
Abstract
Persistent racial disparities underscore the disproportionate burden of poor health among Black men in the United States. Black men also use health care services less often, yet gaps remain in the literature on racial differences in health care utilization patterns. The objective of this study was to examine potential race differences in health care service utilization, specifically whether they had at least one office-based provider visit during the year between Black and White men. Data from the 2022 Medical Expenditure Panel Survey were used, consisting of a sample of 5,921 men (4,837 non-Hispanic White and 1,084 non-Hispanic Black). The dependent variable, health care utilization, was based on the aggregated 2022 annual total of office-based provider visits and was coded as a binary indicator of whether the respondent had at least one visit during the year. Race and ethnicity were based on respondents’ self-reported race and whether they identified as Hispanic, Latino, or of Spanish origin. Approximately 73 percent of the men had at least one office-based provider visit during the year, and 18 percent of the sample were NHB men. After adjusting for covariates, NHB men had a lower prevalence of having an office-based physical annual visit during the year (prevalence ratio = 0.83, 95% confidence interval [0.77, 0.88]) than NHW men. This difference may reflect medical mistrust and other health care system barriers rooted in historical and ongoing discrimination against Black men, which limits access to care. These findings underscore the need to address the root causes of barriers to health care utilization among Black men.
Introduction
Persistent racial disparities in health outcomes remain one of the most pressing public health challenges in the United States (Decoteau et al., 2025; Macias-Konstantopoulos et al., 2023). These inequities are particularly pronounced among men, with Black men experiencing disproportionately high rates of diabetes, hypertension, firearm injuries, and other adverse health outcomes across multiple domains (Macias-Konstantopoulos et al., 2023; National Academies of Sciences et al., 2017). Reflecting these patterns, the health of Black men consistently ranks at or near the lowest across nearly all population subgroups in the United States (Gilbert et al., 2016). Recent Centers for Disease Control and Prevention (CDC) data indicate that the age-adjusted death rate among Non-Hispanic Black (NHB) men is 1,263.3 deaths per 100,000, compared with 971.9 among Non-Hispanic White (NHW) men, highlighting a substantial life expectancy gap with broad implications for population health and health care systems (Murphy et al., 2023). Understanding the persistence of these disparities requires examining not only biological and social determinants of health but also differences in health care access and utilization (Powell et al., 2019).
Although the Affordable Care Act narrowed racial gaps in insurance coverage, disparities in health care access and utilization between Black and White men persist (Courtemanche & National Bureau of Economic Research, 2019; Gong et al., 2022). Black men remain less likely to have a usual source of care, underutilize preventive services, and report higher levels of unmet medical need compared with White men (Artiga et al., 2015; Courtemanche & National Bureau of Economic Research, 2019; Ndugga et al., 2024). These patterns are shaped by structural and contextual factors, such as medical mistrust, stereotype threat, experiences of discrimination, socioeconomic disadvantage, and residential segregation, all of which influence engagement with the health care system (Arnett et al., 2016; Aronson et al., 2013; Hammond et al., 2010; Wallace et al., 2022). As a result, Black men are more likely to delay care, rely on emergency departments, and miss opportunities for early detection and management of chronic conditions, contributing to persistent disparities in morbidity and mortality (Arnett et al., 2016; Wallace et al., 2022).
A growing body of research further suggests that gendered and racialized dynamics intensify these utilization gaps (Powell et al., 2019). For Black men, mistrust of medical institutions, negative prior health care encounters, and cultural norms surrounding masculinity may reduce engagement with preventive, routine, and mental health services (Blumberg et al., 2015; Parker et al., 2017; Powell et al., 2019). Even when insured, Black men are less likely than White men to participate in routine screenings, establish continuous relationships with health care providers, or seek care through formal health information channels (Chandler et al., 2021; Jordan et al., 2024). Taken altogether, these findings suggest that disparities in health care utilization among Black men cannot be explained by insurance coverage alone but are rooted in broader structural and sociocultural processes.
To situate these patterns within a well-established framework for health care access and utilization, this study draws on the Andersen Behavioral Model of Health Services Use (1968, 1995) to examine racial/ethnic differences in health services utilization between NHB and NHW men. Developed to explain how and why individuals use health services, assess inequities in access, and inform policies that promote equitable care, Andersen’s model proposes that health service use is shaped by three key components: predisposing factors, enabling factors, and need factors (Andersen et al., 1968, 1995). Predisposing factors include demographic, social, and health belief characteristics that influence the likelihood of seeking care. Enabling factors reflect the personal, family, and community resources that make health care use possible, including income, insurance, a usual source of care, social relationships, and the availability of services. Need factors refer to both perceived health status and professionally evaluated illness or functional impairment that indicate the necessity for medical care. Under this framework, racial/ethnic differences in health care service use between NHB and NHW men reflect differences in predisposing factors, enabling factors, and need factors that facilitate or impede access to and use of care.
Despite this growing body of evidence, relatively few studies have explicitly examined racial differences in health care utilization patterns between Black and White men. Accordingly, the objective of this study was to examine potential race differences in health care service utilization, specifically whether they had at least one office-based provider visit during the year between Black and White men after adjustment for multiple health-related predisposing factors, enabling factors, and need factors. By focusing on men and comparing annual office-based provider use across racial groups, this study aims to clarify utilization patterns that may contribute to persistent racial health disparities.
Method
Data and Study Population
The Medical Expenditure Panel Survey (MEPS), conducted by the Agency for Healthcare Research and Quality (AHRQ), provides nationally representative data for the U.S. civilian noninstitutionalized population on health care use, cost, and health insurance coverage. The Household Component (HC) of MEPS collects data through several rounds from families and individuals that were sampled from a broader superset of households that had participated in the National Center for Health Statistics (NCHS) National Health Interview Survey (NHIS) in the prior year (Agency for Healthcare Resources and Quality, 2019) Healthcare R. In the 2022 MEPS HC (HC-243) survey, 22,431 persons participated in one of the three panels where data was collected on demographic and socioeconomic characteristics, health characteristics (i.e., condition, utilization, access to care), and insurance coverage and expenditures (Agency for Healthcare Research and Quality, 2024).
Of the 17,909 adults aged 18 years and older, 8,255 were men. We excluded 2,334 men who identified as Hispanic, Asian, another race, or multiple races. The final analytic sample included 5,921 men, comprising 4,837 NHW and 1,084 NHB men.
Measures
Dependent Variable
The dependent variable was office-based provider visits. In each survey round, the Medical Expenditure Panel Survey Household Component (MEPS-HC) collects event-level data on health care utilization across multiple settings. In the Medical Visit (MV) section, respondents report details about each office- or clinic-based visit, including whether the provider seen was a medical doctor. MEPS aggregates these event-level reports across rounds to generate an annual total number of office-based provider visits for each respondent. For this analysis, we used the aggregated 2022 total to create a binary outcome indicating whether the respondent had at least one office-based provider visit during the year.
Independent Variable
The primary independent variable for this study was race and ethnicity. In MEPS, respondents report their race (e.g., White, Black) and, in a separate question, indicate whether they are of Hispanic, Latino, or Spanish origin. NHW men were classified as those who reported their race as White and indicated that they were not of Hispanic, Latino, or Spanish origin. Similarly, NHB men were classified as those who reported their race as Black and indicated that they were not of Hispanic, Latino, or Spanish origin. In all analyses, NHW men served as the reference group.
Covariates
Guided by the Andersen Behavioral Model of Health Services Use (1968, 1995), the covariates selected in this study represented predisposing, enabling and need factors. The predisposing factors included age (in years), educational attainment (Grade 8 or below, some high school, high school or GED, some college/Associates/other degree, Bachelor’s degree, advanced degree), and marital status (married vs. widowed, divorced, separated or never married not). The enabling factors included poverty status (poor/negative, near poor, low income, middle income, high income), employment status (employed during interview date or reference period vs. unemployed), U.S. census region (northeast, Midwest, south, west), whether or not the respondent has health insurance (public or private), and whether or not the respondent has a usual source of care provider. The need factors included self-rated health (fair/poor vs. excellent, very good. or good), self-rated mental health (fair/poor vs. excellent, very good. or good), whether or not the respondent indicated any limitations in ability to work, do housework, or go to school due health problems or impairment, and whether or not the respondent has been diagnosed with three or more of the following priority conditions: diabetes, asthma, high blood pressure, high cholesterol, arthritis, coronary heart disease, angina, heart attack, other heart diseases, stroke, emphysema or joint pain.
Analytic Strategy
Frequencies and means and standard deviations were used to describe the total sample. Using Pearson’s Chi-square tests and Student’s t-tests, we assessed differences between NHW and NHB men as it relates to the respondent characteristics. Given the common occurrence of having at least one office-based provider or physician visit (i.e., prevalence exceeding 10%), modified Poisson regression models were employed (McNutt et al., 2003; Thorpe et al., 2017; Zou, 2004). To examine the association between race and office-based provider utilization among NHW and NHB men, unadjusted and adjusted models were used to estimate prevalence ratios and corresponding 95% confidence intervals. Due to the MEPS’ complex survey design, our study was analyzed using the survey estimation procedures in Stata/SE 18 (StataCorp, College Station, TX, USA). p-values <.05 were considered statistically significant.
Results
The distribution of select characteristics among men for the total sample and by race/ethnicity is shown in Table 1. Of the 5,921 men in the sample, the average age of the men in the sample was 49.2 ± 17.9 years, and 18.3% reported being NHB men. The majority of the men in the sample had more than a high school education (59.7%, n = 3,451), were married (53.8%, n = 3,057), reported high income (51.2%, n = 2,780), were employed (69.1%, n = 3,569), had private or public insurance (94.1%, n = 5,579), had a usual source of care provider (68.7%, n = 4,082), and had at least one office-based provider visit during the year (72.9%, n = 4,469).
Distribution of Characteristics for the Total Sample and for Non-Hispanic Black and Non-Hispanic White Men in the 2022 Medical Expenditure Panel Survey.
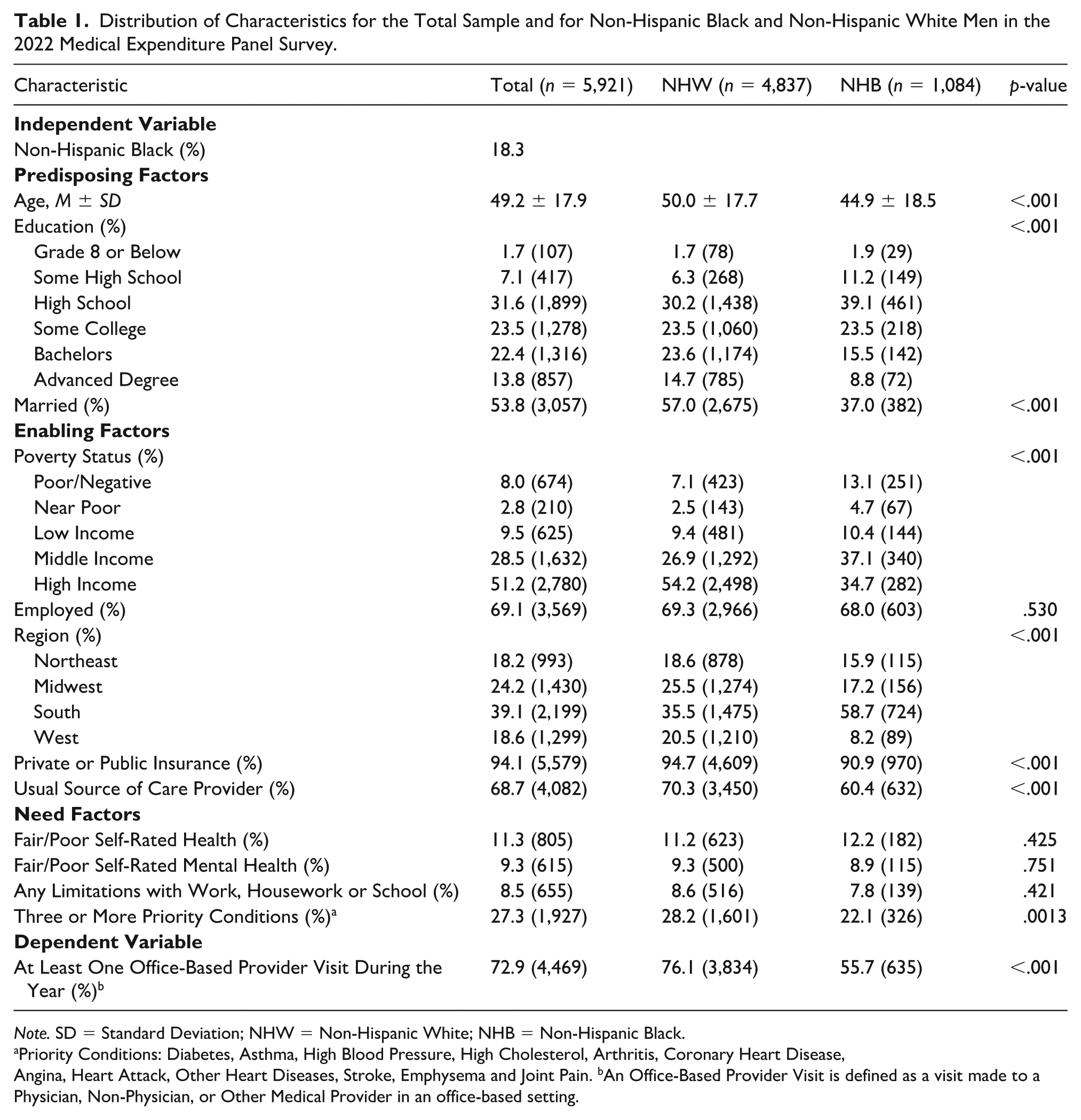
Note. SD = Standard Deviation; NHW = Non-Hispanic White; NHB = Non-Hispanic Black.
Priority Conditions: Diabetes, Asthma, High Blood Pressure, High Cholesterol, Arthritis, Coronary Heart Disease,
Angina, Heart Attack, Other Heart Diseases, Stroke, Emphysema and Joint Pain. bAn Office-Based Provider Visit is defined as a visit made to a Physician, Non-Physician, or Other Medical Provider in an office-based setting.
When examining differences by race/ethnicity, NHB men were on average younger, 44.9 ± 18.5 versus 50.0 ± 17.7, F(1, 259) = 35.32, p < .001, and a smaller proportion of them had an advanced degree, 8.8%, n = 72, versus 14.7%, n = 785, F(4.66, 1,206.01) = 10.84, p < .001, were married, 37.0%, n = 382, versus 57.0%, n = 2,675, F(1, 259) = 79.96, p < .001, reported high income, 34.7%, n = 282, versus 54.2%, n = 2,498, F(3.68, 952.32) = 19.49, p < .001, had public or private insurance, 90.9%, n = 970, versus 94.7%, n = 4,609, F(1.99, 514.84) = 10.41, p < .001, had a usual source of care provider, 60.4%, n = 632, versus 70.3%, n = 3,450, F(1, 259) = 19.08, p < .001, had three more priority conditions, 22.1%, n = 236, versus 28.2%, n = 1,601, F(1, 259) = 10.56, p = .0013, or had at least one office-based provider visit during the year compared with NHW men, 55.7%, n = 635, versus 76.1%, n = 3,834, F(1, 259) = 114.47, p < .001. There were a larger proportion of NHB men who lived in the South compared with NHW men, 58.7%, n = 724, versus 35.5%, n = 1,475, F(2.68, 692.95) = 26.64, p < .001. There were no significant associations observed between NHB and NHW men as it relates to being employed, 69.1%, n = 3,569, F(1, 259) = 0.39, p = .530, reporting fair/poor self-rated health, 11.3%, n = 805, F(1, 259) = 0.64, p = .424, reporting fair/poor self-rated mental health, 9.3%, n = 615, F(1, 259) = 0.10, p = .75, or any limitations in ability to work, do housework, or go to school due health problems or impairment, 8.5%, n = 655, F(1, 259) = 0.64, p = .421.
The association between race and having at least one office-based provider visit during the year among NHB men and NHW men is shown in Table 2. After adjusting for the covariates, NHB men had a lower prevalence of having at least one office-based provider visit during the year (prevalence ratio = 0.83, 95% confidence interval [0.77,0.88]) compared with NHW men.
Association Between Having at Least One Office-Based Provider Visit and Race Among Non-Hispanic Black and Non-Hispanic White Men in the Medical Expenditure Panel Survey 2022.
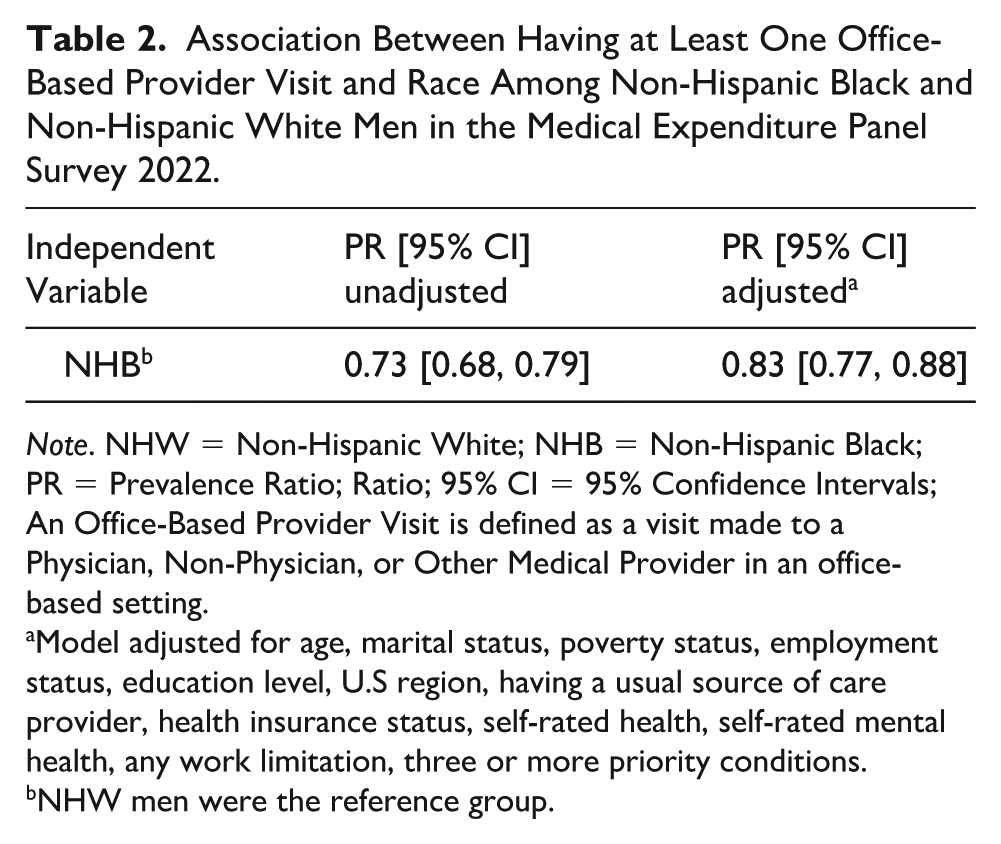
Note. NHW = Non-Hispanic White; NHB = Non-Hispanic Black; PR = Prevalence Ratio; Ratio; 95% CI = 95% Confidence Intervals; An Office-Based Provider Visit is defined as a visit made to a Physician, Non-Physician, or Other Medical Provider in an office-based setting.
Model adjusted for age, marital status, poverty status, employment status, education level, U.S region, having a usual source of care provider, health insurance status, self-rated health, self-rated mental health, any work limitation, three or more priority conditions. bNHW men were the reference group.
Discussion
Understanding racial differences in health care utilization among NHB and NHW men has important implications for preventive care, early detection, and disease management. In this study, we examined whether NHB and NHW men differed in health care service utilization, specifically whether they had at least one office-based provider visit during the year. After adjusting for predisposing, enabling and need factors, NHB men had a 17% lower prevalence of having at least one annual office-based visit compared with NHW men. These results are important because persistent racial disparities in health outcomes among men, particularly NHB men, remain a pressing public health challenge, and differences in health care utilization represent a critical pathway through which inequities in preventable morbidity and mortality may be maintained.
The findings indicated a clear racial/ethnic disparity in annual office-based visits among men. Specifically, NHB men had a lower prevalence of having at least one office-based provider visit during the year than NHW men. This observed utilization gap is consistent with prior evidence that NHB men are less likely to have a usual source of care, underutilize preventive services, and report more unmet medical needs than NHW men, even under expanded insurance coverage (Artiga et al., 2015; Courtemanche & National Bureau of Economic Research, 2019; Gong et al., 2022; Ndugga et al., 2024). Together, these findings suggest that disparities persist beyond the measured predisposing, enabling, and need factors and that insurance coverage alone does not eliminate inequities in access and use (Hirshfield et al., 2018). Structural and sociocultural mechanisms, including medical mistrust, stereotype threat, discrimination, socioeconomic disadvantage, residential segregation, and masculinity-related norms, may suppress routine engagement with care among Black men (Arnett et al., 2016; Blumberg et al., 2015; Parker et al., 2017; Powell et al., 2019; Wallace et al., 2022). As a result, even when insured, Black men may be less likely to establish continuous relationships with providers or obtain routine screenings, limiting opportunities for early detection and chronic disease management (Chandler et al., 2021; Jordan et al., 2024). These finding are also consistent with Alsan et al. (2019) who found Black men were much more likely to select every preventive service, particularly invasive services, once meeting with a racially concordant doctor, reinforcing issues related to communication and mistrust strongly influencing Black men’s health decisions. Overall, our findings extend prior work by documenting persistent racial differences in annual office-based visits among men and highlighting health care utilization as a potential pathway contributing to preventable morbidity and mortality (Arnett et al., 2016; Wallace et al., 2022).
Several limitations should be considered when interpreting these findings. First, office-based visit measures may rely on self-report and are therefore susceptible to recall and reporting bias, which could differ systematically by race. Second, while we adjusted for multiple covariates representing predisposing, enabling, and need factors, residual confounding is possible, particularly for factors that are difficult to measure or not available (e.g., perceived discrimination in health care settings, medical mistrust, stereotype threat, provider availability, prior negative encounters, quality of patient–provider communication, and neighborhood-level access barriers). Third, the visit measures capture whether an annual visit occurred, but do not fully characterize the timing, continuity, content, or quality of care; disparities may be larger (or qualitatively different) when examining preventive service receipt, chronic disease management intensity, or follow-up after abnormal findings. Finally, the results reflect associations and should not be interpreted as causal; unmeasured contextual and structural factors may influence both race-linked exposures and utilization patterns.
Despite these limitations, this study has several strengths. By focusing explicitly on men and directly comparing NHB and NHW men, the analysis addresses a gap in a literature that often examines race and health care use in broader adult populations without attention to gendered dynamics. The use of prevalence ratios facilitates interpretation for common outcomes, and the inclusion of covariate adjustment strengthens inference by accounting for measured differences that could otherwise obscure the association between race and office-based utilization. In addition, examining both overall annual office-based visits and physician-specific annual visits provides a more nuanced picture of where disparities may occur along the pathway to receiving routine and preventive care.
Future research should examine how psychosocial and structural factors, including medical mistrust, experiences of discrimination, masculinity norms, and barriers to access, influence annual office-based visits among NHB men. It is important for scholars to understand how these factors operate independently and jointly among NHB men to improve annual office-based visits. Moreover, incorporating longitudinal and mixed methods study design will prove valuable in understanding how changes in predisposing (those that are modifiable), enabling and need factors shape annual office-based visits over time. Mixed methods and qualitative study designs would provide an opportunity for NHB men’s voices to be heard in research that focuses on them. In addition, research efforts should seek to develop and evaluate multilevel interventions to gain insights from culturally responsive care models, counter stereotyping, trust-building strategies, community-linked primary care navigation, and clinic-level changes that improve continuity of care.
From a public health practice perspective, community-based nursing which consists of bringing care into the communities where Black men live, work, play, and pray, offers a promising strategy to reduce disparities by meeting people where they are and supporting prevention, health promotion, and the maintenance of health in everyday settings (Mtshali, 2005; Zeydani et al., 2023). Delivering services in trusted, familiar spaces may also strengthen relationships and trust, which is especially important given well-documented medical mistrust and the ways racism and mistrust can contribute to delayed preventive care among Black men (Alsan & Wanamaker, 2018; Powell et al., 2019). Aligned with National Academies of Sciences, Engineering, and Medicine recommendations, Neighborhood Nursing is a leading model that embeds a nurse and community health worker within a defined neighborhood to deliver accessible, relationship-based care in homes and trusted community sites (e.g., schools, libraries, senior centers) (Johns Hopkins School of Nursing, n.d.; National Academies of Sciences et al., 2021; Nogueira et al., 2025). CHWs’ cultural familiarity strengthens credibility and trust, which may be especially important for residents who are wary of traditional health systems.
Overall, this study underscores that meaningful racial inequities in routine health care engagement persist among men: NHB men were nearly 20% less likely than NHW men to report an annual office-based or physician visit, even after accounting for key covariates. This disparity matters because routine office-based care is a primary gateway to prevention, early detection, and effective chronic disease management, opportunities that are foundational to narrowing avoidable gaps in morbidity and mortality. The central takeaway is that improving health care coverage alone is unlikely to eliminate these differences; progress will require deliberate, multilevel efforts that address the structural and sociocultural conditions shaping men’s care-seeking and strengthening access to trusted, relationship-based pathways to routine care.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.