
Abstract
Objective
This study was conducted to explore the appropriate radical radiation dose in concurrent chemoradiotherapy (CCRT) for patients with inoperable stage II–III esophageal squamous cell carcinoma (ESCC).
Methods
This retrospective study included patients with esophageal cancer (EC) from the database of patients treated at the Affiliated Zhangjiagang Hospital of Soochow University (1/2015–12/2019). Overall survival (OS), progression-free survival (PFS), objective remission rate (ORR), first failure pattern, and toxicities were collected.
Results
112 patients treated with intensity-modulated radiation therapy (IMRT) combined with concurrent chemotherapy of nedaplatin-based regimens were included. Fifty-eight (51.8%) and 54 (48.2%) patients received 60 (HD) and 50.4 (LD) Gy of radiotherapy, respectively. The HD group showed superior OS and a trend for longer PFS compared with the LD group (median OS: 25.5 vs 17.5 months, P = .021; median PFS: 14.0 vs 10.5 months, P = .076). There were more patients with a complete remission (CR) in the HD group than in the LD group (P=.016). The treatment-related toxicities were generally acceptable, but HD radiotherapy would increase the incidence of grade ≥3 late radiotoxicity (22.4% vs 5.6%, P = .011).
Conclusion
In nedaplatin-based CCRT for stage II–III ESCC, the radiotherapy dose of 60 Gy achieved a better prognosis.
Strengths and limitations of this study
A comparative study of 50.4 Gy and 60 Gy was conducted to evaluate whether 50.4 Gy can be used as a radical radiotherapy dose for inoperable stage II–III esophageal squamous cell carcinoma from a real-world perspective.
The highly consistent selection criteria in our study make analysis results highly reliable and scientific.
The existing research results support that nedaplatin can be used in concurrent chemoradiotherapy for esophageal squamous cell carcinoma, and this study focuses on the discovery of a better nedaplatin-based combination regimen.
The findings of this study are limited to a single-center study with a non-large sample size.
Inevitably, recall bias may exist in this retrospective study.
Surgery was not involved in the follow-up treatment after concurrent chemoradiotherapy, which may worsen the prognosis of some patients.
Keywords
Introduction
Esophageal cancer (EC) is one of the most deadly malignant epithelial tumors with poor long-term survival,1,2 with an estimated 604,100 new cases and 544,076 deaths in 2020 worldwide. 3 Arguably, surgery remains the preferred treatment for early EC.4,5 Still, due to the high rate of lymph node metastasis and the lack of early symptoms, many patients are diagnosed in the late stages, patients that can be cured by surgery are rare, and postoperative recurrence is common, especially for advanced disease.4-7 Unfortunately, most EC patients in China are diagnosed as locally advanced. 8
Squamous cell carcinoma (SCC) is the most common pathological type of EC and accounts for about 95% of all cases of EC in China. 9 Esophageal squamous cell carcinoma (ESCC) is considered moderately sensitive to radiation,10,11 and radiotherapy is currently one of the few treatment modalities with definite curative effects in addition to surgery.4,5 Concurrent chemoradiotherapy (CCRT) is the standard treatment for nonsurgical locally advanced EC, as established by the Radiation Therapy Oncology Group trial 85-01 (RTOG 85-01). 12 Still, controversies are ongoing regarding the optimal radiation dose, radiation volume, and concurrent chemotherapy regimen in CCRT for non-operable EC patients. Based on the result of RTOG 94-05, 13 50.4 Gy can be considered a radical treatment for locally advanced EC by radiotherapy as survival is similar compared with higher doses and with less toxicity. Nevertheless, it is worth noting that the above results were largely based on esophageal adenocarcinoma, which cannot exactly represent ESCC. Otherwise, few randomized clinical trials (RCTs) could provide high-quality evidence to determine the appropriate radical dose and clinical target volume of radiotherapy for inoperable locally advanced EC. The choice of 50.4 or ≥60 Gy remains a major unsolved issue in radiotherapy for EC in the past decade. A meta-analysis that included 18 relative publications was conducted in 2017 14 to compare patients who received CCRT ≥60 vs <60 Gy and found that a total dose of ≥60 Gy appeared to be better in improving overall survival (OS) and locoregional control (LRC), especially in Asian countries. The results of three studies15-17 showed that high-dose (≥60 Gy) radiation in CCRT was safe under the premise of using modern radiotherapy technologies. Zhang et al. 18 considered that the dose-response relationship resulted in LRC for patients with stage II–III EC treated with CCRT. Suh et al. 19 conducted a retrospective study that included 126 patients with stages II-III EC and concluded that high-dose radiotherapy with ≥60 Gy in CCRT was more suitable for East Asians for improving LRC and progression-free survival (PFS) without a significant increase of treatment-related toxicity. In the present study, we discussed the benefits and disadvantages of 50.4 and 60 Gy in CCRT of stage II–III ESCC.
In the past decade, no substantial progress was made in chemotherapy for EC. Cisplatin (DDP) combined with 5-fluorouracil (5-FU) is still considered as a classic regimen for CCRT of EC, which may evoke a tumor response and improve survival.4,5,20-22 Still, outstanding renal, gastrointestinal, and cardiac side effects limit its use. Some drugs have shown more safety compared to 5-FU-or DDP-based regimens with no less or better treatment effect, such as paclitaxel, docetaxel (DOC), tegafur-gimeracil-oteracil potassium (S-1), oxaliplatin (OXA), nedaplatin (NDP), and raltitrexed.23-29 The combination of S-1 and DDP showed superior safety and efficacy compared with 5-FU/DDP.30-32 A phase II clinical trial 33 demonstrated that concurrent chemoradiation with S-1 and cisplatin exhibited encouraging results with pathologic complete response. In a previous study by the authors’ group, 34 nedaplatin-based CCRT regimens as first-line treatment could make the 3-year survival rate of patients with stage II–III ESCC reach 31.4%, with an acceptable toxicity profile. NDP-based chemotherapy combined with radiotherapy is applicable in EC.
Therefore, this study aimed to compare the effects of different doses of radiotherapy (50.4 vs 60 Gy) on survival, treatment responses, failure patterns, and treatment-related toxicities in patients with nedaplatin-based CCRT. The results could suggest the appropriate dosage that could be used as radical radiotherapy dose in CCRT of patients with stage II–III ESCC.
Methods
Patients
This retrospective study included patients with EC from the database of patients treated at the Oncology Department of the Affiliated Zhangjiagang Hospital of Soochow University (Jiangsu, China) between January 2015 and December 2019. This study was approved by the Medical Ethics Review Committee of the Affiliated Zhangjiagang Hospital of Soochow University (#201901-KS001).
The inclusion criteria were (1) histologically-confirmed ESCC by gastroscopy or ultrasound gastroscopy, (2) clinical stage II–III, diagnosed according to the criteria of the International Union Against Cancer 2009, seventh edition, 35 (3) no history of thoracic surgery or radiotherapy, (4) 20–75 years of age, and (5) Eastern Cooperative Oncology Group (ECOG) performance status (PS) score of 0–1. 36 The exclusion criteria were (1) patient scheduled for surgery, (2) poor liver, kidney, or bone marrow function, or diseases that might increase treatment-associated organ dysfunction, (3) severe cardiopulmonary diseases, (4) esophageal perforation or deep ulceration, (5) considerable esophageal bleeding, or (6) contraindications to radiotherapy or chemotherapy.
According to the hospital medical records, the patients were divided into the LD (low dose, 50.4 Gy) or HD (high dose, 60 Gy) group.
Radiotherapy Regimen
Radiotherapy was initiated within 7 days of starting chemotherapy. Intensity-modulated radiation therapy (IMRT) with a 6-MV X-ray was adopted via a high-energy (≥6 MV) linear accelerator. Gross tumor volume (GTV) was defined as the total volume of primary tumor (GTVp) and metastatic lymph node (GTVnd). Involved lymph nodes were confirmed via 64-multislice computed tomography (CT) scan of the cervix, chest, and abdomen or positron emission tomography-computed tomography (PET-CT). Clinical target volume (CTV) included the extensions of primary and metastatic disease plus the elective lymph node regions (CTVen). CTV of primary tumor (CTVp) included 1.0 cm expansion of the GTVp in circumferential direction and 3 cm extension of the GTVp in the craniocaudal direction. CTV of the involved lymph nodes (CTVnd) was defined as GTVnd plus 1 cm all directional margins. For upper-and middle-thoracic EC, CTVen included group supraclavicular nodes plus 1, 2, 4, 5, and 7 thoracic nodes while group 2, 4, 5, and 7 thoracic, left gastric, and paracardiac nodes were designated for lower thoracic EC. Planning target volume (PTV) was set as CTV plus a 5 mm margin in all directions to compensate for set-up variations and internal organ motion. Add up to 60 Gy (2.0 Gy per fraction) radiation dose was delivered to primary tumor and metastatic lymph node in HD group, while it was 50.4 Gy (1.8 Gy per fraction) in LD group. The prescribed dose delivered to elective lymph node region was set as a total of 45-50.4 Gy (1.8 Gy per fraction) consistently in each group. Based on the dose-volume histogram, the organ dose limits were set as follows: (i) Mean lung dose (MLD) ≤16 Gy, V20 ≤30%; (ii) mean heart dose (MHD) ≤40 Gy; and (iii) maximum spinal cord dose ≤45 Gy. If these constraints were not satisfied, the plan was altered to: MLD <20 Gy, lung V20 <40%, and MHD <45 Gy.
Chemotherapy Regimen
The chemotherapy regimen was one of the following: (i) 70 mg/m2 NDP intravenously on day 1 plus 40 mg S-1 orally twice daily for 2 weeks, and repeated on day 22; (ii) 35 mg/m2 NDP intravenously plus 35 mg/m2 DOC intravenously on days 1 and 8, and repeated on day 22. The chemotherapy dose was reduced by 20% in the subsequent cycle if grade 4 hematological or grade ≥3 non-hematological toxicity occurred, and chemotherapy and radiotherapy were suspended until bone marrow/other organ functions normalized. Chemotherapy was terminated if the patient was unable to tolerate the toxicity or withdrew. Additional cycles of chemotherapy were suggested to be performed following CCRT.
Data Collection and Definition
Tumor response, recurrence, and metastasis were evaluated through systematic examinations, including physical examination, enhanced CT of the neck, chest, and abdomen, gastroscopy, and upper gastroenterography. Tumor response after treatment was assessed in accordance with the Response Evaluation Criteria in Solid Tumors version 1.1 (RECIST 1.1). 27
The following data were collected for analysis: (1) patient’s response to treatment including complete remission (CR), local recurrence (LR), partial remission (PR), stable disease (SD), and progressive disease (PD), (2) patient’s survival from the start of treatment to the end of observation including OS and PFS, (3) first failure pattern after CCRT, including local recurrence, regional lymph node recurrence, locoregional failure, distant metastasis, and distant/local/regional failure, and (4) all CCRT-related toxicities during and after treatment including acute and late toxicity. All data were collected from the hospital record system.
OS and PFS were respectively defined as the duration from the start of treatment to mortality or the last follow-up, and tumor progression or death. Locoregional failure was defined as a failure pattern when local recurrence and regional lymph node recurrence were detected at the same time. The objective remission rate (ORR) was defined as CR plus PR. Regional lymph node recurrence was diagnosed by imaging as (1) nodes reappear in the original position following CR, or (2) regional nodes that newly appear after prophylactic irradiation. Distant/local/regional failure was interpreted as local recurrence or regional lymph node metastasis that occurred simultaneously as distant metastasis, including a triple failure pattern.
Statistical Analysis
Data were analyzed using SPSS 24.0 (IBM Corporation, Armonk, NY, USA) and GraphPad Prism 6 (GraphPad Software, San Diego, CA, USA). Student’s t-test or Wilcoxon rank-sum test was used to compare the continuous variables between two groups. Categorical variables were compared using Fisher’s exact test. The D’Agostino-Pearson omnibus normality test was used to examine if the variables had a Gaussian distribution. Survival data were estimated using the Kaplan-Meier method and the log-rank test. Univariable and multivariable analyses were done using the Cox proportional-hazards model. Two-sided P-values <.05 were considered statistically significant.
Results
Characteristics of the Patients
A total of 283 patients with stage II–III EC were screened for inclusion, of whom 141 patients were excluded because of non-ESCC (n = 15) or inconsistent treatments (n = 126) (Figure 1). Of the remaining 142 patients, 30 were not included because of unavailable data. At last, 112 patients were included in the analysis: 58 (51.8%) and 54 (48.2%) patients received 60 and 50.4 Gy, respectively. Patient flowchart.
Baseline characteristics of the patients.

HD = high dose; LD = low dose; ECOG PS = Eastern Cooperative Oncology Group performance status; NS = nedaplatin and S1; ND = nedaplatin and docetaxel.
Follow-Up and Survival
Survival and clinical response.

HD = high dose; LD = low dose; CR = complete remission; PR = partial remission; OR = objective remission; SD = stable disease; PD = progressive disease. OR= CR + PR.

Kaplan–Meier curves displaying (A) overall survival rates and (B) progression-free survival rates for patients in the HD (high-dose) group (green) and the LD (low-dose) group (blue).
Response to Treatment
Table 2 shows the tumor responses. Twenty-eight patients (25.0%) achieved CR, while 55 patients (49.1%) achieved PR, for an ORR of 74.1%. The ORR was 81.0% and 66.7% in the HD and LD groups, respectively, and the former has a better disease response trend (P = .083). There were more patients who achieved CR in the HD group than in the LD group (P = .016).
Univariable and Multivariable Analysis for Factors Affecting OS and PFS
Analysis of the prognostic factors for OS and PFS.

OS = overall survival; PFS = progress-free survival; HR = hazard ratio; CI = confidence index; ECOG = Eastern Cooperative Oncology Group; PS = performance status; CR = complete remission; PR = partial remission; SD = stable disease; PD = progressive disease.
Subgroup Analysis of OS and PFS
The effects of the chemotherapy regimens on patients receiving different doses of radiotherapy were examined by subgroup analyses. In the HD group, patients receiving the ND and NS regimen had a similar OS (26 vs 27 months, respectively, P = .618, Figure 3(A)) and PFS (14 vs 14 months, respectively, P = .816, Figure 3(C)). Coincidentally, non-significant differences in OS (25 vs 17 months, respectively, P = .962, Figure 3(B)) and PFS (14 vs 9 months, respectively, P = .760, Figure 3(D)) were observed in the LD group. Kaplan–Meier curves displaying (A) overall survival rates and (C) progression-free survival rates for patients in HD (high-dose) group treated with ND (nedaplatin plus docetaxel) regimen (blue) and NS (nedaplatin plus S1) regimen (green); (B) overall survival rates and (D) progression-free survival rates for patients in LD (low-dose) treated with ND regimen (blue) and NS regimen (green).
Treatment Failure Patterns
Treatment failure.

CR = complete remission; PR = partial remission; SD = stable disease; HD = high dose; LD = low dose.
Grade ≥3 Toxicities
Radio/chemotherapy-associated toxicities of grade ≥3.
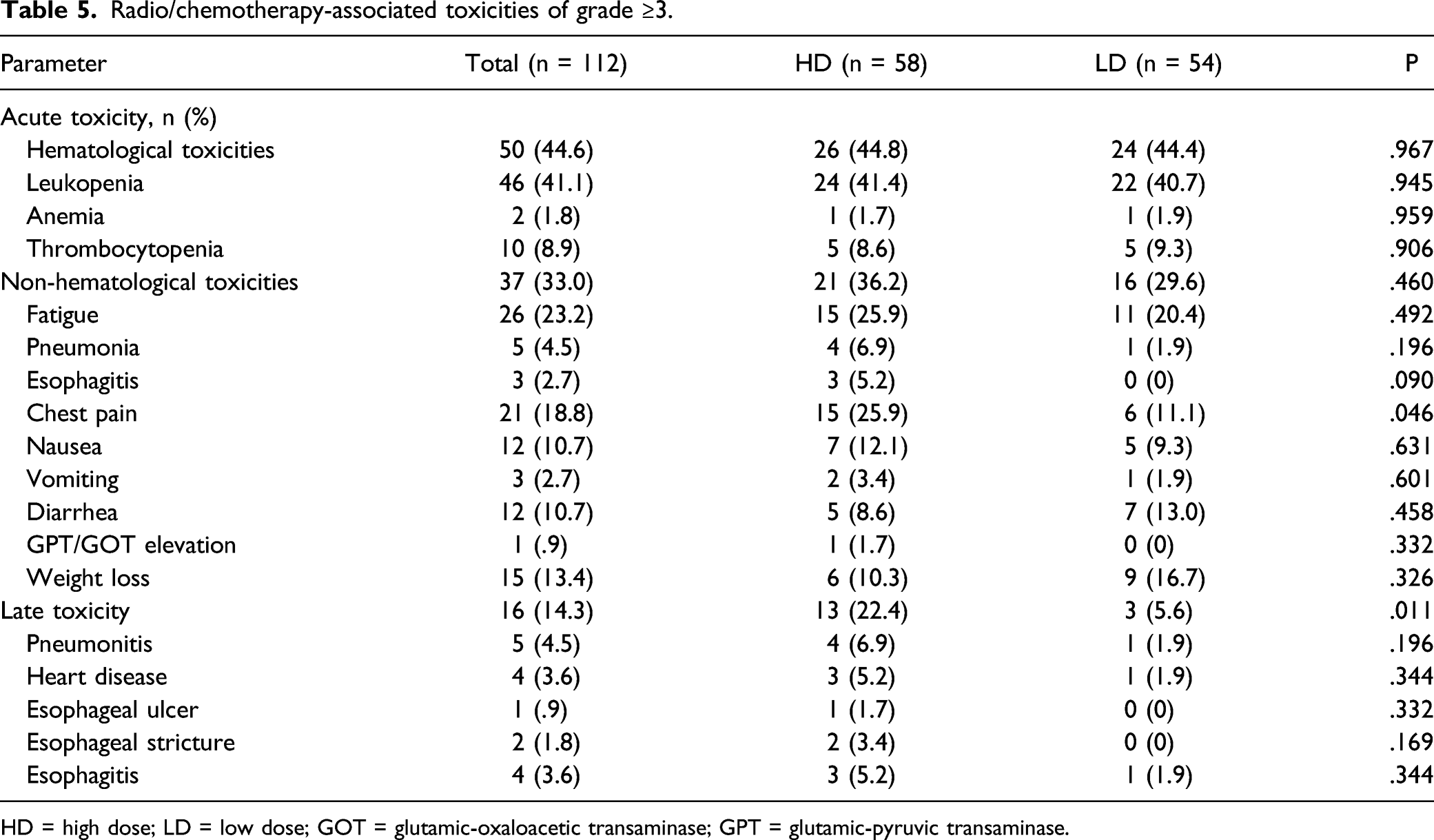
HD = high dose; LD = low dose; GOT = glutamic-oxaloacetic transaminase; GPT = glutamic-pyruvic transaminase.
Discussion
The radical radiation dose in CCRT for patients with stage II–III ESCC is still controversial. Therefore, this study aimed to compare the effects of different doses of radiotherapy (50.4 vs 60 Gy) on survival, treatment responses, failure patterns, and treatment-related toxicities in patients with nedaplatin-based CCRT. This retrospective analysis demonstrated that NDP-based chemotherapy and radiotherapy with a total dose of 60 Gy should be used as a conventional treatment for stage II–III ESCC, resulting in a significantly better OS and CR rate than 50.4 Gy. Multivariable Cox analysis confirmed that achieving an objective remission (CR/PR) was an independent factor predicting a good prognosis.
More than half of the world’s ECs occur in China. 3 Still, no breakthrough was made in the treatment of EC in the past decade, mainly because the inoperable cases account for the majority of the patients. In addition to surgery, radiotherapy is one of the few treatments that can cure locally advanced EC.4,5 Still, controversies regarding the dose of radical radiotherapy, the size of the radiotherapy target volume, and the standard combination therapy impeded the standardization of the treatment of locally advanced EC. Based on the results of RTOG85-01 12 and RGOT94-05, 13 CCRT with a radical dose of 50.0–50.4 Gy delivered to CTV became the standard treatment for locally advanced EC. Nevertheless, because of the differences in race and tumor pathology between Eastern and Western patients, this approach needs to be further explored in the Chinese population. Actually, Chinese authors claimed that ≥60 Gy radiotherapy based on precision radiotherapy techniques like three-dimensional conformal radiation therapy (3D-CRT) or IMRT could improve the survival rates and disease control rates of patients with advanced EC without significantly increasing toxicities.37-39 On the other hand, a multicenter RCT of ESCC patients treated with CCRT showed that a dose-escalation from 50.4 Gy to 60 Gy did not result in a significant improvement in PFS. 40 In the present study, patients treated with a dose of 60 Gy CCRT could improve ORR (81.0% vs 66.7%, P = .083) and a significantly better CR rate (34.5% vs 14.8%, P = .016) compared with 50.4 Gy. On the other hand, high-dose radiotherapy also showed advantages in improving PFS (14.0 vs 10.5 months, P = .076, HR = .703) and OS (25.5 vs 17.5 months, P = .021, HR = .597) compared to low-dose radiotherapy. Furthermore, the multivariable Cox analysis revealed that achieving a positive response (PR or CR) after CCRT independently predicted better OS (HR = .36, P < .001) and PFS (HR = .309, P < .001). The other predictor of poor survival was tumor length ≥5 cm, which might be because a part of the radiation target volume had to be sacrificed or dose to protect organs at risks such as heart, lung, and spinal cord when dealing with long lesions. However, the incidences of grade 3 acute chest pain (P = .046) and total late toxicity (P = .011) associated with radiotherapy were significantly higher in the HD group than in the LD group, but there was no lethal toxicity. Therefore, under the same concurrent chemotherapy background, patients with locally advanced ESCC should receive high-dose (60 Gy) radiotherapy to improve treatment response and survival. Still, whether higher doses (>60 Gy) of radiotherapy would indicate better clinical results remains to be explored.
In addition to the adequate radical radiation dose, the appropriate size of the radiation target volume is also a determinant for an optimal radiotherapy plan. Treatment failures directly result in poor survivals of EC, while the patterns of treatment failure can reflect the inadequacies of the treatment plans. Locoregional control was pivotal in improving survivals in patients with ESCC receiving CCRT. 41 Elective lymph node irradiation (ENI) was conducive to preventing regional nodal failure and distant metastasis and reducing locoregional and distant failure rates.42-44 A previous meta-analysis by the authors’ group evaluating the suitable radiotherapy targets for EC showed that ENI did not lead to superior disease control and survival compared to involved-field irradiation (IFI) but could increase the incidences of acute radiation-related esophagitis and late pneumonia. 45 Still, due to the heterogeneity of radiotherapy doses and chemotherapy regimens of the included studies, the meta-analysis study could not provide a completely convincing answer as to whether ENI or IFI is better. ENI is much more widely used in China than IFI. The present study was conducted using ENI and obtained an overall local recurrence rate of 59%, a regional node recurrence rate of 53.3%, a locoregional failure rate of 41%, and a distant metastasis rate of 14.3%. Local recurrence was the most common of all failure patterns, with a significant difference between the HD and LD groups (44.6% vs 75.5%, P = .001), although patients with T4 disease were significantly more frequent in the HD group. These results precisely demonstrated the necessity of giving a sufficiently high dose (≥60 Gy) of radiotherapy to the primary tumor, especially to the lesion with severe local infiltration (T4). Positive lymph metastasis (cN1-3) was an independent prognostic factor for poor PFS (P = .019) and OS (P = .002) in the univariable Cox analyses but not in the multivariable Cox analysis (P = .114 and P = .073, respectively). However, due to the high recurrence of lymph node metastasis after CCRT, we still advocate high-dose (60 Gy) radiotherapy for metastatic lymph nodes and low-dose (50.4 Gy) radiotherapy for elective lymph nodes in CCRT of locally advanced EC.
NDP is an alternative to DDP and with fewer toxicities. 46 NDP-based chemotherapy regimens showed positive efficacy and tolerability in previous studies of ESCC.47-49 The regimens of NDP combined with DOC or S1 were used as CCRT and maintenance chemotherapy after CCRT in the present study. The subgroup analysis of the HD and LD groups demonstrated that no matter NDP was combined with DOC or S1, significant differences in PFS and OS were not found. Approximately 2/5 of the patients received weekly doses of chemotherapy to weaken acute toxicity caused by one-time high-dose administration. The toxicities were acceptable in patients treated with CCRT, both in the HD and LD groups. Still, the univariable Cox analyses showed that patients would not benefit from receiving additional chemotherapy after CCRT. Therefore, NDP-based CCRT is applicable for locally advanced EC, but the number of cycles of chemotherapy is not a determinant of long-term survival benefit.
There were several limitations in this study. Firstly, this single-center study might not include a large enough sample to detect significant differences in the clinical outcomes completely. Secondly, it was not a rigorously designed randomized controlled clinical study. Therefore, the baseline clinical characteristics between the two arms were difficult to be consistent. In addition, radiotherapy combined with new therapies such as antiangiogenic drugs and immune checkpoint inhibitors should be applied to appropriate patients in the future to tap into the greater therapeutic potential for inoperable locally advanced ESCC.
Conclusion
Patients with stage II–III thoracic ESCC displayed good clinical outcomes following NDP-based CCRT. The radiation dose of be 60 Gy for primary ESCC achieved a better clinical prognosis. The radiation dose for primary EC and metastatic lymph nodes could be 60 Gy to improve treatment response and survival, especially for the lesion with severe local infiltration (T4). A dose of 50.4 Gy radiotherapy for elective lymph nodes is considered safe and recommended to decrease regional lymph metastasis.
Footnotes
Author Contributions
Study design: Y Zuo and XC Sun; literature review: HP Zhu and J Jiang; provision of patients and implementation of treatment: XL Lu, JF Lu, and Y Zuo; collection and assembly of data: HP Zhu and XL Lu; statistical analysis of data: HP Zhu and XC Sun; manuscript writing: all authors; and final approval of manuscript: Y Zuo and XC Sun.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by grants from the Zhangjiagang City Science and Technology Support Program (Social Development) (#ZKS1816).
Patient Consent for Publication
The requirement for informed consent was exempted by the board due to the retrospective nature of the study. Data and associated images and all identifying patient data were removed.
Ethical Statement
This study was approved by the Medical Ethics Review Committee of the Affiliated Zhangjiagang Hospital of Soochow University (#201901-KS001). The requirement for informed consent was exempted by the board due to the retrospective nature of the study.
Data Availability
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.