
Abstract
There is substantial evidence for normal relationships between spine and postural parameters, as measured from radiographs of standing patients. Sagittal balance, cervical lordosis, thoracic kyphosis, lumbar lordosis, pelvic tilt, and the more complex understanding of the interrelations between these essential components of normal stance have evolved to where there are known, established thresholds for normalcy. These spinal parameters are reliably measured from X-ray images and serve as goals of care in the treatment of spine and postural disorders. Initial and follow-up spinal imaging by X-ray is thus crucial for the practice of contemporary and evidence-based structural rehabilitation. Recent studies have demonstrated that improvement in the spine and posture by nonsurgical methods offers superior long-term patient outcomes versus conventional methods that only temporarily treat pain/dysfunction. Low-dose radiation from repeated X-ray imaging in treating subluxated patients is substantially below the known threshold for harm and is within background radiation exposures. Since alternative imaging methods are not clinically practical at this time, plain radiography remains the standard for spinal imaging. It is safe when used in a repeated fashion for quantifying pre–post spine and postural subluxation and deformity patterns in the practice of structural correction methods by chiropractic and other manual medicine practices.
Normal Spine Alignment as a Desirable Treatment Outcome
A normal spine alignment and sagittal balance is critical for optimal biomechanical function. 1 -12 Although some have questioned an ideal spine configuration, 13 these views are antiquated and unscientific. 12 A plethora of biomechanical literature substantiates that an optimal spine configuration is critical for normal activities of daily living, optimal sport performance, optimal lifting, and injury prevention and is associated with a higher quality of life. 14 -20
An ideal biomechanical alignment is also apparent from evolutionary considerations (lumbar lordosis essential for bipedal gait 21 ), anatomical considerations (ie, the backward wedging of the discs create the cervical and lumbar lordosis 9 ; the forward wedging of the vertebra create the thoracic and sacral kyphosis 9 ; the orientation of the facet joints 9 and sagittal spine alignment determines spinal coupling patterns 22,23 ; the essentiality of sagittal balance 4,24,25 ), the biomechanical considerations of spine load-bearing capabilities, 9,26,27 and injury mechanisms. 9,26 -30 For these reasons, an ideal spine alignment is the outcome goal for those who treat and correct spine deformity (subluxation), including specifically spine surgeons, as well as specialty-trained chiropractors and physiotherapists (Figures 1 and 2). 31 -36

Left: The Harrison normal spine model as the path of the posterior longitudinal ligament. Right: Harrison posterior tangent method used to quantify subluxation patterns (Courtesy Chiropractic BioPhysics® (CBP®) seminars). 35

Sagittal full-spine radiographs demonstrating a before and after of a geriatric patient (red line) treated by Chiropractic BioPhysics protocol resulting in dramatic spine and posture improvements toward the ideal spinal configuration that represents the Harrison full-spine normal model (green line) (Image courtesy of Dr J. Haas, Windsor, Colorado).
Posture and Spine Subluxation as the Source of Pathology
While normal spine morphology is essential for normal function, abnormal alignment referred to as spine deformity (surgical literature) or subluxation (chiropractic) results in compensation/adaptation and, over time, dysfunction and named pathology. In the transition from normal alignment to abnormal alignment, critical thresholds of essential spinal parameters get surpassed by either acute traumatic spinal injury events (ie, motor vehicle collision, lifting injury, fall, etc) or chronic repetitive or sustained strain injuries (ie, habitual sitting, habitual bending, habitual slouching, etc). In this process, it is the devolution of the spine from working physiologically to pathologically.
There are 6 main types of spinal subluxation patterns and each type has deleterious effects on the related spinal tissues. 37 For example, thoracic hyperkyphosis (posterior translation of thorax over pelvis) is associated with diverse symptoms and early death. 38 -44 Scoliosis (slow-loading buckling) is also associated with various symptoms including back pains, osteoarthritis, and also early demise. 45,46 Lumbar spine spondylolisthesis (ligament instability featuring a single vertebra shifting/sliding beyond normal limits) is a definitive source of back pain and sciatica often warranting surgery. 47 Lumbar spine hypolordosis is a definitive source of back pain. 48,49 Atlantoaxial rotatory fixation (segmental subluxation) is associated with upper neck and/or neurological symptoms. 50,51 Cervical kyphosis (snap-through forward buckling of neck) is associated with craniocervical and neurological symptoms. 32 -34
It is pointed out that any postural subluxation pattern will change the biomechanical loading onto the spine 9,26,27,52,53 such that Wolff’s Law will dictate a remodeling of the architecture of the bone over time. 54 -56 Thus, the long-term consequences of spinal deformity or subluxation is spinal osteoarthritis and degenerative disc disease. 57 -65 Further, it is a logical premise that if posture deteriorates over time, then the earliest recognition should warrant consideration for its correction. This would change the otherwise untoward trajectory of postural deterioration coupled with the degenerative spine tissue cascade, which would evolve over several years.
The Correction of Spine and Posture in Chiropractic and Manual Medicine
There have been several chiropractic and manual physiotherapeutic methods that have achieved the status of having positive randomized clinical controlled trials (RCT) evidence showing that definitive spine and posture structural improvements can be made for various subluxation patterns. Randomized clinical controlled trial evidence shows efficacy for nonsurgical methods to reduce scoliosis curves, 66 -68 reduce thoracic hyperkyphosis, 17,69,70 reduce anterior head translation, 71 -78 increase cervical lordosis, 71 -78 and increase lumbar lordosis. 79 -81 Further, these postural improvements have been shown to correlate with improvements in various patient outcomes, including pain, disability, quality of life, range of motion, and specific physiological measures including improved neurological central conduction times, which is a measure of the ability of the brain to communicate with the body.
Several recent RCTs have shown that physiotherapy scoliosis-specific exercise (PSSE) programs lead to larger reductions in spinal curve measures versus generalized (nonspecific) exercise programs in the treatment of adolescent idiopathic scoliosis. 66 -68 Since scoliosis of the spine may present in several different patterns, radiographic assessment is critical to prescribe curve-specific corrective exercise programs such as the popular “Schroth method” that has proven to reduce spine curvature. Comparison control groups receiving generic physiotherapy exercises, not specific to the patient’s presenting curve pattern, do show patient improvements, albeit significantly less than PSSE groups.
The reduction in thoracic hyperkyphosis has also been documented in several RCTs. 17,69,70 Radiographic assessment is critical to determine whether there are thoracic vertebral compression fractures which will limit the correction potential. Although the first 2 RCTs 69,70 demonstrate a modest correction (∼3° Cobb angle), a recent trial 17 has shown that more intensive corrective procedures (Schroth methods for hyperkyphosis) are superior (∼9° Cobb angle) to antigravity exercises. Either are superior to no correction from conventional physiotherapy methods.
Importantly, there seems to be an emerging trend in the literature. Methods shown to provide structural correction to the spine and posture for various spinal ailments are proving to provide long-term relief versus “cookie-cutter” treatments that help with temporary pain relief only. In several RCTs, 71 -81 the Moustafa group has demonstrated that only short-term relief is experienced by patients receiving traditional physiotherapy treatments for various craniocervical and lumbosacral disorders, where the trend for regression of symptoms occurs after the cessation of treatment (Figures 3 and 4). Alternatively, in the experimental treatment arms of these trials, patients receiving the same treatment plus spine correcting methods—Chiropractic BioPhysics extension traction to improve the natural lordotic spine alignment for the cervical (Figure 3) or lumbar spinal (Figure 4) areas—show lasting relief of symptoms persisting well beyond the cessation of treatment (3 months to 2 years). 71 -81 These trials also show similar trends in many of the measured neurophysiologic parameters including pain intensity, disability, quality of life, dizziness, headache index, head repositioning accuracy, central somatosensory conduction time, H-reflex, and flexion–extension kinematics.

Spine-specific treatment shows better long-term symptom relief versus non-spine-specific conventional treatments. Data reported for the improvement in cervical lordosis and are weighted average from 4 randomized clinical controlled trials (RCTs). 72,74,75,77 Note: Red line = conventional treatments (n = 166); blue line = conventional treatments plus extension traction to improve cervical lordosis (n = 166). Y-axis = pain intensity (0 = no pain; 10 = worst pain ever).
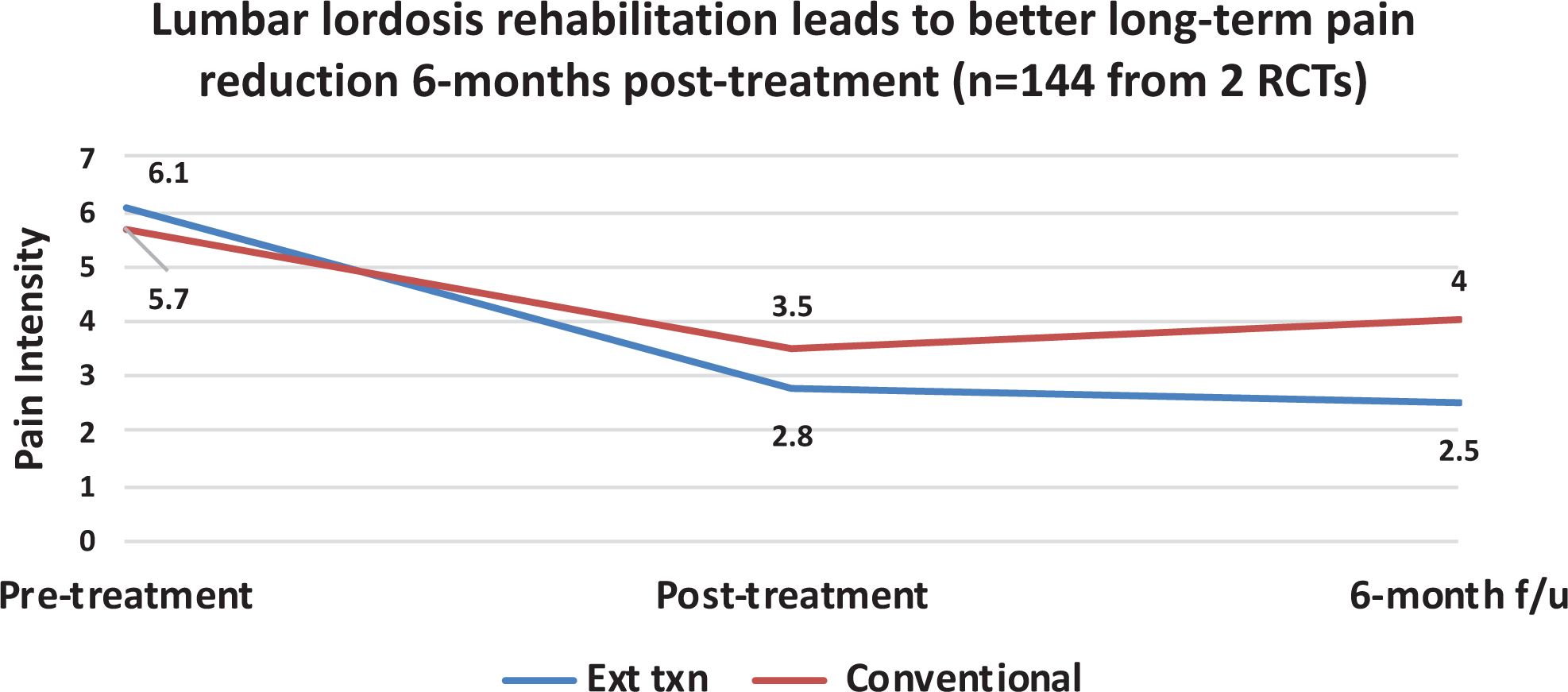
Spine-specific treatment shows better long-term symptom relief versus non-spine-specific conventional treatments. Data reported for the improvement in lumbar lordosis and are weighted average from 2 randomized clinical controlled trials (RCTs). 80,81 Note: Red line = conventional treatments (n = 72); blue line = conventional treatments plus extension traction to improve lumbar lordosis (n = 72). Y-axis = pain intensity (0 = no pain; 10 = worst pain ever).
Due to the recent and expanding evidence base for nonsurgical structural spine and posture correction methods, these protocols are expected to gain traction and become more popular. These contemporary methods should prove to help humanity by reducing the need for risky surgical procedures that are often associated with adverse events including major complications, hospital readmissions, and unplanned reoperations. 82
Safety of Low-Dose Radiation From Repeated Radiographs
Despite the traditional notion of the risk of radiogenic cancers associated with medical X-rays, the lack of harm from (low-dose) computed tomography scans and radiography has been thoroughly discussed in several recent articles. 83 -89 It has been argued that the linear no-threshold (LNT) assumption for assessing radiation risk for low-dose exposures is erroneous as the most recent atomic bomb lifespan study data 90 show a better fit to a hormetic dose–response model. 91 -93
Despite the fact that the main data underpinning the LNT concept have now been shown to better support the hormesis model (nonlinearity), there continues to be an acknowledged discount by those who downplay the concept of hormesis in defense of LNT ideology. Specifically, in discouraging the routine use of X-rays in clinical practice, for example, Kawchuk et al state: “While knowledge in topics such as radiation exposure modeling and radiation hormesis continually evolve, there are no large-scale studies that would justify the application of this principle in clinical practice today. To suggest otherwise at this time is professionally irresponsible.” 94 Ironically, the use of radiation hormesis (“radiotherapy”) in the treatment of human ills is not a new concept but has great historical evidence and documentation.
Throughout the early 20th century, many human diseases were treated by X-rays. This includes arthritis, 95 bronchial asthma, 96 carbuncles, 97 cervical adenitis, 98 deafness, 98 furuncles, 97 gas gangrene, 99 necrotizing fasciitis, 100 otitis media, 98 pertussis, 101 pneumonia, 102 sinus infection, 103 and tendonitis/bursitis. 104 In a recent summary of radiotherapy treatment by X-rays, 105 it was determined that success rates typically ranged from 75% to 90% from exposures that typically ranged from 30 to 100 roentgen (263-877 mSv). It was also noted that often the symptoms would be mitigated after only a single treatment and would occur within 24 hours; the treatment effect would even last for months to years. 105 Radiotherapy was a very effective treatment but lost popularity due to the emergence of pharmaceuticals and the fears from radiation following the atomic bombings during WWII. It should be noted that radiotherapy (whether given by X-rays or radon) is quietly making a resurgence in the literature; recent cases have documented successful treatment for those suffering from cancers (prostate, colon, uterine, lung, and liver cell), ulcerative colitis, rheumatoid arthritis, pemphigus, diabetes types I and II, Alzheimer disease, and Parkinson disease. 106 -110
It should be noted that there were no studies found documenting increased cancers from those treated for various health ailments from radiotherapy treatment. There are studies, however, that demonstrate that doses in the range of what was experienced by radiotherapy patients show less cancer rates. For example, in reanalyzing the Canadian breast fluoroscopy study data, 111 Cuttler and Pollycove showed that females treated for tuberculosis to up to 300 mGy had one-third less breast cancer incidence. 112 Further, Tubiana et al 113 determined the cancer incidence for secondary malignant neoplasms in those who have been treated by high-dose radiation for cancers in childhood. The findings indicated that those who received doses up to 0.5 Gy (500 mGy) had less cancers than expected. 113 The question is how can those receiving doses (much higher than X-rays) experience health improvements if LNT modeling tells us that radiation exposures are cumulative and harmful?
The answer is that it has been shown that the collective dose concept that is consistent with the prevailing LNT ideology for risk assessment is not valid for low-dose exposures since the body’s adaptive response mechanisms lead to repair of any damage caused. 114 In fact, there are numerous and redundant tissue-inherent protective mechanisms that prevent, repair, or remove damage (Table 1). 115 -118 Ironically, the most damage induced on a daily basis is metabolically produced reactive oxygen species (ROS) and H2O2 from aerobic respiration, and this damage is many orders of magnitude larger than any induced from low-dose radiation exposures. 115 -117 Due to this fact, X-rays are rendered negligible. 89
Body’s Multiple Adaptive Response Mechanisms That Prevent, Repair, and Remove Damage Caused From Mostly Endogenous Reactive Oxygen Species and H2O2 From Aerobic Metabolism. 118

As recently discussed by Oakley et al, the only consideration about repeated radiographs given to spine patients is the radiation dose they receive during each radiograph, not the sum of all the X-ray doses that they received during other radiographic sessions, taken weeks or months apart. 119 The radiation exposure a patient would receive could range from 0.25 mGy for a single posterior–anterior image to 3 mGy for a full-spine radiographic examination. 88 A 3 mGy dose is several times lower than the 1100 mGy (95% confidence interval, 500-2600 mGy) dose threshold of radiation-induced leukemia, 120 the first cancer expected from a high-dose exposure (Figure 5). Therefore, it is very unlikely that X-ray images of the spine taken in a serial fashion over several months or years, as currently performed in the treatment of patients with spinal subluxation, would ever contribute to the induction of future malignancies.

Leukemia incidence versus absorbed radiation dose for 95 819 Hiroshima atomic bomb survivors, indicating a threshold of about 1100 mGy for radiation-induced leukemia. 120
Conclusions
The treatment goal of achieving an improved spine alignment, as has been practiced by spine surgeons for many decades, is also an evidence-based practice by chiropractors, physiotherapists, and other manual medicine providers who specialize in modern methods of spine and posture rehabilitation. This is because the cause of spinal pain, dysfunction, and disability often lies in the failure of the body’s attempt to compensate for a discordance within biomechanical relationships of the specific spinal regions and pelvis. Various advances in nonsurgical methods have evolved showing spine and posture corrections that lead to simultaneous pain, dysfunction, quality of life, and physiological and biomechanical improvements. These methods are also displaying the trend that improving posture and spine alignment lead to better long-term outcomes versus traditional or conventional treatments that do not improve spine alignment. Lastly, the essential reliance on repeat radiographs to monitor treatment effect over time is a safe and evidence-based practice.
Footnotes
Acknowledgments
The authors thank Jerry M. Cuttler for critical review of an earlier version of the manuscript as well as for the image used in Figure 5. The authors also thank Dr Jason Haas for the image used in ![]() .
.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: P.A.O. is a paid research consultant for CBP NonProfit, Inc. D.E.H. teaches spine rehabilitation methods and sells products to physicians for patient care that require radiography for biomechanical analysis.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funds from CBP NonProfit, Inc.