
Abstract
This article reviews both traditional and emerging aspects of pain medicine within the context of a “whole-person,” lifestyle-based approach. This is consistent with contemporary systems theory formulations of chronic disease in general. A traditional approach sees ongoing pain as a fixed biological disorder and much of its management as the task of medically palliating or learning to cope. Within this framework, chronic pain has been conceptualized by some authors as a disease in its own right based on underlying alterations in nervous system processing. This explains the stronger correlation of chronic pain with neural sensitization than with structural change in bodily tissues. However, recent research findings are expanding current views of causation and management, and there is now a growing recognition that pain-related nervous system changes are potentially reversible. The so-called paradox of plasticity proposes that the same property of changeability in the nervous system that allows chronic pain to develop can also lead to its resolution. Nutrition and personal story are key aspects of an emerging whole-person approach and can be combined with traditional biomedical and cognitive behavioral interventions to enhance therapeutic gains. An interesting hypothesis deriving from recent research is that multiple unhelpful aspects of lifestyle contribute to systemic metaflammation, which in turn spills over to sensitize the nervous system and facilitate pain-related transmission. Therefore, addressing lifestyle factors therapeutically has the potential to desensitize the nervous system and reduce pain.
The question of why pain exists has fascinated philosophers, theologians, and scientists alike over the centuries, and this search for meaning continues to the present day.
Pain is a universal human experience. For the majority, experiences of pain last for relatively short periods. Such “acute” pain is generally linked to injury to bodily tissues and resolves as those tissues heal. However, in some situations the pain does not resolve and continues beyond the expected time for tissue healing. When pain lasts longer than 3 months, it is defined as “chronic” or “persistent.” 1
The question of why pain exists has fascinated philosophers, theologians, and scientists alike over the centuries, and this search for meaning continues to the present day. In considering the meaning of pain, it is necessary to differentiate acute and chronic forms. At one level, the meaning of acute pain is straightforward, pointing to actual or threatened tissue injury, a reality sign to an individual organism in an often adversarial environment. However, the meaning of chronic pain is more elusive. Certainly at times there remains a link between chronic pain and obvious tissue damage. For example, advanced osteoarthritis of the hip may cause persistent pain that resolves with joint replacement surgery. However, it is more often the case that the link between pain and obvious tissue damage is lost. Hence, it is possible to have severe osteoarthritis in a hip joint with reduced range of movement but minimal or no pain. In fact, the majority of chronic pain conditions demonstrate this lack of concordance between pain and structural change in bodily tissues, as consistently demonstrated in multiple studies.2-6 Back pain provides a typical illustration of this conundrum. Some people have severe back pain with normal spinal imaging (eg, magnetic resonance imaging), whereas others have marked structural changes but no pain.
This review focuses on chronic pain and considers both traditional and emerging aspects of management within the context of a “whole-person,” lifestyle-based approach. This is consistent with contemporary systems theory formulations of chronic disease in general. A traditional view sees chronic pain as a fixed biological disorder and much of its management as the task of medical palliation or learning to cope. Within this framework, chronic pain has been conceptualized by some authors as a disease in its own right based on underlying alterations in nervous system processing. 7 This explains the stronger correlation of chronic pain with neural sensitization than with structural change in bodily tissues. However, recent research findings are expanding current views of causation and management, and there is now a growing recognition that pain-related nervous system changes are potentially reversible in both acute and chronic settings.
Early research into the role of the nervous system in pain focused on sensitization of peripheral nerves and the spinal cord.8,9 In more recent times, and particularly with the advent of techniques to study brain function (eg, functional magnetic resonance imaging), it has been noted that changes in sensory and affective regions of the brain are fundamental to the experience of chronic pain.10-13 Hence, it is now recognized that a variety of bodily injuries or disease processes can trigger sensitization in the nervous system. Sensitization can also occur in response to psychosocial stressors via the mind–body connection.14-16 Over time, if the neural sensitization resolves, so too does the pain. On the other hand, if the sensitization persists, chronic pain is the outcome.
Many factors, including those associated with lifestyle and physical and psychological trauma, contribute to the process of neural sensitization. This understanding brings with it a greater sense of therapeutic optimism as there are consequently multiple potential management strategies that may be used to retrain or desensitize the nervous system. Therefore, the concept of pain as a reality sign is still meaningful in the chronic setting. However, its meaning needs to be interpreted more broadly than in the familiar tissue injury context of acute pain; this includes consideration of lifestyle.
Historical Perspectives
The prevailing Western medical view of pain has been strongly influenced by Descartes in the 17th century. His reductionist view promoted linear cause and effect and saw pain as a fixed response to tissue injury. The limitations of this “Cartesian” approach were challenged by Melzack and Wall in their famous gate control theory of pain,17,18 which acknowledged neural modulation and fitted well with the biopsychosocial model subsequently published by Engel. 19 In contemporary pain medicine practice, however, the biopsychosocial model is often still interpreted in a dualistic way, with the focus on biomedical interventions aimed at pain reduction on one hand or simple acceptance and learning to manage on the other. Such dualism does not recognize the potential for active self-management to retrain the nervous system and hence reduce or resolve pain. In recent times, the concept of person-centered care20,21 has brought a greater focus on the individual and his or her unique story. This has resulted in a shift away from any simplistic, recipe-book notion of pain management strategies that the person in pain is expected to apply.
Epidemiological Perspectives
Expert opinion favors the view that prevalence of chronic pain has increased with the development of Westernized lifestyles, 22 but this is difficult to verify because of lack of preindustrialization data. Nevertheless, epidemiological studies comparing prevalence across diverse race, ethnicity, and cultural settings can provide useful clues to the potential for lifestyle factors to influence chronic pain.
Considerable variation in prevalence of chronic pain in the community has been reported. Studies in Canada, 23 Australia, 24 and across Europe 25 have reported prevalence rates of less than 20%. Higher prevalence has been reported in Denmark (20.2%), 26 Norway (24.4%), 27 Kansas (United States; 26%), 28 Sweden (35.3%), 29 Ireland (35.5%), 30 and Hong Kong (45.9%). 31 The highest community prevalence reported has been 64.4% in Olmsted County (United States). 32 Relatively low prevalence has been reported among Chinese men living in Malaysia (9.9%) 33 and rural, as opposed to urban, Mexicans. 34 Such variation can be explained in part by differences in study methodology, genetics, and cultural influences on reporting. However, it is likely that lifestyle factors also contribute.
Although genetic factors may contribute to variation in prevalence of chronic pain, many of the above studies highlight the association between pain, psychological factors, and low socioeconomic status. In a further exploration of the relative roles of genetic determinants and socioeconomic factors, Stanaway et al compared Italian-born immigrants with Australian-born men aged 70 years or more in an Australian urban setting. 35 They reported that differences in pain were strongly explained by socioeconomic rather than racial factors. Other authors have similarly emphasized the importance of socioeconomic status in chronic pain.36-38 This association between low socioeconomic status and chronic pain is yet to be fully analyzed; however, it is possible that lifestyle factors and psychological health play mediating roles.
Of additional interest from an epidemiological perspective is the association of chronic pain and other medical comorbidities with established lifestyle contributors.39,40 Furthermore, increased mortality has been documented in chronic widespread pain and attributed to lifestyle factors and cardiovascular disease. 41
Stress has been linked epidemiologically to chronic pain. Prevalence of chronic pain was found to be higher in an Israeli town frequently subjected to missile attacks as compared with another town of similar sociodemographic character but without the imminent threat of attack. 42
Thus, it is likely that multiple factors including ethnicity, culture, genetics, socioeconomic status, stress, psychological health, and nutrition all contribute to the community prevalence of pain. Further epidemiological research is needed to explore more fully potential links between these factors and the genesis and management of chronic pain.
Emerging Lifestyle Perspectives
The field of psychoneuro- immunology has for several decades witnessed research on the relationships between psychological stress and the nervous, immune, and endocrine systems.14-16 There has been recognition that stress is linked to pro-inflammatory cytokines, inflammation, and, in turn, the risk of chronic disease.
In recent years, the term metaflammation has been coined to differentiate low-grade chronic, systemic inflammation, with its associated metabolic impact, from classical acute inflammation. 43 Metaflammation typically produces only a modest increase in inflammatory mediators such as TNF-α, IL-6, CRP, and some transcription factors. 44 From a lifestyle perspective, metaflammation can be seen to be induced by aspects of the modern industrialized world to which humans are yet to adapt.45,46 Metaflammation is known to affect the vascular endothelium, in part mediated by activated macrophages. Insulin resistance is proposed as the link with metabolic disease. It is via these mechanisms that metaflammation is thought to play an underpinning role in the genesis of many modern chronic diseases. 47
Recent research has recognized that the process of metaflammation is not confined to the vascular endothelium and that it can extend to affect the nervous system. This has led to the concept that the vascular and nervous systems function together as a “neurovascular unit” (Figure 1). 48 Metaflammation can spread across the vascular wall to activate adjacent glial cells. The activated glial cells then release pro-inflammatory cytokines that can sensitize the nervous system and contribute to chronic pain.49,50 Two types of glial cells have a potential role, microglia and astrocytes. Microglia are known to be activated by signals from damaged brain tissue, infection, and, interestingly, opioid therapy (possibly contributing to tolerance and opioid-induced hyperalgesia). 51 Once activated, microglia release inflammatory cytokines in the brain and spinal cord.52,53 Astrocytes provide the structural support matrix for the central nervous system, are constituents of the blood–brain barrier, and, when activated, may also facilitate pain pathways. 51 See Box 1.
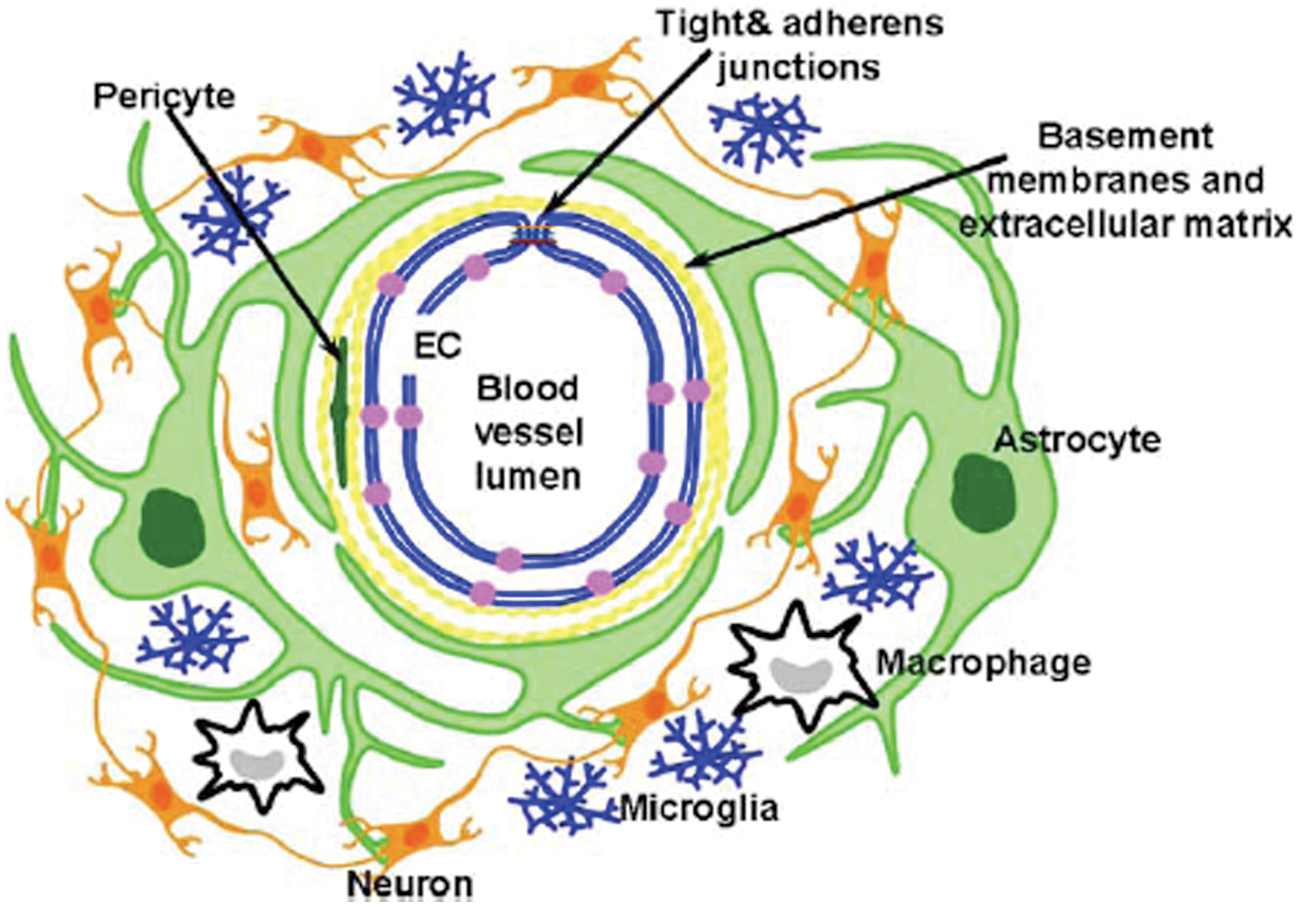
The Neurovascular Unit.
An Analogy to Assist Patient Understanding of Chronic Pain Using Recent Glial Cell Theory
Indigenous societies such as Australian Aborigines have complex but efficient communications (“song-lines”) between groups, through which tribe-to-tribe diffusion of information can occur. The message might be slower than through the transmission of a modern telephone line but is more widespread and likely to be more deeply “locked in.” This is similar to glial transmission in the brain. The message is slower, more diffuse, and hence relatively “locked in” and hard to change. Neural transmission is like the telephone system, through which rapid one-to-one communication can occur but which is easily disrupted by cutting the phone line.
Glial activation in the brain means that pain-related messages can be locked in after the original stimulus has healed. Fortunately, new findings on brain plasticity show that this can be reversed, although it is not a simple willful process, just as the changing of an accepted tribal communication.
This simple metaphor can be extended to incorporate the main glial cell types: Astrocytes are represented by a tribal community milling around the village phone box and passing messages from those travelling by road or river (the bloodstream), among themselves and to an individual in the phone box (neural system). Microglia are represented by the travelling maintenance workers who search for and repair any breaks in the phone line.
The question yet to be fully elaborated is whether or not lifestyle inducers of metaflammation in the vascular endothelium can cause neural sensitization via glial activation and facilitate pain processing. Certainly, this is a potential mechanism whereby diverse factors such as stress, nutrition, activity, and sleep could contribute to chronic pain.
Pro-inflammatory nutritional factors have been reviewed by Seaman 54 and Esposito and Giugliano. 55 A diet that is low in fruit and vegetables and has excessive refined carbohydrates adds to inflammation. Key elements of such a diet are deficiencies of antioxidants and phytochemicals and an imbalance in the ratio of omega 3 to omega 6 essential fatty acids. Egger and Dixon 46 have reviewed nutritional triggers of metaflammation in relation to the environment, economics, and policy imperatives. Further research is required to assess more fully the impact of nutritional therapy on metaflammation, neural sensitization, and pain.
Physical activity programs have been noted to reduce metaflammation in the context of obesity management and weight loss. 56 Sleep impairment has been associated with cytokine changes in the brain 57 and elevations in adipokines related to inflammation and insulin resistance. 58 Two recent studies concluded that sleep disturbance or restriction was associated with higher levels of IL-6, which were in turn associated with higher levels of perceived pain.59,60 Thus, these factors can be targeted as part of a lifestyle approach to chronic pain.
It is a fascinating hypothesis that lifestyle factors may contribute to the processing and perception of chronic pain by facilitating metaflammation that extends beyond the vascular endothelium and across the neurovascular unit to sensitize the central nervous system.48-50
Brain Plasticity
Nervous system changes, in the physical sense, provide a common pathway for the development of chronic pain. Multiple influences including biological, environmental, lifestyle, and psychosocial factors directly affect the nervous system and can, therefore, be seen to play a role not only in causation but also in the treatment of chronic pain. The therapeutic application of strategies targeting neuroplasticity, particularly at the level of the brain, is a very significant recent advance.
It was the development of techniques such as functional magnetic resonance imaging that first opened the way to an appreciation of the association between chronic pain and brain reorganization at cortical and deeper levels. 10 Subsequently, Ramachandran and others have begun to explore innovative treatments, including mirror imagery, that aim to retrain these disordered brain pathways with a view to pain reduction. 61 Doidge has discussed the “paradox of plasticity,” 62 which recognizes that the same property of neural changeability that contributes to the causation of chronic pain may be used therapeutically to bring resolution.
Therefore, treatment strategies addressing diverse aspects such as lifestyle, nutrition, psychotherapy, and movement can all be seen as potential neuroplasticity tools. Various physical therapy approaches have been adapted using a neuroplasticity framework. The aim is retraining of brain pathways through awareness of movement and addressing the quality and meaning of movement.63-65 Physical approaches are also being used as an adjunct to psychotherapy, again with a view to brain retraining.66-69 From a lifestyle perspective, there is a need for further research, as discussed previously, to investigate which aspects can be used most effectively to retrain a sensitized nervous system and restore normal brain processing.
Mind–Body Approaches
The concept that psychological stress can profoundly influence physical state has been pioneered in the field of psychoneuroimmunology, as previously discussed. In regard to chronic pain, it is well recognized that traumatic life events can play either a predisposing or a precipitating role in terms of the onset of pain. Background sexual abuse has been linked to chronic pain.70,71 Other predisposing traumas of relevance are childhood illnesses and painful events 72 including neonatal intensive care unit admission 73 and male infant circumcision. 74 These traumas are seen as priming the nervous system and hence increasing the likelihood of chronic pain.
Psychotherapeutic approaches have often been used in a dualistic sense. The first use is simply to address mental health issues. However, from a mind–body perspective it becomes conceivable to use psychotherapy to treat “physical” problems. Thus, gaining an awareness of suppressed emotions related to earlier life trauma and releasing of those emotions can at times bring resolution of chronic pain and other complex health problems. In effect, this means using “personal story” and psychotherapy 75 as brain plasticity tools. Such mind–body approaches have resulted in large case series reporting abolition of chronic pain.75,76 Such approaches have not been in the mainstream of pain management, perhaps because they have not been recognized by the dominant cognitive behavioral paradigm. Nevertheless, reports are beginning to enter the contemporary pain literature. 77
Limitations of Traditional Treatment Approaches
In part, it has been the limited benefit from traditional pain management approaches that has driven the exploration of a new generation of treatments incorporating lifestyle, brain plasticity, and mind–body strategies. Pain management in past decades has often, as mentioned, involved a dualistic split between biomedicine on one hand and cognitive behavioral therapy on the other. This has led to only modest treatment gains.
Biomedical approaches to chronic pain include medication use and procedures such as nerve blocks and surgery. Over time, it has become apparent that unimodal biomedical approaches typically produce only limited benefit for a limited duration. Problems of tolerance and opioid-induced hyperalgesia52,78,79 have major implications for pharmacotherapy. The current generation of implanted devices such as intrathecal pumps and spinal cord stimulators have limited efficacy and high complication rates.80-82 Other procedural interventions are also limited in degree and duration of benefit.83,84 Furthermore, any unimodal use of biomedical strategies runs the risk of drawing the recipient away from active management, for which the evidence base is higher. A key therapeutic challenge, therefore, lies in seeking the optimum balance between biomedical treatment (which may yet improve with future research) and more active management, including lifestyle approaches.
A cognitive behavioral approach to pain considers patterns of thinking, emotion, and belief alongside behaviors and external reinforcers. Catastrophizing, fear avoidance, low mood, and either over- or underactivity are key aspects. Often, cognitive behavioral principles are applied in group pain management programs that help provide education, develop problem-solving and communication skills, and teach relaxation, pacing of activity, and gradual medication reduction. 85 The benefits of such programs have been consistently reported.86-88 Demonstrated outcomes included lowered levels of disability, less health care utilization, and improved emotional functioning. However, more recent reports have been less encouraging. In 2009, a systematic review of both cognitive behavioral therapy and behavioral therapy for persistent pain in adults reported only a weak effect on pain intensity, minimal effect on disability, and modest improvement in mood. 89 The authors noted that although the quality of trial design has improved over the years, clinical outcomes have not. In 2010, similarly modest results were reported for behavioral therapies in chronic low back pain. 90
A cornerstone of the traditional cognitive behavioral approach to chronic pain has been the belief that pain should be accepted and managed with the underlying assumption that it will persist for life. Although one recognizes that it is better to learn to manage pain, rather than not, this belief can be seen as unduly pessimistic in light of recent neuroplasticity research. As a core belief, it has the potential to become negatively prophetic over a person’s life, effectively an overdose of acceptance at the expense of hope. A more paradoxical frame acknowledges the need to maintain tension between the polarities of acceptance and hope. 91 This greater sense of optimism is consistent with a lifestyle approach to the management of other chronic conditions, which acknowledges the potential for significant improvement in the underlying disease process and the possibility of complete reversal at the best end of the therapeutic spectrum. 92 The challenge in regard to cognitive behavioral approaches lies in taking the helpful aspects and incorporating them into a broader model.
A Whole-Person Approach
The emerging paradigm in chronic pain management draws together aspects of all the treatments discussed above and has been described as a “whole-person” approach.22,93 Biomedical interventions are still applicable; however, given current evidence, the emphasis is on time-limited use. Thus, biomedical treatment can be used to provide a window of opportunity to develop active strategies for which the evidence base is higher. Once active approaches are incorporated, biomedical treatment can be ceased. Clearly, there is scope to incorporate any new pharmaceutical breakthroughs, particularly those that might target the process of nervous system sensitization. There is also scope to incorporate any meaningful improvements from surgical and other procedural interventions.
In addition, there are very positive aspects of cognitive behavioral therapy that address inaccurate cognitions, avoidance of activity, and deficiencies in problem solving. These can be applied to advantage in a broader context. However, the foundational belief of cognitive behavioral therapy that chronic pain will never change or resolve needs to be discarded.
These changes in approach to pain have occurred within a broader chronic disease context. There is now recognition that a “linear” approach, suggesting that “problem = extraneous treatment = cure,” brings only limited benefit in any long-term health problem. Such traditional thinking is now giving way to a more complex systems theory or whole-person approach that takes account of the iterative processes of feedback in disease causation and the need to recognize multiple pathways in prevention and management. 94
A diagrammatic representation of whole-person chronic pain management is shown in Figure 2. The traditional elements of biological characteristics (biomedicine), and thoughts and actions (cognitive behavioral aspects) are included. However, these are extended to include nutritional and personal story elements. This effectively harnesses the therapeutic optimism inherent in the concept of brain plasticity and incorporates a focus on lifestyle with a view to reducing metaflammation and, by extension, neurovascular inflammation. There is an emphasis on allowing the person in pain to choose the aspects of active management that he or she would like to address. This motivational approach aims to facilitate engagement with the overall management plan. 95 In certain situations, such a person-centered approach allows a vulnerable patient to work with less threatening aspects of management initially until sufficient trust has been developed to allow exploration of deeper emotional issues.
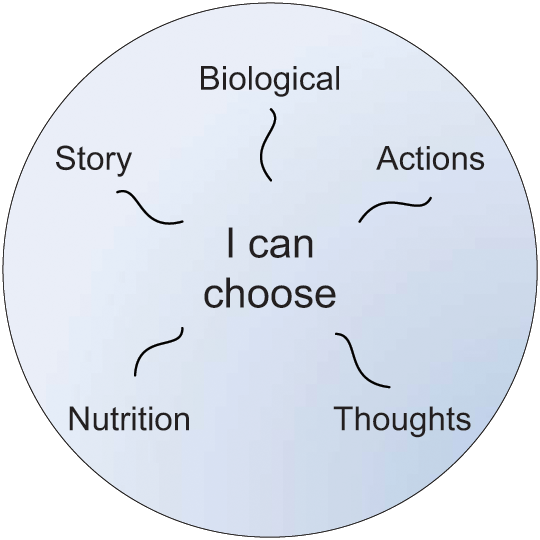
A Whole-Person Approach.
Time and ongoing research will clarify whether the sense of therapeutic optimism that surrounds the emerging whole-person approach is justified.