
Abstract
Objectives
To highlight the detail obtained on a Cone Beam Computed Tomography (CBCT) scan of the craniocervical junction and its usefulness to Chiropractors who specialize in the upper cervical spine. A review of the dose considerations to patients vs radiography in a chiropractic clinical setting and to review the effective radiation dose to the patient.
Methods
A review of studies discussing cervical biomechanics, neurovascular structures, and abnormal radiographic findings, was discussed in relation to chiropractic clinical relevance. Further studies were evaluated demonstrating radiation dose to the patient from radiographs compared to CBCT.
Results
Incidental and abnormal findings of the craniocervical junction were shown to have superior visualization with CBCT compared to radiography. The radiation dose to the patient for similar imaging protocols to the craniocervical junction and cervical spine was equal or less utilizing CBCT when compared to radiographs.
Conclusions
The use of CBCT for visualization of the craniocervical junction and cervical spine in the chiropractic clinical setting allows for adjunctive visualization of the osseous structures which is germane to clinical protocol. Further with CBCT the effective dose to the patient is equal or less than similar imaging protocols utilizing radiographs to evaluate the craniocervical junction.
Keywords
Introduction and History of Cone Beam Computed Tomography
The clinical use of Cone Beam Computed Tomography (CBCT) in healthcare has grown steadily since the first commercial CBCT system was offered in the US in the 2001 timeframe. Initially, CBCT was utilized by dental specialists for acute conditions typically related to surgical procedures. The use of CBCT for routine diagnostic imaging is being explored within other healthcare specialties, such as chiropractic. 1
Since the early 1900s chiropractic doctors have used radiographic imaging of the spine to provide care to patients. Visualization of the spine has helped chiropractors assess contraindications to care and differentially diagnose patient with upper cervical conditions. Imaging has also been used to determine spinal positioning, which allows for the measurement of force vectors for the upper cervical specific chiropractic adjustment procedures. There are techniques within the profession in which imaging of the craniocervical junction (CCJ) heavily influences treatment protocols.
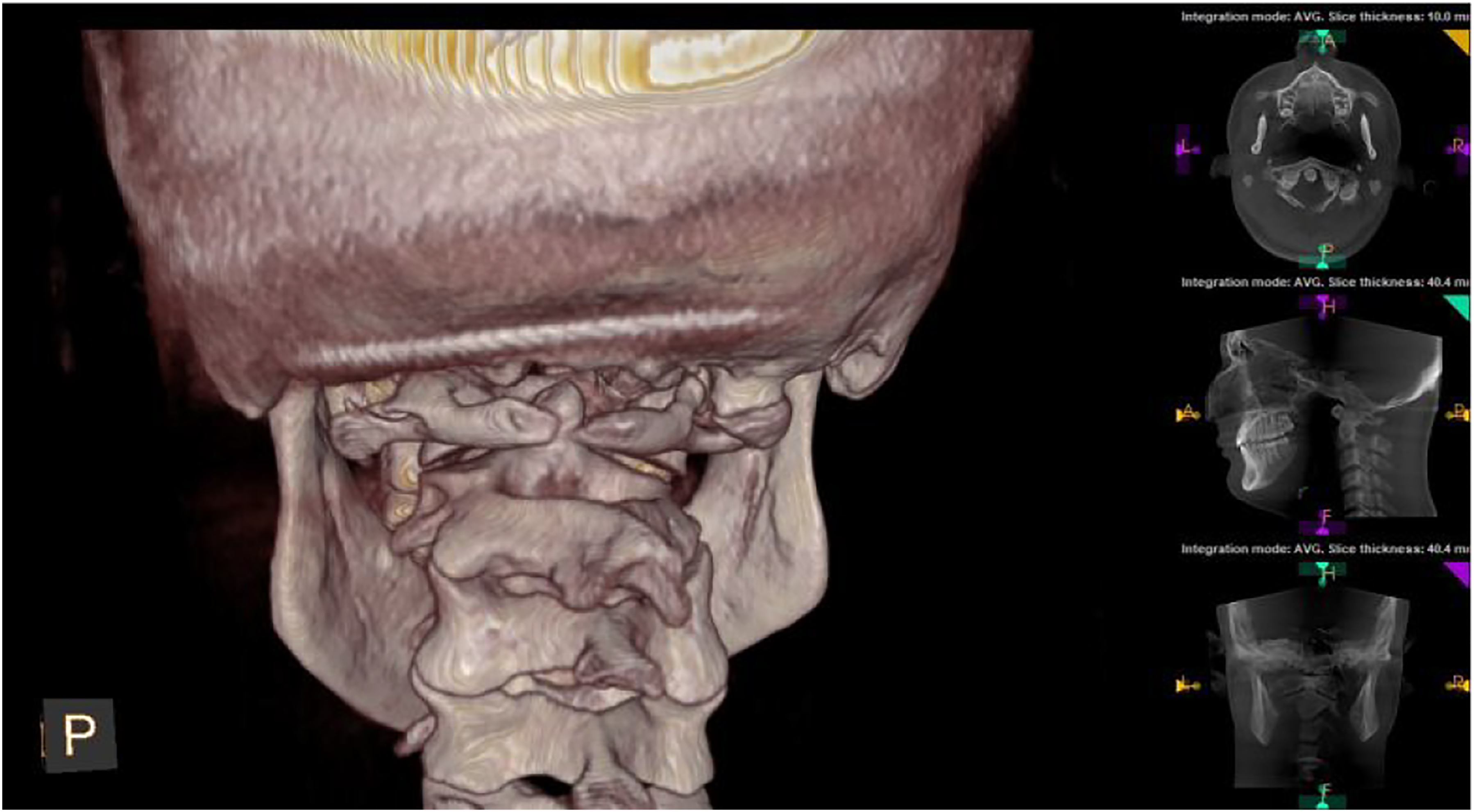
Chiropractic providers, utilizing various techniques, are now among the healthcare specialties utilizing CBCT. Within the chiropractic profession there exists a sub-specialty, called Upper Cervical Chiropractic (UCC) which concentrates on the craniocervical junction and how the structural integrity of the neck influences the nervous system, vascular system and cerebrospinal fluid flow in and out of the cranial vault.2,3 CBCT imaging offers a high quality imaging technique that minimizes radiation exposure to patients, and this type of imaging is of particular interest to UCC practitioners. Figure 1 demonstrates neutral lateral radiograph typical in an upper cervical chiropractic clinical setting. Figure 2 is the same person as Figure 1 with the 3-D rendering available with CBCT, allowing for appreciation of detail. Lateral cervical radiograph. Same person as Figure 1 showing increased visualization and large field-of-view.

Understanding the Biomechanics and Structure of the Craniocervical Junction (CCJ)
The craniovertebral junction (CVJ) or craniocervical junction (CCJ) are interchangeable and both terms refer to the Occiput (C0), Atlas (C1), and Axis (C2), and the supporting ligaments (Reddy et al, 2015). For the purpose of this paper, we will refer to the area as the craniocervical junction (CCJ). The Atlanto-occipital Joint (C0 on C1) and the Atlanto-axial joint (C1 on C2) are unique because they are diarthrodial, synovial pivot joints, with motion around hyaline cartilage surfaces. All vertebrae inferior to these 2 joints are fibrocartilaginous symphysis joints, classified as amphiarthroses and separated by discs.
The joints of the CCJ work together to allow for dynamic head and neck motion, while at the same time allowing the CNS to maintain its complex functions throughout the body (Reddy et al, 2015). The CCJ plays an important role in the overall motion of the cervical spine, accounting for 25% of the flexion and extension, and up to 50% of the axial rotation of the neck. 4 Although the CCJ consists of two distinct joints (atlanto-occipital and atlanto-axial), it functions as a single mobile unit, with the atlas acting like a washer between the cervical spine and the occiput. Each of these joints, however, has unique kinematic properties that contribute to the complex motion of the CCJ. 5
The CCJ is the most complex joint in the spine. 6 The complex nature of the structure and function of the craniocervical junction makes it particularly vulnerable to injury and deformation, as forces acting upon the head and cervical spine may occur in complex patterns. 3
The cervical spine exhibits complicated 3-dimensional movements according to Ref. [7], which could be adequately described using the 3-dimensional CT reconstruction method. Analysis of the reliability of 3-D CT reconstruction method showed very high inter-rater and intra-rater reliability, suggesting very good consistency. 7 Rotation at the upper cervical spine, specifically the occiput through C2, encompassed at least 60% of the total cervical rotation. Rotation at different parts of the cervical spine in the control group measured 69.7±5.5 for the total rotation of the cervical spine. The upper cervical spine contributes up to 63.13% of total rotation. The C1–C2 segment makes up 86.14% of the rotation of upper cervical spine and 54.40% of the total rotation of the cervical spine. 7
The CCJ protects the soft tissue contents within and around the upper cervical spine, including neurological and vascular tissue, while also allowing for significant mobility of the head and neck. 8 It is vital for UCC providers to consider how boney anatomy may influence structures in and around the CCJ. These structures, which may affect the nervous system can be influenced by abnormal biomechanics and fixations of the CCJ.6,9 A distorted axis of motion may create pathologic neurophysiologic changes to the specialized and sensitive neurology located at the skull base, such as changes to the suboccipital muscles. The suboccipital muscles have the highest density of proprioceptors per gram of muscle tissue compared to the rest of the body, 10 and therefore are important pain generators among patients with neck pain and headache.
Osseous malformations, misalignment, and traumas which contribute to aberrant CCJ biomechanics may alter cerebrospinal fluid and blood flow, thus resulting in altered hydrodynamics between the cranium and spinal cord. Misalignments, malformation, and anomalies of the CCJ have been shown to obstruct flow through the vertebral arteries.3,6,9 According to Ref. [9], the hydrodynamics of arteries, veins, and cerebrospinal fluid influence the pressure gradients that occur within an essentially closed cranial vault that has little room for expansion. This potential “choke point” at the CCJ for fluid flow may play a role in neurodegenerative disorders and conditions affecting brain health.3,6,9
Given the significance of the CCJ area, it has been notably absent from textbooks because the area is “in between” standard skull imaging and cervical spine imaging. 11 This area of the spine is poorly understood and is open to a potential of a multitude of misdiagnoses. For the most complete assessment, the CCJ should be visualized separately from the cranium and the cervical spine (Offiah and Day, 2017).
Difference in the Detail: CBCT versus Conventional Radiographic Imaging
According to Ref. [12], one third of reported traumas in the cervical spine occur at the CCJ. The CCJ may be closely correlated to brain health with consideration to concussion and post-concussion syndrome. Linear acceleration measurements causing concussive forces have been measured with head impact telemetry systems in high school and college football players, with the highest predictive value at 96.1 g (gravity). 13 Biomechanical studies for whiplash associated disorders reveal as little as 4.5 g of neck accelerate can cause mild strain injury to the soft tissue of the cervical spine.13,14 The prevalence of injury to the CCJ area can affect the osseous alignment resulting in neurologic and vascular implications that warrant increased clinical consideration, including detailed imaging.
The detail of boney anatomy provided by a CBCT image of the CCJ is useful to appreciate the components of the CCJ and its role in cervical spine stability and clinical implications. 12 The craniocervical junction is an area of unique consideration given bone morphology, biomechanics, ligamentous structures, fluid dynamics, neurology, and neurophysiologic effects attributed to that area.
The use of CBCT for chiropractic clinical imaging of the cervical spine and craniocervical junction has shown to provide a more diagnostic image as related to structure, due to its detailed capture characteristics as compared to traditional 2-D radiography. 15 CBCT allows for a 3-dimensional visualization leading to the identification of structural anomalies, vertebral misalignments, and often times results in a lower patient absorbed dose when compared to traditional 2-D radiography.15,16 Therefore, utilizing CBCT in an upper cervical chiropractic clinical setting would follow the principle of ALARA “as low as reasonably acceptable” that guides radiographic procedures for patients.
Identifying normal, abnormal, incidental, and anomalous findings on diagnostic imaging is paramount for specific manual therapy techniques, like UCC. Additionally, CBCT may be indicated to evaluate for traumatic fractures and hairline fractures within the cervical spine. It may also be used to evaluate cervical spine spondylosis, intervertebral foraminal stenosis, and facet joint arthrosis. These abnormal findings are regularly evaluated for in chiropractic offices that specialize in the craniocervical junction. One study reported that out of 427 CBCT scans performed for orthodontic evaluations, 356 of those scans had 842 separate findings that were not relevant to orthodontic work in the boney anatomy visualized. 17 While these finding were not relevant to orthodontic work, they may be relevant to chiropractic or medical treatment of the CCJ.
A retrospective study of CBCT scans by Ref. [18] found that 47.8% of all incidental findings pertained to the cervical vertebrae. This highlights the significant presence of anatomical variation in the CCJ. Incidental findings of the craniocervical junction that may influence both clinical diagnosis and application of treatment include fusions, flattening of joint surfaces, osteoarthritis, rotation, bony ossicles, single and bilateral posterior ponticus, non-union of posterior arch, elongated styloid processes, and asymmetrical mastoid processes. 18
Posterior ponticuli are the most commonly noted on CBCT scans within 26.2% of the population, 19 and has been associated with symptoms such as neck pain, headaches, shoulder and arm pain, that are otherwise unexplainable. 20 Future investigation is needed to clarify the clinical impact for the patient of posterior ponticuli; however, noting calcification of the posterior atlanto-occipital ligament in the upper cervical spine informs the clinical picture for the provider and may influence the force vectors or contact point chosen for treatment by the UCC chiropractor with each patient.
The goal of the study by Ref. [21] was to define the presence and prevalence of incidental findings in and around the base of skull from large field-of-view CBCT of the maxillofacial region and to determine their clinical importance. In this retrospective study, 400 large fields of view CBCT scans from January 1, 2007, to January 1, 2014, were reviewed with findings categorized into cervical vertebrae, intracranial, soft tissue, airway, carotid artery, lymph node, and skull base findings. 21 A total of 653 incidental findings were identified in 309 of the 400 CBCT scans. 21 Incidental findings of the cervical vertebrae made up 20.06% of the findings. Skull base incidental findings made up .15% of the findings. 31.24% of the findings required referral, and 17.76% required monitoring. If the provider determines that imaging is necessary, Ref. [21] concluded that a review of CBCT images surrounding the region of interest, specifically the base of skull, cervical vertebrae, pharyngeal airway, and soft tissue, would be warranted.
Ref. [22] found that a review of 7689 CBCT reports revealed 732 incidental findings, of which 9.5% occurred in the cervical spine or the clivus. Cervical spine findings made up 92.3% of those findings, and 78.7% were degenerative in nature, primarily occurring in females over 60 years of age. A more comprehensive analysis of the data showed that the odds of presenting with a degenerative incidental finding in the cervical spine or the clivus was 5.5 times higher in patients 50 years of age or older. 22
It is important to note that the incidental findings vary in significance. Given the large range of incidental findings in the cervical spine as well as the complex boney and soft tissue considerations, it is ideal that upper cervical chiropractors, who are applying directed forces into the CCJ, have the most detailed visualization with the lowest risk to patients possible. Figure 3 and 4 demonstrate the difference in appreciating incidental findings with 2-D compared to a 3-D rendering of the same patient. Radiograph view showing malformation of the CCJ: Agenesis of the posterior arch of C1, Right accessory articulation of C1 transverse process and skull, Left posterior ponticus. Identical patient as Figure 3 demonstrating increased visualization of CCJ malformation utilizing CBCT.
Radiation Dose Rate: Planmeca CBCT versus Conventional Radiographic Imaging
Effective doses attained using Planmeca VISO CBCT scanner using (skull 30 × 30 cm FOV protocol) for different patient sizes (XS, S, M, L, XL), voxel sizes (300, 450, 600 μm) and using ultra low dose (ULD) protocol.

Ref. [23] document the effective doses for AP and lateral cervical radiographs to be 120 μSv (.12 mSv). Ref. [24] found the effective dose for AP and lateral cervical spine films at 50 μSv and 30 μSv (.05 mSv, .03 mSv), respectively. It is important to note that UCC practitioners take multiple images when utilizing plain film radiographs, both as follow up and to obtain the necessary detail needed for treatment. A common five image series taken in the Upper Cervical Chiropractic protocol would have a total dose of 200 μSv or .20 mSv. 2 This is in comparison to the 41 μSv dose from Planmeca CBCT imaging. The views needed for “legal” set of films include two views, at right angles to each other. Ofori’s study did not include imaging of the skull (2014). CBCT effective dose for the head and cervical spine was 50-250 μSv (.05–.25 mSv). As a point of reference, annual background radiation dose for the average citizen of the U.S.A. is 3100 μSv (3.1 mSv) and average daily background radiation dose is 17.8 μSv (.0178 mSv) 25 ; August 06). Retrieved from https://www.epa.gov/radiation/radiation-sources-and-doses).
According to Ref. [26], the typical radiation exposure of common x-rays consisting of AP and lateral views of the cervical spine is 200 μSv or .2 mSv.
In a study by Ref. [16], it was found that the dose distribution can be inconsistent for dental CBCT exposures of a homogeneous phantom. This can be attributed to asymmetrical positioning and/or partial rotation of the X-ray source. This study revealed that the scatter tail along the z-axis was found to have a defined shape, generally resulting in a 90% drop in absorbed dose outside the primary beam. 16
The CBCT study by Ref. [15] measured dose-area product to calculate effective dose. Dose-area product values from 90 patient examinations allowed for estimation of effective dose, which was estimated for three diagnostic tasks. Tasks included examinations of impacted lower third molars and retained upper cuspids and implant planning of the posterior mandible. Results varied between 11 and 77 μSv.
The paper by Casselman states the following: “These non-dental CBCT studies gradually replaced conventional X-rays and CT/MDCT studies because they allowed imaging with higher resolution, lower radiation dose and less metal artifacts. In this paper the most important non-dental CBCT indications will be discussed” (Casselman et al, 2013, pg. 333). Among the areas discussed were imaging of the temporal bone, skull base, and vertex. Casselman maintains that the images only need to show bone, which is why they can be taken utilizing CBCT with its low dose and high resolution.
To evaluate scoliosis, the standard radiographic examination as set forth by the CLEAR Board of Advisors consists of (in part) the following: Five Cervical Spine x-rays (Lateral Cervical Neutral, Lateral Cervical Flexion, Lateral Cervical Extension, A-P Open Mouth, and Base Posterior) are taken, totaling 90 μSv (.09 mSv). Two additional cervical spine x-rays (APOM and a stress x-ray) may need to be taken depending on the individual patient necessity and the clinical decision-making of the healthcare provider to evaluate the effect of the treatment, adding an additional 40 μSv (.04 mSv). 27 Therefore, cervical spine total dose is the initial 90 μSv in addition to 40 μSv for the additional views, totaling 130 μSv. Again, these values are compared to Planmeca’s CBCT ultra low dose of a large skull of 41 μSv.
According to Ref. [28], cervical spine plain film radiography measurements of the effective dose for children less than 1 year of age through 15 years of age ranged from 20 to 100 μSv (.02–.10 mSv) and the effective dose for adults averaged 80 μSv (.08 mSv).
From Ref. [29], the dose rate to the skull from plain film radiography is shown to be 30 μSv (.03 mSv) for the AP view and 10 μSv (.01 mSV) for the lateral view, for a total dose rate of 40 μSv. These dose rates are very similar to CBCT dose rates, but do not show the detail of CBCT.
In the upper cervical chiropractic clinical practice, imaging of the craniocervical junction, when indicated, is a vital aspect of the protocol. The above studies report a sampling of patient dose factors that highlight the overall reduced risk to the patient when CBCT is used to visualize the CCJ.
Discussion
Modern CBCT uses a conical beam of pulsed x-radiation that is directed 90° to a Flat Panel Detector (FPD). The beam and FPD move in tandem, spinning in varying degrees (180 to 540, depending on image requirements) around the region to be imaged. Great advancements have been made in recent years to both the reconstruction algorithms and the FPD to increase image detection while decreasing patient radiation exposure.30–32
Current literature on the effective dose utilizing CBCT to evaluate the craniocervical junction is limited. Extrapolations were made utilizing dental cranial scans as a close comparison. This is a unique publication in its mention of CBCT as a method for evaluation of the craniocervical junction for chiropractic clinical practice. Additional limitations include a lack of literature on the current trends of use of CBCT in chiropractic clinical settings. More research is needed to gain full understanding of the scope use for CBCT by chiropractors.33-36
The authors are not suggesting that traditional 2-dimensional radiographs of the cervical spine are insufficient for evaluation of the cervical spine. Attention should be given to current technologies available with reported x-radiation effective dose that approximates or is less than conventional methods of imaging, with additional benefit of three dimensional visualizations. These three dimensional images can deliver greater detail and may enhance diagnosis and treatment considerations in a chiropractic clinical setting.37-40
Conclusion
The craniocervical junction is a complex anatomical,41,42 kinematic and neurophysiologic region of human anatomy which is often under-reported with current imaging modalities. Additionally, it is an area of increased osseous malformation and significant clinical consideration with respect to trauma of the head and neck. Visualization of the CCJ with Cone Beam Computed Tomography offers an option for detailed osseous assessment of this region readily accessible in a private chiropractic clinical setting, with equal to or lesser effective dose to the patient.43-47
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.