
Abstract
Lower body positive pressure (LBPP) treadmill activity might benefit patients with heart failure (HF). To determine the short-term effects of LBPP on left ventricular (LV) function in HF patients, LV ejection duration (ED), a measure of systolic function was prospectively assessed in 30 men with stable HF with LV ejection fraction ≤ 40% and 50 healthy men (N). Baseline measurements (100% body weight), including blood pressure (BP), heart rate (HR) and LVED, obtained via radial artery applanation tonometry, were recorded after 2 minutes of standing on weight support treadmill and after LBPP achieving reductions of 25%, 50%, and 75% of body weight in random sequence. Baseline, HR, and LVED (251 ± 5 vs 264 ± 4 ms; P = .035) were lower in the HF group. The LBPP lowered HR more (14% vs 6%, P = .009) and increased LVED more (15% ± 7% vs 10% ± 6%; P = .004) in N versus HF. Neither group had changes (Δ) in BP. On generalized linear regression, the 2 groups showed different responses (P < .001). Multivariate analysis showed %ΔHR (P < .001) and HF (P = .026) were predictive of ΔED (r 2 = 0.44; P < .001). In conclusion, progressive LBPP increases LVED in a step-wise manner in N and HF patients independent of HR lowering. The ΔLVED is less marked in patients with HF.
Keywords
Introduction
Despite technical advancements in cardiac imaging, there are significant pitfalls in assessment of left ventricular (LV) contractility. Major limitations of assessing and monitoring LV systolic function include load dependence of commonly used indices and the reliance on invasive techniques. 1 –3 Applanation tonometry is a portable noninvasive technology that is capable of providing high fidelity recordings of the aortic waveform from which systolic ejection duration (ED) can be calculated. 4,5 Left ventricular systolic ED is the duration of systolic ejection in milliseconds and is a reproducible measure of systolic performance. In general, LV ED is shortened in the presence of LV systolic dysfunction and correlates with LV stroke volume. 5 –10 Recently, LV ED determined by radial artery pulse wave analysis via applanation tonometry has been shown to be predictive of all-cause mortality. 11 Applanation tonometry provides a noninvasive portable method to determine LV ED responses to varying preload.
Lower body (LB) positive pressure (PP) treadmills are used to rehabilitate orthopedic and neurological patients because they consist of a pressurized chamber that temporarily reduces the effective weight of the person walking on it. 12 –14 Weight support (WS) treadmills could potentially benefit patients with heart failure (HF) with limited exercise tolerance in whom LV contractility is of concern. However, responses of LV ED to alterations in preload with the use of these treadmills have not been studied. Applanation tonometry allows the opportunity to noninvasively assess preload induced alterations in LV contractility with the use of the WS treadmill. Accordingly, the objective of this study was to evaluate the short-term effects of increased preload using the LBPP treadmill on LV ED in normal patients compared to patients with HF with reduced EF. Specifically, we hypothesized that progressive LBPP would increase LVED less in the HF group.
Materials and Methods
We prospectively studied the effects of LBPP on LV ED in 30 clinically stable men with HF and 50 healthy men (N) without known cardiovascular risk factors or disease. The HF group was recruited from an outpatient clinic and met inclusion criteria if they carried a prior diagnosis of HF with an LV ejection fraction ≤ 40% by an imaging method, and were clinically stable for the prior 4 weeks as evidenced by stable symptoms and medications. All participants had adequate radial pulses for applanation tonometry and were in sinus rhythm. The institutional review board approved this study and participants provided written consent. Medications were not withheld for study purposes.
Procedures
Baseline measurements (100% body weight) were recorded after 2 minutes of standing on the WS treadmill (AlterG Anti-Gravity Treadmill, Alter G, Fremont, California). Brachial artery (BA) systolic and diastolic blood pressures (BPs) were measured by use of an automated blood pressure cuff (Omron HEM-780, Schaumburg, Il) around the left upper arm. Baseline radial artery applanation tonometry using SphygmoCor (AtCor Medical, Sydney, Australia) was performed to obtain aortic waveform and baseline pulse wave analysis measurements on the participant’s outstretched arm stabilized and resting on the treadmill rail. 4 The weight of each subject was covertly measured by the treadmill. Lower body positive pressure was then applied to achieve reductions of 25%, 50%, and 75% of body weight in random sequence. After 2 minutes, BP and arterial tonometry measurements were repeated on the same arm. The degree of WS was adjusted to study levels in random order immediately after the measurements were obtained, without a rest period. Brachial artery mean arterial pressure (MAP) was calculated as diastolic BP +1/3 pulse pressure.
Determination of Left Ventricular Ejection Duration
Radial artery pressure waveforms were recorded at the wrist with the applanation tonometer according to previously published methods. 4 In brief, the aortic pressure waveform was derived from the radial artery waveform by a previously validated generalized transfer function. 15,16 The systolic duration of the reflected pressure wave was determined from the inflection point to the incisura and represents LV ED. 4 In 10 men LV ED measurements were repeated to assess repeatability. The intra-class correlation coefficient was 0.99. Others have reported an inter-observer variability of 0.3 ± 3.3%. 5
Results
Subject Characteristics and Comparative Responses
Participant’s baseline characteristics are shown in Table 1. Lower body positive pressure lowered HR more prominently in N versus HF group (14% ± 12% vs 6% ± 8%, P = .009, Figure 1). Lower body positive pressure did not change peripheral or central BPs in either group (P = ns). Lower body positive pressure increased LV ED more markedly in N versus HF group (15% ± 7% vs 10% ± 6%, P = .004). As shown in Figure 2, both the N and HF groups showed a stepwise increase in ED with increasing LBPP, however generalized linear model analysis demonstrated the HF group had a less marked increase after adjusting for age and HR at each stage (P < .001). These results did not change after adding mean arterial pressure at each stage into the model. Since the HF group was older than the N group, we performed an age matched subgroup analysis (n = 12 in each group), which demonstrated a similar pattern of increasing LV ED in the 2 groups (9% ± 7% vs 16% ± 5%, P = .006). Changes in LV ED correlated with percent change in HR (r = 0.63, P < .001). On multivariate analysis, both percent change in HR (P < .001) and HF (P = .026) were predictive of change in ED (r 2 = 0.44, P < .001). All but 2 patients in the HF group were taking β blockers so it was not possible to assess the effects of β blockade. With regard to β blocker dose, we divided the patients with CHF taking β blockers into high and low dose groups. The high group consisted of patients taking a carvedilol dose >25 mg daily or equivalent (n = 9) and the low dose group (n = 15) were taking <25 mg/day. Mean ED changes were similar between the 2 groups (10.9 ± 4.27 ms vs 11.4 ± 6.01 ms, P = .80).
Baseline Characteristics of the Study Groups.
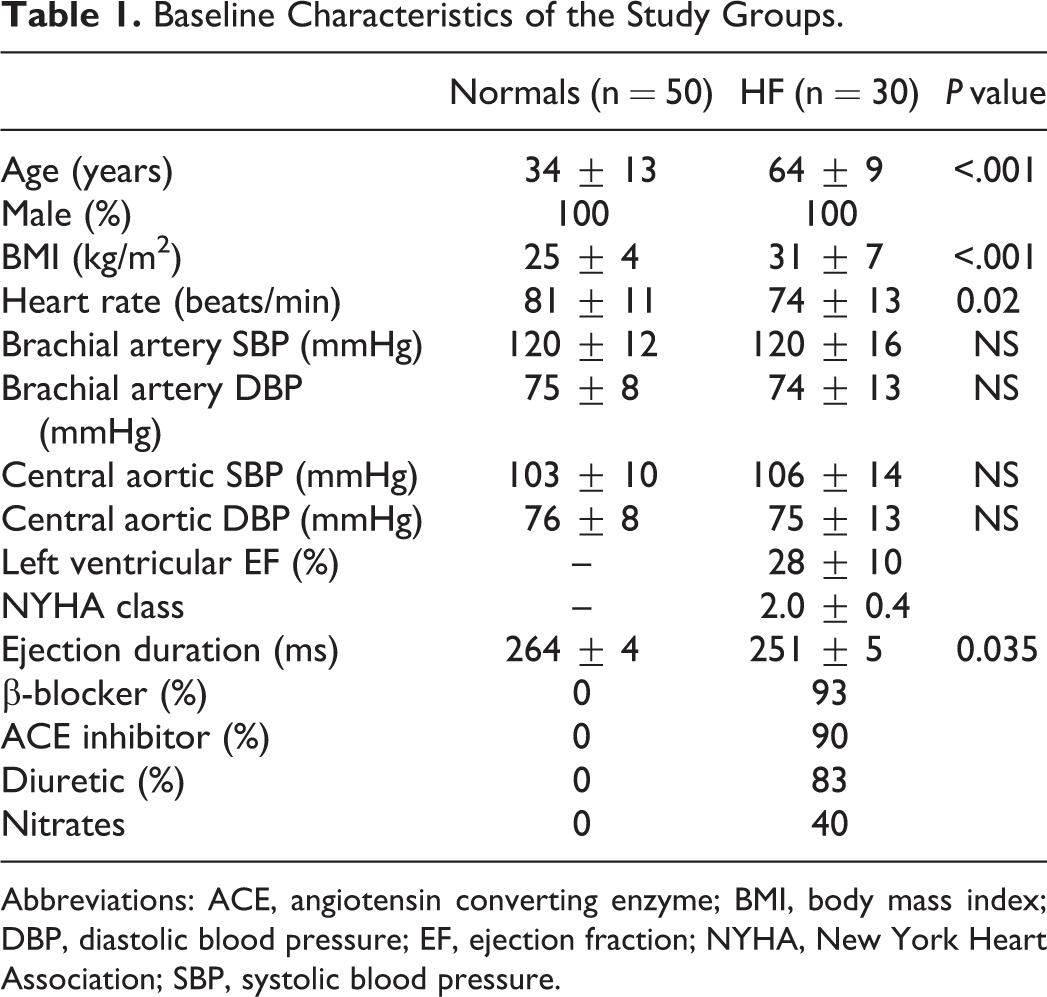
Abbreviations: ACE, angiotensin converting enzyme; BMI, body mass index; DBP, diastolic blood pressure; EF, ejection fraction; NYHA, New York Heart Association; SBP, systolic blood pressure.

Changes in heart rate induced by LBPP in the N and HF groups. HF indicates heart failure; LBPP, lower body positive pressure; N, healthy men.

Changes in LV ED induced by LB PP in N and HF groups. ED indicates ejection duration; HF, heart failure; LBPP, lower body positive pressure; LV, left ventricular.
Discussion
Main Findings
This study compared LBPP induced changes with the use of the WS treadmill in LV ED in patients with and without HF. The major finding was that LBPP increased the duration of LV ejection in a dose response manner in both groups, with the HF group exhibiting a less marked LV ED prolongation. We found LBPP to lower HR in both groups, and although the increase in LV ED correlated with percent HR change, the association of LBPP with LV ED persisted after adjustment for HR changes.
Chronotropic Responses
The HR decline in response to LBPP is consistent with prior studies and is likely related to centripetal blood transfer causing baroreceptor activation and increased parasympathetic activity. 17 –20 Evans et al found that standing at reduced bodyweight suppressed indexes of sympathetic control of heart rate. 20 Less prominent LBPP induced HR lowering observed in the HF group was likely related to depressed baroreceptor function, which is well known to accompany HF. 21 In addition, since resting HR was lower in the HF group, likely due to treatment with β blocking drugs, less of an absolute decline was needed to reach the nadir HR. Moreover, the association of HR lowering with LV ED prolongation is consistent with and expands older studies showing LV ED is directly related to resting HR. 6,8,10
Significance of Prolongation of Left Ventricular Ejection Duration
In addition to HR lowering, LBPP increases in LV ED are likely related to increased forward stroke volume resulting from higher preload due to the increase in intrathoracic volume. Consistent with this notion, LBPP is well known to augment venous return causing intravascular volume to redistribute more centrally. 17 –19,22 Earlier studies established stroke volume as an important determinant of LV ED. 6,10 Previous studies have utilized the preload recruitable stroke work relation, which plot stroke work as a function of end-diastolic volume. 23 –25 This relation is experimentally linear and its slope reflects left ventricular contractility. 26 The preload recruitable stroke work relation has been suggested to more accurately reflect contractile reserve of the intact heart than the Frank-Starling curve. 26 Given that stroke work is calculated as the product of stoke volume and arterial pressure and that arterial pressure was unchanged, the LBPP–LV ED relation likely reflects LV function and may be similar to the concept of the preload recruitable stroke work. Lower body positive pressure did not significantly affect central and peripheral BP in either group, which may relate to the opposing effects of increased blood flow and arterial vasodilation on BP. The finding of LV ED prolongation is similar to results obtained with head out of water immersion, which is also known to centralize blood volume and to increase LV ED. 27
Use of Lower Body Positive Pressure Treadmill
Lower body (LB) positive pressure (PP) treadmills are used to rehabilitate orthopedic and neurological patients because they consist of a pressurized chamber that temporarily reduces the effective weight of the person walking on it. 12 –14 Lower body positive pressure lowers musculoskeletal strain and load, compresses the lower body and increases intrathoracic volume. 17 –19,22 In general, such systems consist of a computer-controlled treadmill equipped with a pressurized air chamber that generates a vertical upward force directly opposing the force of gravity and effectively decreasing body weight. The airtight chamber is formed by neoprene shorts that zip around the waist, and form a kayak type skirt from the waist down. This chamber suspends the subject over the treadmill surface upon inflation. Variable degrees of WS can be achieved by pumping greater air pressure as WS is proportional to the level of lower body PP. Weight support treadmills could potentially benefit heart failure patients with limited exercise tolerance in whom LV contractility is of concern.
Weight support treadmills also provide an opportunity to vary venous return, which is required to determine the end-systolic pressure volume relation (ESPVR), the gold standard measure of LV contractility, as it is relatively load-independent. 3,28,29 Measurement of ESPVR generally requires catheterization of the LV with a high-fidelity pressure catheter and preload reduction with a balloon catheter placed in the inferior vena cava to obtain the ESPVR slope from individual pressure volume curves. 3 A rightward shift of the ESPVR indicates a negative inotropic effect whereas a leftward shift shows a positive inotropic effect. The procedure is invasive and requires specialized equipment to record LV pressure and volume simultaneously 28 and since it is performed in the supine position, the ESPVR may not be representative of hemodynamic changes that occur while upright. Accordingly, the combination of LBPP and applanation tonometry measured LV ED may offer a method to assess LV contractility relative to preload reserve.
Limitations
These results are limited to the acute short-term effects of LB WS in men. We studied only men to limit gender as a confounding variable. The HF group was older than the N group, thereby necessitating adjustment for age. Although there exist formulas by which to correct LV ED for HR, they were not used since the original validation studies did not include patients taking β blockers contrary to our HF patients and did not assess relations between changes in HR and changes in LV ED. 6 Given that the vast majority of HF patients were treated with β-blockers and ACE inhibitors/angiotensin receptor blockers, it was not possible to determine medication effects on the LBPP–LV ED relation. Specifically, all but 2 patients in the HF group were taking β blockers, it is difficult to know the effects of β blockade. However, we were able to divide the patients taking β blockers into low and high dose groups and found similar changes in mean LV ED between the 2 groups. With regard to β blocker dose, we divided the patients with CHF taking β blockers into high and low dose groups. The high group consisted of patients taking a carvedilol dose >25 mg daily or equivalent (n = 9) and the low dose group (n = 15) were taking <25 mg/day. Mean ED changes were similar between the 2 groups: 10.9 ± 4.3 ms versus 11.4 + 6.0 ms, P = .80.
Conclusion
It is concluded that progressive LBPP with the use of the WS treadmill increases LV ED in a step-wise manner in N and HF patients independent of decreases in HR. This increase is less marked in patients with HF. The clinical importance of the change in LV ED in patients with HF during resting WS with these treadmills, and whether this varies among patients and reflects myocardial reserve is unknown. The combination of LBPP and applanation tonometry measured LV ED may offer a method to assess LV contractility relative to preload reserve, as the technique may provide a measure similar to the LV end diastolic volume–stroke work relation. Thus, LBPP treadmills may provide a noninvasive method to assess LV contractility. The effect of LBPP supported exercise on LV ED during is also unknown and may provide further information regarding LV contractility.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by an equipment grant by AlterG Inc. Fremont, CA. The sponsor provided an equipment grant without any input or influence into specific research questions or objectives conducted with the lower body positive pressure treadmill. The sponsor had no involvement in study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.