
Abstract
Coronary artery aneurysm is a relatively rare disorder that is usually discovered as a secondary finding in patients undergoing coronary artery angiography. Coronary artery fistulas are relatively more frequent than rare aneurysms and are often associated with other cardiac abnormalities. The etiology of aneurysms is mostly atherosclerotic, and they are less frequently associated with other acquired or congenital diseases, such as Kawasaki disease, connective tissue diseases, septic emboli, arteritis, and iatrogenic disease. We report a 70-year-old woman with a rare combination of a coronary artery aneurysm associated with a coronary artery fistula, which drained into the pulmonary artery. The diagnosis of our patient was made by selective coronary angiography and confirmed by computed tomography angiography. The patient was treated surgically because of the symptomatic course of the disease.
Keywords
Introduction
Coronary artery aneurysm is a rare disease of the coronary arteries. Coronary artery aneurysm is found in 0.3% to 5% of patients undergoing coronary artery angiography. 1 Atherosclerosis is the most common etiology of this condition, accounting for approximately 50% of cases. Less frequent causes of aneurysmal formation include Kawasaki disease (17%), infectious septic embolization (11%), connective tissue diseases such as Marfan’s syndrome (<10%), arteritis (<10%), and iatrogenic disease (rare). A congenital etiology is rare, and it is frequently associated with other cardiac abnormalities.2,3
Coronary artery fistulas are also a rare finding because they occur in only 0.002% of the general population. The etiology of fistulas can be congenital or acquired (traumatic, iatrogenic, and infectious). Fistulas can be isolated or associated with other congenital heart diseases. In some cases, a secondary rupture of a coronary artery aneurysm in the direction towards the right-sided heart chambers may occur, and this forms a left-to-right shunt. 1 These fistulas are usually present as single fistulas, and are less frequently found as multiple fistulas, often originating from both coronary arteries. 4
Coronary fistulas can cause myocardial ischemia owing to coronary blood steal or, rarely, congestive heart failure due to left-to-right shunting. 5 Coronary artery aneurysms may manifest as angina pectoris or acute coronary syndrome due to local thrombosis, distal embolization, or vasospasm. 6 There is also a risk of aneurysm rupture, leading to a range of typical consequences. 7 We report a case of a combination of two coronary artery aneurysms and a coronary artery fistula that drained into the pulmonary artery.
Case report
The reporting of this study conforms to the CARE guidelines. 8 A 70-year-old woman with no history of any cardiac disease was admitted to the local Department of Cardiology with chest pain. Upon admission, an electrocardiogram showed a discrete elevation of the ST segment in the lateral wall of the left ventricle (1 mm). Coronary angiography was immediately performed owing to the electrocardiographic findings and symptoms. During angiography, a saccular aneurysm 22 × 18 mm in diameter, which was connected to the left anterior descending artery by a narrow neck, was found. Tortuous aberrant vessels originated from this aneurysm. These vessels supplied another smaller aneurysm of 11 × 13 mm, which subsequently drained into the pulmonary artery. Another aberrant vessel, which originated from the ostial part of the right coronary artery, was found, and this terminated in the aneurysm. Coronary artery blood flow was not limited, and no coronary artery stenosis was found (Figures 1, 2). The chest pain subsided after administration of nitrates during angiography. Echocardiography showed normal kinetics of the left ventricle and no valvular malfunction.

Left coronary angiography shows two aneurysms. The cranial and smaller aneurysm is supplied by vessels that originate from the left and right coronary arteries.

Right coronary angiography shows an aberrant vessel, which terminates in the smaller aneurysm, and this is connected to the pulmonary artery.
To further examine the aneurysms, computed tomography coronary angiography with three-dimensional reconstruction was performed (Figure 3). The diagnosis of coronary artery aneurysms was confirmed, and an intra-aneurysmal adherent thrombus was found. The serum cardiac high-sensitivity troponin T level was not increased. Surgical treatment was performed because of the complexity of the findings. The patient underwent a cardiac surgical procedure using a heart-lung machine with cardiac arrest. The adhering thrombus was removed after the aneurysms had been opened (Figure 4). The aberrant supplying arteries were ligated and the fistula to the pulmonary artery was treated by a direct suture. The aneurysmal sacs were then sutured (Figure 5).
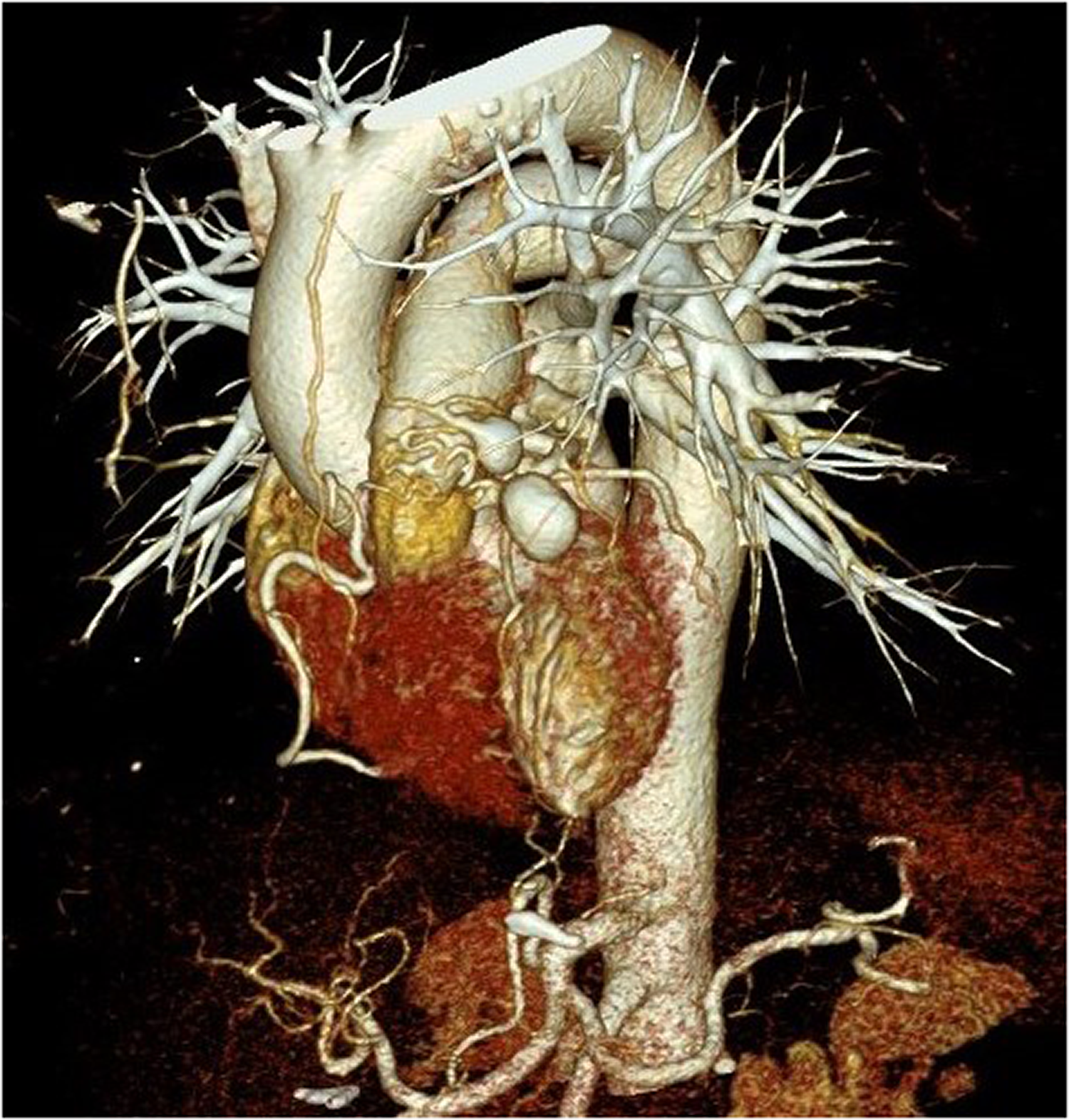
Three-dimensional reconstruction of computed tomography coronary angiography shows the position of both aneurysms and their supplying arteries.
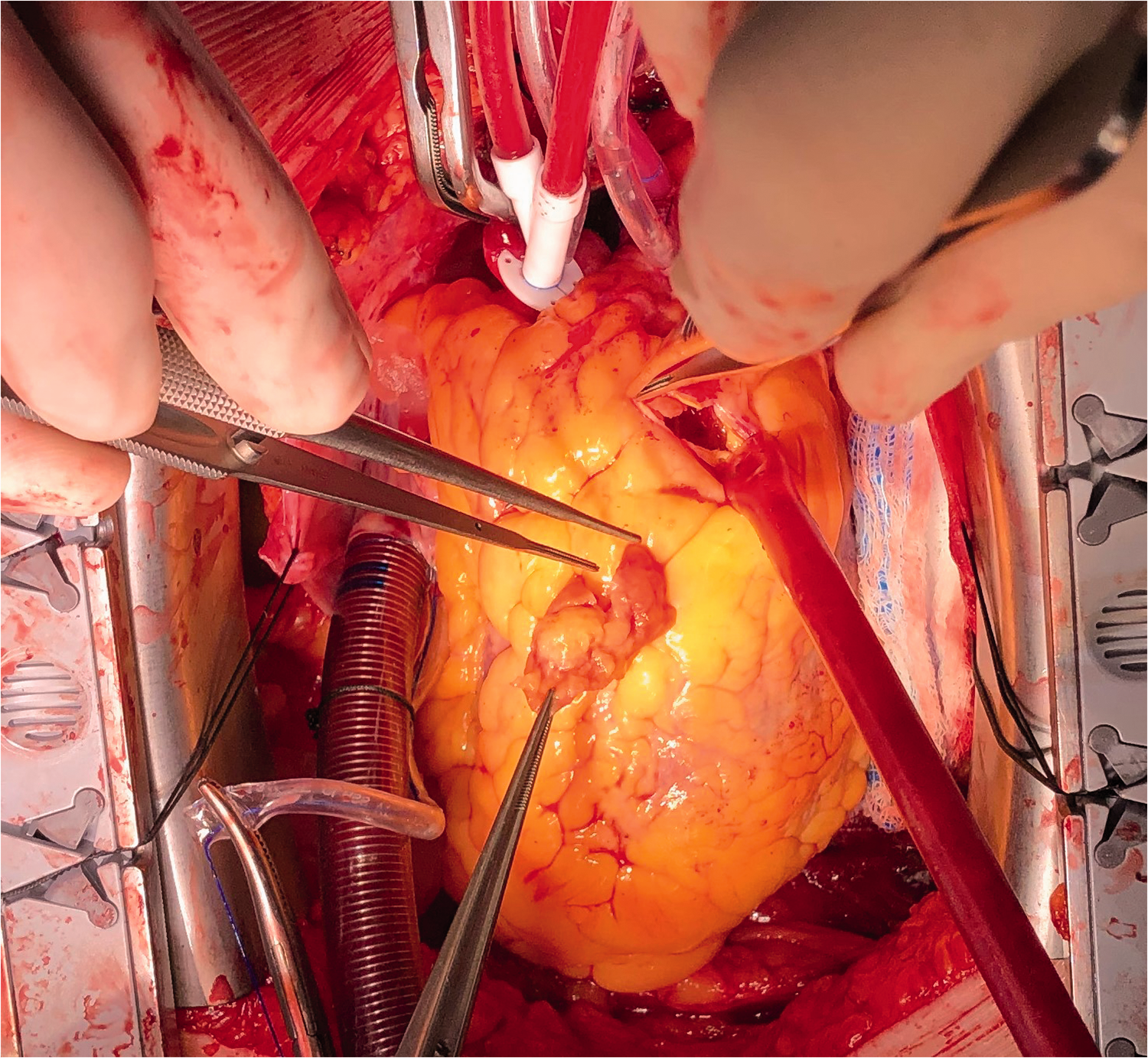
Perioperative photograph of removal of an adhering thrombus on a coronary artery aneurysm.

Perioperative photograph showing the opened aneurysms and fistula to the pulmonary artery (smaller aneurysm 2).
The histological findings in our case showed degenerative changes with fibrosis, thinning, and focal hemorrhage in the tunica muscularis. Fibrotic changes and atheromatic plaques with foamy histiocytes in the tunica intima were also found. Some of the plaques were calcified and partially dissected with fresh thrombus formation.
The intraoperative and postoperative periods were uneventful, and the patient was discharged from the hospital on the 11th postoperative day.
Discussion
Coronary artery aneurysm and coronary artery fistula are rare disorders. The course of both of these disorders can be asymptomatic. When symptoms are present, the most common manifestation is angina pectoris or myocardial infarction.1,2,9 Fatal complications, such as a rupture of the aneurysm with cardiac tamponade, can also occur. 10 In the present case, the patient’s symptoms resembled acute coronary syndrome with chest pain and a discrete elevation of the ST segment on electrocardiography. Formation of coronary artery aneurysms and fistulas have various pathways of origin. In most cases, the etiology of coronary artery aneurysm is atherosclerotic. Coronary artery aneurysm is rarely associated with other diseases, such as Kawasaki disease, infectious septic embolization, connective tissue diseases (e.g., Marfan’s syndrome), and arteritis. Coronary artery fistulas are usually congenital and associated with other congenital heart diseases. The histological findings in our case showed degenerative and fibrotic changes. An atherosclerotic etiology was finally confirmed. Matrix-degrading enzymes are likely to contribute to the development of coronary aneurysms, and therefore, they may represent a therapeutic strategy.2,11
The etiology of the coronary artery fistula was probably congenital in our case because it terminated in the aneurysm, which was positioned in front of the pulmonary artery. Surgical treatment was the preferred intervention in our case because of the complexity of the lesions. This case was interesting because of its complexity and well documented results. The incidence of a coronary artery aneurysm and coronary artery fistula is low. Therefore, our results will be useful for future cases because of our successful surgical treatment.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics statement
Approval of a study protocol was not required in our institution because this was a case report. The patient provided consent for publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was funded by the Czech Ministry of Health (grant number MZCZ – DRO – VFN64165). The article processing charge was funded by the Open Access Fund of the General University Hospital in Prague, Czech Republic.