
Abstract
The completion of primary treatment for breast cancer has been referred to as a “teachable moment” for health behavior change, suggesting that women are receptive to receiving physical activity counseling. However, the majority of breast cancer survivors are not sufficiently active. Health care providers may play a pivotal role in increasing patients’ physical activity behavior, yet physician counseling for physical activity is not done regularly. One reason for this failure may relate to the limited guidelines put forward to assist health care providers in how best to optimize the benefits of physical activity among breast cancer survivors. To help provide guidelines for physical activity counseling with breast cancer survivors, the authors synthesized evidence-based recommendations based on a review of 30 intervention studies. The evidence on (1) type, (2) intensity, and (3) frequency and duration of physical activity for this population was examined. On the basis of the reviewed studies, the authors find that physical activity programs for breast cancer survivors should include aerobic training at least 3 times/wk for 30 minutes, resistance training 2 to 3 times/wk (6-12 exercises), and flexibility training 3 times/wk for 50 to 60 minutes to obtain health benefits. The provision of these recommendations may facilitate effective and consistent delivery of physical activity counseling to breast cancer survivors.
Introduction
The number of women diagnosed with breast cancer each year is increasing, with more than 125 000 new diagnoses per year in North America. However, early detection and improved treatments have led to an increase in survival rates. 1 As a result, there is a growing population of breast cancer survivors (ie, women who have completed active medical treatment) 2 who are at increased risk for recurrence, secondary cancers, and both mental and physical health comorbidities.3,4 In addition, many breast cancer survivors experience a number of short- and long-term physical and mental side effects because of the treatments endured (eg, pain, lymphedema, nausea, fatigue, lung fibrosis, cardiomyopathy, cardiotoxicity, weight gain, muscle loss/weakness, osteoporosis, and decreased well-being).5-9 Studies have shown that physical activity may help prevent or minimize some of these health risks and side effects. 10 Based on recent meta-analyses and systematic reviews, the most common benefits include improved physical fitness, overall functioning, quality of life, and reduced fatigue in breast cancer survivors.2,11-17 Furthermore, physical activity has been linked to decreased depression and anxiety; improved social and emotional well-being, body self-esteem, body image, body composition, and survival rates; and reduced risk of breast cancer recurrence and death.10,12,14,18-29 Considering this evidence, the American College of Sports Medicine (ACSM) convened an expert committee consisting of clinical and research experts in the field to review existing evidence on the safety and efficacy of physical activity during and after adjuvant cancer therapy. 30 The consensus was that physical activity is safe during and after cancer treatment and leads to better quality of life.
‘Combining the evidence across studies, which consistently demonstrate that moderate-intensity activities lead to improvements in physical and psychological health, physicians should focus on promoting moderate-intensity activity among patients.’
The completion of primary treatment for breast cancer (ie, surgery, radiation, and/or chemotherapy) has been referred to as a “teachable moment” for health behavior change,31,32 suggesting that women may be receptive and responsive to receiving physical activity recommendations. However, the majority of breast cancer survivors (>58%) are not sufficiently active.18,28,33-38 Targeted efforts are required to address the state of physical inactivity in this population.
Physician counseling on physical activity in the primary care setting may be an effective targeted strategy to increase physical activity.39-41 In fact, several reviews examining the impact of physical activity interventions in primary care settings have supported the effectiveness of counseling to increase physical activity.42-44 Unfortunately, physician counseling on physical activity is not done on a regular basis. 45 This may partly be a result of the limited guidelines put forward to assist physicians in providing physical activity recommendations to patients who have completed primary treatment for breast cancer. It is important to synthesize and disseminate evidence to physicians to help the implementation of physical activity counseling. Advances have been made in this respect, such as the recommendations that cancer survivors follow the Physical Activity Guidelines for Americans with adaptations. 30 However, explanations of the components included in the guidelines and specific guidelines for breast cancer survivors are still needed. Providing physicians with specific recommendations for breast cancer survivors, along with a concise description of the recommendations, may facilitate individual physical activity counseling to patients.
To facilitate more effective, efficient, and consistent delivery of physical activity counseling, this report introduces and explains evidence-based recommendations derived from the evidence available for physical activity for breast cancer survivors. Specifically, it provides an overview of the physical activity parameters related to (1) type, (2) intensity, and (3) frequency and duration for breast cancer survivors that have been shown to yield health benefits. This goal is different from the consensus statement published by the ACSM. 30 It is intended to offer physicians practical recommendations to help them counsel breast cancer patients who have completed active treatment.
Materials and Methods
Literature searches were performed using Medline, Cumulative Index for Nursing and Allied Health Literature (CINAHL), PubMed, PsycINFO, and SPORTdiscus electronic databases for studies. The following headings and keywords were used as search terms: “breast cancer” or “neoplasm” in combination with “exercise” or “physical activity.” Searches were limited to articles in English. Reference lists of included articles were scanned for additional relevant studies, as well as reference lists from meta-analyses and systematic reviews on this topic.
The first author conducted the initial screening of retrieved articles by examining the titles and abstracts to determine the relevance. Selected articles were fully reviewed. Inclusion criteria were as follows: (1) women who had completed primary treatment for breast cancer (ie, surgery, chemotherapy, and radiation), (2) physical activity or exercise intervention studies only (because the effect of the physical activity intervention could not be separated from the effect of a multiple intervention program), (3) studies with data on change in one or more health outcomes, and (4) studies published in a peer-reviewed journal. Exclusion criteria were the following: (1) review, descriptive, correlational, observational, or survey studies (other than for initial identification of articles); (2) multicomponent interventions; (3) studies including survivors of multiple cancer types; (4) unpublished dissertations; and (5) abstracts only. A total of 30 published studies based on 22 interventions met the study inclusion criteria.21,24,28,29,46-71 The mean age across studies varied between 48 and 65 years, and the majority of women were diagnosed with stage I to stage III breast cancer.
Data regarding the interventions and health outcomes were collected and summarized by the authors in Tables 1 to 4. Then, the physical activity recommendations were developed based on the evidence regarding what type(s), intensities, frequency, and duration of physical activity effectively improved health outcomes.
Summary of Aerobic Training Studies With Breast Cancer Survivors
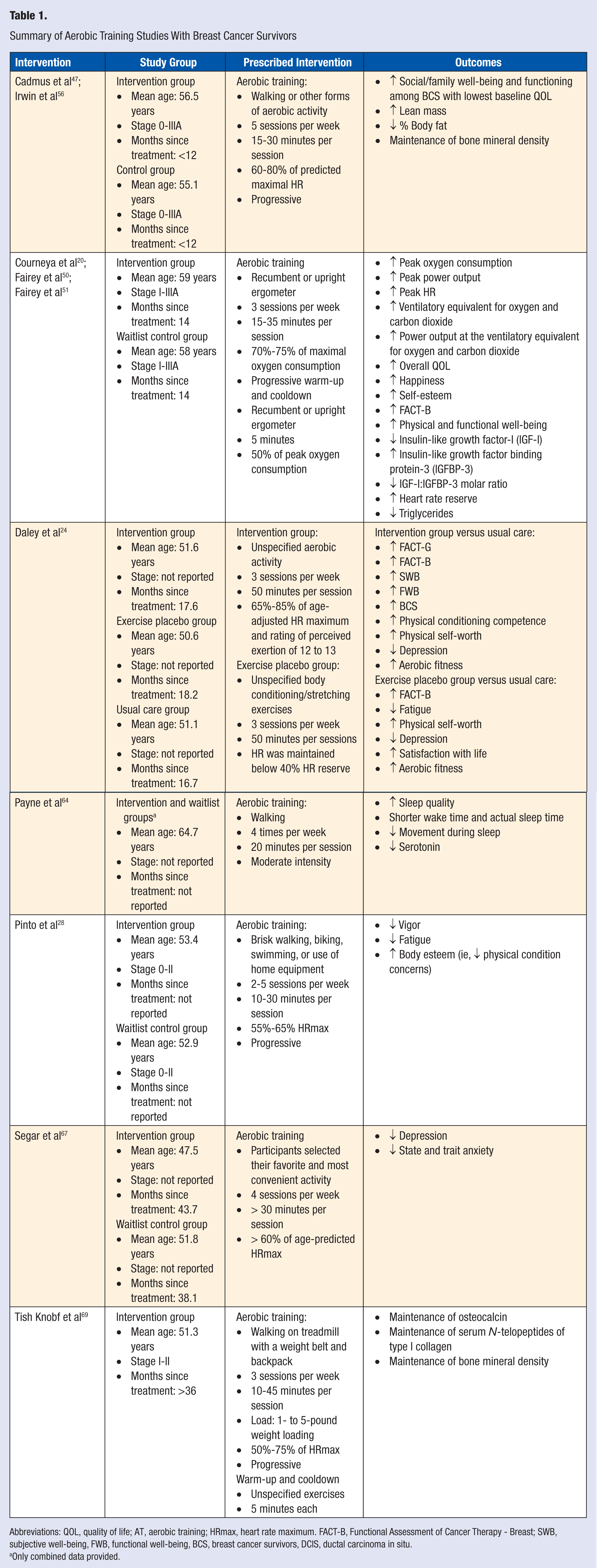
Abbreviations: QOL, quality of life; AT, aerobic training; HRmax, heart rate maximum. FACT-B, Functional Assessment of Cancer Therapy - Breast; SWB, subjective well-being, FWB, functional well-being, BCS, breast cancer survivors, DCIS, ductal carcinoma in situ.
Only combined data provided.
Summary of Resistance Training Studies With Breast Cancer Survivors
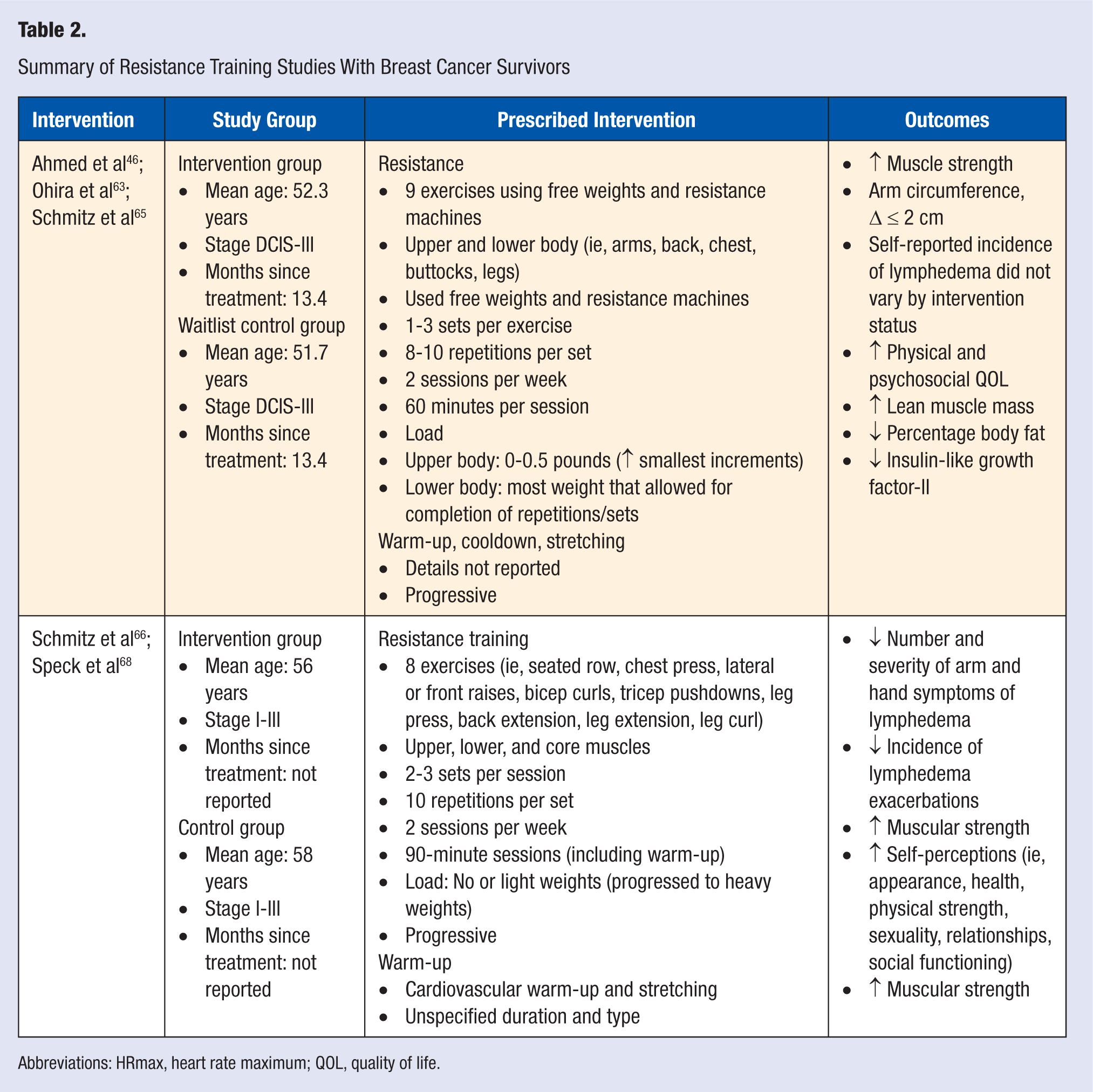
Abbreviations: HRmax, heart rate maximum; QOL, quality of life.
Summary of Mixed Aerobic and Resistance Training Studies With Breast Cancer Survivors

Abbreviations: HRmax, heart rate maximum; QOL, quality of life.
Only combined data provided.
Summary of Flexibility Training Studies With Breast Cancer Survivors a
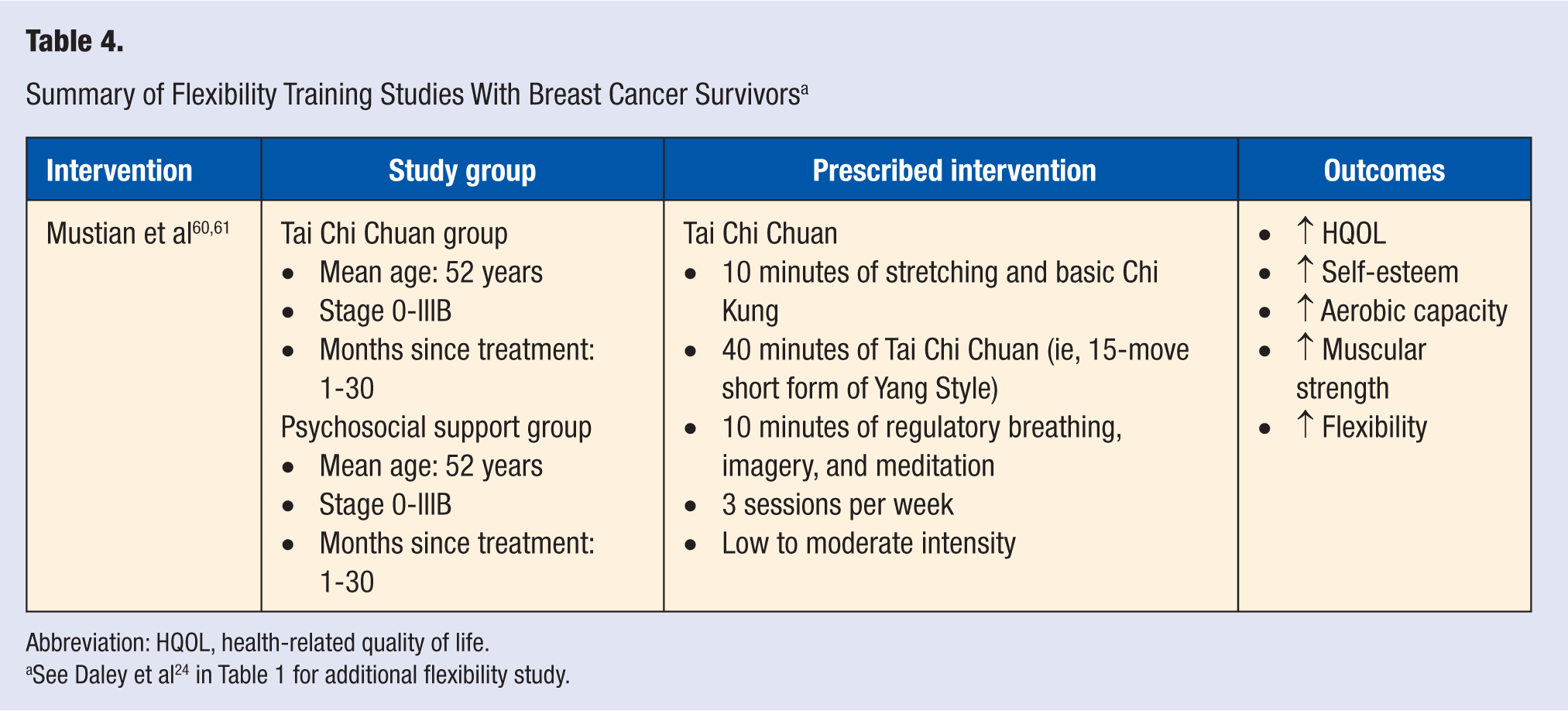
Abbreviation: HQOL, health-related quality of life.
See Daley et al 24 in Table 1 for additional flexibility study.
Types of Physical Activity
Physical activity refers to “any bodily movement produced by skeletal muscles that results in energy expenditure above basal requirements.”72(p126) There are different types of physical activities that meet this definition, which can be categorized based on the main physiological systems they activate. The main types of physical activity are aerobic, resistance training, and flexibility training. 73 Aerobic (or endurance) activity refers to any activity that uses large muscle groups, can be maintained continuously for a long period of time, and is rhythmic in nature. 73 Examples include walking, jogging, running, cycling, dancing, skating, swimming, aerobics classes, and household chores (eg, vacuuming, sweeping, mopping, and raking). Walking is a commonly reported aerobic activity that is also enjoyable to many breast cancer survivors. 12 Resistance (or strength) training refers to any activity that uses resistance methods (eg, free weights, an individual’s own weight, machines, and elastic bands) to increase one’s ability to exert or resist force. 73 These activities involve concentric (ie, lifting and pushing/pulling) and eccentric (ie, controlled lowering/returning) muscle contractions and are done for each major muscle group (ie, quadriceps, hamstrings, hip adducters/abductors, upper/lower back, abdomen, chest, shoulders, biceps/triceps, and neck). Flexibility training refers to activities that lengthen muscles to increase range of motion around the joints. These activities can be static (ie, stretch is held for a period of time), dynamic (ie, fluid motion, such as Tai Chi), or active (ie, hold stretch while balancing, such as yoga). 73 These types of activities, alone or in combination, have been used in physical activity programs.
Of the reviewed studies, 10 studies examined the effect of aerobic training alone,24,28,47,49-51,56,64,67,69 12 examined the effect of aerobic training in combination with resistance training,21,29,48,52-55,57,58,62,70,71 5 examined the effect of resistance training alone,46,63,65,66,68 and 3 examined the effect of flexibility training24,60,61 on various health outcomes. The majority of the reviewed studies focusing on aerobic training prescribed the activity for participants,21,29,49-51,53-55,62,64,69-71 whereas others allowed participants to choose their preferred aerobic exercise28,47,48,56,57,59,67 or did not specify which aerobic activities were performed.24,52 Of the studies including resistance training, most had participants perform full-body exercises,29,46,48,53-55,63,65,66,68 whereas the remaining studies either had participants perform upper and core-body exercises,21,57,71 lower- and core-body exercises, 59 or did not specify which muscle groups were targeted.52,62,70 Of the studies including flexibility training as a main component of the intervention, 2 had participants do Tai Chi Chuan,60,61 and 1 did not specify what types of stretching exercises were used. 24 In addition, 12 studies included a flexibility component in the warm-up and/or cooldown21,29,46,48,53,55,57-59,66,68,71 but did not describe it.
All these studies concluded that physical activity led to improvements in physical and psychological health. The details for each exercise intervention and the main findings are found in Tables 1 to 4. The cumulative results of these studies suggest that all 3 types of physical activity (ie, aerobic, resistance, and flexibility training) are positively associated with numerous physical and psychological health benefits. Of note, in several studies, physical activity was not found to increase the incidence or severity of lymphedema.46,48,52,66,71 In 1 study, a change of less than 2 cm in arm circumference was recorded. 46 This finding is particularly important given clinical guidelines that previously cautioned against repetitive upper-body exercise (eg, upper-body resistance training) to prevent the development or worsening of lymphedema. 74 Based on the reviewed studies, physicians should recommend to patients that they engage in (1) resistance training for all major muscle groups, (2) aerobic training, and (3) flexibility training because all 3 types of physical activity optimize health outcomes. Although a comprehensive program is ideal, survivors may start with one type of activity and progressively incorporate other activities. The physical activity compendium 75 provides a broad list of physical activities from which survivors can choose from to develop their individualized program.
Intensity of Physical Activity
The intensity of aerobic and resistance training is important because this may affect the effectiveness of a program to improve overall health. It refers to the magnitude of the effort that is exerted to perform an activity. Intensity is most often characterized as light (ie, heart rate does not increase considerably above resting heart rate), moderate (ie, heart rate and sweating increases; can still maintain a conversation), or vigorous/strenuous (ie, fast and hard breathing, heart rate increases considerably, cannot maintain a lengthy conversation) and is monitored and measured using a variety of parameters. In 19 of the aerobic training studies reviewed, aerobic training intensity was monitored using physiological parameters—namely, a percentage of maximum heart rate (HRmax), heart rate reserve, or maximum oxygen consumption.21,24,28,47-51,53-59,62,67,69,70 One study also monitored intensity using a rating of perceived exertion, which is a subjective parameter whereby a person self-evaluates their level of fatigue, 24 and 3 studies did not specify how aerobic intensity was monitored.52,64,71
There was considerable heterogeneity in the magnitude of intensity between the studies. One study focused on light-intensity training, 57 9 focused on low- to moderate-intensity training,21,28,47,54,56,58,59,67,69 4 focused on moderate training,52,53,62,64 4 focused on moderate- to vigorous-intensity training,24,48,55,70 and 3 focused on vigorous-intensity training.49-51 Combining the evidence across studies, which consistently demonstrated that moderate-intensity activities led to improvements in physical and psychological health, physicians should focus on promoting moderate-intensity activity among patients. There are different approaches to monitoring aerobic intensity, and the preferred method of assessment may depend on each patient’s access and ability to acquire equipment. Based on the reviewed studies, physicians could suggest to patients that they monitor their intensity by wearing a heart rate monitor to ensure that they stay within a specific heart rate zone (ie, a percentage of their HRmax, whereby HRmax is calculated as 220 − age in years). According to the Centers for Disease Control and Prevention (CDC), light intensity is exercising at less than 50% of one’s HRmax, moderate intensity is exercising at between 50% and 70% of one’s HRmax, and vigorous training is exercising at more than 70% of one’s HRmax. For example, the estimated maximum age-related heart rate for a patient of 55 years would be 165 beats per minute (bpm). Moderate-intensity activity for this patient would require a heart rate between 83 and 116 bpm. It is important to note that deconditioned patients will likely reach their target heart rate more quickly than conditioned patients.
Patients could also determine whether they are exercising within their target rate zone by taking their pulse. Alternatively, physicians could tell patients to become aware of the physical symptoms experienced during exercise. For instance, physicians could explain to them that moderate-intensity aerobic activity will result in faster, less rhythmic, and often more shallow breathing and should make carrying on a conversation more difficult but achievable. Regardless of the approach used to monitor intensity, it is important to note that progressive aerobic training interventions (ie, participants start at light intensities and progress to moderate or vigorous intensities) yield positive physical and psychological benefits. Accordingly, physicians should recommend to their patients that they initially focus on increasing overall aerobic activity and then progress slowly to moderate-intensity activities as their bodies adjust to the physical challenges.
Within the resistance training interventions, a common strategy used to monitor intensity was to manipulate the workload, which consisted of 3 components: (1) number of sets (ie, series of repetitions performed without a break), (2) number of repetitions (ie, a single cycle of lifting/lowering a weight), and (3) weight lifted. In relation to the first 2 components, the majority of studies had participants complete between 2 and 3 sets per exercise and between 6 to 12 repetitions per set.29,46,48,53,55,57-59,62,63,65,66,68,70,71 In regard to the weight lifted, most studies had participants start with no weight or a light weight (ie, 0-0.5 pounds) for upper-body exercises.21,29,46,57,63,65,66,68,71 Alternatively, 3 studies had participants start at a percentage of their 1-repetition maximum effort,48,58,59 and 5 had participants select weights that invoked momentary feelings of muscle failure at the highest repetition being worked with.46,54,63,65,70 Most studies also had participants progressively increase the weight lifted by 5% or 10% or the smallest increments possible during the program to foster adaptation.29,46,54,57,66,68,71 Using such principles to monitor resistance training intensity, study participants experienced physical and psychological health benefits when they engaged in 2 or 3 sets of 6 to 12 repetitions per exercise using light weights and progressively using heavier weights throughout the duration of the interventions. Accordingly, physicians should recommend to patients that they initially focus on mastering the proper form and posture with a weight that is easy to lift and then progress slowly (ie, smallest increments possible) to heavier weights. Breast cancer survivors may want to consult a physical therapist, physical activity counsellor, or licensed fitness professional to assist them with developing a progressive physical activity program that reflects these recommendations as well as with learning proper and safe posture and form.
Frequency and Duration
Frequency refers to the number of times (or sessions) per week a person participates in physical activity. Of the reviewed studies, aerobic training sessions were held 2 to 5 times per week, with the majority having at least 3 sessions21,28,29,47-51,53-57,62,64,67,70,71,76; resistance training sessions were performed 2 or 3 times per week21,29,46,48, 53-55,57-59,62,63,65,66,68,70,71; and flexibility training sessions were performed 3 times per week.60,61,76 Results from these studies demonstrated that breast cancer survivors experienced health benefits by engaging in physical activity at these frequencies. Thus, physicians should recommend to patients that they engage in aerobic training at least 3 times per week, resistance training 2 to 3 times per week, and flexibility training 3 times per week. Of note, within the 12 studies that included an aerobic and a resistance training component, most interventions had participants perform both types of activities during the same session, which resulted in fewer (ie, 2 or 3) sessions per week21,29,54,55,70,71 than when participants completed both types of activities on alternative days (ie, 3 to 5 sessions/wk).48,53,58,59,62 However, given that both the concurrent training and alternative training interventions had positive effects on physical and psychological health, the approach used should depend on the patient’s preference and time availability. Physicians should therefore encourage patients to choose whether they prefer to engage in aerobic and resistance training sessions concurrently or on alternate days.
Duration refers to the length of time an exercise session lasts. The duration of the resistance training sessions was not consistently reported. When reported, the duration of these sessions varied between 40 and 90 minutes per session.46,53,58,59,63,65,66,68 The sessions for which the duration was longer (ie, 60 and 90 minutes)46,63,65,66,68 also included aerobic training and/or warm-up and/or cooldown components (ie, easy stretching and light-intensity aerobic activities), which makes it difficult to estimate the optimal duration for each type of activity. Despite this observation, some studies reported that the duration of the resistance training session depended on the time it took participants to complete the number of sets and repetitions of each exercise.21,29,48,55,57,62,70,71 These latter studies reported that participants experienced health benefits by performing between 6 and 12 exercises, suggesting that physicians should recommend to patients that they complete between 6 and 12 strengthening exercises per session.
The duration for flexibility sessions was consistently between 50 and 60 minutes per session, and health benefits were observed with these durations.24,60,61 Thus, physicians should recommend that patients participate in flexibility training sessions that last between 50 and 60 minutes. In contrast, there was substantial variation in the duration of aerobic training sessions (ie, ranging from 10 to 50 minutes per session).21,28,29,47-51,53,55-57,62,64,67,69,71,76 However, the majority of studies had participants striving to perform upward of 30 minutes of aerobic training per session.21,28,29,47-49,53,56,62,64,67,71 Given the evidence that breast cancer survivors experienced positive physical and psychological benefits by participating in 30 minutes of aerobic training per session, patients should be encouraged to participate in aerobic training for at least 30 minutes.
Discussion and Recommendations
This article introduces and explains evidence-based physical activity recommendations for breast cancer survivors to facilitate more effective, efficient, and consistent delivery of physical activity counseling by physicians. The findings from the studies reviewed herein provide consistent evidence that physical activity is safe and feasible and provides numerous physical and psychological health benefits.
On the basis of the results from the reviewed studies, a comprehensive program includes participation in aerobic training at least 3 times per week, resistance training 2 to 3 times per week, and flexibility training 3 times per week (see Table 5). These 3 types of activities can be done during 1 session (ie, concurrently) or on alternative days depending on the patient’s preference and time availability. There are certain commonalities between these guidelines and those put forward by the ACSM for cancer survivors, 30 the most notable being that both suggest that individuals should be active at moderate-intensity levels and include both aerobic and resistance training as part of their physical activity program. However, in light of the current evidence regarding the safety of flexibility training for breast cancer survivors observed in this review, the current recommendations also support the inclusion of flexibility training as an independent component of a physical activity program.
Recommended Characteristics of Exercise Program for Physical and Psychological Health Benefits
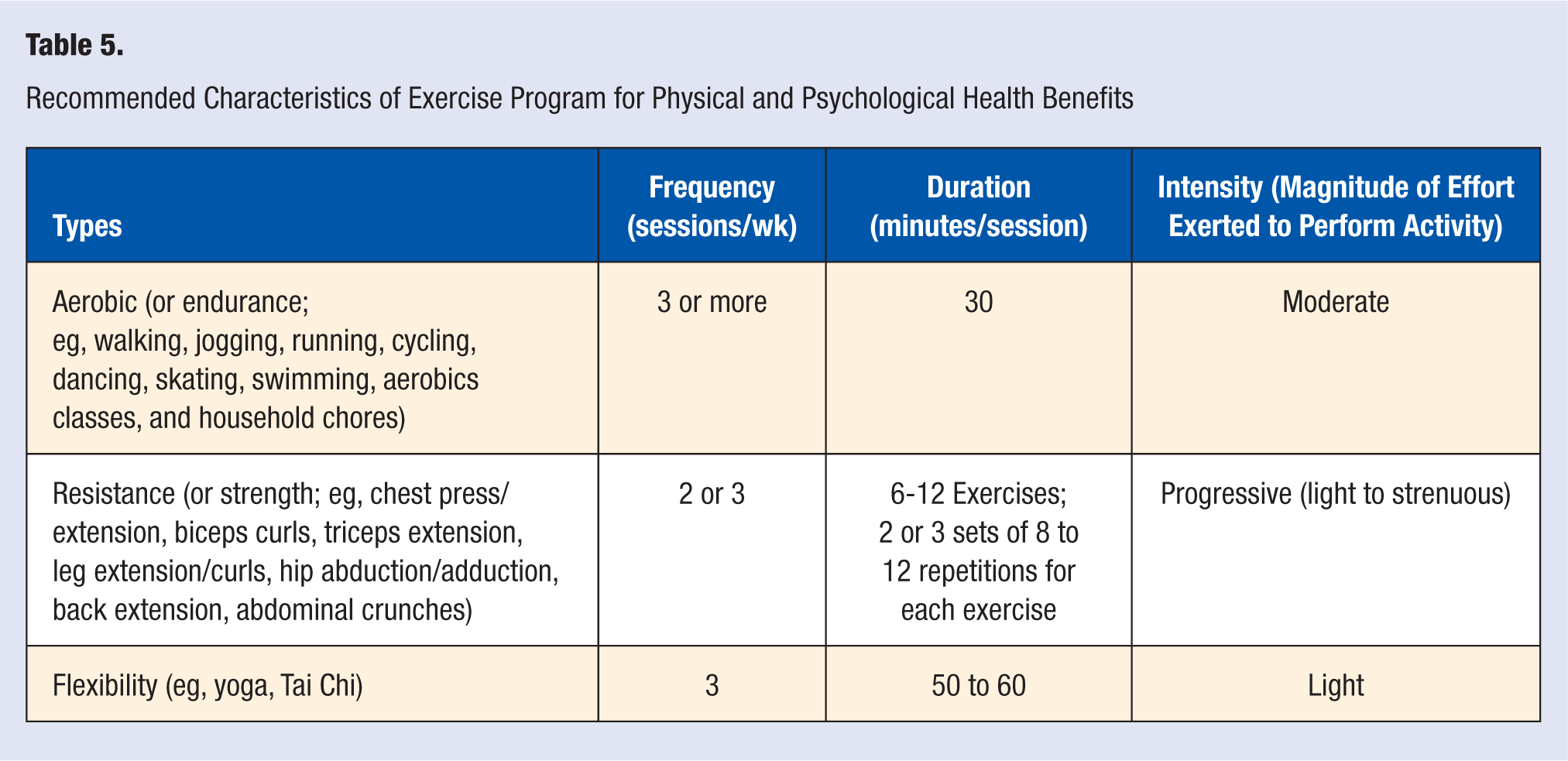
The first step in providing physical activity counseling to breast cancer survivors is to inform them about the health benefits 17 and provide them with clear evidence-based recommendations. Physicians are optimally positioned to provide physical activity counseling because they provide ongoing care to survivors, and this offers multiple opportunities to repeatedly convey this information. Physicians may want to distribute take-home handouts to patients, which include information on the benefits and recommended types, frequency, duration, and intensity of physical activity as displayed in Table 5, because handouts have been found to be effective in changing behavior. 77
Physicians should also try to support behavior change among patients. One approach to supporting physical activity behavior change would be to encourage patients to engage in intermittent bouts of activity throughout the day until they are able to complete a continuous longer bout of activity. Adherence to physical activity programs is higher among breast cancer survivors who engage in shorter exercise bouts (ie, 3 to 4 bouts of 10 minutes each) than among breast cancer survivors who engage in longer bouts (ie, one 30- to 40-minute bout). 78 This approach may be effective because it may be more appealing to patients who cite lack of time as a barrier to physical activity, and it may be better tolerated than continuous bouts among patients who cite fatigue resulting from treatment as a barrier. Shorter bouts may also be easier to accomplish, thus increasing enjoyment and motivation to persevere and enhancing longer-term adherence.79,80 Similarly, shorter bouts of activity may foster self-efficacy beliefs, 81 which in turn may positively relate with longer bouts and more challenging physical activities. 82 That is, patients who successfully complete shorter bouts may start to believe in their ability to complete longer physical bouts.
Another strategy to increase physical activity is to promote lifestyle physical activities. These activities are planned or unplanned activities that are part of everyday life such as leisure, occupational, household, and caregiving/childcare activities that provide an opportunity for patients to accumulate physical activity throughout the day. 83 This lifestyle approach may be particularly beneficial for patients who are reluctant to begin a traditional physical activity program because they fear that intense activity may worsen their breast cancer–related symptoms (eg, fatigue, pain, and nausea).
Successful physical activity counseling also requires that physicians and people trained to counsel special populations in physical activity recognize that breast cancer survivors may face the same common barriers to being physically active as healthy adults (eg, lack of time, motivation, and enjoyment), as well as disease/treatment-specific barriers, such as feeling sick and tired, experiencing pain and being afraid to exercise.84,85 Thus, physicians interested in helping patients increase physical activity levels should address these barriers and offer strategies to overcome these barriers when counseling patients. According to Courneya and colleagues, 84 breast cancer survivors should be encouraged to engage in physical activity when fatigue levels are lowest (eg, in the morning), for shorter durations, and at lower intensities and perform interval training (ie, alternate activity and rest bouts).
Another aspect to consider when providing physical activity recommendations to patients is the nature of the collaboration between physicians and patients. 86 Although physicians can make suggestions to patients on how they can increase their physical activity levels, patients should be encouraged to make their own choices. There is evidence that providing choices for physical activity is associated with greater participation. 87 Given that studies where breast cancer survivors selected their favorite and most convenient activity documented significant health benefits,28,47,48,56,57,59,67 physicians should encourage patients to choose activities that are of interest to them because this will likely motivate them to initiate and maintain a physical activity routine.
Whereas the findings from the reviewed studies indicate that breast cancer survivors who follow these guidelines will likely experience increased physical and psychological well-being (see Tables 1 to 4), it is important to keep in mind that the current physical activity recommendations were developed based on findings from published studies that have inherent limitations, such as attrition bias of study participants, failure to fully describe intervention (eg, rate of progression) and report adherence to intervention, and publication bias. Findings were also derived from studies that did not examine dose effects, such that the current recommendations suggest that benefits are experienced by engaging in aerobic activity at a minimum of 3 times per week for at least 30 minutes, whereas it is possible that engaging in physical activity less often also yields benefits (and/or increasing the frequency of physical activity yields additional benefits). Furthermore, the reviewed studies included samples of breast cancer survivors who were screened for eligibility. Many of the reviewed studies did not include samples that represent the complete spectrum of breast cancer survivors (ie, survivors exhibiting a primary or secondary medical condition, metastases, and comorbidities). Thus, although not reported in the reviewed studies, it is possible that physical activity may pose some risk (eg, falls, bone fractures, and increased pain) for some cancer survivors. 88 It is recommended that physicians working with patients who have or who are predisposed to underlying medical conditions consult the guidelines for preexercise medical assessments and exercise testing forwarded by Schmitz et al. 30 In addition, physicians may want to encourage patients to participate in physical activity sessions that are supervised by a fitness professional who has received certification from an international authority to work with special populations (eg, ACSM and National Strength and Conditioning Association)—at least until their medical condition is under control.
Conclusions
In conclusion, although the various treatment options offer a positive outlook for surviving breast cancer, there are a number of notable short- and long-term physical and mental side effects associated with them.5-9 It is therefore necessary to consider interventions that may reduce the negative symptoms experienced by this population. Physical activity may help in the prevention and management of many of the side effects and is beneficial for breast cancer survivors. Thus, it is hoped that the evidence-based recommendations provided herein will facilitate more effective, efficient, and consistent delivery of physical activity counseling and that this will lead to improved patient outcomes in breast cancer survivors. To this end, physicians are encouraged to at least inform patients about the benefits and recommendations for physical activity. Subsequently, physicians may choose to refer patients to other allied health professionals (eg, physical activity counselors, physical therapist, or exercise specialists) to help them develop and initiate a physical activity program. 89