For example, a health practitioner could ask a male patient, “During times of stress and difficulty, people cope in very different ways. Some people rely on their religious and spiritual beliefs. Have your religious or spiritual beliefs been helpful to you?” Finally, men may also prefer the spiritual intervention of “being there,” 120 which entails the health practitioner to maintain a respectful and peaceful presence with the patient without “a doing to”. Milstein 120 contends that “being there” can help create a space for patients and their families to find meaning, engage in their own spiritual/religious practice of healing, and contribute to a model of holistic care.
Summary
With the necessary increased attention being paid to men’s health in the past few decades, there is a growing need to understand the various social determinants that contribute positively and negatively to men’s health. Religion and spirituality is one component that may have major influences on men’s lives, health, and health behaviors. Interventions focused on male patients have been shown to decrease confounding risk factors and illness-related stress while increasing health knowledge, resiliency, life meaning, and adherence to treatment regimens. The literature consistently describes the many ways that men exhibit lower levels of religiosity than do women. However, the evidence demonstrates that men’s conception of religion and spirituality does have a mediating and buffering effect on positive health outcomes in the 4 areas of prostate, HIV/AIDS, addictions, and palliative care. Due to likely religious and spiritual differences between health practitioners and patients, we encourage health practitioners to engage in self-reflection about their beliefs and attitudes. Increased self-awareness among health practitioners may facilitate a better understanding of how religion and spirituality impact the health of male patients. Thus, health practitioners may be more effective and comfortable incorporating these important components of health in their encounters with male patients.