
Abstract
A subset of victims who experience concussion suffer from persistent symptoms spanning months to years post-injury, termed post-concussion syndrome (PCS). Problematically, there is lack of consensus for the treatment of PCS. Concussion injury involves a neurometabolic cascade leading to oxidative stress and neuroinflammation which parallels the oxidative stress loading occuring from age-related neurodegenerative conditions. Historical and recent evidence has emerged showing the efficacy of low-dose radiation therapy for many human diseases including neurodegenerative diseases such as Alzhiemer’s disease (AD). Due to the pathognomonic similarities of oxidative stress and neuroinflammation involved in PCS and neurodegenerative disease, treatments that prove successful for neurodegenerative disease may prove successful for PCS. Recently, low-dose ionizing radiation therapy (LDIR) has been documented to show a reversal of many symptoms in AD, including improved cognition. LDIR is thought to induce a switching from proinflammatory M1 phenotype to an anti-inflammatory M2 phenotype. In other words, a continual upregulation of the adaptive protection systems via LDIR induces health enhancement. It is hypothesized LDIR treatment for PCS would mimic that seen from early evidence of LDIR treatment of AD patients who suffer from similar oxidative stress loading. We propose the application of LDIR is a promising, untapped treatment for PCS.
Introduction
Concussion is a traumatically induced transient disturbance of brain function that involves a complex pathophysiological process. 1 It is understood to be a mild traumatic brain injury (mTBI) where most patients recover quickly, within 7–10 days. 2 Some patients, however, do not fully recover and have persistent symptoms, so-called post-concussion syndrome (PCS) that may last for months or years after the initial injury. 3
The treatment of acute concussion involves rest with light and graded activity, but there is a lack of consensus for the treatment for those concussion patients whom experience lingering and persistent symptoms (PCS). 3 Here, we present the rationale for a novel treatment for concussion, particularly PCS, that is, low-dose ionizing radiation (LDIR) therapy.
Neurometabolic Cascade of Concussion Parallels Other Neurodegenerative Diseases
Current understanding of concussion involves a neurometabolic cascade as the main pathophysiological process leading to the sequelae of C/PCS. 4 One aspect consistent across concussion injury and neurodegenerative conditions such as Alzhiemer’s disease (AD) involves the role of oxidative stress and neuroinflammation.
Oxidative stress is a disturbance in the prooxidant-antioxidant ratio that favours oxidants. 5 A more current explanation includes the fact that it also leads to a ‘disruption of redox signalling and control and/or damage’. 6 Adaptive oxidative stress responses are activated by molecular redox switches that initiate the activation of multiple gene expressions of defence systems to counteract the challenge. This results in redox homeostasis or a ‘reset’ of redox balance. 7
Oxidative stress is a normal and vital phenomenon, and under normal conditions it is considered a ‘eustress,’ meaning it is physiologic. 7 However, when circumstances initiate the production of excessive oxidant levels, such as occurs in age-related, gradual evolution of neurodegenerative disorders or in the acute neurometabolic cascade of concussion, this becomes non-physiologic; that is, pathologic. Thus, pathogenic oxidative stress, so-called oxidative distress, is the common underpinning for both age-related neurodegenerative diseases and acute neurologic brain injury such as concussion.
LDIR Therapy for Neurodegenerative Diseases
Recently, there has been interest in LDIR treatment for patients suffering from neurodegenerative diseases including, for example, AD.8,9 In 2016, Cuttler et al 10 described the successful application of LDIR for an 81-year old female with advanced AD. After receiving 5 head CT scans over 3 months, the patient displayed improvements in cognition, speech, movement and appetite. In 2017 11 and 2018, 12 two updates reported that the patient continued to do well after ‘booster scans’. Most recently, a case series of 4 advanced AD patients were treated with the same initial treatment protocol as the original case 10 ; three of the four patients had significant clinical improvements in behaviour and wellbeing as reported by caregivers and family members. 13
LDIR Therapy for Concussion
Due to the pathognomonic similarities of oxidative stress and neuroinflammation involved in C/PCS and neurodegenerative disease, treatments that prove successful for neurodegenerative diseases may also prove effective for C/PCS. The use of the Parkinson’s medication amantidine, for example, increases the availability of dopamine by facilitating its release and inhibiting its reuptake; preliminary studies show this medicine can improve symptoms and quality of life in PCS patients. 14
The similarities in pathogenesis of increased oxidative stress in neurodegenerative disease and C/PCS taken together with early evidence of successful treatment to AD patients from LDIR suggest this treatment could be effective in the treatment of PCS. Since most patients suffering from concussion recover relatively quick, 2 this treatment may be particularly promising for the subset of patients who fail to recover; this ranges between 11% and 39% of concussed patients whom develop PCS (depending on differences in diagnostic classification). 15
Since concussion is not an age-relative deterioration process like neurodegenerative diseases, ongoing or booster treatments would not be necessary. Low-dose ionizing radiation treatment would be a limited treatment protocol for concussion, but could prove to expediate the recovery process, again, particularly for PCS patients.
LDIR Mechanism of Action for Brain Disorders/Concussion
As discussed, the common denominator between neurodegenerative disorders and C/PCS is oxidative stress and neuroinflammation. Low-dose ionizing radiation is thought to induce a switching in the central nervous system from a proinflammatory M1 phenotype to an anti-inflammatory M2 phenotype. 16
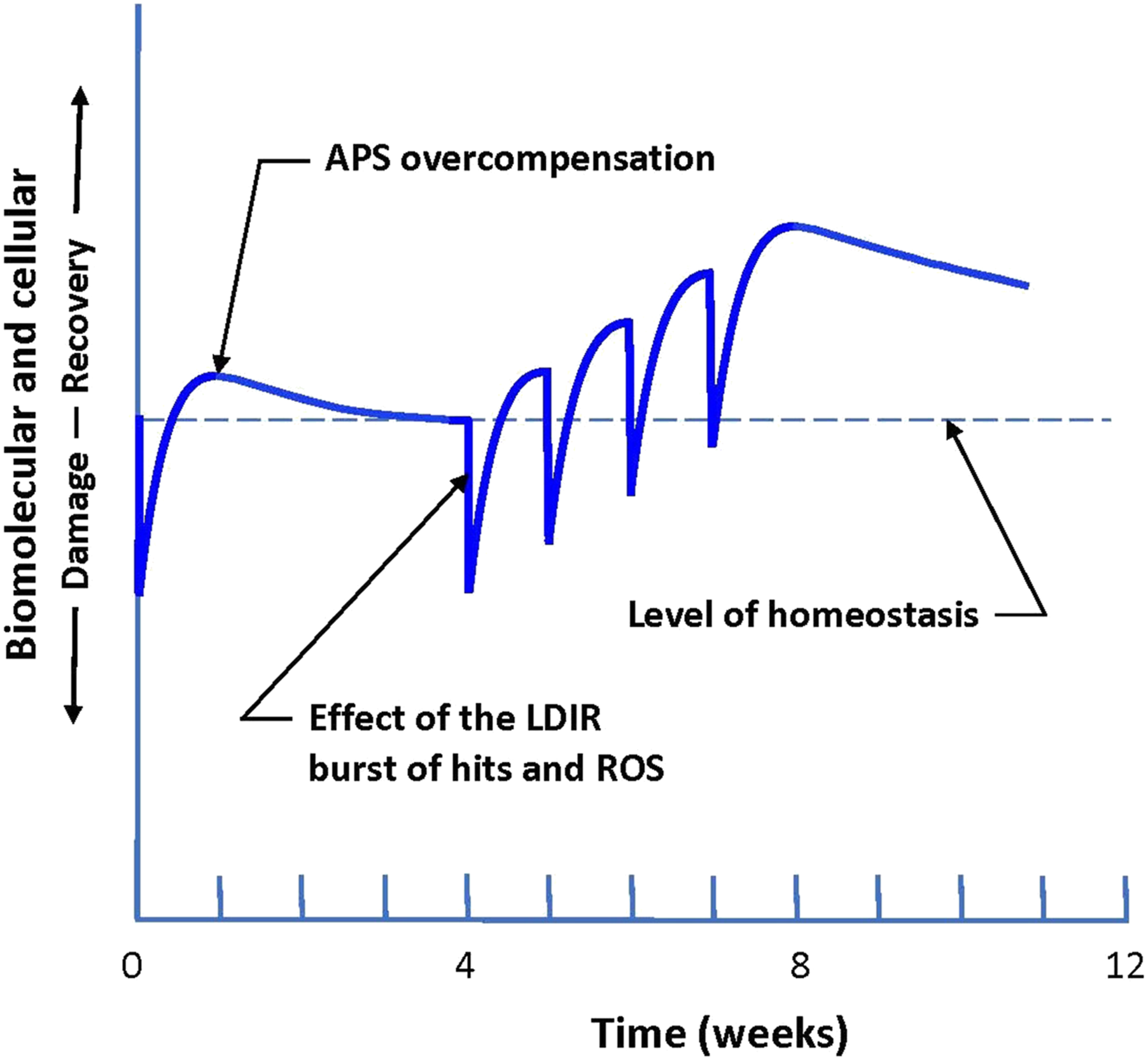
Indeed, low-dose radiation exposures induce an upregulation in the innate adaptive protection systems (APS).17-19 As illustrated by Cuttler, when LDIR exposures are performed in a repeated fashion, a continual upregulation induces health enhancement (Figure 1).
13
A burst of LDIR damages the tissues of the patient and causes reactive oxygen species (ROS). The body’s APS subsequently ‘over-repairs’ the damage caused
20
; that is, it repairs the induced radiation damage as well as other endogenous damage that was pre-existing (e.g. neurodegenerative/PCS oxidative stress and neuroinflammation).
20
This results in an enhanced level of oxidative homeostasis or an improved level of cognitive functioning. LDIR treatment induced damage and recovery to patient. Repeated treatments are hypothesized to create reactive oxygen species (ROS) that gets ‘over-repaired’ by the adaptive protection systems (APS) from the initial damage caused by the radiation burst. Each burst encourages an upregulation of the APS and further improves the health of the patient.
13
Conclusion
The application of LDIR is a promising, untapped treatment for PCS. The risks are non-existent as the radiation doses are in the range that have been shown to enhance health in previously and recently documented human studies. It is expected that LDIR treatment for PCS will mimic that seen recently in the LDIR treatment of patients suffering from neurodegenerative diseases that have similar oxidative stress loading such as AD. 13
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.