
Abstract
This article provides an overview of mental and physical health outcomes of child maltreatment to help health care providers identify the consequences of maltreatment and consider treatment options. Child maltreatment is associated with a variety of negative physical and mental health outcomes that affect the individual throughout the lifespan and place a substantial burden on both victims and the population as a whole. The review begins with an overview of the role of physicians in identifying abuse and neglect in the clinic setting. Next, current research findings on physical and mental health outcomes in children, adolescents, and adults are reviewed. Finally, opportunities for primary prevention of abuse and neglect are discussed. Primary prevention strategies can avoid risk for maltreatment, and subsequent interventions for victims have the potential to greatly improve their health.
“Child maltreatment comprises both child abuse, including physical, sexual, and emotional abuse, and child neglect.”
Child maltreatment, defined as “any act or series of acts of commission or omission by a parent* or other caregiver that results in harm, potential for harm, or threat of harm to a child,” † is a substantial problem in the United States with serious consequences for the individual, his or her family, and the community. 1 In this article, we will review the literature on the long-term physical and mental health outcomes of child maltreatment and discuss the impact on the lives of survivors.
Child maltreatment comprises both child abuse, including physical, sexual, and emotional abuse, and child neglect. Definitions of the types of maltreatment are presented in Table 1, and prevalence estimates by type are presented in Table 2.Depending on the data source and definition of maltreatment used, estimates of the prevalence of child maltreatment vary from 1 to 10 out of every 100 children in the United States.2-4 Approximately 1740 children in the United States died as a result of maltreatment in 2008, ‡ a mortality rate of 2.34 per 100,000 children in the United States. 4 Child neglect accounts for the majority of maltreatment, and neglect alone or in combination with other types of maltreatment accounts for the majority of child maltreatment fatalities. 4 Emotional abuse is least often substantiated, or confirmed, by Child Protective Services, yet it is a common behavior reported by parents. 5
CDC Definitions of Maltreatment Types
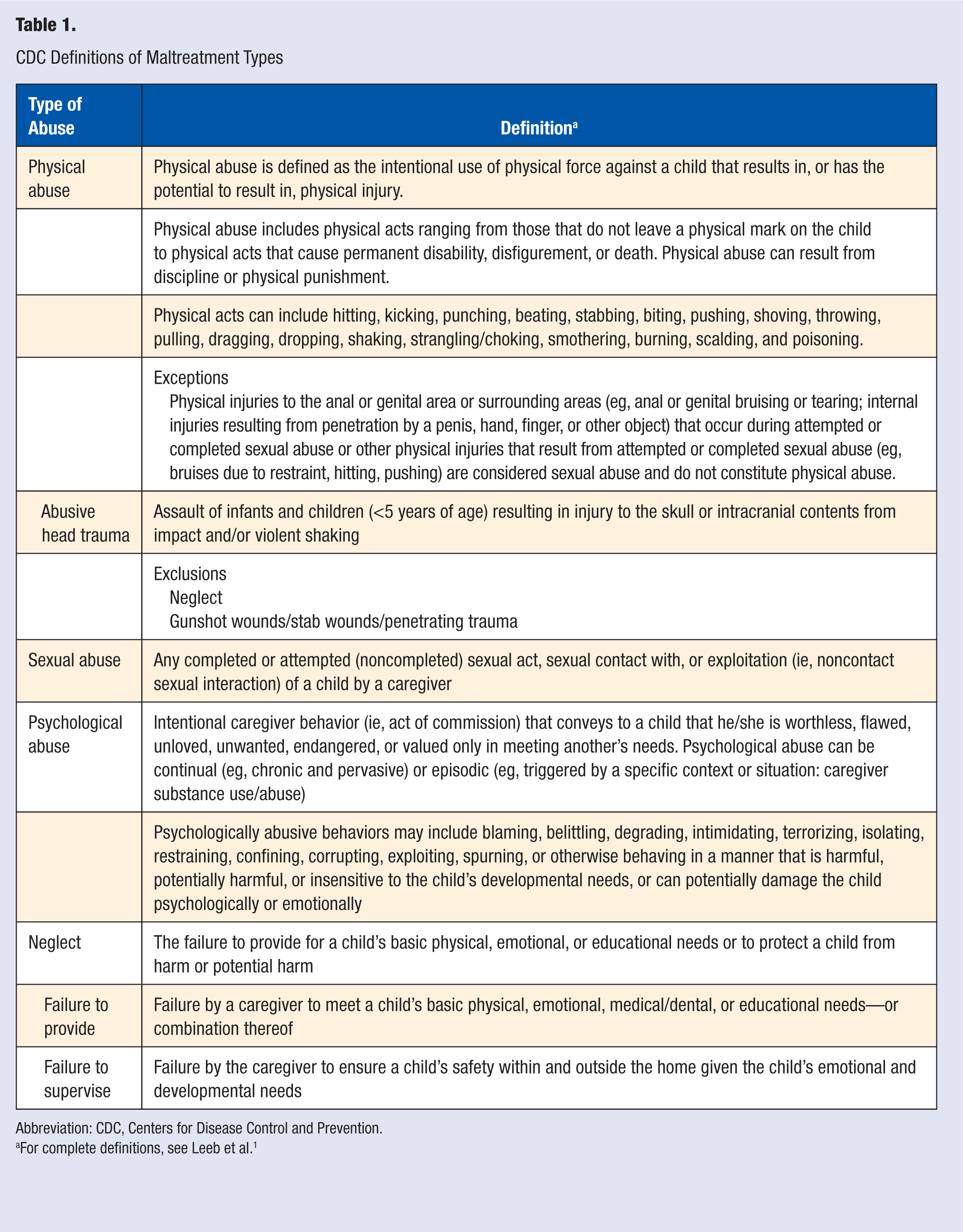
Abbreviation: CDC, Centers for Disease Control and Prevention.
For complete definitions, see Leeb et al. 1
Comparison of Counts of Maltreated Children as Reported by National Child Abuse and Neglect Data System (NCANDS) and the Fourth National Incidence Study (NIS-4)
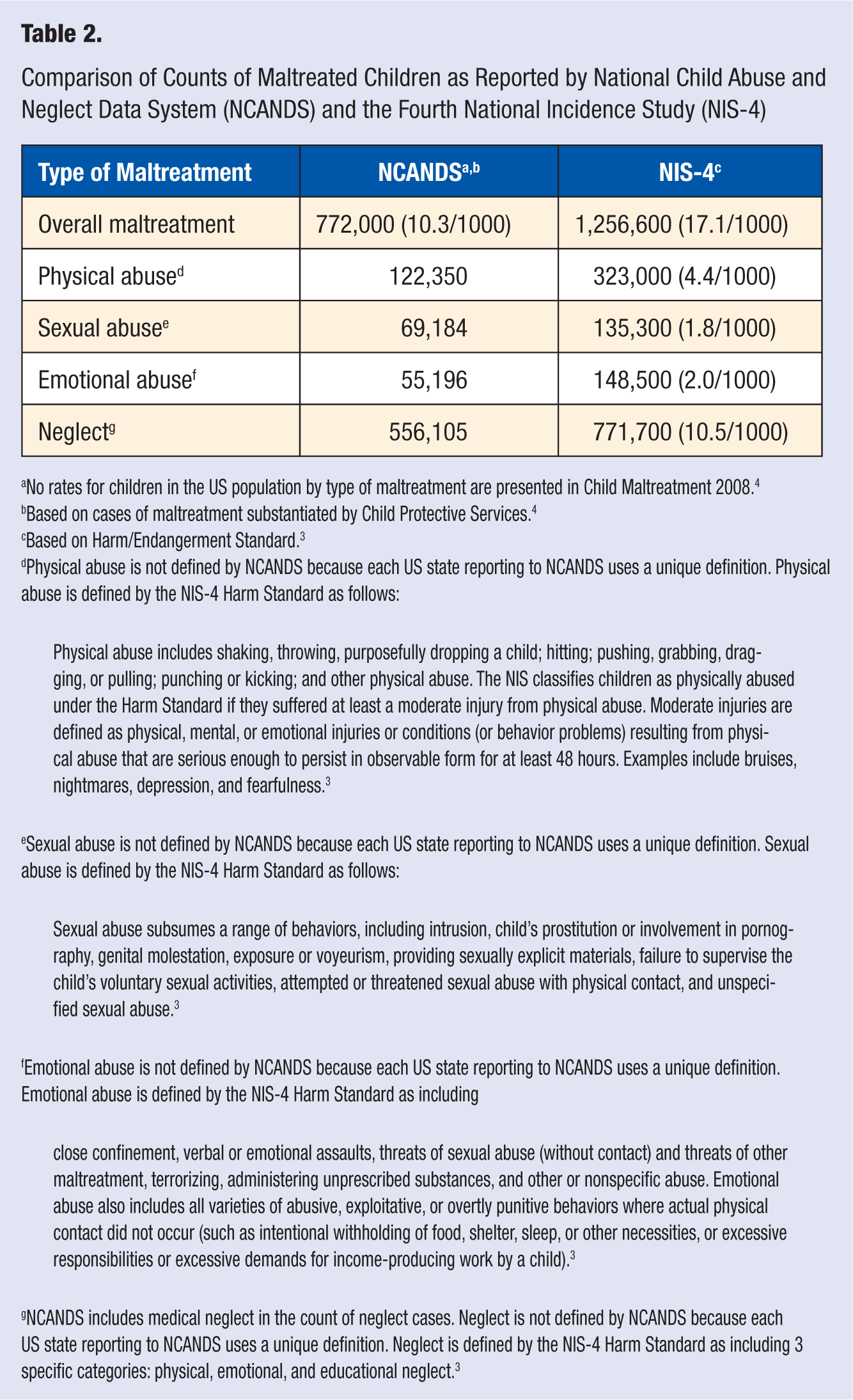
No rates for children in the US population by type of maltreatment are presented in Child Maltreatment 2008. 4
Based on cases of maltreatment substantiated by Child Protective Services. 4
Based on Harm/Endangerment Standard. 3
Physical abuse is not defined by NCANDS because each US state reporting to NCANDS uses a unique definition. Physical abuse is defined by the NIS-4 Harm Standard as follows:
Physical abuse includes shaking, throwing, purposefully dropping a child; hitting; pushing, grabbing, dragging, or pulling; punching or kicking; and other physical abuse. The NIS classifies children as physically abused under the Harm Standard if they suffered at least a moderate injury from physical abuse. Moderate injuries are defined as physical, mental, or emotional injuries or conditions (or behavior problems) resulting from physical abuse that are serious enough to persist in observable form for at least 48 hours. Examples include bruises, nightmares, depression, and fearfulness.
3
Sexual abuse is not defined by NCANDS because each US state reporting to NCANDS uses a unique definition. Sexual abuse is defined by the NIS-4 Harm Standard as follows:
Sexual abuse subsumes a range of behaviors, including intrusion, child’s prostitution or involvement in pornography, genital molestation, exposure or voyeurism, providing sexually explicit materials, failure to supervise the child’s voluntary sexual activities, attempted or threatened sexual abuse with physical contact, and unspecified sexual abuse.
3
Emotional abuse is not defined by NCANDS because each US state reporting to NCANDS uses a unique definition. Emotional abuse is defined by the NIS-4 Harm Standard as including
close confinement, verbal or emotional assaults, threats of sexual abuse (without contact) and threats of other maltreatment, terrorizing, administering unprescribed substances, and other or nonspecific abuse. Emotional abuse also includes all varieties of abusive, exploitative, or overtly punitive behaviors where actual physical contact did not occur (such as intentional withholding of food, shelter, sleep, or other necessities, or excessive responsibilities or excessive demands for income-producing work by a child).
3
NCANDS includes medical neglect in the count of neglect cases. Neglect is not defined by NCANDS because each US state reporting to NCANDS uses a unique definition. Neglect is defined by the NIS-4 Harm Standard as including 3 specific categories: physical, emotional, and educational neglect. 3
Research has clearly demonstrated that child maltreatment places a substantial burden on children, families, and society. One of the most important consequences of childhood maltreatment is the impact to health and development.6-11 Child maltreatment affects all aspects of the lives of those victimized including changes to brain architecture, poor physical health, reduced cognitive ability and educational attainment, and impaired psychosocial functioning and mental health.6,7,10-26
In 2008, the combined estimate of the direct cost (including hospitalization, chronic physical health problems, mental health care, welfare costs, law enforcement, and court action) and indirect long-term economic effects (eg, loss of educational attainment and work productivity, burden on insurers) of child maltreatment was approximately US$104 billion. 27 Health care usage factors significantly into the societal cost of maltreatment.6,28-30 For example, individuals with a history of physical or sexual abuse are more likely to use emergency services and report greater use of health professionals than adults without a history of childhood abuse.31-33 Increased utilization of health care services by adult survivors of childhood maltreatment may be explained or exacerbated by the higher rates of pain complaints, disability, and somatic symptoms as well as comorbid psychiatric disorders reported by, and diagnosed in, these individuals.6,32-34
The purpose of this article is to provide an overview of mental and physical health outcomes of child maltreatment in order to help health care providers identify the consequences of maltreatment and consider treatment options. We begin with a review of the role of physicians in identifying abuse and neglect in the clinic setting. Next, we will review the literature on physical and mental health sequelae beginning with an examination of the effect of abuse and neglect on brain architecture and consequences for development. Finally, we will discuss opportunities for, and efforts toward, primary prevention of abuse and neglect.
Identifying Child Maltreatment in the Clinic Setting
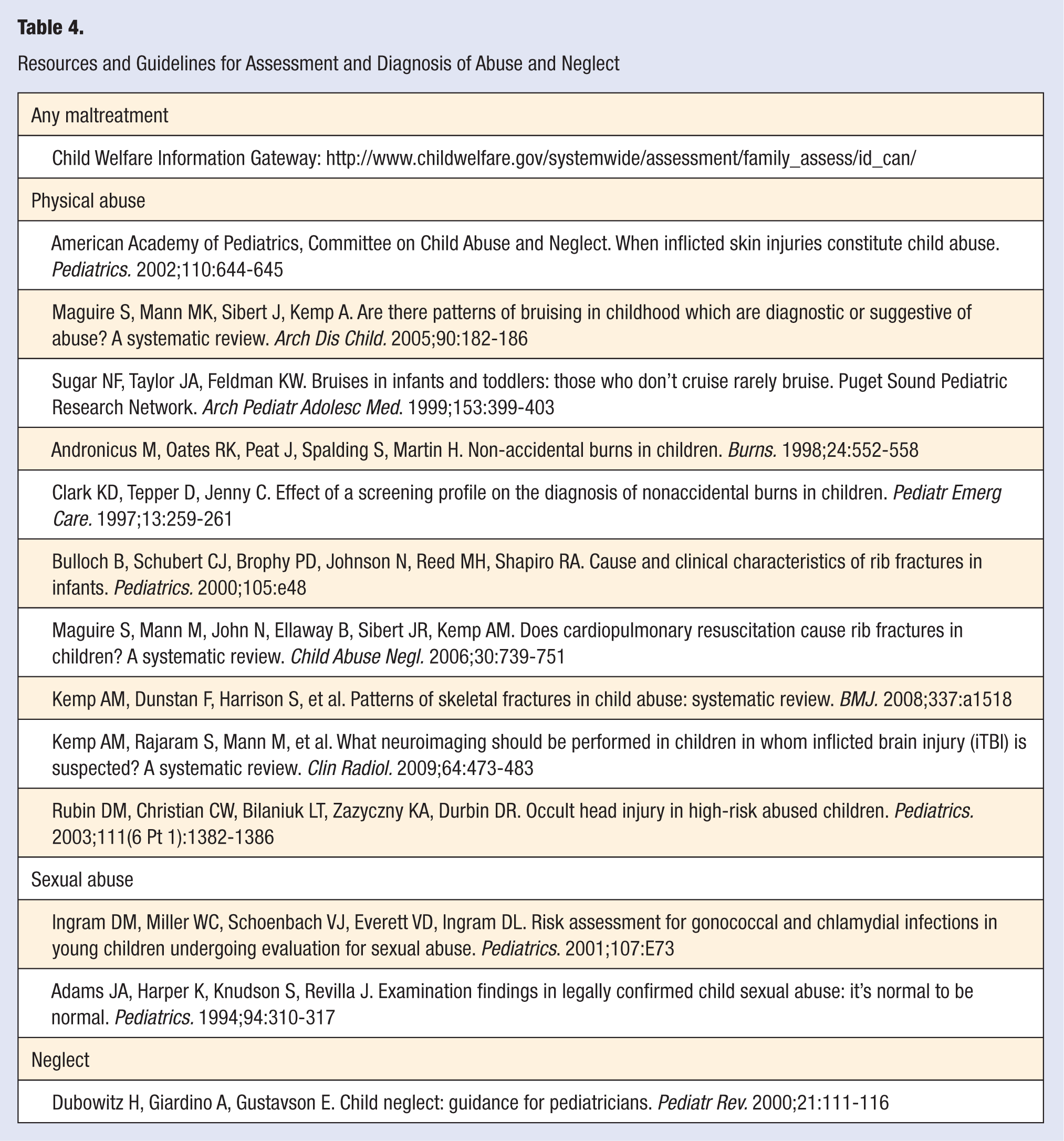
Physicians, as first-line responders to physical and mental health symptoms, are in a unique position to identity signs of injury or distress early and interrupt the development of deleterious health consequences. To improve health outcomes at the population level, primary prevention, that is, preventing a disease or condition before it begins, is the ultimate goal. In this section, we will provide an overview of conditions that may suggest possible maltreatment in children when presented in a clinical setting. Table 3 lists some common signs and symptoms of abuse and neglect. Various guidelines exist for assessing and diagnosing maltreatment within the clinic setting, and Table 4 provides some specific resources, references, and guidelines for assessment and diagnosis. Barriers to reporting maltreatment to social services and implications of not reporting on the lives of victims will also be discussed.
Proximal Indicators of Abuse and Neglect a
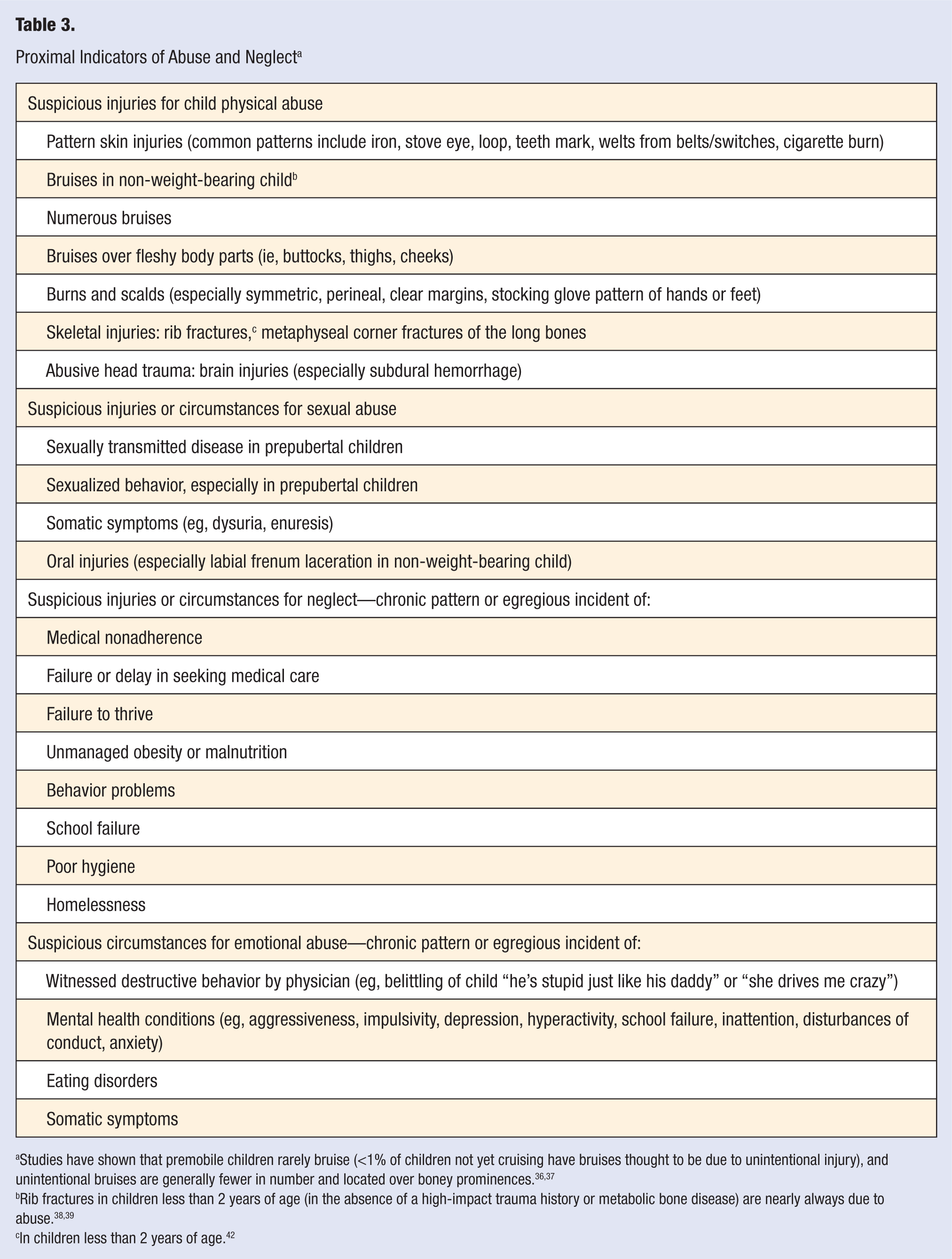
Studies have shown that premobile children rarely bruise (<1% of children not yet cruising have bruises thought to be due to unintentional injury), and unintentional bruises are generally fewer in number and located over boney prominences.36,37
Rib fractures in children less than 2 years of age (in the absence of a high-impact trauma history or metabolic bone disease) are nearly always due to abuse.38,39
In children less than 2 years of age. 42
Resources and Guidelines for Assessment and Diagnosis of Abuse and Neglect
Physical Abuse
Physical abuse accounts for approximately 19% of the maltreatment cases substantiated by Child Protective Services 4 (Table 2). Injuries that are unexplained, inconsistent with the history provided by the child or caregiver, in a pattern suspicious for inflicted injury, developmentally inconsistent, or due to punishment with excessive force may suggest abuse when presented in the clinic or emergency setting. 35 Children who suffer physical abuse may manifest a variety of external and internal injuries that can be life threatening. Abusive head trauma (AHT), which can result from shaking or a blunt impact to the head, is a common form of physical abuse in very young children (<5 years of age) and is the most common cause of death due to child physical abuse.36,37 Common injuries related to AHT include a pattern of skull fracture, retinal hemorrhaging, subdural hematoma, permanent neurologic disability, mental retardation, cortical blindness, seizure disorders, and learning disabilities. AHT often results from inappropriate caregiver response to crying and a lack of caregiver understanding of age-appropriate behavior in infants and toddlers. The American Academy of Pediatrics, Committee on Child Abuse and Neglect, provide guidelines on the epidemiology and clinical management of AHT. 36
Sexual Abuse
Child sexual abuse is unique in that it usually presents with child disclosure. However, presentation may vary and include acute sexual trauma, sexually transmitted disease, and pregnancy. Risk for sexual abuse appears to be greatest during 2 developmental periods: in early childhood and again in adolescence. 38 Information on gender differences in the prevalence sexual abuse is equivocal because many boys are reluctant to disclose sexual abuse. Interviewing children for evidence of sexual abuse requires special skill and training. In a nonthreatening and familiar setting, a child may disclose abuse to a physician in the context of a thorough medical history.
Neglect
Neglect is the most common form of maltreatment accounting for more than 60% of all substantiated Child Protective Services cases. 4 Because neglect is characterized by a chronic pattern of caregiving behaviors, it is important for primary care physicians to understand the symptoms of neglect (see Table 3) and be vigilant to recognize signs of neglect over time. Additionally, various other factors, such as access to resources and cultural practices, may affect caregiving behavior. Guidance for physicians for recognizing neglect is available. 39
Emotional Abuse
In surveys of parenting behavior, it is not unusual for caregivers to report engaging in emotionally abusive behaviors toward their children, for example, belittling behaviors: “he’s stupid just like his daddy” or “she never does anything right.” However, the diagnosis of emotional abuse is often made only through long-term observation of parent–child interaction because, like neglect, this form of maltreatment is characterized by an ongoing pattern of caregiver behaviors. Consequently, emotional abuse is the type of maltreatment that is least often reported to child welfare. Symptoms of emotional abuse include child and adolescent mental health conditions, including aggressiveness, impulsivity, depression, hyperactivity, school failure, inattention, disturbances of conduct, anxiety, eating disorders, and somatic symptoms. Identification of families that are at risk or may be engaging in emotionally abusive behavior can be facilitated by querying other adults involved with the child (eg, teachers, coaches) when possible. Physicians can discuss destructive behavior and role modeling positive behavior with caregivers, which may help parents identify more constructive responses to their children.
Reporting Maltreatment to Authorities
When abuse and neglect are identified early, physical and psychological impacts can be significantly reduced and a better environment can be created for the child. However, to get needed services and intervention for maltreated children as early as possible, suspected maltreatment must be reported to authorities. Issues of reporting child maltreatment are particularly salient and have a direct impact on the future health, well-being, and quality of life for children and adults who have been victimized.
All states, districts, and territories in the United States have child abuse reporting statutes that include physicians as mandated reporters for suspected child abuse and neglect. However, many physicians report reluctance to report maltreatment. Physicians report fear of liability, lack of expertise, concern with providing testimony in court, and concern that the child and family may not be better off after social intervention. Rates of failure to report suspected abuse are in the moderate range (8% to 28%).40-43 Education and exposure to medical expertise related to child abuse can improve knowledge and comfort with reporting. 44 In response to the need for education, a new medical subspecialty in Child Abuse Pediatrics was developed in 2006 and the first board exams were offered in 2009. This subspecialty is designed to train pediatricians to recognize and identify child maltreatment as presented in a clinical setting. Additionally, understanding that reporting is a legal responsibility may absolve some of the guilt that many physicians may feel in making a report to Child Protective Services.
Physical and Mental Health Outcomes of Child Maltreatment
Unfortunately, because of the secretive nature of child maltreatment, it is estimated that 50% to 90% of maltreated children do not come to the attention of authorities, and thus do not receive any intervention to offset potential negative consequences of maltreatment. Furthermore, abuse history goes largely unassessed in clinical settings. 45 Walker et al reported that only 4% of health care providers in a primary care clinic had inquired about abuse history, and Lechner et al reported that only 5% of their study participants disclosed abuse to a physician.29,46,47
Neurobiological Impacts of Child Maltreatment and Effects on Child Development
There is evidence for neurobiological changes resulting from childhood abuse and neglect that appear to have an impact on development, health, and behavior. Both animal and human models indicate that there may be lasting changes to specific anatomical features of the brain, for example, reduction in overall brain volume, and changes to specific physical structures (eg, corpus collosum, hippocampus, amygdala) and the stress-response system (hypothalamic–pituitary–adrenal axis).17,19,23,48-51 Nonprimate animal research on early stress has shown evidence for atypical stress responses in rat pups after repeated separation from their mothers during the neonatal period. In nonhuman primate studies, researchers have found anatomical brain changes (decreased corpus collosum volume) and increased stress response in rhesus monkeys reared in atypical social environments.17,48
Advances in technology, such as functional magnetic resonance imaging (fMRI), have allowed researchers to examine changes to human brain anatomy and function resulting from child maltreatment. Similar to animal models, changes to neuroanatomy and stress response in humans have been seen in MRI and fMRI studies, as well as changes to salivary and urinary cortisol levels.19,52 In adults, stress resulting from childhood victimization may be responsible for chronic activation of the stress response system, which may result in hypersensitivity or vulnerability to pain, such as that seen in conditions like fibromyalgia.6,19,54-56 The most current work in the neurobiology of maltreatment focuses on identifying neurobiological changes to specific features that constitute particular physical and mental health outcomes, such as posttraumatic stress disorder (PTSD), as well as efforts to understand whether neurobiological changes related to trauma reflect preexisting individual vulnerability rather than direct consequences of trauma exposure. 19
Chemical and anatomical brain changes almost certainly impact children’s development and behavior.57,58,59 It is hypothesized that traumatic events sensitize the brain, particularly during periods of critical brain growth and development, which leads the brain to become chemically organized in an atypical and dysfunctional fashion.58,59 Similarly, when children are exposed to high levels of physical trauma (eg, physical or sexual abuse), the neurological pathways in the brain that are responsible for the “fight or flight” response are overactivated for prolonged periods of time, again, causing the brain to become organized in a dysfunctional manner. 58 The dysfunctional organization manifests in poor physical and mental health and maladaptive behaviors such as somatization, aggression, and substance abuse.
Physical Health Outcomes in Children
The consequences of maltreatment in childhood manifest most conspicuously in the form of physical injury. Common injuries, especially in the abuse of infants and toddlers, include fractures, traumatic brain injury, bruises, burns, and subdural hematomas. Sexual abuse may involve genital and anal injury and sexually transmitted infections in children of any age and pregnancy in post-pubertal girls. Health consequences of neglect may include failure to thrive, untreated obesity, vitamin deficiencies, untreated medical conditions, and injuries such as burn or overdose/poisoning resulting from lack of supervision. 60 To help physicians distinguish between abuse and unintentional injury, efforts have been made to identify distinguishing features of abusive injury types. For example, head injury in combination with retinal hemorrhaging in children aged 5 years and younger may be indicative of abusive head injury, and certain patterns of skeletal fractures such as spiral fractures may be indicative of inappropriate or abusive discipline.24,61 In addition to the direct injuries related to abuse and neglect, there is evidence to suggest that other aspects of poor physical health are also more prevalent in maltreated children. Children who have been victimized have increased risk of asthma and other cardiorespiratory diseases, infections (eg, intestinal, bacterial, viral), and greater use of hospital care.16,62
Mental Health Outcomes in Children and Adolescents
The most common childhood mental health outcomes related to maltreatment are attachment disorders, behavior disorders (including externalizing behaviors, anger and aggressive behavior, and antisocial behavior), posttraumatic stress, and mood disorders (depression, anxiety, withdrawn behavior).* In general, children who have experienced maltreatment are more likely to evidence higher rates of internalizing (eg, depression and anxiety) and externalizing (acting out behaviors, eg, aggression) behaviors.12,18,65,66,69
The role of posttraumatic stress symptoms and PTSD on physical health in abused children has received substantial attention. PTSD is common in children who have been victimized by caregiver abuse or neglect. The reported incidence rates of PTSD in children who experienced sexual abuse have been found to be as high as 90% and as high as 50% for children with a history of physical abuse. These symptoms continue to be evident in many children for a significant time after the victimization experience indicating that the effects of abuse on childhood mental health may be long-lasting. 70 The enduring mental health impacts of maltreatment may be associated with the chemical and anatomical brain changes discussed earlier. PTSD has been linked to brain abnormalities in both maltreated children and adults, especially those who experience more severe forms of maltreatment.71-76 These changes may cause maltreated children to have difficulty self-regulating behavior and contribute to engagement in health risk behaviors later in life. 70
Various aspects of maltreatment (eg, timing, chronicity, type, severity) play an important role in children’s mental health. Children who experienced severe physical neglect during the preschool period were found to exhibit greater internalizing symptomatology and withdrawn behavior compared with other maltreated children. 69 Similarly, children who experienced neglect prior to age 2 years, but not other types of maltreatment, evidenced more aggressive behavior measured in early and middle childhood. 77 In addition, toddlers and young children who experience physical abuse may be more aggressive and exhibit more externalizing behaviors with peers than children who experience other forms of maltreatment. Maltreated children have been shown to respond to friendly overtures by peers and adults with avoidance, fear, and anger.14,24,63,64,69 Physically abused children also evidence more severe behavioral and emotional outcomes than children who experience other forms of maltreatment.14,26,68 Chronic maltreatment with onset during the infancy, toddlerhood, or preschool periods is associated with more adverse outcomes than maltreatment that begins later in childhood.20,69 Experiencing multiple types of maltreatment also has particularly severe consequences. As the number of maltreatment experiences increases, there appears to be a linear increase in depression and anger/aggression. 26 Thus, when considering mental health outcomes in maltreated children, it is important to also consider the specifics of the abuse and neglect experience(s).
Poor mental health outcomes continue into adolescence for youth who have experienced maltreatment. Adolescent mental health outcomes build on the platform of problematic behaviors and emotional consequences seen in younger children and manifest in unique ways. As is the case in the childhood research literature, the predominant focus in the adolescent literature is on internalizing and externalizing behaviors.18,22,78-89 Overall, adolescents who have experienced maltreatment, or are currently experiencing maltreatment, are more likely to be involved in acting-out behaviors such as truancy, running away, vandalism, and property offenses, as well as physical fighting, weapon carrying, and threatening with or using a weapon.25,85,89-100 In general, boys are more likely than girls to be involved in physical violence; however, girls who experience sexual abuse are much more likely than other girls to participate in violent behavior and may choose to carry or use a weapon for protection.90-93 Adolescent boys who have experienced abuse are also more likely than nonabused adolescent boys to be involved in physical violence, gang membership, and weapon carrying and use.94,95 There is speculation that maltreated youth may develop attributions that others possess hostile intent even when no hostility is intended and as a result respond to perceived threats with aggression and other violent behavior. 96
Depression and deliberate self-harm (suicidal ideation, suicide attempts, eating disorders, and self-harm without suicidal intent) are the most commonly discussed internalizing behaviors in maltreated adolescents.22,78-86,88 A great deal is known about internalizing problems in maltreated females with a history of sexual abuse, but less is known about males or youth who experience other forms of maltreatment. However, there is some evidence that maltreatment has an impact on internalizing behaviors in both male and female adolescents. Sexual abuse has been found to be a strong predictor of suicidality, including suicidal thoughts, plans, threats, and attempts, and deliberate self-harm for both male and female adolescents.22,84-86 The relationship between experiencing multiple forms of abuse, as the vast majority of maltreated children do, and internalizing behavior is particularly strong. Adolescents who have experienced multiple forms of abuse are more likely to report greater withdrawn and anxious/depressed symptoms.4,18
Child and adolescent mental health problems, both acting-out (externalizing) behaviors and depression/anxious behaviors, may manifest in health risk behaviors such as early initiation of tobacco, alcohol, and other substance use; sexual behavior and teen pregnancy; as well as involvement in risky friendships and dating relationships, truancy, and running away.20,89,97,98 As is the case for much of the literature, a significant portion of research on health risk behaviors has focused on girls with a history of sexual abuse. However, a recent report focusing on a mixed-sex sample of adolescents found that adolescents who experienced abuse were more likely than their nonabused peers to begin drinking alcohol prior to age 13 years and engage in binge drinking. 97 Adolescents who experienced physical abuse were more than twice as likely as their nonabused peers to report preteen alcohol use. Gender differences were also found with adolescent boys with a history of sexual abuse 2.5 times as likely to report binge drinking than boys with no such history. Furthermore, adolescents who reported experiencing 2 or 3 types of maltreatment versus 1 type were more than 3 times as likely to report ever using alcohol. There is some evidence that these behaviors may be related to depression, posttraumatic stress, and cognitive distortions.6,7,99
Injuries and other symptoms of poor physical health as well as internalizing and externalizing behaviors and other mental health issues may be used as markers or warning signs of maltreatment in children and youth. Poor health indicators can prompt further investigation by health care professionals and early identification of abuse and neglect. If this approach is taken to the treatment of children then subsequent negative sequelae may be attenuated and quality of life improved.
Adult Health Outcomes Related to Child Maltreatment
There is substantial evidence that the untreated effects of child maltreatment extend into adulthood to impact physical and mental health outcomes, as well as vulnerabilities to other victimization in adulthood. †
Physical health
Associations between various aspects of childhood maltreatment and numerous specific physical health outcomes in adults have been noted, including functional pain disorders, migraines, gynecological pain, ischemic heart disease, cancer, chronic bronchitis, hepatitis, skeletal fractures, as well as overall ratings of poor physical health.7,63,107 Chronic pain syndromes and gastrointestinal disorders have received considerable attention, particularly in women.30,53,108,109 For example, childhood abuse has been strongly linked to fibromyalgia and chronic fatigue syndrome in samples of women.30,109-111 There is also evidence that other functional syndromes are associated with childhood abuse.29,96,108,112 Sexual and physical abuse have been associated with irritable bowel syndrome and functional versus organic gastrointestinal disorders.29,96,108 Individuals with a history of abuse are more likely to also report nonabdominal symptoms, more lifetime surgeries, and are at greater risk for pelvic pain than their nonabused counterparts. Greater prevalence of somatization disorders or multiple somatic symptoms in those with a history of abuse is also a common finding.29,108,112 Taken together, these studies suggest higher rates of gastrointestinal symptoms and greater prevalence of somatic symptoms in patients with a history of maltreatment.
In addition to specific pain syndromes, complaints of chronic pain or pain that interferes with activities appear to be prevalent in adults with a history of childhood maltreatment.30,113-116 For example, adult women who self-reported a history of childhood sexual or physical abuse were 4 times more likely to report 6 or more physical symptoms compared with those reporting no symptoms or 2 symptoms. 117 Greater prevalence of other conditions associated with pain complaints, such as migraines and headaches, have also been documented in those with a history of childhood physical abuse and sexual abuse.118-120 Similarly, associations have been found between abuse history and poor gynecological health with women who experienced childhood abuse reporting more pelvic pain, vaginismus, and genitourinary disorders. ‡ Finally, associations have been found between childhood victimization and chronic diseases such as respiratory problems, cardiopulmonary problems, arthritis, musculoskeletal problems, neurological problems, cancer, obesity, and liver disease. § Adults with a history of physical abuse have been shown to be at significantly greater risk (34% to 167%) of allergies, arthritis/rheumatism, asthma, bronchitis/emphysema, circulation problems, high blood pressure, heart troubles, liver troubles, and ulcers. 11
Overall, the literature on physical health outcomes in adults with a history of maltreatment indicates that there are significant impairments to physical health associated with abuse and neglect. Outcomes for adults with a history of abuse and neglect, particularly physical and sexual abuse, are poorer than for adults with no history of maltreatment. Furthermore, it has been suggested that many of the physical health outcomes seen in adult survivors of abuse and neglect may be partially explained by mental health problems and/or engagement in health risk behaviors.
Intervening factors that may impact physical health outcomes
Risk behaviors, poor social relationships, poor mental health, and poor attitudes about health are more prevalent in survivors of childhood abuse. These factors may help explain the association between abuse history and poor adult physical health. 123 For example, health behaviors such as smoking, alcohol use/abuse, and obesity appear to be critical pathways for physical health problems such as bronchitis and poor general physical health in individuals with a history of abuse and neglect. Similarly, poor mental health is an important pathway for ulcers and poor general physical health.7,124,125
Mental health
A wide range of psychological symptomatology and psychiatric disorders have been associated with abuse and neglect. Overall, adults who have experienced childhood abuse or neglect manifest a vast array of poor mental health outcomes including significantly greater likelihood of being diagnosed with clinical disorders such as personality disorders, mood disorders (including depression and anxiety), and PTSD.6,104,126,127 Additionally, many adult victims of childhood abuse report symptoms such as anxiety, depression, trauma, somatization, paranoia, and hostility; manifest dysfunctional interpersonal attachment styles; have increased risk of suicide attempts; and display cognitive distortions. ‖ (For a detailed review of outcomes related to sexual violence in women see Basile and Smith, 100 this issue.)
Intervening factors that may impact mental health outcomes
There is evidence that factors such as the timing, severity, and type(s) of maltreatment experienced; other co-occurring adverse childhood experiences; and family background characteristics may exacerbate or attenuate the effects of childhood maltreatment on adult mental health outcomes. Poorer outcomes have been found for those who experience early onset, chronic, severe, or multiple types of maltreatment. ¶ Multiple victimizations (not limited to childhood abuse or neglect), or “polyvictimization,” has been shown to have an impact on both mental and physical health. It has been suggested that there is a direct relationship between the number of different types of negative experiences in childhood and the degree to which the individual’s health is impaired in adulthood.2,7,132 Individuals with a history of a greater number of victimizations also have increased odds of reporting multiple health problems, pain, poor self-rated health, disability, and utilization of health services in adulthood. 31
Quality of Life
The broad range of impacts of child maltreatment suggests that there may also be an impact on the life expectancy and the quality of life experienced by adult survivors of abuse and neglect. Surprisingly, little is known about life expectancy and perceived quality of life for individuals who experience childhood maltreatment. The limited work that has been done in this area shows that individuals with a history of maltreatment report poorer quality of life than those without, and this reduced quality of life translates to a significant loss in days per year of good health.7,32,133-136 Younger adults (ie, 19-39 years) with a history of maltreatment report the lowest perceived quality of life relative to other adults. 133 Thus, not only does abuse and neglect have an impact on physical and mental health but also on how individuals with a history of maltreatment perceive the “goodness” of the life they lead.
Challenges to Translating Research to Practice
While it is evident that there are significant negative physical and mental health outcomes as well as health risk behaviors related to childhood abuse and neglect, there are challenges in translating what is known into clinical practice for a variety of reasons. First, the medical literature often fails to include child maltreatment as an important predictor of adult health outcomes. 11 As a result, practitioners who rely on this literature are less likely to consider abuse and neglect when diagnosing and treating physical and mental health disorders in their patients.
Second, a disproportionate number of studies have focused on women and childhood sexual abuse. In an analysis of 24 studies assessing the effect of childhood abuse on medical outcomes in adults, the authors noted that only 6 studies included men, 92% focused on sexual abuse, and less than 25% included childhood neglect. 122 Thus, we have a better understanding of outcomes affecting a subset of the population rather than the population as a whole, and it remains unclear whether what is known can be generalized to the population at large.
Third, there is substantial variation in the definitions and terminology used in the field. For example, definitions of abuse and neglect are inconsistent across the many disciplines involved in presenting research on this topic. Other terms are also used inconsistently. For example, use of the term disorder is equivocal with some using clinical definitions and DSM criteria to define disorders and others using research definitions and/or symptomatology to define disorders. The lack of consistent definitions and terminology makes communication between professionals involved in helping children and adults who have experienced maltreatment difficult, and health professionals should be mindful of this when translating research into practice.
Finally, 2 omissions in the current body of work that have important ramifications for practice are the lack of focus on specific health outcomes in children and a lack of attention to factors that may buffer individuals from the long-term deleterious consequences of maltreatment. Additional work on outcomes for children is needed to identify developmental indicators of maltreatment that are amenable to modification and intervention. This can inform research, practice, and intervention efforts for adolescents and adults, which, in turn, will improve the health, well-being, and lifestyle choices of these individuals. Likewise, examining the factors that may attenuate, buffer, or protect individuals from deleterious outcomes related to abuse and neglect is needed. Focusing on developmental indicators and examining child development in general, and child maltreatment specifically, within a framework of factors that may buffer the effects of adversity can help the field to better understand the epidemiology of maltreatment and improve intervention and prevention efforts.
Implications for Practice
It is important for medical professionals to take an active role in the primary prevention of, and interventions for, maltreatment. This can be done through knowledge of the conditions and contexts that may put a child at risk for maltreatment, understanding the signs and symptoms of current abuse in children and adolescents, having knowledge of developmental indicators of maltreatment, and being willing to report abuse and neglect when it presents in a clinical setting. Reviews of the available research shows that population-based screening instruments to detect maltreatment are neither sufficiently sensitive nor adequately evaluated. As such, screening is not recommended. Instead, many professional medical organizations recommend that physicians be alert for signs and symptoms of both current (for children) and past victimization in the medical visit. 137 In adolescent and adult health care settings, it may be useful for physicians and other health care providers to inquire about maltreatment history when individuals present with health problems or symptoms that are consistent with a history of abuse. In cases where victimization is identified, it is important to provide appropriate care and referrals in order to improve health outcomes and lifestyle choices.
However, medical professionals do not carry the sole onus for intervening to prevent maltreatment. As noted earlier in this article and in other articles in this issue (see Haegerich and Dahlberg), primary prevention of maltreatment is fundamental to improving health outcomes for individuals, as well as attenuating or ameliorating burden at the population level. One of the 10 essential services identified for public health is research for new insights and innovative solutions to health problems. 138 CDC and other federal agencies are supporting child maltreatment prevention efforts from a protective framework in which essential aspects of childhood including enhancing safe, stable, and nurturing relationships between children and caregivers are the focus to reduce risk for abuse and neglect before it occurs. 139
There is a substantial body of knowledge on the factors and contexts that put children at risk for maltreatment, but much of this knowledge has not been effectively translated into prevention strategies that can be applied in an efficacious manner by providers. 140 Recent neurobiological work is providing new insights into brain architecture and chemical pathways to health that may offer translation opportunities for intervention and prevention efforts to improve health outcomes of individuals with a history of victimization.
In addition, Haegerich and Dahlberg (this issue) review common risk factors for violence and provide an overview of the primary prevention approach. Haegerich and Dahlberg also provide an overview of a number of primary prevention strategies for child maltreatment, including Chicago Child-Parent Center program, Triple P, Nurse Family Partnership, and The Period of PURPLE Crying (AHT prevention).
Two of the most common primary prevention strategies for child maltreatment are parent education or training and home visiting programs. Home visiting models are the most common approach to preventing child maltreatment before it occurs. As described by Reynolds and colleagues, a typical home visitation program involves a trained professional (eg, nurse) or paraprofessional visiting the homes of parents and providing some combination of parenting advice, health advice, and other services (eg, connecting families to social services). 141 In parent education or training programs, parents typically attend classes or support groups where they are presented with information on parenting practices often within the context of, or in addition to, information on child development. Research demonstrates that the most effective parent training programs offer opportunities for parents to practice new parenting skills with their own child in the parent training setting. 142
In a study to determine the efficacy of existing child maltreatment prevention programs, Reynolds et al 141 reviewed 14 current programs designed to prevent abuse and neglect before it occurred in families with children less than 5 years of age. Most programs used the home visiting model (10 programs). The remaining programs used parent education, either alone or in combination with other programs. The researchers found there was an average of a 31% reduction in the rate of maltreatment for the children involved in the primary prevention programs. The 2 most effective programs reviewed, Nurse–Family Partnership (home visiting model; described in more detail in Haegerich & Dahlberg, this issue) and Chicago Child–Parent Centers (enhanced parent education model; described in more detail in Haegerich & Dahlberg, this issue), shared several common elements: family support provided through a mentoring relationship or partnership, implementation by professional staff, and consistent implementation of core program features.143,144 Other intervention and prevention program research corroborates the importance of these program elements. 142
Summary
Child maltreatment is associated with a variety of negative physical and mental health outcomes that affect the individual throughout the lifespan and place a substantial burden on both victims and the population as a whole. Children and adults with a history of abuse and neglect are more likely to experience and report poorer physical health and manifest psychiatric symptomatology than those who have not experienced maltreatment. Furthermore, maltreated individuals are more likely to use the health care system and make unhealthy lifestyle choices than their nonvictimized peers. Primary prevention requires a collaborative effort by researchers, medical professionals, and state and federal agencies to improve research on effective prevention and intervention programs and educate medical professionals to recognize risk factors and early warning signs of maltreatment in children and youth and risk behaviors and health indicators of maltreatment in adults. Preventing maltreatment before it occurs can avoid victimization, and interventions once maltreatment has occurred have the potential to improve the health and well-being of victims.
Footnotes
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
*
The term parent includes custodial and noncustodial parents.
†
The terms maltreatment and abuse are often used interchangeably in the literature. However, in this article, maltreatment is a general term that includes both abuse and neglect; abuse refers explicitly to acts of commission, whereas neglect refers specifically to acts of omission.
‡
2008 is the most recent year for which statistics are available (US Department of Health and Human Services 4 ).