
Abstract

Background
The first analysis of long-term exposures to air pollution and risk of mortality using the American Cancer Society Cancer Prevention Study II (ACS CPS-II) cohort was published in 1995. 1 Subsequently, extensive independent reanalysis 2 and multiple extended analyses 3 -7 were conducted. These studies have consistently demonstrated that exposure to fine particulate matter air pollution (PM2.5) is associated with increased risk of mortality, especially cardiopulmonary or cardiovascular disease mortality. A recent analysis by Enstrom, based on early data from the ACS CPS-II cohort, reports no significant relationship between PM2.5 and total mortality. 8 The author asserts that the original analyses, reanalyses, and the extended analyses found positive PM2.5–mortality relationships because of selective use of CPS-II and PM2.5 data.
Expanded Analyses of the ACS CPS-II Cohort
The assertion regarding selective use of the CPS-II and PM2.5 data is false. The scope of analyses of the ACS CPS-II cohort conducted over more than 2 decades were explicitly expanded over time to characterize population health risks of PM2.5 in more detail and with greater accuracy. Table 1 provides an outline of key published studies of this expansive body of air pollution research. The highlights of the obvious progress made during the course of these studies include the following: increased mortality follow-up from 7 to 22 or 26 years; increased number of participants included in the analyses from approximately 295 000 to 670 000; increased number of deaths (a key determinant of study power) included in the analyses from approximately 21 000 to 237 000; improved assessment of PM2.5 exposures (and exposures of co-pollutants) from metro-level averages for cities with air pollution monitoring to modeled PM2.5 exposures at geocoded residential addresses throughout the United States; and improved statistical models, including improved control for individual and ecological covariates, and better representation of spatial patterns in the data.
Overview of Key Studies of Particulate Matter Air Pollution and Risk of Mortality Using the ACS CPS-II Cohort.
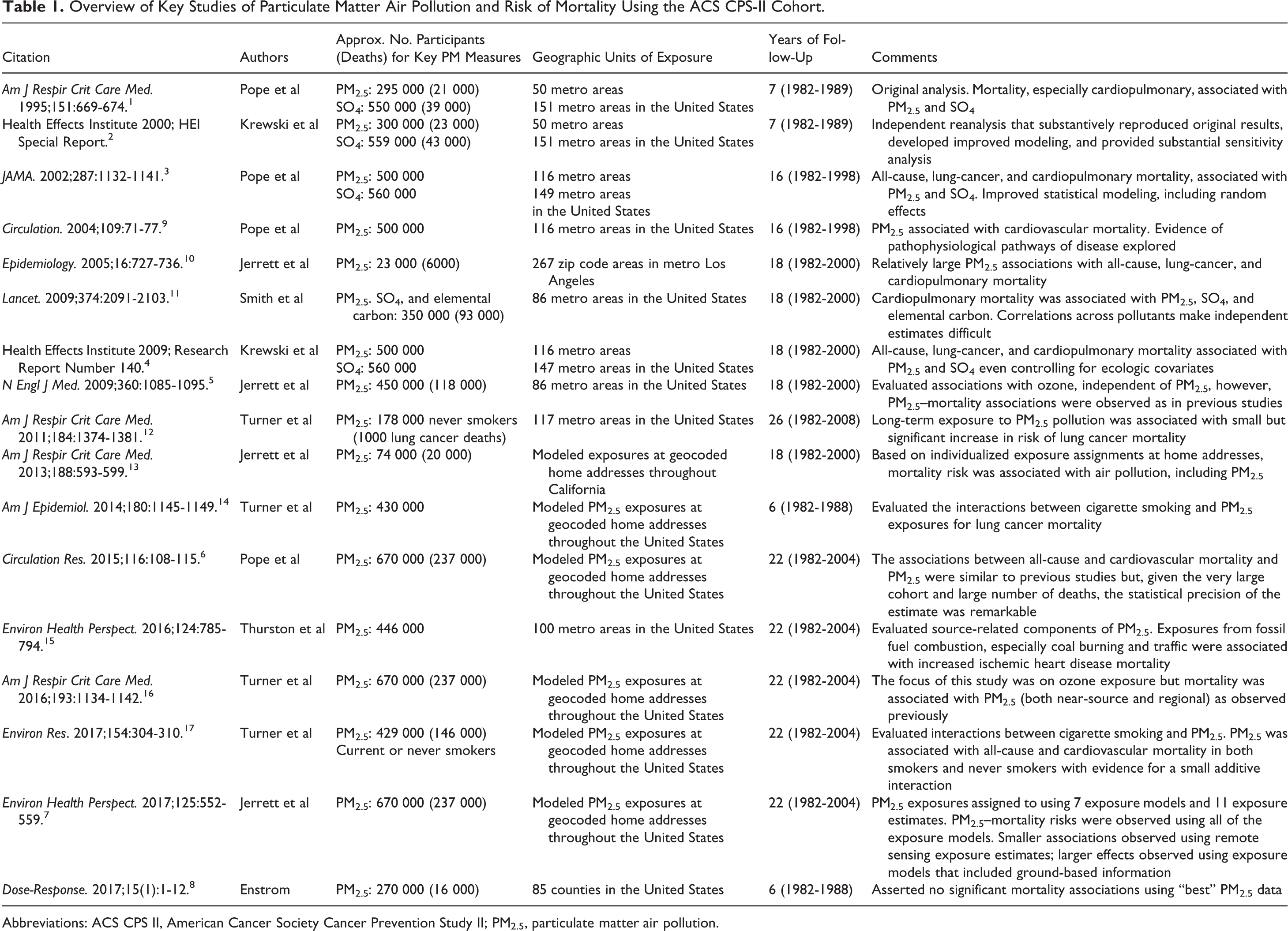
Abbreviations: ACS CPS II, American Cancer Society Cancer Prevention Study II; PM2.5, particulate matter air pollution.
As shown in Figure 1, estimates of the percentage increase in mortality risk per 10 µg/m3 increase in PM2.5 for all-cause and for cardiovascular disease mortality from studies using the ACS CPS-II cohort have been remarkably consistent across the expanded analyses over the last 20+ years. The recent analysis by Enstrom 8 shows an estimated PM2.5–mortality association that is smaller than observed in the original analysis, the reanalysis, multiple subsequent extended analyses, or meta-analyses of studies throughout the world. 18

Nationwide estimates of percentage increase in mortality risk per 10 µg/m3 increase in PM2.5 from various published studies using the ACS CPS-II cohort (indicated by circles) with comparison estimates from meta-analysis of the literature (indicated by diamonds). The size of the circles is relative to the length of the follow-up period. Gray and white circles indicate metro-level and county-level geographic units of exposure, respectively. Black circles indicate that exposures were modeled at geocoded residential addresses. Asterisks indicate that, in addition to controlling for individual covariate, the models also controlled for ecological covariates. Note. (1) Krewski et al 2 report the results of an independent, confirmatory reanalysis of the ACS cohort organized by the Health Effects Institute. (2) In the investigation of alternative measures of PM2.5 conducted by Jerrett et al, 7 the highest quality models (those with the lowest AIC) produced the highest risk estimates; remote sensing models with no ground-based data produced the lowest risk estimates, likely because of greater exposure misclassification. (3) The lowest risk estimate reported by Enstrom 8 is based on a dated and short follow-up of the ACS cohort and is likely subject to exposure mismatching. ACS CPS II indicates American Cancer Society Cancer Prevention Study II; PM2.5, particulate matter air pollution.
Deficiencies in Enstrom’s Reanalysis
Enstrom’s recently published analysis 8 is the least advanced analysis of the ACS CPS-II cohort to date (see Table 1). The Enstrom’s analysis uses a data set with a shorter follow-up period, fewer participants, and fewer deaths than any previous PM2.5–mortality analyses that used the CPS-II cohort, including the original 1995 analysis. He controls for a relatively limited number of individual-level covariates and does not control for any ecologic covariates. Moreover, the key deficiency in the Enstrom’s reanalysis is the absence of advanced modeling approaches for exposure assessment that have been developed over the last 2 decades. Estimates of PM2.5–mortality associations are affected by the quality of the PM2.5 data and the accuracy of matching participants and exposures. In a recent analysis, 7 we evaluated PM2.5 exposures using multiple exposure assessment methods. Figure 1 illustrates that there were significant PM2.5–mortality risk associations for all PM2.5 measures, but the associations were lower for the presumably less accurate measures that used remote sensing without ground-based data. Based on measures of model quality, the PM2.5 exposure values that best fit (lowest Akaike Information Criteria, AIC) the data resulted in relatively larger PM2.5–mortality associations (see Figure 1). In contrast, Enstrom 8 asserts that he estimates smaller PM2.5–mortality associations because he uses the “best” PM2.5 data. He provides neither evidence in support of this assertion nor any measures of the relative quality of models using alternative PM2.5 data. It is not clear how or why his “IPN” PM2.5 data differ from the “Health Effects Institute” PM2.5 data—especially given that these data come from the same monitoring network.
Furthermore, Enstrom’s PM2.5 exposure assessment is likely subject to greater exposure misclassification because of inadequate assignment of geographic units of exposure. Although other published ACS CPS-II studies assigned geographic areas of exposure based on participants’ residence information, the Enstrom’s analysis used the ACS Division and Unit numbers to assign PM2.5 exposures (see letter from ACS). The ACS Division and Unit numbers, however, were for the ACS volunteers that recruited the participants. These volunteers did not always live in the same area or even in the same state as the participants. Enstrom does not document the extent of this participant-exposure mismatching, but it has the potential for substantial exposure misclassification and resultant attenuation bias. Our published research using the ACS CPS-II data is based on participant-exposure matching that is accurate, includes highly spatially resolved exposure models, and utilizes ground-based monitoring and land use data.
An inexplicable deficiency of the Enstrom’s article is its inadequate documentation of the relevant and extensive peer-reviewed literature. References provided in the article largely include an unconventional mix of unpublished and non-peer-reviewed correspondence (including letters, e-mails, and transcript of a teleconference call), presentation slides, press releases, and a compilation of manuscript rejections. Key published extended analyses of the ACS CPS-II cohort, 3,5,6,7,9 -17 studies of other cohorts, 18 -31 or even major reviews and evaluations of the literature 32,33 are not cited or discussed.
Broader Evidence
The PM2.5–mortality associations observed from the various analyses of the ACS CPS-II cohort are consistent with a much broader body of evidence from other studies. As examples, these include studies of other cohorts from the United States 19 -26 Europe, 27 -29 and Canada. 30,31 In addition, meta-analytic estimates of the PM2.5–mortality associations based on a 2013 meta-analysis of the overall literature 18 are also provided for comparison purposes in Figure 1.
Previous studies of the ACS CPS-II cohort consistently demonstrated PM2.5–mortality associations with cardiovascular mortality. 7,9 There has also been substantial work in exploring and understanding the biological pathways and mechanisms linking PM2.5 exposures and cardiovascular disease and death. 32 -35 Similarly, the ACS CPS-II cohort has demonstrated PM2.5–mortality associations with lung cancer mortality, 3,12,14 and recently, the International Agency for Research on Cancer concluded, based on multiple sources of evidence, that particulate matter in outdoor air pollution is a cause of human lung cancer (group 1). 36 Enstrom 8 presents no results for cardiovascular or lung cancer mortality and largely dismisses the substantial and growing literature regarding relevant pathophysiological pathways and related biological mechanisms.
The Global Burden of Diseases, Injuries, and Risk Factors Study 2015 (conducted by the Institute for Health Metrics and Evaluation) identified ambient PM2.5 air pollution as the 5th leading risk factor for global mortality, contributing to approximately 4.2 million deaths in 2015. 37,38 These results are based on recent and comprehensive estimates from ACS CPS-II cohort studies and 23 other peer-reviewed studies of long-term exposure to PM2.5 and mortality from cause-specific cardiovascular and respiratory disease and lung cancer. These results underscore the importance of PM2.5 as a substantial determinant of mortality in the general population. Consequently, these results also suggest substantial health benefits from further reductions in ambient air pollution.
In summary, we welcome thoughtful criticism of our research. But the study by Enstrom does not contribute to the larger body of evidence on the health effects of PM2.5, as it does not utilize adequate approaches for exposure assessment, suitable methods for linking participants to exposure, and sufficient statistical control for potential confounding factors and fails to recognize the larger body of evidence on PM2.5 exposure and disease risk.
Footnotes
Declaration of Conflicting Interests
The author(s) provided the following declaration of interests with respect to the research, authorship, and/or publication of this article: Daniel Krewski reports to serving as Chief Risk Scientist and CEO at Risk Sciences International (![]() ), a Canadian company established in 2006 in partnership with the University of Ottawa conducting work in air quality risk assessment for both public and private sector clients. He also holds an Industrial Research Chair in Risk Science under a peer-reviewed university–industry partnership program administered by the Natural Sciences and Engineering Research Council of Canada, which involves methodological research in air pollution risk assessment. He also recently served as Chair of the US Health Effects Institute Diesel Epidemiology Panel, which conducted an evaluation of recent epidemiological evidence on quantitative risk assessment of diesel emissions and lung cancer. Michelle C. Turner reports personal fees from ICF Incorporated, LLC, outside this work.
), a Canadian company established in 2006 in partnership with the University of Ottawa conducting work in air quality risk assessment for both public and private sector clients. He also holds an Industrial Research Chair in Risk Science under a peer-reviewed university–industry partnership program administered by the Natural Sciences and Engineering Research Council of Canada, which involves methodological research in air pollution risk assessment. He also recently served as Chair of the US Health Effects Institute Diesel Epidemiology Panel, which conducted an evaluation of recent epidemiological evidence on quantitative risk assessment of diesel emissions and lung cancer. Michelle C. Turner reports personal fees from ICF Incorporated, LLC, outside this work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The American Cancer Society funded the creation, maintenance, and follow-up of the Cancer Prevention Study II cohort. C. Arden Pope was funded by the Mary Lou Fulton Professorship, Brigham Young University. Daniel Krewski is the Natural Sciences and Engineering Research Council of Canada Chair in Risk Science at the University of Ottawa.