
Abstract
Liquid biopsy has the great potential of detecting early diseases before deterioration and is valued for screening abnormalities at early stage. In oncology, circulating DNA derived from shed cancer cells reflects the tissue of origin, so it could be used to locate tissue sites during early screening. However, the heterogenous parameters of different types limit the clinical application, making it inaccessible to encompass all the cancer types. Instead, for reproducible scenario as pregnancy, fetal cell-free DNA has been well utilized for screening aneuploidies. Noninvasive and convenient as is, it would be of great value in the next decades far more than early diagnosis. This review recapitulates the discovery and development of tumor and fetal cell-free DNA. The common factors are also present that could be taken into consideration when collecting, transporting, and preserving samples. Meanwhile, several protocols used for purifying cell-free DNA, either classic ones or through commercial kits, are compared carefully. In addition, the development of technologies for analyzing cell-free DNA have been summarized and discussed in detail, especially some up-to-date approaches. At the end, the potential prospect of circulating DNA is bravely depicted. In summary, although there would be a lot of efforts before it’s prevalent, cell-free DNA remains a promising tool in point-of-care diagnostic medicine.
Introduction
Early detection provides many ways to improve outcomes for patients. Take patients with cancer as an example, who benefit a lot from early detection and treatment, the overall survival rate of patients with tumor declines as the diagnostic and therapeutic time delays. Most of the patients have progressed into mid–late stages when cancer is diagnosed, when the best time for treatment has been missed. If those late-stage patients could be treated well as early as possible, then the death rate would decrease at least by half. Unfortunately, most of the diagnostic methods currently used in clinics, such as imaging and biomarkers, could not meet the requirement to uncover subtle clues, that’s where liquid biopsy comes out. Liquid biopsy makes early screening into possible by tracing peripheral circulating cell-free DNA (cfDNA), cell-free RNA, circulating proteins, and so on. 1 -5 Among them, cfDNA is the one commonly used to detect corresponding diseases. Cell-free DNA has been applied to help screen and diagnose various illnesses depending on their origins. However, tumor cfDNA that is derived from degraded tumor cells and fetal cfDNA that comes from placental trophoblast cells attract the most attention of doctors and researchers. Especially, fetal cfDNA has widely been translated into clinical noninvasive screening. Nowadays, the rocketing research about tumor cfDNA facilitates the early cancer screening for various types. In this review, we will take a glance of those 2 biotools for enhancing personalized early-stage diagnosis.
Tumor-Associated cfDNA
Circulated cell-free DNA originates from degraded DNA in apoptotic and necrotic cells that are released into blood plasma, consisting of small fragments (70∼200 bp) and large fragments up to 21 kb. 6 The very first discover about circulating nucleic acids was published in 1948 by Mandel and Metais. 7 Subsequently, it was reported to be significantly increased in patients with systemic lupus erythematosus. 8 Later than that, higher cell-free DNA presented in 173 patients with various cancer compared with 55 normal healthy ones, which was positively associated with metastatic disease and negatively affected by radiotherapy. 9 Actually cfDNA can be detected in healthy normal controls, usually less than 100 ng/mL, while tumor patients generally have 10∼40 fold than that, 10,11 which can be explained by high metabolism and hence increased programed apoptosis in tumor cells. 12 This is further supported by characteristics of shorter DNA fragments (∼180 bp) that are usually accompanied by apoptotic cells. 13 It’s less likely that necrotic cells directly produce shorter plasma cfDNA; although hypoxia is commonly seen in cancer cells, the phagocytosis of resident macrophages and other scavenger cells, nevertheless, release cell components, including fragment DNA into the circulation. 14
Except self-derived, the presence of DNA of cancer-related viruses in peripheral blood also contributes to the diagnosis and prognosis of cancer. In 1999, Lo et al 15,16 reported that the presence of DNA of Epstein-Barr virus (EBV) in patients with nasopharyngeal carcinoma is closely related to disease progression, which is further supported by a study of expanded patient population. 17 Following, this potent group pronounced that circulating EBV DNA could be considered as a potential biomarker for EBV-related gastric carcinoma 18 as well as natural killer/T-cell lymphoma. 19 Except that, EBV can also be used as biomarker for EBV-positive lymphomas such as B-cell, Hodgkin lymphomas and even in immunosuppression situations such as graft-versus-host disease after hematopoietic stem cell transplantation. 20 Other cancer-related viruses include hepatitis C virus (HCV) that was reported to be a surrogate marker for HCV-associated hepatocellular carcinoma. 21 Moreover, it can be used to predict distant metastasis after curative hepatectomy. 22
Mutation and abnormal methylation are important for the onset of cancers. DNA methylation usually occurs at the CpG islands of the promoter of targeted genes. Hypermethylation results in inappropriate transcriptional silencing in tumor suppressor genes and thus various malignancies, 23 while hypomethylation leads to gene mutation and genome instability. 24 So, it’s more valued to detect methylation in cfDNA for risk evaluation in cancer. There was report supporting that hypermethylation of glutathione-S-transferase pi could be identified in early stages of patients with prostate cancer. 25 Other methylated tumor DNAs in serum for evaluating detection of early-stage colorectal cancer are adenomatous polyposis coli protein, 26 septin 9, 27,28 as well as ALX homeobox 4 and 2 follistatin-like domains 2 (TMEFF2). 29 Some tumor suppressor genes such as RAS association domain family 1A and retinoic acid receptor β are not specific to certain types of cancer so the aberrant methylation could be detected in various cancer. Except epigenetic changes, tumor-specific gene mutations contribute to onset and progression of cancers, either. Both epidermal growth factor receptor (EGFR) and KRAS proto-oncogene (KRAS) mutations can be identified noninvasively in patients with lung cancer and B-Raf proto-oncogene (BRAF) mutation in plasma specimens from patients with melanoma. 30,31 Besides, KRAS or BRAF mutations are confirmed in the plasma samples in patients with metastatic colorectal cancer as well. 32,33 Specifically, they also found the mutant cfDNA was mostly of fragments less than 138 bp, differentiated from nonmutant one (138-300 bp). 33 Others also reported that estrogen receptor α (ESR1) mutations are dominant in estrogen receptor–positive patients with metastatic breast cancer and are associated with poor outcomes. 34,35 Except that, PIK3CA mutations can be identified in patients with metastatic breast cancer as well. The concordance (same mutation status in plasma and tumor) can be as high as 80% to 95%, 31,36 which is extremely encouraging. For other cancers such as high-grade serous ovarian carcinomas, the tumor suppressor gene TP53 is commonly considered as a driver mutation. Interestingly, mutated TP53 in plasma can be detected and the sequences reach as high as more than 50%. 37 Surprisingly, in patients with pancreatic cancer, exosome-derived circulating DNAs contain mutated KRAS and p53 with DNA fragments more than 10 kb, proving a new source of cfDNA. 38 The evaluation of cfDNA for pancreatic ductal adenocarcinoma (PDAC) has been well summarized recently. 39 In 2018, Shen et al 40 identified massive tumor-derived differentially methylated regions in plasma between early-stage PDACs and controls and further confirmed tumor-associated transcriptional networks that are abnormally active in patients. The discovery of this new method makes early cancer detection more accurate and effective (Table 1).
A Scheme of Tumor Cell-Free DNA Research Development Associated With Technology.

Abbreviations: BRAF, B-Raf proto-oncogene, serine/threonine kinase; cfMeDIP, cell-free methylated DNA immunoprecipitation and high-throughput sequencing; DMR, differentially methylated regions; EBV, Epstein-Barr virus; EGFR, epidermal growth factor receptor; ESR, estrogen receptor; HCC, hepatocellular carcinoma; HCV, hepatitis C virus; KRAS, KRAS proto-oncogene, GTPase; NK cells, nature killer cells; PCR, polymerase chain reaction; PIK3CA, phosphatidylinositol 3-kinase catalytic alpha polypeptide; TP53, tumor protein p53.
In recent years, there is an emerging assay that addresses the integrity (the ratio of longer fragments to shorter/total DNA) of some noncoding genomic DNA in cfDNA. This is possible because complex source mechanisms of cfDNA from tumor cells besides apoptosis that truncates DNA into small and uniform DNA fragments of 185 to 200 bp. So the longer interspersed nuclear elements (LINEs) as LINE1 to shorter ones can be applied to detect cancers and evaluate progression. 42 For example, ALU integrity was much higher in patients with breast cancer and could be considered to predict metastasis. 43 Currently, these assays are still in starting stage and validation from more researches will be needed to address the clinical utility.
Although cfDNA is advantageous and promising to be a potent biomarker in oncology, there are many factors that may affect the application. In a recent review, 44 these factors are well described, including technological and analytical limitations, sampling noise, the specificity and sensitivity regarding diagnosis, and ambiguity about cancer-specific mutations. However, more attention has been put to the comprehensive utility of cfDNA, that is, to integrate multiple methods together to resolve the uncertainty and ambiguity. In conclusion, it’s becoming promising to detect early-stage tumors by various methods of cfDNA. In the future, combination of different means of cfDNA may be necessary, for instance, integrity coupled with mutation genes or methylation change in cfDNA, to translate liquid biopsy into clinics more successfully.
Fetal cfDNA
The discovery of fetal cfDNA is a little late than tumor cfDNA, but the impact has no less significance than tumor one. In 1997, the finding that fetal DNA is present in maternal plasma and serum opened a new gate for noninvasive prenatal testing (NIPT). 45 After years of researches and studies, first large validation studies of NIPT for trisomies 21, 18, and 13 in high-risk pregnancies reported in 2011 and then commercial tests were launched by companies in Hong Kong/China and the United States. 46 -48 Then clinical validation studies confirmed its positive predictive values with lower false-positive rates regardless of high or low-risk pregnancies. 49,50 This highly positive results may be associated with its shorter half-life, 16.3 minutes in average. Moreover, fetal cfDNA become undetectable since 2 hours till 1 day after delivery, excluding the possibility from previous pregnant carryover. 51 Besides, fetal cfDNA can be distinguished from maternal one by shorter DNA fragments, with a predominant peak of ∼143 bp compared to 166 bp, 52 suggesting that the enzymatic processing of DNA from apoptotic cells is the main source of plasma DNA, especially from placenta trophoblastic cells, which was confirmed by the fact that normal fetal cfDNA could be detected before fetal circulation established 53 and even in pregnancies without a fetus (anembryonic gestation). 54 Therefore, it’s supposed fetal cfDNA would undergo abnormal change in cases of pathological pregnancies, especially those associated with placental dysfunction. Indeed, fetal cfDNA was found to be increased in women with invasive placenta called placenta increta. 55,56 Other situation like preterm birth that is obviously related to placental dysfunction was fetal fraction, which was reported to be elevated as well around early mid-gestation and could be considered as an auxiliary predictive tool, 57 but not in early gestation. 58
Like tumor cfDNA, fetal markers for NIPT provide a variety of tools for clinical prenatal testing. Compared with maternal cfDNA, fetal cfDNA is usually hypomethylated so that extra dose of chromosomes would lead to dilution of total methylation level of target chromosome compared with normal pregnancies. 59 More specifically, in maternal plasma, unmethylated SERPINB5, which is present on chromosome 18, could serve as a fetal-specific marker for detecting a trisomy 18 fetus noninvasively. 60,61 Other genes include PLAC4 gene on chromosome 21 for detecting Down syndrome, 62 as long as the fetus was heterozygous for the single nucleotide polymorphism (SNP) analysis. Moreover, NIPT could be applied to monogenic diseases, like β-thalassemia, which can be detected by targeted genomic regions flanking the HBB gene 63 and congenital adrenal hyperplasia can be approached by flanking CYP21A2. 64 The diagnosis depends on 2 steps, first to determine from which parent the affected fetus has inherited and second to figure out that the excessive maternal haplotype is the one inherited by the fetus. For some monogenic disorders associated with de novo mutations, NIPT becomes available as well such as variant in the COL1A gene accompanied by a fetus with skeletal abnormalities, FGFR3 gene associated with skeletal disorders, NIPBL gene related to Cornelia de Lange syndrome, and splice site variants in TSC2 gene consistent with tuberous sclerosis. 65 Even though mutation genes are widely scattered in case as Duchenne muscular dystrophy, which is a kind of sex chromosome disorder, NIPT can be applied either with the aid of haplotype-assisted strategy. 66
However, most of the clinical validation was carried on singleton pregnancies. Only recently, scholars start to put question mark on NIPT in twin or multiple pregnancies. The earlier application of cfDNA was used to determine zygosity depending on the proportions of apparent fractional fetal DNA concentration which is higher in dizygotic twin pregnancies compared with monozygotic ones. 67 That’s interesting because zygosity plays an important role in twin pregnancies, as well as chorionicity and amnionicity. Nevertheless, it’s also the reason why NIPT is limited in twin pregnancies due to the intrigue factors. It’s reported that NIPT in first trimester achieved higher failure rate in twin pregnancies (9.4%) compared to singleton pregnancies (2.9%). 68 In contrast, Fosler et al 69 published their data in 2016 demonstrating NIPT was highly successful for screening fetal aneuploidy as first-line testing from 2 groups with missing zygosity and chorionicity information. After that a larger cohort study, 70 providing detail chorionicity and amnionicity, claimed the overall specificity for trisomy 21 was as high as 99.8%. It sounds promising. To date, few reports regarding sex chromosome aneuploidy in twin pregnancies can be found, although Milan et al 71 had tried to predict fetal sex in twin pregnancies by NIPT. Summarily, the application of NIPT for singleton pregnancies is more successful to detect aneuploidy, while other congenital diseases are gathering evidence for it to be clinical validated. As in twin or multiple pregnancies, NIPT is of great value, but it waits for more data before it becomes powerful enough.
Factors Affecting Extraction of cfDNA
Since cfDNA could be eliminated by plasma deoxyribonucleases, let alone tumor or fetal cfDNA only account for a small portion of total circulating DNA, some researchers evaluate the possible factors that might have an impact on the stability of cfDNA. A brief report in 2003 claimed that fetal cfDNA concentrations were as stable as 24 hours after collection. 72 That is further extended to 7 days if maternal blood was stored in cell-stabilizing agents containing tubes even at ambient temperature, 73 which is moreover supported by Toro et al 74 who recommended using specific tubes (Streck Cell-Free DNA Blood Collection Tubes [BCT] in their article) to preserve circulating plasma DNA. Similarly, a series of comparison demonstrated tubes containing cell-stabilizing solutions could provide more stable concentration of cfDNA by minimizing nucleated cell disruption during handling, shipping, and storage samples. 74 -76
Traditionally, cell-free DNA is collected from plasma in blood samples. 77 For some instance, cfDNA is obtained through a 2-step centrifuge: the first centrifuge under relatively low speed (2500g for EDTA tubes, 1600g for BCT) is to eliminate cells or similar density particles, the second one with higher speed (15 500g for EDTA tubes, 2500g for BCT) is generally used to get more pure samples. 73 Irrespective of the centrifugal force, contaminating cells that remained in the plasma were reported to be removed after low-temperature storage. 78 Whatever circumstance, cfDNA needs to be purified from final plasma, either through classic phenol–chloroform DNA precipitation method or commercial DNA extraction kits. The advantage of traditional precipitation method is more DNA can be obtained if more input. However, cfDNA is so low in human plasma, which seems not a strong point. Therefore, adaptations based on classical method emerge. One modified method published in 2013 79 proclaimed almost 4-fold output could be obtained from plasma, of either patients with cancer or normal healthy controls, compared with previous phenol–chloroform extraction method. This could be expanded to dozens or even hundreds fold when compared to commercial kits. The method had a minor change in salt concentration when precipitating cfDNA and avoided losing DNA by using a single DNA precipitation.
Although much more cfDNA could be gained by traditional methods, the specificity discounts when found more in healthy controls. To cutoff the time spending on preparing solutions, it’s more convenient and much easier to get cfDNA using commercial cfDNA extraction kits. Kuang et al 80 compared 3 protocols in their study, QIAamp DNA Micro Kit from Qiagen, NucleoSpin Plasma XS (Macherey-Nagel), and Promega Wizard. They found that using NucleoSpin Plasma Kit could get most total cfDNA (0.086 ng/μL compared to 0.064 and 0.021 ng/μL, respectively) while templates from QIAamp DNA Micro Kit could be amplified successfully as high as 100% using 2 independent methods (75% for Promega Wizard and 67% for NucleoSpin Plasma XS). When more kits were compared comprehensively, although the QIAamp Circulating Nucleic Acid Kit remained to be reliable to extract cfDNA from different kinds of plasma, the Norgen Plasma/Serum Circulating DNA Purification Mini Kit seemed to be more superior in more cfDNA yield but less plasma input (200 μL). 81 To a less extent, NucleoSpin Plasma XS Kit yielded satisfying DNA compared to those 2 brands. Contrary to previous reports, almost all of those commercial kits performed better than homemade protocols, except Chemagic DNA Extraction Kit which was probably owing to less initial plasma volume loaded. Nevertheless, the multiple manual steps involved and the relatively fewer loading amounts force scientists to invent a more effective way that is centrifugation-free by automatically integrating those cumbersome procedures. As so generates PIBEX, a new vacuum-driven approach named as Pressure and Immiscibility-Based Extraction, 82 using oil stacking on the elution buffer to differentiate polarity. PIBEX yielded stable output independent of loading volume with better reproducibility compared to that of centrifugation (Figure 1). Nevertheless, neither centrifuge nor vacuum-dependent methods cannot be finished without cumbersome instruments. But a dimethyl dithiobispropionimidate platform can. It’s a microchannel platform based on the principle that the chemical structure of the capture agent is responsible for binding to nucleic acids electrostatically or covalently. 83 Independent of various instruments and procedures, more cfDNA could be purified from colorectal cancer samples within 15 minutes. Above all, all the descriptions here just are a small portion of the emerging cutting-edge technologies. After years, cfDNA purification will be much faster and cost-efficient,

Comparison of mechanisms based on (A) centrifugation, (B) pressure without immiscible solvent, and (C) pressure with immiscible solvent: PIBEX (cited from the study by Lee et al 82 ). Electrical power corresponds to each driving force. For (A) centrifugation, each flow through a pore is independent of the others, and thus, it can be regarded as a set of independent serial circuits. So the captured liquid needs a high g-force to be released from silica membrane due to the surface tension in microscale pore structure. For (B) pressure without immiscible solvent, some pores are easily forced to be opened due to the different magnitude (R), then most of air tends to flow though the opened pores, like an electrically shorted line in a parallel circuit, so not all the residual liquid in the silica membrane can be recovered. Whereas, PIBEX (C) uses mineral oil to differentiate polarity so irregular openings will not occur and hydrodynamic resistance of mineral oil (R0) becomes much higher than that of water (Rn), and thus, Rn can be neglected for total resistance (R0 + Rn ∼ R0). Thus, all of the residual elution buffer will be completely pushed out. In the following steps, the nonpolar solvent as water can be used for later process like polymerase chain reaction or next-generation sequencing with careful selection, while the oil solvent can be used to generate droplets in a droplet digital polymerase chain reaction assay.
Techniques for Quantifying and Analyzing cfDNA
Among various methods that were used to measure cfDNA, polymerase chain reaction (PCR) is widely accepted as standard, which can be further specified. The earlier method used to quantify cfDNA was real-time PCR, 84 which only shows the concentration difference, making it inaccessible for detection of a single-base substitution, insertion, or deletion. To discriminate an amplicon containing the mutant allele versus an amplicon containing the wild-type allele, other modified methods are considered such as fluorescence detection (by labeling difference in fluorescence into corresponding incorporation), direct DNA sequencing of the PCR amplicon, or measuring product lengths for insertion or deletion. 85 Instead, Spindler et al developed a quantitative PCR method to calculate KRAS mutation of traceable cfDNA even in high background of circulating DNA. 32 Shortly later, a method called Intplex, based on allele-specific blocker quantitative PCR, was approached to detect site mutations and concentrations in cfDNA. 33 However, for some diseases, mutations are located throughout the genes so that identification is challenging across sizeable genomic regions spanning entire genes from tiny number of fragmented templates. To address that, tagged-amplicon deep sequencing approach was described, which combines parallel PCR with 15 cycles of 4-minute extension in multiple reactions to capture the starting molecules of aim template, followed by tagging samples with specific barcodes. This approach makes it possible the detection abundant and rare mutations on massive genomic regions. 37
Benefit from recent developments in microfluidics and surfactant chemistries, a method based on water–oil emulsion PCR called droplet digital PCR (ddPCR), seems much advantageous over conventional digital PCR which involves an occasionally onerous process of diluting input DNA into individual wells for analysis. Droplet digital PCR separate the template DNA molecules into thousands of partitions, which serve basically the same function as individual test tubes or wells in a plate in which the regular PCR reaction takes place, although in a much smaller format. Then PCR amplification is carried out within each droplet and labeled with fluorescent hybridization probes followed by reading in an automated droplet flow cytometer. 30,86 The massive sample partitioning is a key aspect of the ddPCR technique. With the aid of ddPCR, liquid biopsy in clinical screening and diagnosis has been widely extended. Now, commercial companies provide systematic service of ddPCR, for instance, BioRad QX200 ddPCR system which makes completing ddPCR in a much faster and cost-effective way (Figure 2).

Illustration of cell-free DNA (cfDNA) analysis using droplet digital polymerase chain reaction (ddPCR), adapted from Bio-Rad QX200 manual guide. Blood is collected peripherally along with other medical care works (for noninvasive prenatal testing or cancer screening), then extract cell-free DNA from plasma. Mix DNA templates and ddPCR reaction mix to generate droplets, followed by regular PCR reaction. The final data could be interpreted by an automated droplet flow cytometer. All the time spent, except sample collection, can be as less as fewer hours.
Unlike cancer, fetal cfDNAs present in maternal plasma rarely mutate, although variants in monogenic disorders have been identified by next-generation sequencing recently. 65 Therefore, the methods to evaluate fetal cfDNA majorly depend on quantitative analysis or deep sequencing. 87 Those approaches depending on barcoding are usually time- and cost-consuming because efforts are needed to take to reduce noise and construct library, which has been summarized well in 2016. 88 Some researchers attempted to read fetal SNP alleles by excluding those that do not exist in mother. 89 For now, scientists are much interested to read the methylation change carried in cfDNA, but due to the traceable fragmented cfDNA, it’s challenging to directly adapt bisulfite conversion on cfDNA which causes huge loss of input DNA. That drives scholars to develop more sensitive approaches to determine plasma DNA methylation profiling. Shen et al developed a new method named as cell-free methylated DNA immunoprecipitation and high-throughput sequencing (cfMeDIP-seq) to enrich CpG islands in cfDNA for analysis, 40,90 by which reading massive methylation profile in cfDNA seems to be possible in a cost-effective and accurate way. The crucial step for cfMeDIP-seq is to use filter DNA, usually exogenous, to increase input DNA template amount. Other brand new approaches that can detect micro-amount DNA methylation include APOBEC-coupled epigenetic sequencing, 91 which depends on enzyme to discriminate cytosine modifications without bisulfite conversion, and TET-assisted pyridine borane sequencing combining the DNA demethylation enzyme and pyridine borane reactions to separate 5 mC and 5 hmC. 92 So far, no data were achieved from cfDNA by these 2 new methods, but one of the key aims for researchers to develop these methods is to sequence peripheral cfDNA for detecting early-stage tumors. Thus, very soon, data from cfDNA got from brand new approaches will be presented.
To sensitize and specify liquid biopsy in screening and diagnosing early-stage diseases, it needs to combine various sorts of biomarkers as well as different technics. One breakthrough about earlier detection was pioneered in 2018 by Cohen et al, 41 which coupled 8 circulating protein biomarkers and 16 tumor-specific mutations in cfDNA. The methodology is called cancerSEEK, which can be applied to identify 8 nonmetastatic, clinically detected cancers of the ovary, liver, stomach, pancreas, esophagus, colorectum, lung, or breast (Figure 3). 93 With as much as 1000 patients and 850 healthy controls, it can reach up to sensitivity of 98% and specificity of 99%. Exceptionally, cancerSEEK can identify the primary tumor to 2 anatomic organs in a median of 83% of these patients and 1 site of 63%. Most importantly, cancerSEEK is a noninvasive test so that it could be administered routinely along with other medical cares. According the latest news, cancerSEEK will be developed by a new company named as Thrive Earlier Detection Corp that launched with $110 million in Series A funding. So it can be envisioned that the test will eventually cost much less to support physicians and patients in catching up the clues before tumors fueled.
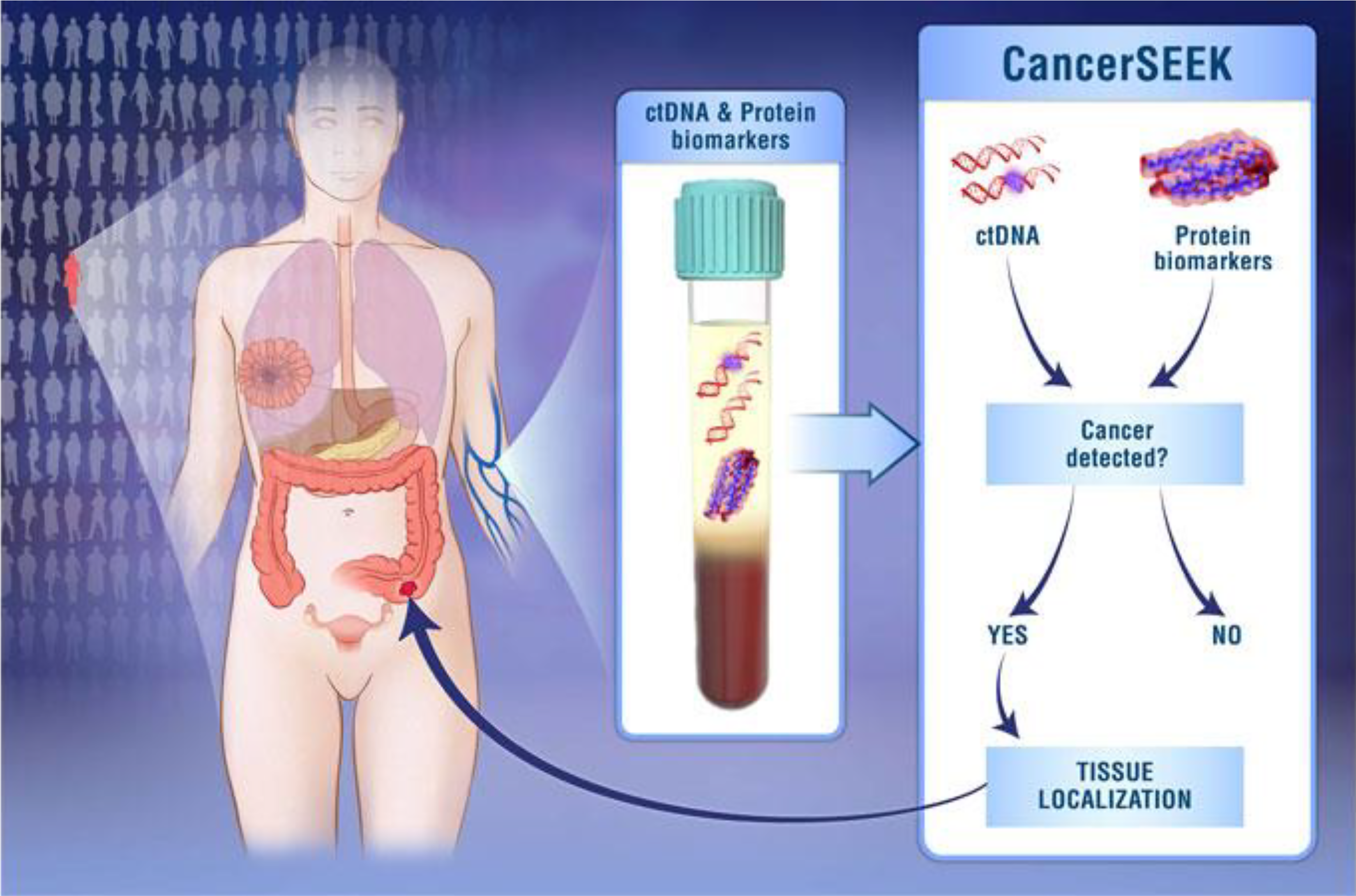
Scheme of cancerSEEK. 93 CancerSEEK combines identifying 2001 mutations in 16 genes commonly observed in different types of cancers from cfDNA and 8 cancer-associated proteins to screen 8 common cancer types: breast, lung, colorectal, ovary, liver, esophagus, pancreas, and stomach cancer, making it possible to locate tissue of origins so as to screen early tumors in large population.
Conclusion
Diagnosis of early-stage diseases has pivotal significance to improve prognosis. Few existing testing methods, however, can catch up with the traceable clues before sickness spreads. That’s why so many generations have worked so hard to exploit new and more effective ways of screening illness as early as possible. Cell-free DNA has been shown to be a useful and encouraging tool for clinical diagnosis for cancer to find in situ carcinomas before metastasis and fetal medicine to improve birth healthy qualities, providing a potential prospect for future medicine. Except fetal cfDNA that has been well applied to NIPT clinically, tumor cfDNA remains uncertain due to the requirements upon extreme high sensitivity and specificity. However, along with the deep exploration of cfDNA, new orientation has been aroused with regard to cfDNA-associated proteins, generally histones and transcriptional factors, which can be used to infer tissues of origin. 94 As so the noninvasive screening in oncology will be much precise and reliable. In fact, epigenetics plays an equal important role in pregnancy as well. If exploration of cfDNA binding proteins can be applied, and even fetus inherit normal genes, the functional proteins expression may be different. Thus, NIPT can be used to assess difference in proteins besides genes. That may facilitate the utilization of cfDNA in twin pregnancies to discriminate the inconsistence between the 2 babies who are supposed to harbor the same genetic information. Recently, there are reports focusing on enhancers in tumor cfDNA to marker tumor origin, 95 since enhancers could potentially serve as targets of cancer therapy. It’s boldly envisioned that cfDNA may be considered as a powerful carrier for genetic treatment once in vivo targeting becomes surmountable. In the next decades, cfDNA research would be more comprehensive, combining epigenetics, proteomics, and genomics together to enable noninvasive screening and diagnosis more competent. Moreover the development of technology and microchip would further minimize the facilities. When it comes to the time, cell-free DNA detection would be widely accepted as commercial kits, much similar to what is prevalent now such as gene detection kits. People who benefit from cell-free detection kits might be capable to buy kits over-the-counter and complete it using few drops of blood within minutes. Summarily, convenient, noninvasive, repeatable as it is, cell-free DNA provides enormous merits that lead itself to be an imperative tool for health-care providers to grasp the best therapeutic chance and to ameliorate livings.
Footnotes
Authors’ Note
Fan Jiang and Xiaoxiao Yang contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.