
Abstract
Objective:
To analyze changes in immune functions by detecting lymphocyte subsets in the peripheral blood of residents in the vicinity of radon from hot springs.
Methods:
Two groups were randomly selected; 61 residents in the vicinity of the hot springs were assigned to the radon group, and 51 residents with a similar lifestyle and habits but no contact with hot springs were assigned to the control group. The percentages of lymphocyte subsets (CD3+, CD4+CD8−, CD4−CD8+, CD4+/CD8+, and TCR/CD3) in the 2 groups were evaluated on a FACS Aria flow cytometer. The absolute values of lymphocytes (LYMPH#) and percentages of lymphocytes (LYMPH%) were measured by an automatic blood analyzer.
Results:
In the radon group, the numbers of CD3+ (Z = −0.140, P > .05) and CD4+CD8− (Z = −0.964, P > .05) T cells were higher, as compared with the controls, but this difference was not significant. In addition, the number of CD4−CD8+ (t = −2.141, P < .05) T cells was significantly lower in the radon group. Furthermore, the average ratios of CD4+/CD8+ (t = −2.201, P < .05) and TCR/CD3 (t = 2.047, P < .05) cells were significantly higher in the radon group than in the controls. Compared with the control group, the LYMPH# (t = −0.485, P > .05) and LYMPH% (Z = −0.835, P > .05) showed no significant change.
Conclusion:
Radon-rich hot springs could alter the proportions of lymphocyte subsets and possibly affect immunologic functions.
Introduction
Radon is a natural radioactive inert gas that exists widely in the ambient air. The natural radiation dose from radon and its daughters is the largest among normal background radiation, accounting for 54% of the total natural radiation dose. Higher radon levels appear in some mines and indoor environments decorated with radon-containing building materials. Radon has been recognized as the first environmental etiology and second risk factor (after smoking) for lung cancer. Early epidemiological studies have confirmed a significant correlation between radon and lung cancer, even at low levels of exposure. In recent years, health problems caused by long-term radon exposure in daily living have been attracting increased attention. Residents living in the vicinity of radon-rich hot springs for a long duration may be affected by the persistence and accumulation of radon and its daughters.
Animal studies, cell studies, clinical trials, and epidemiological investigations have confirmed that long-term exposure to high levels of radon and its daughters can initiate biological effects at molecular and cellular levels. Although some studies have suggested that radon and its daughters can pose potential health risks to the population, it is generally accepted that radon hot springs can relieve pain, alleviate the symptoms of arthritis and skin diseases, and exert specific regulatory effects on physiological and cardiovascular functions. 1 -7 In Japan, many people often go to hot springs to relieve symptoms of osteoarthritis and bronchial asthma. Europeans believe that radon hot springs can treat inflammation and pain. 8 -15 In this study, the lymphocyte subsets in the peripheral blood of residents around radon-rich hot springs were detected and analyzed to explore the effects of the hot springs on the health of the residents in China.
Materials and Methods
Selection of Participants
The inclusion criteria for residents in Pingshan County, Hebei Province, included long-term residence, no history of migration, no recent history of viral or bacterial infections, no history of malignant diseases or the administration of medications, and no exposure to X-rays within the previous 6 months. In the radon hot spring group, 61 local inhabitants were sampled randomly, aged between 29 and 68 years, with an average age of 42.85 years. Moreover, 51 inhabitants from other villages with similar living habits but with no exposure to radon hot springs were sampled randomly as the control group. They were aged between 25 and 71 years, with an average age of 45.90 years. There were no significant differences in age and gender between the radon hot spring group and the control group (max 2 = 0.78, P > .05). This study was approved by the Ethics Committee of the National Institute for Radiological Protection of the Chinese Center for Disease Control and Prevention (Beijing, China), and all participants gave informed consent.
Background Information
The concentration of radon in the hot springs was 102 ± 11.4 Bq/L, the concentration of indoor radon was 41.9 + 18.6 Bq/m3 over 6 months, and the typical equilibrium factor was 0.61. In some places, the radon concentration in spring water had reached the recommended levels for medical hot springs and radon springs, and the concentration in bathrooms was increased during water use. The measured radon concentration exceeded 200 Bq/m3 (indoor radon limit in China) and 100 Bq/m3 (World Health Organization radon limit value), resulting in an additional annual effective dose of about 0.09 mSv. 16 The distance between the sampling location for the control group and the radon hot springs was about 11.2 km, and there were no other outdoor radon hot springs in the area (the annual indoor radon concentration in Shijiazhuang was 42.4 ± 20.2 Bq/m3).
Bathing or Showering Habits
In the radon hot spring group, 52.38% of households had hot spring baths. The mean number of baths taken was 10.48 a month per person in the winter and 27.31 in the summer. Furthermore, among the persons in the radon hot spring group, 45.24% took traditional baths and 9.52% took showers. In the control group, no households had hot spring baths. The mean number of baths taken was 3.30 a month per person in the winter and 28.25 in the summer. In the control group, 86.36% of persons took showers, whereas no one took baths.
Instruments and Reagents
Four-color labeled CD3 FITC/CD8 PE/CD45 PerCP/CD4 APC antibody, 2-color labeled CD3 PerCP, and anti-TCR-α/-1 FITC antibody were purchased from BD Company (San Jose, California). In addition, BD FAC lysing solution and the FACS Aria system were obtained from BD Company.
Detection of Lymphocyte Subsets, Absolute Values, and Percentages of Lymphocytes
Each specimen was divided into 3 tubes, to which 100 µL of whole blood was added. In addition, 5 µL of CD3/CD4/CD8/CD45 antibody and TCR/CD3 antibody were added to each tube. The tubes were then shaken and mixed, and left to react at room temperature for 30 minutes. A volume of 2 mL of prepared erythrocyte lysate was then added, and the tubes were again shaken and mixed, and left to stand at room temperature in the dark for 10 minutes. The tubes were subsequently centrifuged at 1000 rpm for 5 minutes. The supernatant was discarded, and the cells were washed once with 1× phosphate buffer saline, after which 500 µL phosphoric acid buffer was added. The cells were then analyzed using a flow cytometer. The various lymphocyte groups were detected and selected, and the percentage of each subset was determined. The absolute values of lymphocytes and percentages of lymphocytes were measured by an automatic blood analyzer.
Epidemiological Investigation on the Prevalence of Rheumatism and Cancer in Radon Hot Spring Area and Control Area
By 2019, the total population of the radon hot spring area was 21 071and the total population of the control area was 35 762. The prevalence of cancer and rheumatism in the 2 areas was investigated.
Statistical Analyses
SPSS version 21.0 statistical analysis software and the χ2 test were used to analyze the distribution of basic characteristics between the 2 groups. The χ2 test was used to analyze the prevalence of rheumatism and cancer between radon hot spring area and control area. The normal distribution of lymphocyte subsets between the 2 groups was evaluated. CD45, CD4+/CD8+, TCR/CD3 cells, and the number of lymphocytes were normally distributed so the Student t test was applied. The CD4−CD8+, CD4+CD8−, CD3+ cells, and percentage of lymphocytes were not normally distributed; thus, the Mann-Whitney U test was used for analysis. Value of P < .05 was considered statistically significant.
Results
Basic Data Analysis
The constituent ratios of basic data (gender, age, alcohol consumption, smoking, and body mass index [BMI]) are presented in Table 1. The distribution of basic data showed no significant difference between the 2 groups (P > .05).
Comparison of Basic Data in the 2 Groups.

Abbreviations: BMI, body mass index; F, female; M, male.
Multiple Linear Regression Analysis of Lymphocyte Subsets
Multiple linear regression analysis of lymphocyte subsets showed a significant correlation between radon exposure factors and CD4−CD8+ and TCR/CD3 cells (Table 2).
Regression Analysis of Lymphocyte Subsets in Peripheral Blood.
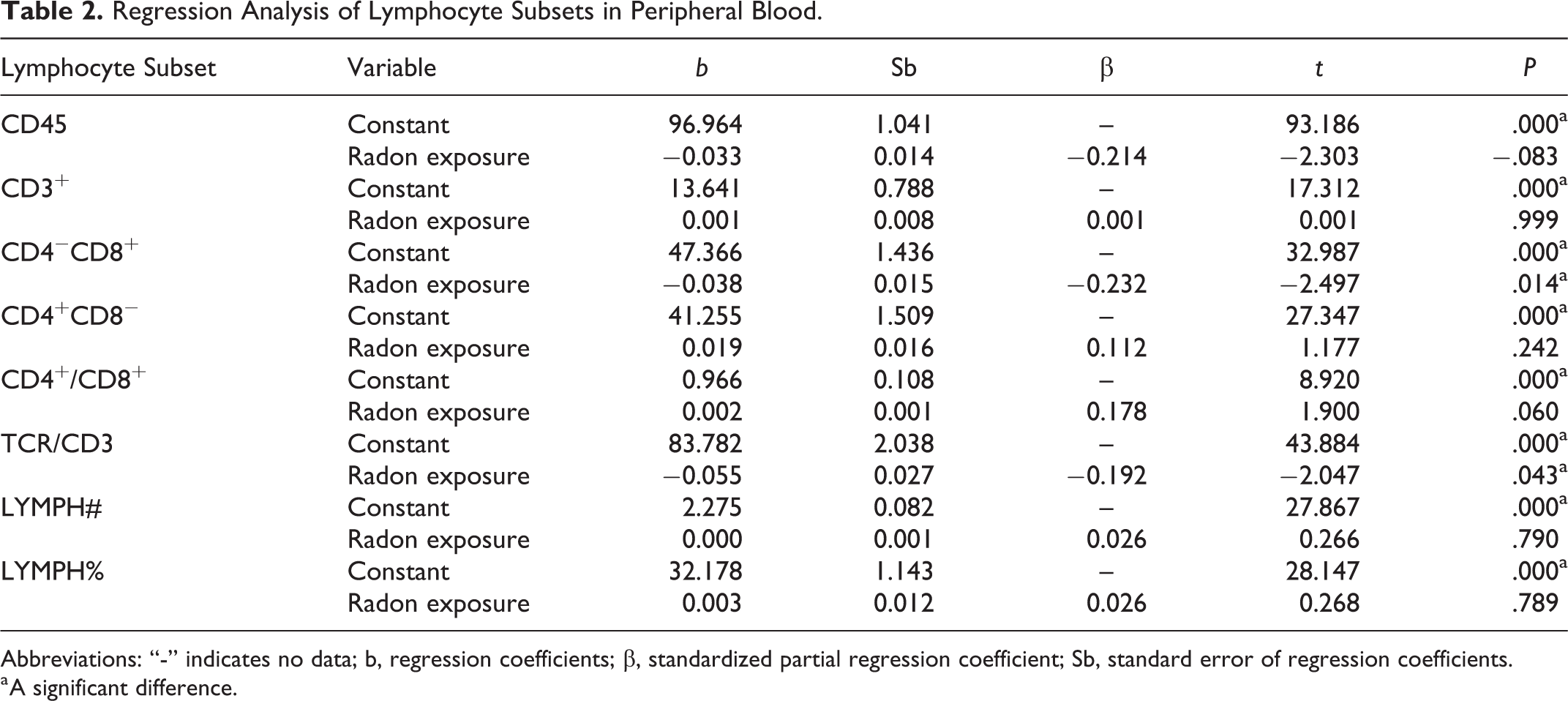
Abbreviations: “-” indicates no data; b, regression coefficients; β, standardized partial regression coefficient; Sb, standard error of regression coefficients.
a A significant difference.
Comparison of Lymphocyte in Peripheral Blood Subsets Between the 2 Groups
The percentage of CD45, CD4+/CD8+, and TCR/CD3 lymphocyte subsets was significantly higher in the group exposed to radon than that in the control group (P < .05; Table 3). Compared with the control group, the percentage of CD4−CD8+ lymphocytes was significantly lower in the group exposed to radon. In contrast, the percentage of CD4+CD8− and CD3+ lymphocytes was higher in the radon group, as compared with that in the control group; however, this difference was not significant (Table 4).
Percentage Change in Lymphocyte Subsets in the Radon Hot Spring Group.

Abbreviation: SD, standard deviation.
a A significant difference.
Comparison of the Percentage Change in Lymphocyte Subsets by Mann-Whitney U Test.

a A significant difference.
Comparison of the Prevalence of Rheumatism and Cancer Between Radon Hot Spring Area and Control Area
Compared with the control group, there was no significant difference in the total prevalence between the 2 area (P = .814). The prevalence of rheumatism in radon hot spring area was higher (0.2% vs 0.1%, P < .001), the prevalence of cancer was lower (0.1% vs 0.2%, P = .009) (Table 5).
Comparison of the Prevalence of Rheumatism and Cancer Between Radon Hot Spring Area and Control Area.

a A significant difference. Prevalence, number of sick people; nonprevalence, number of people not ill; rheumatism + cancer, sum of the number of patients with rheumatism and cancer.
Discussion
Studies have shown that low-dose radiation can induce hormetic effects in organisms. 17 Liu 18 observed the results of immune enhancement by low-dose radiation through a high-background radiation study in Yangjiang, China, and a series of animal experiments. They found the change in T lymphocytes was the key factor of immune enhancement by low-dose ionizing radiation, which was conducive to T-cell differentiation toward T-helper (Th) 1 cells and could have induced an adaptive response. At present, the low-dose radiation hormetic effect is evaluated mainly by low-linear energy transfer (LET) radiation. However, whether low-dose high-LET radiation causes hormetic effects have been less reported.
The impact of radon and its daughters on human health arise mainly from the α particles produced by its decay, which is high-LET irradiation. Studies on α-particles have been conducted mainly in vivo through animal experiments, cell levels in vitro, and clinical treatment of certain human diseases using radon hot spring. Chauhan et al 19 irradiated human pulmonary epithelial cells with different doses of α-particles. Pathway analyses showed that radiation from α-particles could affect cell-cycle arrest, DNA replication, and repair of DNA damage. Those data suggested that high-LET radiation could activate different biological pathways compared with low-LET radiation.
In the present study, the concentration of radon in the hot springs was 102 ± 11.4 Bq/L, the concentration of indoor radon was 41.9 ±18.6 Bq/m3 over 6 months, and the typical equilibrium factor was 0.61. The radon concentration in the bathroom increases rapidly during water use. The indoor radon concentration increases rapidly from the normal background value (<50 Bq/m3) to more than 200 Bq/m3. After about 3 hours, the indoor radon concentration recovers gradually to a lower level. The variation in the concentration of radon daughters is consistent with that of radon concentration. The additional annual effective dose is about 0.09 mSv. 16 Some residents have been exposed to low-dose ionizing radiation for a long time (more than 5 years). Therefore, radon in hot springs is considered long-term low-dose and high-LET radiation.
Our research team has studied genetic/molecular levels and antioxidant damage in residents of the radon hot spring in Pingshan area. 20 -24 Ruan et al 20 compared the micronucleus frequency and micronucleus cell numbers in different age groups of 2 groups of residents. They found that the micronucleus rate and micronucleus cell rate of the radon hot spring group were significantly higher than those of the control group, but that micronucleus rate was within the normal range. Furthermore, they found no significant differences in the chromosome aberration rate compared with that in the control group. In studies by Liu et al 21-22 and Gao et al 23 of the lymphocyte cell cycle and regulatory proteins, upon radon exposure, the S-phase proportion of lymphocytes in peripheral blood was increased; expression of related cyclic regulatory proteins CDKl, CDK6, and cyclin El was decreased; expression of microRNA-449a was increased significantly in the radon hot spring group; and expression of cyclin El and CDKl was decreased due to upregulation of microRNA-16 expression. Gao et al 24 showed that radon can activate antioxidant function, scavenge oxygen free radicals, and reduce oxidative damage. These phenomena may be related to the hormesis of low-dose radon exposure, which is manifested in various facets. In present study, we observed the effect of long-term low-dose radiation on immune function.
Lymphocytes are radiation sensitive and comprise the main immune cell type. Therefore, they are often used as an important indicator for the early diagnosis of, and dose estimation in radiation sickness. T lymphocytes are important immunocompetent cells. In addition to mediating cellular immune functions directly, T lymphocytes have key roles in regulating the immune response. The molecules on the surface of T lymphocytes enable these lymphocytes to recognize antigens, interact with other immune cells, and receive signal stimulation, among other functions. These membrane-surface molecules also play a key part in identifying and separating T lymphocytes and T-lymphocyte subsets. The T-lymphocyte subsets play an important role in regulating the stability of immune function.
The distribution of lymphocyte subsets can reflect the immune status of the body. Studies 25 -30 have shown that the distribution of lymphocyte subsets is influenced by age, gender, ethnicity, and region. Therefore, we first compared general data (gender, age, alcohol consumption, smoking, BMI) of the 2 groups in Pingshan County. No significant differences were noted in the constituent ratios between the 2 groups (Ps > .05), and both were comparable.
We found that the percentage of CD3+ cells and CD4+ cells in the peripheral blood of residents living near the high-radon hot springs in Pingshan was higher than that of residents living in the control areas, but this difference was not significant. In addition, the percentage of CD8+ cells was significantly lower, and the percentage of TCR/CD3 complexes, and ratio of CD4+/CD8+ were significantly higher in the residents living near the high-radon hot springs in Pingshan group than in the control aera, and these differences were significant (P < .05). Routine blood testing showed that the percentage of lymphocytes and absolute values of lymphocytes in peripheral blood showed no significant change in the residents of the high-radon hot spring area compared with the control group.
Lymphocyte subsets regulate each other in terms of the immune response to maintain normal immune function. Both Th (CD4+) cells and Ts (T inhibition cells, CD8+) cells play an important regulatory role in the immune response. CD8+ cells play an effective cell-mediated immune killing role after being stimulated by foreign antigens, which destroy target cells directly. In addition, CD4+ cells, sensitized by foreign antigens, produce lymphokines, which induce the proliferation of T lymphocytes, B lymphocytes, and macrophages. The balance between the proportions of CD4+ and CD8+ T cells plays an important role in inhibiting tumors, infections, and autoimmune diseases. Immune dysfunction can be caused by an imbalance between these cells, resulting in a series of immunopathological changes that can affect the immune protective mechanisms. 31,32
In the present study, the percentage of TCR/CD3 cells in the peripheral blood of residents near the radon hot springs was increased significantly, which may have been related to the hormesis effect caused by low-dose radiation. Low-dose low-LET radiation accelerates the renewal and growth of thymocytes and, thus, increases the number of thymocytes, and accelerates upregulation of TCR/CD3 expression. Therefore, the ability of the thymus to transport T cells to the periphery is enhanced. Simultaneously, cytokine secretion is stimulated, and the intercellular interactions form an enhanced network which, ultimately, improves the anticancer and anti-infection capabilities of the body. Our study implied that long-term exposure to low-dose high-LET radiation also has the same hormesis effect on the immune system.
Anderson et al 33 suggested that “low-dose” radiation might inhibit Ts with higher sensitivity, thus altering the ratio of Th to Ts, leading to the dominant position of Th, increasing the immunopotentiatory regulation of Th, and enhancing immune function. In their study of the long-term immune effects of high-level natural radiation on residents in Yangjiang, China, Kun et al 34 also observed that long-term exposure to low-dose radiation stimulated different CD4+ and CD8+ T lymphocytes and enhanced immune function. However, few reports have focused on the effects of low-dose and high-LET radiation on immune function. Yamaoka et al 35 found that radon treatment and heat treatment could enhance antioxidant capacity, increase the percentage of CD4+ cells, and reduce the percentage of CD8+ cells among killer T cells and suppressor T cells. Those findings are consistent with our results.
Based on our previous research in this area, 23,24 2 factors may be involved in enhancing the immune function among residents of the radon hot springs region in Pingshan County. First, the proportion of S-phase lymphocytes in peripheral blood increased and that of the G0/G1 phase decreased among inhabitants around radon hot springs. These data indicated that the S phase was prolonged, radiation sensitivity of the S phase was poor, and this phase marked a period of DNA repair/synthesis. Lymphocytes might be protected by prolonging the S phase in conditions of long-term low-dose radiation. Second, several studies in China and overseas 36 -41 have shown that long-term bathing in radon hot springs leads to reductions in oxidative damage and that the ability to scavenge reactive oxygen species increases. The level of 8-hydroxy-2′-deoxyguanosine in the peripheral-blood plasma of residents in the radon hot spring group in Pingshan County was decreased, whereas the level of thioredoxin reductase was increased significantly. These effects may activate antioxidant functions, reduce oxidative damage, and protect radiation-sensitive lymphocytes.
The cancer prevalence in the radon hot springs area was significantly lower than that in the control area (0.1% vs 0.2%, P = .009). Combined with laboratory analyses of the immune function in the 2 areas, we postulated that the decrease in cancer prevalence in the radon hot springs area may have been due to long-term low radon exposure, which can stimulate immune function, activate the antioxidant capacity of the body, and reduce the oxidative damage caused by radiation. However, the prevalence of rheumatic diseases in the radon hot springs area was significantly higher than that in the control area. The complex etiology of rheumatic diseases (eg, environmental conditions, living conditions) and many other factors can affect the immune function. The cause of the increased prevalence of rheumatic diseases in radon hot springs areas needs to be studied further. Because the sample size of our study was small, how radon hot springs influence lymphocyte subsets and immune function must be tested further in much larger cohorts.
Conclusions
Radon hot springs in Pingshan County posed no obvious threats to the health of residents and may enhance immune function.
Footnotes
Authors’ Note
Chunnan Piao undertook on-site sample collection, processing of laboratory samples data analyses, and wrote the manuscript. Mei Tian and Hongjun Gao guided the research ideas, research programs, experimental methods, and manuscript revision. Jianlei Ruan, Yanxiao Gao, Gang Gao, Lirong Yi, and Lina Wu contributed significantly to on-site investigation, sample collection, and guidance for experimental methods. Jianxiang Liu conceived and designed the work and approved the final version of the manuscript.
Acknowledgments
The authors thank the staff of Hebei CDC, Pingshan CDC, and all participants for their support and cooperation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by the National Institute for Radiological Protection, Chinese Center for Disease Control and Prevention.