
Abstract
Decades of research now support the positive relationship of religion/spirituality (R/S) with physical health, mental health, morbidity, and mortality. While lifestyle medicine (LM) practitioners often recognize R/S as important, they can face common challenges of how to integrate R/S into their holistic, patient-centered care. To help, this article presents a faith-practice framework, as a starting point for considering incorporating R/S into LM practice—in light of common concerns and challenges, as a guide for patient-centered care through adjusting lifestyle prescriptions to accommodate individualized R/S beliefs and practices for improved health behavior and outcomes, and as an encouragement to stimulate openness for positive, thoughtful discussion into the future of R/S in LM practice and research.
“Religion varies greatly amongst religious traditions, and affects how that religion is translated into personal praxis that can impact health and well-being.”
Introduction
At its core, lifestyle medicine (LM) is holistic, characterized by an emphasis on the whole person in the prevention, treatment, and reversal of disease—a breadth and depth. Breadth, at the practice or clinical level, promotes an interdisciplinary approach with involvement from a broader team of practitioners (e.g., dietitians, exercise specialists, health coaches) to assist in lifestyle prescriptions. At the patient or client level, a widened lens recognizes the individual complexities that either inhibit or assist in adoption of lifestyle prescriptions. Depth considers how LM can deepen one’s practice, and more specifically, the patient-practitioner relationship—considering each patient, as a person, with individual differences, and personally meaningful beliefs and histories. In fact, a presumed pillar of evidence-based practice is centered around knowing and engaging patients’ beliefs, preferences, values, and cultures in their patient-centered care.1,2
Through such a lens, health behavior is seen as a confluence of multiple factors or dimensions, such as emotional, social, intellectual, environmental, financial, and of interest here, religion/spirituality (R/S), of which increase or decrease probability of healthy lifestyle adoption. This perspective also encourages classical approaches to patient care, such as virtue ethics, personal morality, and of other deeper dimensions of the role of R/S that has a long history in the culture, education, and practice of medicine across various subspecialties.3–11
Decades of research now support the positive relationship of R/S with physical health, mental health, morbidity, and mortality. In lieu of re-reviewing the expansive literature here, we recommend previously published reviews of the evidence.3,12–16 Notably, religious service attendance has been found to be associated with a significantly lower risk of all-cause, cardiovascular, and cancer mortality,17,18 and can hold similar effect sizes on all-cause mortality to those from other important preventative lifestyle prescriptions, including physical activity, tobacco smoking cessation, and consumption of fruits and vegetables. 19 With the recognition of methodological concerns (e.g., study designs, controlling for confounding factors, and the possibility of reverse causation), the evidence in support of R/S on physical and mental health has become increasingly strong—providing ample support of the inclusion R/S in LM practice.12,14,15,20
Yet, with its historical complexities and controversies, practitioners of contemporary medicine might choose to disconnect or renunciate R/S from patient care, and more generally, medicine from its historical integration with religion and its traditional role as a “moral community.”21–23 In contrast, LM practitioners can also recognize R/S as integral, especially within holistic, whole person health models, 24 but face common challenges of how to integrate R/S into their patient-centered care. To date, however, there has been little attention to the intersection of R/S and LM, and how to structure its application. Thus, the purpose of this article is to introduce such a framework for practitioners, as a starting point, and encourage further conversation on the important role of R/S in LM practice.
Religion, Spirituality, and Lifestyle Medicine
In general, religious values and beliefs are important and prevalent aspects of many patients’ daily lives. Nationally, the Pew Religious Landscape Study has found that nearly 80% of polled adults identify with a religious affiliation (70% Christian), and nearly 80% self-report that religion plays an “important” to “very important” role in their lives. 25 These data suggest that adults, and subsequently patients, are making many decisions in their lives based on their religious values and beliefs, and decisions related to health is no exception—even if the practitioner does not recognize such an influence.26,27
While many historical and philosophical reasons abound for the discomfort of bridging R/S with healthcare,9,28 more practical reasons often center around perceived practitioner barriers, such as poor knowledge, having a lack of training and time, and being afraid to impose one’s own religion or disrespect the patient.29,30 However, R/S can be an essential component of LM and influence its pillars—offering opportunities for social connection, altering motivation and choices around diet and risky substances, coping with stress and shaping perceptions of body and health. More deeply, R/S influences the relationship of meaning of life and intrinsic motivation to pursue lifestyle choices that are consistent with R/S values, beliefs, and practices. As shown in Figure 1, this perspective of the meaningfulness, essentiality, and role of R/S in a LM and/or whole health model provides various models for future discussion: (a) R/S, alongside meaning and purpose, serving as a foundation for holding up and influencing impact within all LM pillars, (b) R/S serving as the deeper foundation, underlying and establishing meaning and purpose, which then influence the impact within LM pillars, or (c) R/S serving as an additional LM pillar. Example perspectives of the essentiality and role of religion/spirituality (R/S) in whole health models that include lifestyle medicine (LM) pillars.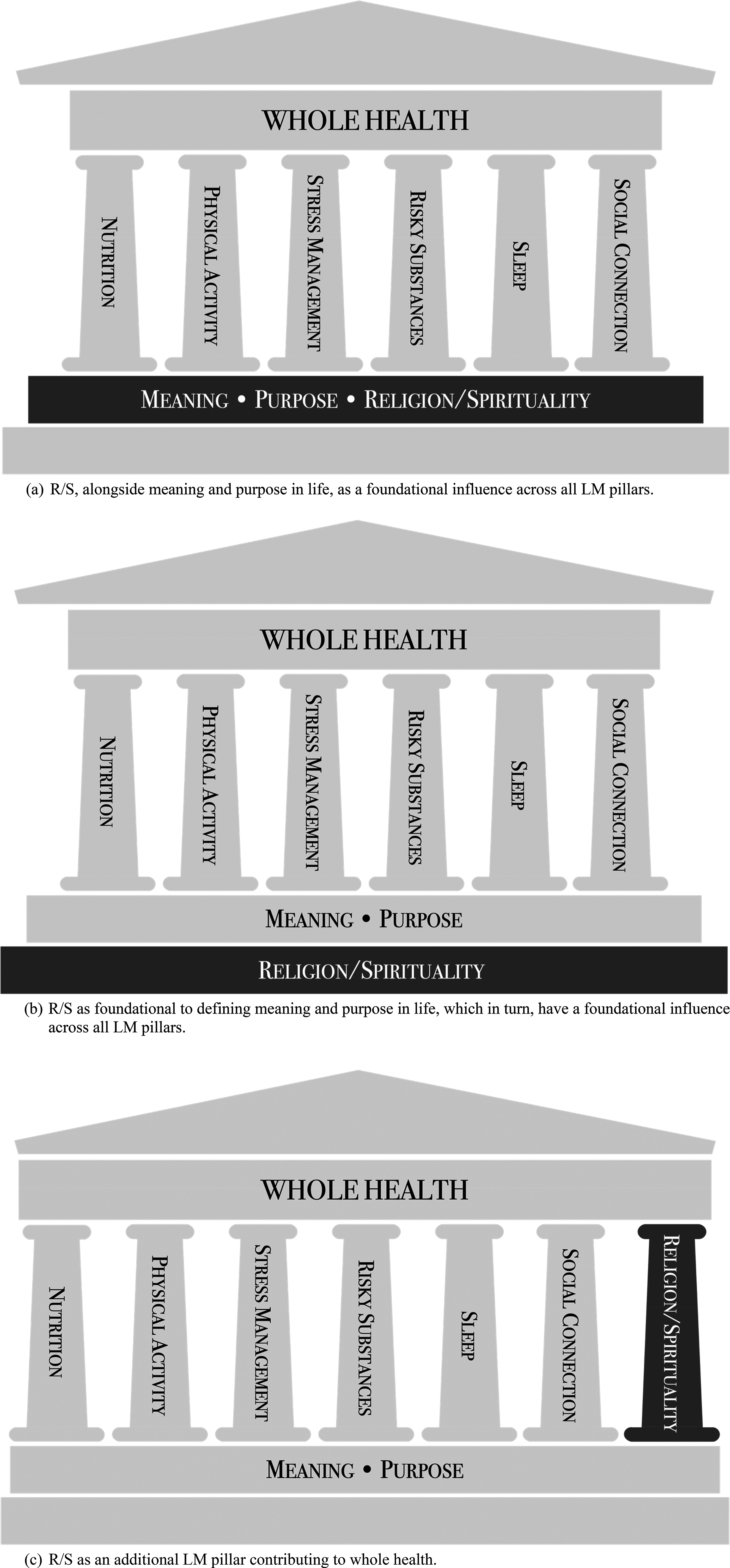
In Context
The contextualizing and defining of religion or spirituality is a classical problem, varying greatly between the lens from which it is approached—within philosophy, sociology, anthropology, psychology, ethics, medicine, and so on.3,31,32 Thus, any attempt to create a definition of religion or its relation to spirituality, is perhaps an impossible task. With that said, what follows is an attempt to express contemporary considerations, as they relate to research and practice relevant to LM, while encouraging deeper considerations to this topic.
Religiosity
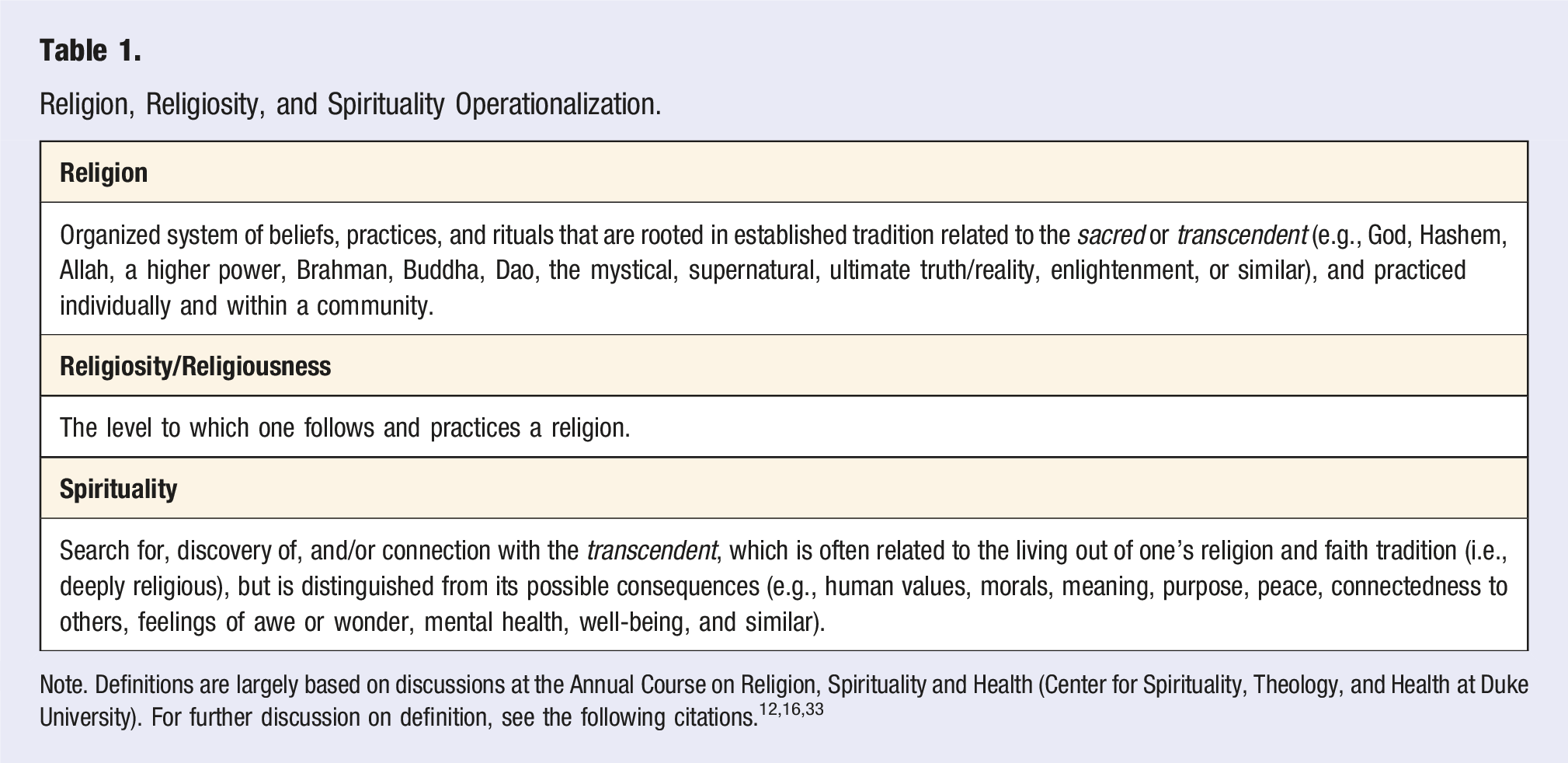
Religion, Religiosity, and Spirituality Operationalization.
Spirituality
Spirituality, while historically rooted in and based on religion, its contemporary use is often vague and defined by individuals, thus it is difficult to produce a single definition that encompasses the varied perspectives on what spirituality represents. This vagueness of meaning can lead to comfort for the use of the term “spirituality,” especially in clinical and public health settings, and perhaps in preference over the term “religion.”
Traditionally, spirituality has overlapped to varying degrees with religiosity (even used as a synonym). However, the idea of being “spiritual” is not equal amongst various faith paradigms, and the term can be particularly nuanced, and at times, in conflict with each other. For example, to an ancient Christian perspective, being spiritual (lower case “s”) means being in service to and communion with any spirit (e.g., unclean spirits, evil spirits, demonic spirits, deceitful spirits, spirits of the world), and does not necessitate a positive state, rather a sickness of the soul in need of healing—in contrast to being Spiritual (capital “S”; e.g., communion with the one, true God, “walking in the Spirit,” see Gal. 5:16-18; 1 Cor. 2:12, 4:14-22; 10:20; 1 Tim. 4:1; 1 John 4:1). 35 Also, there is a more recent phenomenon of a “secular spirituality,” which generally represents adherence to a spiritual philosophy without a religious framework (i.e., “spiritual, but not religious”), emphasizing personal development, subjective well-being, and search for personal meaning rather than participation in a religion and relationship with God, the divine, or transcendent.36,37 Spirituality has also been divided into sub-dimensions, such as a cognitive aspect (the search for meaning, purpose and truth, beliefs and values), an experiential aspect (feelings of hope, love, connection, inner peace, comfort, and support), and a behavioral aspect (the way a person externally manifests individual spiritual beliefs and inner spiritual state). 38
A complication, however, is that if spirituality is labeled in this way (secular or not), it can overlap with theories of mental health and well-being, positive psychology/character traits, and its outcomes (e.g., meaning or purpose in life, inner peace, hope, or harmony)—all of which are common in LM circles, and can be outcomes of R/S beliefs and praxis. Thus, for our purposes, we chose to define spirituality as a construct that holds it as distinguishable from its outcomes or consequences, and related to religion/religiosity, yet separate from those who are neither religious or spiritual (i.e., secular, humanistic; see Table 1).
In Theory
Theoretical explanations generally focus on the nuance of the individualized religious experience each patient or client will encounter, how much support (or not) they will receive from their religious community, and how integrated their religious values and beliefs are with health behavior.15,39 However, the understanding of how R/S affects patient-specific health behavior is less clear, and relatively nascent in understanding to inform LM practice. For example, relationships between R/S and chronic disease are often mixed, and unhealthy behaviors and disease risk/outcomes (highlighted by chronic disease) can be as prevalent with religious groups as with non-religious groups. Specifically, studies have revealed either a negative or lack of relationship between religiosity and heart disease, diabetes, high blood pressure, arthritis and asthma, and a positive or lack of relationship between religiosity and high body mass index (BMI) or obesity.40–51
As discussed by Faries and colleagues, 39 R/S might play a much smaller role in health lifestyle choices and behavior than presumed in contemporary American society—connected with certain health behaviors (e.g., excessive alcohol, tobacco smoking), but not others (e.g., unhealthy eating, physical inactivity). However, such connectedness or internalization can vary across faith traditions and individuals, which encourages individualized LM prescriptions and their modification, and support for a basic framework to engage R/S in practice.
In Practice
The following faith-practice framework is presented as a starting point to assist in overcoming concerns and challenges to incorporating R/S into LM practice, stimulate discussion and novel research questions, and foster insight into future opportunities for practice models. In community and public health, a dichotomous approach has been roughly outlined as faith-placed vs faith-based, and has been used here to keep coherency and coordination in language between community and clinic perspectives. As described below, we have broken faith-based into two sublevels of faith-recognized and faith-integrated, in order to create a more nuanced, spectrum-based approach from which practitioners can choose for patient-centered interactions.
Faith-Placed
Community
In community settings, faith-placed approaches represent those with no R/S components, often developed by health professionals outside of a faith community. So, while faith perspectives and practices are active within the faith community where the health program or initiative is placed, these perspectives and practices are not incorporated. Common examples include screening or immunization opportunities in a church parking lot, food pantries on the grounds, or health education programs utilizing an inside a room, kitchen, or activity space.
Clinic
In clinical or other one-on-one settings, we propose that faith-placed also represents a patient-practitioner interaction with no incorporation of R/S components, perspectives, or practices. While patients likely have their own faith-related perspectives and practices, they are not recognized or integrated into the diagnosis, discussion, or lifestyle prescription. Like community approaches, in certain cases, this lack of awareness or incorporation might not be a hindrance. For example, an examination of patients at a faith-based health center in South Africa generally reported they attended the clinic because of the quality of service (e.g., staff taking the time with, listening to, and respecting each patient) rather than the clinic’s religious practices—although, many of the factors related to quality of service were likely a result of the clinicians’ religious values. 52 On the other hand, if patients/clients are likely to filter, interpret, and/or apply a particular diagnosis and/or lifestyle prescription through the lens of their faith, then faith-placed interactions could be inadequate for successful behavior change and maintenance.
Faith-Recognized
Community
Within community settings, faith-based approaches generally represent a certain level of connection to one’s religious beliefs and praxis—although there can be great variation in the depth of the connection. On the shallow end of this continuum are faith-recognized approaches, which recognize and promote personal application of one’s R/S beliefs, behaviors, and/or culture into the healthy lifestyle programming. For example, a community-based healthy eating class might recognize the influence that R/S beliefs and the faith community culture can have on dietary choices, and encourage individuals to modify their food choices to align with those influences.
Clinic
Similarly, in clinical or other one-on-one settings, faith-recognized interactions involve the practitioner actively inquiring about and recognizing any personal R/S beliefs and behaviors that might influence the lifestyle diagnosis and prescription. There is recognition that certain lifestyle prescriptions, particularly the associated behaviors and/or medications, are going to be viewed through the lens of their R/S beliefs and practices. However, at this point, there is little to no further discussion of such influences and/or modifications. Rather, in faith-recognized approaches, the LM practitioner is simply encouraging patients or clients to consider their own personal R/S beliefs and behaviors, as they consider how to make necessary lifestyle changes.
It should be noted, while a majority of studies support patients’ desire for healthcare practitioners to recognize and consider their R/S beliefs and values in clinical care, a meaningful minority of patients do not want or object to their healthcare practitioners inquiring about R/S, especially in situations where the practitioner is of a different faith tradition, or R/S support is preferred outside of healthcare settings (e.g., family or clergy). 30
Thus, faith-recognized approaches might be most helpful in situations where the practitioner is unwilling or uncomfortable moving into a more in-depth discussion of personal R/S beliefs of the patients, but want to support personally relevant R/S beliefs in the clinical interaction. A simple recognition can further reveal the practitioner’s care, acceptance, and positive concern for such valued beliefs, and in turn, support personal autonomy—a prominent determinant of possible health behavior change. For example, consider the following items from the Healthcare Climate Questionnaire, a measure of autonomy support.
53
I feel that my physician accepts me.
My physician listens to how I would like to do things.
I feel that my physician cares about me as a person.
My physician tries to understand how I see things before suggesting a new way to do things.
Similarly, within the VA’s Whole Health approach, a patient completes a Personal Health Inventory by assigning numerical values (1 = being miserable to 5 = being great) for where they are in regard to various health behaviors and life factors, including R/S, and where they would like to be (same 1-5 scale). If there is a gap, the clinician can then recommend resources to close the gap. In turn, faith-recognized interactions open the opportunity for patients/clients to find appropriate support and internalize healthy behaviors into their R/S beliefs—thus increasing the theorized probability of behavior adoption, as well as an opportunity for deepening a discussion within the faith-practice continuum.
Faith-Integrated
Community
On the deepest end of the faith-based continuum, faith-integrated allows for the greatest level of connection of one’s faith beliefs and behaviors within a healthy lifestyle approach. There is an understanding that lifestyle decisions, particularly around one’s health and related behavior, are inseparable from their R/S values, beliefs, and culture. In community health programs, for example, personal R/S beliefs, values, and cultures not only inform development, but are included as an integral part of the education—often pairing theory-based concepts with religious study about health, prayer, and other R/S praxis.54–56 Public health initiatives can also adapt education to help guide autonomous decision making around one’s health, such as providing information about vaccines that might conflict with R/S values and practice—which vaccines contain animal products (e.g., gelatin, fetal bovine serum, eggs), which are derived from aborted fetal cell lines, or accommodating concerns of vaccination during fasting periods.
Clinic
In clinical or other one-on-one settings, faith-integrated interactions include inquiring about a patient’s or client’s R/S values and practices, but then actively engaging and cooperating their values and practices into the lifestyle prescription. The goal of such interactions is to increase the probability that the patient/client will internalize and be motivated to follow through with the prescription through enhanced behavior change, since the prescribed behaviors are aligned with perhaps one of the most valuable aspects of their lifestyle decision making. While a deeper understanding of a particular faith tradition can be helpful with diagnoses, care options, and lifestyle prescriptions, the practitioner need not have personal knowledge of the R/S particulars of each patient—rather, employ use of various assessments, histories, discussions, and strategies to deepen an understanding to the purposes of benefiting a patient-centered approach. For example, the practitioner might modify prescriptions based on avoidance of animal products (e.g., other options for dietary changes or medicines with gelatin capsules) fasting schedules (e.g., weekly and feast-related fasting with Orthodox Christians, or Ramadan in Islam), or connect the prescription to a meaningful belief (e.g., Christian belief that the body is God’s temple, 57 or within Buddhism’s noble eightfold path). 8
Assessment
In concert with the proposed faith-practice framework, various R/S assessments can be implemented. Religious or spiritual assessments, often referred to in clinical settings as taking a “religious or spiritual history,” invite patients to share their R/S beliefs and values with the practitioner, while also identifying the commitments, influences, and concerns within R/S wellness. The end goal is to acknowledge the role of R/S beliefs and values of the patient/client, and to maintain whole, patient-centered care. In LM practice, as detailed in the following sections, such an evaluation opens the opportunity for fruitful discussion into how lifestyle prescriptions might be modified and implemented to accommodate R/S values, beliefs, and behaviors.
As a starting point, a basic decision tree for patient-centered LM practice can be utilized based on a simple set of two questions working from the aforementioned definitions of a patient or client being religious or spiritual (Figure 2). General, neutral questions might also be asked to open conversation around one’s R/S values and beliefs related to their health, which the patient/client might already be considering themselves, such as:15,58,59 “What are your concerns?” “What’s important to you?” “What gives your life meaning?” “Are religion or spirituality important to you in thinking about health and illness or at other times?” “Do you have, or would you like to have, someone to talk to about religious or spiritual matters?” Decision tree for clinical purposesa.

From here, various R/S assessments spanning various dimensions of R/S are available to clinical practice, education, and research. As a starting point, the following sections provide a general overview of common, relevant assessments. For more detailed analysis of R/S measurement, please see the following citations.3,12,13,33
Common Assessments
One of the most common and widely utilized measures of religiosity is the brief, five-item Duke University Religion Index (DUREL), captures these organizational and non-organizational dimensions, as well as an intrinsic religiosity (i.e., religious belief, experience) dimension. 60 The DUREL is advantageous due to its brevity, and coverage of key dimensions of religiosity. If there is deeper interest in and methodological sensitivity to religious commitment, the Belief into Actions Scale (BIAC), 61 Hoge Intrinsic Religiosity Scale, 62 and Religious Commitment Inventory 63 might be considered (all are 10-items). In addition, there are religion-specific scales, and although most scales have been developed in Protestant and Catholic Christians, there are a growing number of assessments across other faith traditions—such as Judaism, Hinduism, Buddhism, and Islam.
Coping Assessments
Another key aspect of LM clinical practice builds upon external and internal support one finds within R/S (i.e., coping), and or the negative effects of religion. As a starting point, the Brief Multidimensional Measure of Religiousness/Spirituality (BMMRS) scale has both a Religious Support (8 items) and R/S Coping sub-scales (8 items) (see Fetzer.org). The Brief RCOPE 64 is widely utilized, with 14-items that assess two sub-scales: Positive Religious Coping (e.g., looked for stronger connection with God, sought God’s love and care, tried to put my plans into action together with God) and Negative Religious Coping (e.g., wondered whether God had abandoned me, questions God’s love for me). In addition, the 3-item Religious Coping Index 65 can be used as a more in-depth discussion of patient-specific use of religion to cope with illness-related stress. Religious coping assessments are also coming more accessible across other faith traditions—such as, Judaism (16-item JCOPE), 66 Hinduism (15-item Hindu RCOPE), 67 and Buddhism (44-item BCOPE). 68
Clinical Assessments
The above assessments have been mostly utilized in research contexts, with promotion of providing possible benefit as clinical settings. However, specific instruments to take R/S history in clinical practice have been identified, varying from 2 to 30 minutes. 69 For example, two clinically relevant scales promoted are the validated Faith, Importance and Influence, Community and Address (FICA)59,70 and the HOPE spiritual assessment tools. 71
The FICA guides the patient-provider interaction with simple questions, such as importance of R/S beliefs, practices, and values of meaning in one’s life, how such beliefs might affect healthcare decision, R/S community support, and autonomy support by the practitioner—taken as a part of regular medical histories or exams. The HOPE questionnaire allows for discussion into R/S beliefs as a source of
Conclusion
Lifestyle medicine practitioners are interested in incorporating R/S into LM perspective and practice—stemming from the growing evidence supporting the prominent role of R/S in physical and mental health, its importance to patients’ lives and healthcare decisions, as well as their own personal R/S influences and experiences. The faith-practice framework presented here provides a starting point for considering incorporating R/S into LM practice in light of common concerns and challenges, and serving as a guide for patient-centered care through adjusting lifestyle prescriptions to accommodate individualized R/S beliefs and practices for improved health behavior and outcomes. Yet, there remains ample opportunity for innovative practice models and novel research questions, such as a deeper dive into the connection of current research with LM Pillars, and further examination of the bi-directional predictive and/or moderating role of R/S on lifestyle behaviors prominent in LM prescriptions across various populations (e.g., religions, denominations, ethnicities, and so on). We are hopeful that this brief review will encourage a prominent consideration of R/S in LM practice and research, support those already practicing in this way, and stimulate openness for positive, thoughtful discussion into the future.
CME/CE Article Quiz
American College of Lifestyle Medicine (ACLM) members can earn FREE CME/CE credit by reading this approved CME/CE article and successfully completing the online CME/CE activity. Non-members can earn CME/CE for $40 per article. Visit lifestylemedicine.org to join the ACLM.
AJLM CME/CE Articles and Quizzes are offered online only through the American College of Lifestyle Medicine and are accessible at lifestylemedicine.org/store. ACLM Members can enroll in the activity, complete the quiz, and earn this CME/CE for free. Non-members will be charged $40 per article.
A Passing score of 80% or higher is required in order to be awarded the CME/CE credit.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.