
Abstract
Background:
The personalized, heart rate-dependent computed tomography angiography (CTA) protocol can reduce the use of contrast medium (CM) and the radiation dose. This is especially beneficial for patients with CTA of coronary combined with pulmonary arteries.
Purpose:
To evaluate the feasibility of low CM in one-stop coronary and pulmonary arterial CTA tailored by patients’ heart rate.
Material and Methods:
94 patients set to undergo CTA of coronary combined with pulmonary arteries with one-stop scans. Patients were prospectively randomized into two groups: For group A (n = 47), the timing of the scans was determined according to the patient’s HR using 30 mL CM; For group B (n = 47), in which the routine bolus tracking was applied by setting the ascending aortic threshold of 80 HU with 70 mL CM, scans were performed simultaneously.
Results:
Compared with group B, group A had slightly higher computed tomography (CT) value and image quality of pulmonary artery (CT value: group A 484.7HU; group B 457.9HU; t = 2.446, P = .016; image quality: χ2 = 8.292, P = .016), but in coronary artery wasn’t statistically different between two groups(image quality: χ2 = 2.516, P = .642).
Conclusion:
The heart rate-dependent CM injection protocol can greatly reduce the use of CM, simplify the work-flow, and may obtain comparable or even better image quality compared with the routine bolus tracking.
Keywords
Introduction
Chest pain, shortness of breath, and syncope are common symptoms related to coronary heart disease.1-4 Other life-threatening diseases such as aortic dissection (AD) and pulmonary embolism (PE) may also cause chest pain and require immediate medical intervention.2,3,5,6 Indeed, PE is a potentially fatal disorder, and is the third most common acute cardiovascular disease worldwide after myocardial infarction and stroke. 7 Moreover, a missed diagnosis of PE can be fatal. 8 Unfortunately, PE-related clinical symptoms are often non-specific, and a timely correct diagnosis mainly relies on clinical imaging, including computed tomography angiography (CTA).9,10 Indeed, multislice computed tomography (CT) has been shown to reduce the time spent in the diagnosis of PE and it diminishes patient costs.11-13 However, CTA also has important shortcomings, including contrast agents and radiation exposure—contrast agents reportedly can be toxic to the kidneys.14,15 Therefore, reducing the contrast agent dosages has become an interesting and important study topic in the clinic. 16
By combining a low voltage setting and the iterative algorithm, it may be possible that a low volume of the contrast agent could be used for cardiovascular and the other vascular high-pitch scanning. 17 Revolution CT scanners with high speed and high maneuverability have a 16-cm wide detector for one-stop CTA of the coronary and pulmonary artery. Compared with the traditional triple rule-out protocol, the one-stop protocol is triggered manually tailored by patients’ heart rates, which greatly reduces the volume of contrast agent. At the same time, the images obtained are pure pulmonary artery and pure coronary artery in a single injection, avoiding the interference of venous imaging and obtaining higher quality image. 18 The aim of this study was to further evaluate the feasibility of administering a small volume (30 mL) of contrast agent (iopamidol-370) in one-stop coronary and pulmonary arterial computed tomography angiography (CTA) tailored by patients’ heart rates.
Methods
Demographic and Clinical Characteristics of the Patients
This study protocol was approved by the Ethics Committee of Liaocheng People’s Hospital. Written informed consent were obtained from all participants. A total of 94 patients with Chest pain, or/and shortness of breath, or/and syncope or/and Patients with suspected pulmonary embolism or/and coronary artery disease were enrolled. All patients with a body mass index (BMI) between 18 and 26 underwent CTA of coronary and pulmonary arteries with one-stop contrast agent injection. These patients were randomly divided into two groups (A and B) with different CT scanning protocols being performed in the patients of these two groups (see below). Group A included 18 males and 29 females, with a mean age of 59.06 ± 11.44 years (range:23–83 years). Group B consisted of 25 males and 22 females, with a mean age of 58.69 ±10.63 years (range: 31-81 years). The heart rate, heart rate during the scan, GFR, and BSA in Group A were 68.60±7.24 bpm, 67.51±10.89 bpm, 94.53 ± 6.32, 1.72 ± .16 m2, respectively. The heart rate, heart rate during the scan, GFR, and BSA in Group B were 70.34 ± 11.18 bpm, 68.43 ± 11.22 bpm, 94.28 ± 6.13, and 1.73 ± .15 m2, respectively. Risk factors include hypertension, diabetes, and smoking history, and the amount of Group A is 29, 9, and 11 and the amount of Group B is 32, 12, and 15, respectively.
Protocol for group A and B ECG-gating methods: For patients with a HR>80 beats per minute (bpm), HR = 60–80 bpm, underwent retrospective ECG-triggered spiral scan. HR <60 bpm, underwent prospective ECG-triggered axial scan. No drugs are used to interfere with heart rate changes before the CT scan.
Computed Tomography Examination
An American GE256 row, 512-slice spiral CT scanner was used for the patients’ examination. Scan parameters were X-ray tube rotation speed of .28s/r, tube voltage kV assist of 80–140 kV, baseline of 100kV, tube current SmartmA of 150–650 mA, and NI of 20. The detector covered 12–14 cm, 50% ASiR-V, with a conventional scanning thickness of .625 mm. The helical pitch is 1, Cardiac blood vessels related scanning parameters were: window width 800 HU and window location 180 HU. All images were transmitted to the workstation(AW461) through the PACS system.
Computed Tomography Scanning Protocols
Protocol for group A (one-stop protocol)
For patients in group A (n = 47), scanning was performed with an injection of 30 mL contrast agent and the scan timings were set according to the patients’ heart rates (HR) to determine the delay between the initiation of pulmonary artery CTA and the initiation of coronary CTA (ΔT). For patients with a HR>80 beats per minute (bpm), the pulmonary artery CTA scan started 5s after the injection of contrast material and the delay between the initiation of pulmonary artery CTA and initiation of coronary CTA were 6–8s. For patients with a HR = 60–80 bpm, the pulmonary artery CTA scan started 7s after the injection of contrast material and the delay between the initiation of pulmonary artery CTA and the initiation of coronary CTA was 9–11s. For patients with a HR <60 bpm, the pulmonary artery CTA scan started 9s after the injection of contrast material and the delay between the initiation of pulmonary artery CTA and the initiation of coronary CTA was 12–15s. A total of 30 mL contrast medium was used for each patient in group A. The whole scan was divided into two steps of scanning, that is, helical scans for the pulmonary artery CTA and axial scans for the coronary artery CTA. The contrast agent flow rate was 5 mL per second. Scan start timing is 17.48±3.14 s. Protocol for group A undergoing prospective ECG-triggered axial scan.
Protocol for group A underwent prospective ECG-triggered axial scan: For patients with a HR>80 beats per minute (bpm), we only acquire the systolic phase, HR = 60–80 bpm, acquire the both systolic and diastolic phase, HR <60 bpm, only acquire the diastolic phase. This scanning protocol can obtain pure pulmonary artery and pure coronary artery images in a single injection, avoiding the interference of venous imaging and obtaining higher quality image.
Protocol for Group B (Traditional CT Scan Protocol)
For patients in group B (n = 47), the routine bolus tracking technique was applied by setting the ascending aortic threshold of 80 HU with an injection of 70 mL contrast agents. Scanning of coronary and pulmonary arteries was performed simultaneously. The contrast agent flow rate was 5 mL per second. Scan start timing is 17.42±3.28 s. Protocol for group B undergoing retrospective ECG-triggered spiral scan.
Image Evaluation
The CT values of left anterior descending artery (LAD), left circumflex artery (LCX), right coronary artery (RCA) were measured. The image quality was evaluated by two experienced radiologists based on a 5-point Likert scale (1–un-assessable to 5–excellent): 1, failure in meeting the diagnosis; 2, poor image quality; 3, basically meeting the diagnosis; 4, good image quality; and 5, high image quality. The radiation dose and contrast agent volume were also recorded.
Statistical Analysis
All statistical analyses were performed using the SPSS v15.0 statistical software package (SPSS Inc., Chicago, IL.) Univariate analysis of variance was used to determine the differences in the CT values of LAD, LCX, and RCA between group A and B. Rank sum test was used to determine the difference of image quality between these two groups. A P-value less than .5 was considered statistically significant.
Results
Comparison of CT Values of Pulmonary Artery and Three Major Coronary Arteries between Group A and B
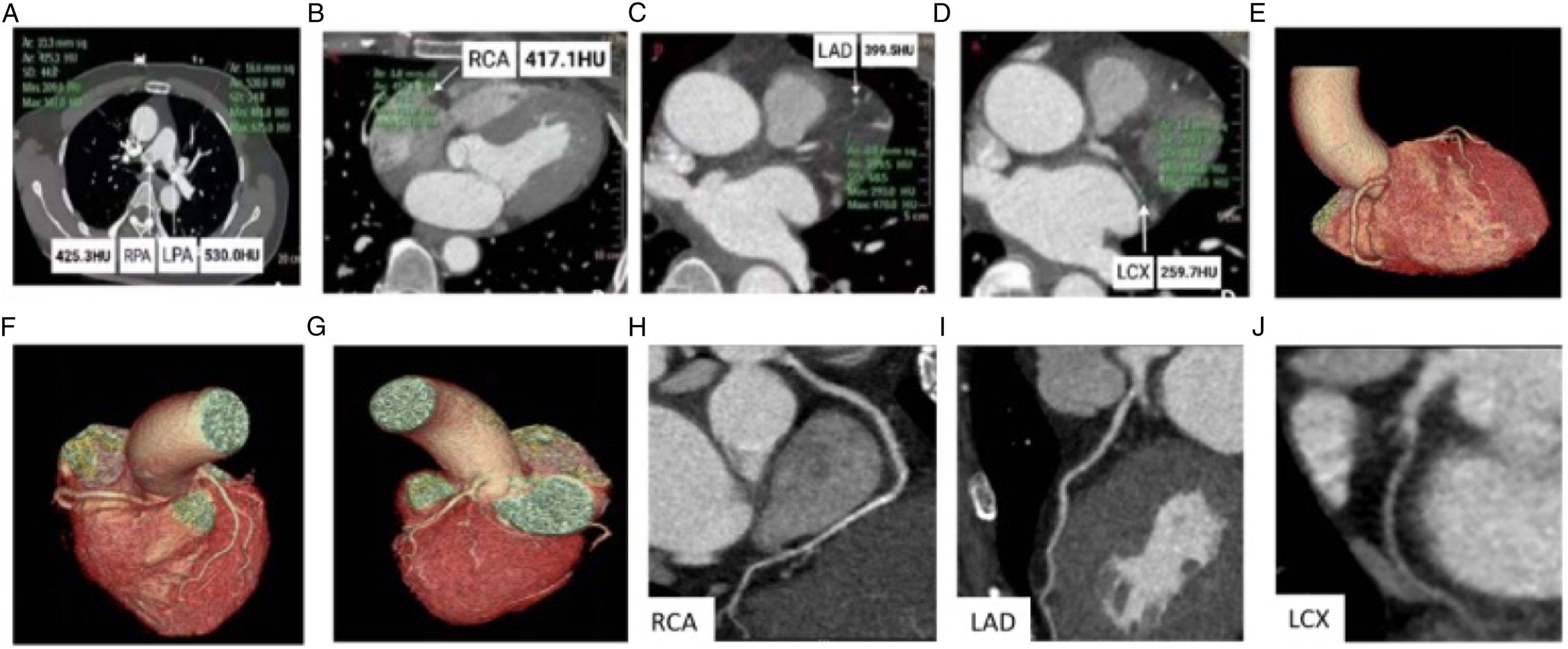
Figures 1A-1D and Figures 2A-2D show the representative images of CTA of coronary and pulmonary arteries. As shown in Table 1, the CT value of pulmonary artery in group A (484.7HU) was slightly but significantly higher than in group B (457.9HU) (t = 2.446, P = .016), while no significant differences in the CT values of LAD, LCX, or RCA were found between these two groups (P > .05). Thus, based on the CT scan timings defined according to patients’ HRs, a smaller amount of contrast agent (i.e., 30 mL) obtained a better CT value of pulmonary artery compared with the traditional tracking technique, which using 70 mL of contrast agent. Coronary and pulmonary artery CTA images of a patient receiving 30 mL of contrast medium. (A–D) The axial CT images of pulmonary artery, RCA, LAD, LCX, and associated CT values. (E–G) Three-dimensional volume-rendered reconstruction of coronary CTA. (H-J) Curved multiplanar reformatted view of RCA, LAD, and LCX. RCA: right coronary artery; LAD: left anterior descending artery; LCX: left circumflex artery. Coronary and pulmonary artery CTA images of a patient receiving 70 mL of contrast medium. (A–D) The axial CT images of pulmonary artery, RCA, LAD, LCX, and associated CT values. (E–G) Three-dimensional volume-rendered reconstruction of coronary CTA. (H-J) Curved multiplanar reformatted view of RCA, LAD, and LCX. RCA: right coronary artery; LAD: left anterior descending artery; LCX: left circumflex artery. Comparison of CT Values of Pulmonary Artery and Three Major Coronary Arteries between Group A and B. Abbreviations: LAD, Left anterior descending; LCX, left circumflex artery; RCA, Right coronary artery.

Comparison of Image Quality of Pulmonary Artery and Three Major Coronary Arteries between Group A and B
Comparison of Image Quality of Pulmonary Artery between Group A and B.

* 1, 2, 3, 4, and 5 represent the image grading level.
Comparison of Image Quality of Coronary Artery between Group A and B.

* 1, 2, 3, 4, and 5 represent the image grading level.
Radiation Dose in DLP and ED
The DLP and ED of group A are 217.05 ± 37.31 and 3.15 ± .54, respectively. The DLP and ED of group B are 230.31 ± 36.98 and 3.34 ± .54, respectively.
Discussion and Conclusion
In conclusion, in the present study, we have found that a smaller volume of contrast medium (30 mL of iopamidol 370) could still qualitatively enhance the CTA images of the pulmonary artery. With regard to the diagnostic performance and image quality of the HR-dependent contrast agent administration protocol, we reduced the amount of contrast agent used in the routine bolus tracking technique protocol (30 mL vs 70 mL) by more than 50% with no significant differences in the quality of images of three major coronary arteries obtained between these two protocols. Compared with traditional scanning protocol, HR-dependent contrast agent administration protocol has more advantages including obtaining pure pulmonary and coronary artery images.
Patient Characteristics, Radiation Dose, and Risk Factors in both Groups.

There are some limitations in our study. First, traditional pulmonary and coronary artery scanning takes place simultaneously, while our HR-dependent contrast medium injection protocol was axial scanning and included two scanning steps: pulmonary artery implemented spiral scanning, and coronary artery implemented axial scanning. Second, the HR-dependent protocol used a slightly higher radiation dosage than the traditional scanning. Third, we are failure to reduce the volume of contrast medium according to different body habitus.
The HR-dependent contrast medium injection protocol can greatly reduce the use of contrast medium without compromising of the image quality of major coronary arteries. Furthermore, it can simplify the work-flow and may obtain better CTA image quality of pulmonary artery compared with the traditional bolus tracking technique.
Footnotes
Authors' contributions
PJS contributed to the study conception and design. XML SHY, and HRY performed the Material preparation, data collection and analysis. XML was a major contributor in writing the manuscript. HW, ZG, GYC, and HS performed reconstruction images. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Jinan Clinical Medical Science and Technology Innovation Program Project [202019133]; the the Jinan Central Hospital’ s 2020 first-batch research fund for introducing talents [YJRC2020005]; the Jinan Government 5150 Project for Innovative Talents.
Abbreviations
Computed tomography angiography(CTA), computed tomography (CT), left anterior descending artery (LAD), left circumflex artery (LCX) and right coronary artery (RCA), body mass index (BMI), heart rates (HR), Hounsfield unit(HU).
Ethics approval and consent to participate
This study was approved by the Ethic Committee of Jinan Central Hospital. Written informed consent was obtained from all patients.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author (Peiji Song: