
Abstract
The prevalence of type 2 diabetes (T2D) is increasing among non-Hispanic Black and Hispanic communities, especially among men who develop this chronic condition at earlier ages. Personal agency and social support are vital aspects to diabetes management. However, less is known about the relationship between these variables among men living with diabetes. The purposes of this study were to identify (1) levels of personal agency to manage health, (2) sources of social supports to manage health based on personal agency levels, and (3) factors associated with lower personal agency to manage health. Cross-sectional data from non-Hispanic Black (n = 381) and Hispanic (n = 292) men aged 40 years or older with T2D were collected using an internet-delivered questionnaire. Three binary logistic regression models were fitted to assess sociodemographics, health indicators, and support sources associated with weaker personal agency to manage health. About 68% of participants reported having the strongest personal agency relative to 32.1% reporting weaker personal agency. Men who relied more on their spouse/partner (odds ratio [OR] = 1.22, p = .025), coworkers (OR = 1.59, p = .008), or faith-based organizations (OR = 1.29, p = .029) for ongoing help/support to improve their health and manage health problems were more likely to have weaker personal agency. Conversely, men who relied more on their health care providers for ongoing help/support to improve their health and manage health problems were less likely to have weaker personal agency to manage health (OR = 0.74, p < .001). Findings suggest personal agency may influence men’s support needs to manage T2D, which may also be influenced by cultural, socioeconomics, and the composition of social networks.
Introduction
Among the U.S. adult population, type 2 diabetes (T2D) continues to be a burden, with approximately 30 million U.S. adults being diagnosed with diabetes and another 96 million adults having prediabetes (Centers for Disease Control and Prevention [CDC], 2022a). In 2000, the age-adjusted prevalence of diagnosed diabetes was 6.0%; by 2019, the estimated prevalence of undiagnosed and diagnosed T2D had reached 14.7% (CDC, 2022a, 2022c). The upward trend is even more striking for communities of color, particularly within the non-Hispanic Black and Hispanic populations (American Diabetes Association, 2022; CDC, 2022b; Haw et al., 2021). Levels of diagnosed and undiagnosed diabetes are higher for these two minority groups compared with non-Hispanic Whites, with Black and Hispanic people being 50% and 57% more likely to suffer from diabetes than their White counterparts, respectively (CDC, 2022a). The risk for men is especially high, reaching a T2D prevalence of 9.8% in 2018, in contrast with 8.6% for females (CDC, 2022d).
For men in minority communities, lifestyle and modifiable risk factors such as poor dietary habits, physical inactivity, and regular alcohol use, in combination with lower socioeconomic status (SES), are associated with risks of developing T2D at earlier ages (Tenkorang, 2016). Once developed, successful T2D management calls for behavior changes that might contradict how non-Hispanic Black and Hispanic men had been socialized prediagnosis. Exploratory studies have identified the tendency for men of color and those residing in rural areas to delay seeing a doctor until symptoms become severe (Spleen et al., 2014), as well as cultural habits and expectations that place food and masculinity in tandem and opposed to dieting, which, just like seeking care, is coded as a feminized practice to be avoided by men (Hawkins et al., 2017; Hurt et al., 2020). These gendered characteristics and cultural factors pose challenges to promoting behavior change for the management of T2D. Recognizing and supporting patient strengths that help overcome those challenges have significant promise to foster behavior modification in the context of chronic disease management (Wallace et al., 2021). One such strength to promote a healthier lifestyle is individual’s possessing a sense of personal control or agency to manage their health (O’Donnell, 2020).
Personal agency refers to “the sense that I am the one who is causing or generating an action” (Gallagher, 2000) and involves the four core properties of intentionality, forethought, self-regulation, and self-reactiveness, which describe humans’ abilities to plan, anticipate likely outcomes, regulate courses of action, and reflect on their efficacy (Bandura, 2006). Personal agency is considered a protective factor in the self-management of chronic conditions and has been reported to benefit patients’ motivation in glycemic control efforts and physical activity regimens among people with T2D (Romo, 2020). However, older age is associated with a reduction in the sense of agency especially for people aged 50 and beyond, which, in turn, is linked to poorer health and declines in quality of life (Moore, 2016). Not enough is known about personal agency levels to manage health among Hispanic and non-Hispanic Black men, especially middle-aged and older adults. A few studies have focused on goal-setting experiences of Hispanic people (Alicea-Planas, 2013) or strategies to adapt chronic disease self-management programs for non-Hispanic Black seniors (Gitlin et al., 2008). As such, there remains an insufficient understanding about which individual-level factors might help foster healthy aging by enhancing personal agency among these populations.
Literature regarding illness self-management points to the role of supportive social interactions in reinforcing beliefs about one’s efficacy and, thus, agency, positively influencing behavior and health outcomes (Farley, 2020; Gallant et al., 2007; Vassilev et al., 2014). Therefore, social support, defined as the act of providing assistance or comfort to help manage biological, psychological, and social stressors (American Psychological Association, 2023), may potentially promote personal agency. Social support from health professionals, family, and friends has been reported to improve adherence to glucose testing, medications, exercise, and diet (Gallant, 2003; Hurt et al., 2015, 2020; Rosland et al., 2008; Tang et al., 2008). When studying minority communities, providing social support to manage health concerns often centers around caregiving within household or family units, where greater self-efficacy can be modeled and exert a positive influence through intergenerational transmission (Warren-Findlow et al., 2011). A gap exists in understanding how personal agency may be associated with a broader variety of social support sources for non-Hispanic Black and Hispanic men with chronic conditions. The purposes of this study were to identify (1) levels of personal agency to manage health, (2) sources of social supports to manage health based on personal agency levels, and (3) factors associated with lower personal agency to manage health by race and ethnicity among a sample of non-Hispanic Black and Hispanic men with T2D.
Method
Sample and Procedures
Cross-sectional data were collected using an internet-based questionnaire between September and November 2019. Participants were recruited nationally from a Qualtrics panel as part of a larger study investigating health-related attitudes and behaviors, and facilitators and barriers to medical and preventive health service utilization. To qualify for inclusion in the study, respondents had to identify as non-Hispanic Black or Hispanic men, be aged 40 years or older, and report having one or more chronic diseases (Kew et al., 2023; Merianos et al., 2023; Sherman et al., 2021; Smith et al., 2022). Participants completed a 105-item survey developed by the research team, which largely comprised content from other validated sources (The Atlantic Philanthropies, 2009; CDC, 2020; Center for Community Health Development, 2013; Ory, Ahn, Jiang, Lorig, et al., 2013; Ory, Ahn, Jiang, Smith et al., 2013; Smith et al., 2013). The research team reviewed the instruments from these sources and purposively selected items, measures, and scales based on their relevance to the aims of the larger study and their inclusion in other grand-scale initiatives. Overall, 2,028 men who met the inclusion criteria completed the questionnaire.
Given this study’s focus on men with self-reported T2D, 1,227 men were omitted because they did not report this condition. An additional 82 men were omitted as they did not have health insurance. This decision was made because many of the study variables of interest (e.g., agency, barriers to care, health care frustrations, support sources) relate to interactions with health care providers. Therefore, to eliminate bias and account for potential confounders, men without health insurance were omitted because they often have less opportunity to interact with or rely on health care professionals. The remaining analytic sample consisted of 673 non-Hispanic Black (n = 381) and Hispanic (n = 292) insured men aged 40 years or older with T2D (33.2% of the larger study sample). When comparing this study’s analytic sample with the larger sample of men who completed the survey, the analytic sample was significantly older, had significantly lower education levels, and was significantly more likely to have a routine check-up with a physician in the past year. This study was reviewed and approved by the Institutional Review Board at (Texas A&M University) (#2018-1684).
Measures
Dependent Variable
The dependent variable in this study was a single-item measure of participants’ personal agency to manage their health. Participants were asked about their level of agreement with the following statement, “I am the person who is responsible for taking care of my health” (Hibbard et al., 2005). This single item was selected from the 13-item Patient Activation Measure (PAM) short form (Hibbard et al., 2005) because it is indicative of a person’s self-awareness about their responsibility and role in the management of their health. Response choices for this item were strongly agree (67.9%, n = 457), agree (27.3%, n = 184), disagree (2.2%, n = 15), and strongly disagree (2.5%, n = 17). Due to the skewed nature of the responses, they were collapsed into two categories: strongest agency (i.e., strongly agree) and weaker agency (i.e., agree, disagree, or strongly disagree). Men reporting the strongest agency served as the reference category and were those who perceived themselves to have the highest degree of responsibility to manage their health. Men reporting weaker agency were those who perceived themselves to have anything less than the highest degree of personal responsibility to manage their health.
Chronic Conditions and Medication Use
Compared with non-Hispanic Whites, middle-aged non-Hispanic Blacks develop multimorbidity earlier, while Hispanics accumulate chronic diseases at a faster pace (Quiñones et al., 2019). Thus, to account for co-occurring chronic conditions, participants were asked to complete a self-reported “check all that apply” list of 18 conditions beyond T2D. The list included (1) asthma/emphysema/chronic breathing or lung problem, (2) arthritis/rheumatic disease, (3) cancer or cancer survivor, (4) chronic pain, (5) depression or anxiety, (6) heart disease, (7) high cholesterol, (8) hypertension, (9) kidney disease, (10) memory problem, (11) obesity, (12) osteoporosis, (13) obstructive sleep apnea, (14) schizophrenia or other psychotic disorder, (15) stroke, (16) thyroid problem, (17) urinary incontinence, and (18) “other” chronic condition not listed. The number of selected conditions was summed to create a count variable and treated continuously in analyses (range = 0–18). In addition, participants reported the number of different medications they took daily, which was treated continuously in analyses (range = 0–≥6).
Diabetes-Related Health Interactions and Screenings
To assess the utilization of recommended health practices for persons with diabetes, participants were asked to report how long it has been since they last had a routine check-up with a physician, a blood sugar test, and an eye exam (CDC, 2020). Response choices for each item were within the past year (less than 12 months), within the past 2 years (more than 1 year, but less than 2 years), within the past 3 years (more than 2 years, but less than 3 years), within the past 4 years (more than 3 years, but less than 4 years), within the past 5 years (more than 4 years, but less than 5 years), and 5 or more years. For each item, responses were grouped into two categories according to whether the preventive health screening happened within the past year or more than a year before taking the survey.
General Health Status
Overall general health status was measured by asking participants to rate their health based on the following categories: poor, fair, good, very good, and excellent. From this questionnaire item, general health status was assessed as an ordinal variable ranging from poor (scored 1) to excellent (scored 5) (CDC, 2000).
Barriers to Self-Care
The barriers to self-care scale comprised five items that participants agreed or disagreed with using a 4-point Likert-type scale (The Atlantic Philanthropies, 2009; Smith et al., 2013). Response options for each item were strongly disagree, disagree, agree, and strongly agree. The specific items include (1) need help learning what they should be doing to take better care of their health; (2) need help learning how to take better care of their health in a way that works for them and their life; (3) do not have the money it takes to do things that will improve their health or condition; (4) wish they could change and do things that are healthier, but they just do not think they can; and (5) all of their different health problems and conditions make it difficult for them to take better care of themselves. Possible scores for this index ranged from 5 to 20, with higher scores indicating more barriers. Cronbach’s alpha value for the current sample was .832, which is consistent with Cronbach’s alpha value .813 from a sample of women from a previous study (Smith et al., 2013).
Frequency of Support Received and Reliance on Others for Help and Support to Improve Health and Manage Health Problems
The frequency of participants receiving help and support needed to improve their health and manage health problems was measured using a 5-point scale based on the following categories: never (scored 0), rarely (scored 1), occasionally (scored 2), frequently (scored 3), and always (scored 4) (The Atlantic Philanthropies, 2009; Smith et al., 2013). Higher scores indicate more frequent support received. Reliance on receiving ongoing help and support needed to improve their health and manage health problems was assessed using a 5-point scale including the following options: not at all (scored 1), a little (scored 2), a moderate amount (scored 3), a lot (scored 4), and a great deal (scored 5) (The Atlantic Philanthropies, 2009; Smith et al., 2013). This scale was used to determine the level of reliance on (1) their spouse or partner; (2) friends or relatives; (3) people with similar health problems; (4) coworkers; (5) doctors, nurses, or other health care providers; (6) church, synagogue, or other faith-based organizations; (7) community groups or clubs; and (8) the internet. Higher scores indicate more reliance on receiving help and support from that source, respectively.
Sociodemographics
Individual-level social characteristics and place-based factors are associated with health and health-related outcomes, including T2D prevalence, self-management, and control (CDC, 2022b; Rabi et al., 2006; Solar & Irwin, 2010; Stephens et al., 2014). All analyses in this study included the following sociodemographic measures: race and ethnicity (i.e., non-Hispanic Black, Hispanic), age (range = 40–89 years), educational attainment (i.e., ≤high school graduate, some college/2-year degree, ≥4-year degree), marital status (i.e., married/partnered, never married, divorced/separated, widowed), job status (i.e., employed, retired, disabled/not employed/student), residential rurality status (i.e., urban, rural), number of persons living in the household (including self), and annual household income level (in mostly US$10,000 increments).
Data Analysis
All analyses were performed using SPSS Version 28 (IBM Corp., 2021). Descriptive statistics were calculated for all variables of interest (i.e., means, standard deviations, frequencies). Bivariate analyses were performed to compare sample characteristics by participants’ race/ethnicity (i.e., non-Hispanic Black, Hispanic) and participants’ personal agency to manage their health (i.e., strongest, weaker). Pearson’s chi-square tests were used to assess differences across race/ethnicity and personal agency level for categorical variables. Independent samples t-tests were used to assess mean differences across race/ethnicity and personal agency level for continuous variables. Three binary logistic regression models (i.e., for all men, non-Hispanic Black only, and Hispanic only) were fitted to assess factors associated with weaker personal agency to manage health (i.e., strongest personal agency served as the referent category). All three logistic models controlled for the independent variables described in the “Measures” section; however, only the model including all men controlled for race/ethnicity. A p value of <.05 was used to determine statistical significance for all analyses in this study.
Results
Table 1 presents the sample characteristics by race/ethnicity and personal agency to manage health. Overall, 56.6% (n = 381) of participants were non-Hispanic Black and 43.4% (n = 292) were Hispanic. About 68% (n = 457) of participants reported having the strongest personal agency relative to 32.1% (n = 216) reporting weaker personal agency. On average, participants were aged 58.40 (±10.00) years. In this sample, 22.1% (n = 149) of participants had a high school education or less, 43.2% (n = 291) had some college or a 2-year degree, and 34.6% (n = 233) had a 4-year degree. The majority of participants were married (55.0%, n = 370), with 23.9% (n = 161) never being married, 17.1% (n = 115) divorced/separated, and 4.0% (n = 27) widowed. About 41% (n = 278) of participants were employed, 34.3% (n = 231) were retired, and 24.4% (n = 164) were disabled, not employed, or students. The average household size of participants was 2.55 (±1.48), and the majority resided in urban areas (94.4%, n = 635). On average, participants had 3.96 (±3.28) chronic conditions (beyond diabetes), with the most frequently reported conditions being hypertension (65.4%, n = 440), high cholesterol (59.6%, n = 401), chronic pain (32.8%, n = 221), obesity (30.8%, n = 207), arthritis/rheumatic disease (29.7%, n = 200), and depression or anxiety (27.0%, n = 182). On average, participants took 4.32 (±1.74) medications daily, and most had a routine check-up (90.5%, n = 609), blood sugar test (88.0%, n = 592), and eye exam (70.3%, n = 473) in the past year. On average, participants reported getting moderate help and support needed to improve their health and manage health problems (i.e., 2.72 out of 4). Participants reported relying on health care providers as the primary source for ongoing help and support needed to improve their health and manage health problems (i.e., 3.53 out of 5), followed by their spouse or partner (i.e., 2.68 out of 5), the internet (i.e., 2.24 out of 5), and friends or relatives (i.e., 2.13 out of 5).
Sample Characteristics by Race and Ethnicity and Personal Agency to Manage Health

Continuous variables compared with independent samples t-tests.
When comparing sample characteristics by race/ethnicity, a larger proportion of Hispanic men had higher education levels (χ2 = 17.63, p < .001) and were married (χ2 = 23.72, p < .001) compared with their non-Hispanic Black counterparts. On average, Hispanic men had higher annual household incomes (t = −2.97, p = .003) and relied more on their spouse or partner for ongoing help and support to improve their health and manage their health problems (t = −4.28, p < .001).
When comparing sample characteristics by personal agency to manage health, a larger proportion of men with weaker personal agency resided in rural areas (χ2 = 6.11, p = .047), and a smaller proportion of men with weaker personal agency to manage their health got a blood sugar test in the past year (χ2 = 6.44, p = .011). On average, men with weaker personal agency to manage their health were younger (t = 2.06, p = .039), had worse general health status (t = 4.20, p < .001), more barriers to self-care (t = −4.08, p < .001), and received less help and support to improve their health and manage their health problems (t = 5.68, p < .001). On average, men with weaker personal agency to manage their health relied more on their spouse or partner (t = −2.56, p = .011), friends or relatives (t = −2.55, p = .011), people with similar health problems (t = −2.44, p = .015), coworkers (t = −3.97, p < .001), faith-based organization (t = −3.44, p < .001), and community groups or clubs (t = −2.68, p = .007) for ongoing help and support to improve their health and manage their health problems. On average, men with the strongest personal agency to manage their health relied more on their health care providers for ongoing help and support to improve their health and manage their health problems (t = 3.49, p < .001). Support sources by personal agency level are displayed graphically in Figure 1.
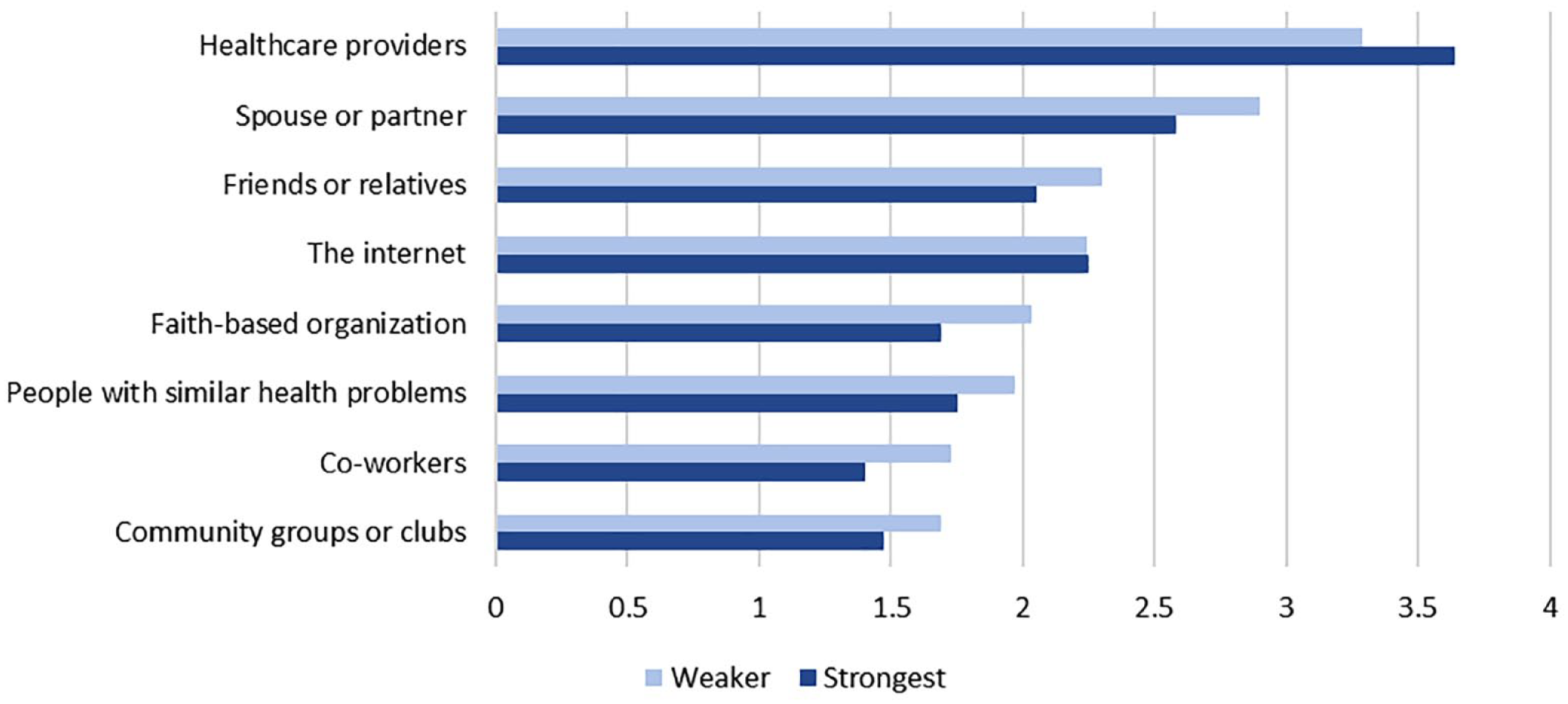
Source Reliance for Ongoing Help/Support to Improve Health Hand Manage Health Problems by Personal Agency Level
Table 2 reports findings from the three logistic regression models. In the overall model including all men in the sample, men residing in rural areas were more likely to have weaker personal agency to manage their health compared with those residing in urban areas (OR = 2.50, p = .018, 95% confidence interval [CI] = [1.17, 5.34]). Perceiving better health status (OR = 0.69, p = .001, 95% CI = [0.54, 0.86]) and getting more help and support to manage health (OR = 0.71, p < .001, 95% CI = [0.59, 0.85]) were associated with lower odds of weaker personal agency to manage health. Men who relied more on their spouse or partner (OR = 1.22, p = .025, 95% CI = [1.03, 1.44]), coworkers (OR = 1.59, p = .008, 95% CI = [1.13, 2.23]), or faith-based organizations (OR = 1.29, p = .029, 95% CI = [1.03, 1.62]) for ongoing help and support to improve their health and manage health problems were more likely to have weaker personal agency to manage health. Men who relied more on their health care providers for ongoing help and support to improve their health and manage health problems were less likely to have weaker personal agency to manage health (OR = 0.74, p < .001, 95% CI = [0.62, 0.89]).
Factors Associated With Lower Personal Agency to Manage Health

Note. CI = confidence interval; OR = odds ratio.
Reference group: strongest personal agency to manage health.
In the model including only non-Hispanic Black men, those residing in rural areas were more likely to have weaker personal agency to manage their health compared with men residing in urban areas (OR = 3.60, p = .012, 95% CI = [1.32, 9.82]). Getting more help and support to manage health was associated with lower odds of weaker personal agency to manage health (OR = 0.63, p < .001, 95% CI = [0.48, 0.81]). Non-Hispanic Black men who relied more on their spouse or partner for ongoing help and support to improve their health and manage health problems were more likely to have weaker personal agency to manage health (OR = 1.30, p = .038, 95% CI = [1.01, 1.66]). Non-Hispanic Black men who relied more on the internet for ongoing help and support to improve their health and manage health problems were less likely to have weaker personal agency to manage health (OR = 0.76, p = .045, 95% CI = [0.58, 0.99]).
In the model including only Hispanic men, those who attended some college or received a 2-year degree were more likely to have weaker personal agency to manage health than their counterparts who had a high school education or less (OR = 2.86, p = .025, 95% CI = [1.14, 7.17]). Reporting better health status was associated with lower odds of weaker personal agency to manage health (OR = 0.53, p = .001, 95% CI = [0.36, 0.78]). Hispanic men who relied more on their coworkers (OR = 1.89, p = .028, 95% CI = [1.07, 3.33]) and faith-based organizations (OR = 1.78, p = .006, 95% CI = [1.18, 2.67]) for ongoing help and support to improve their health and manage health problems were more likely to have weaker personal agency to manage health. Hispanic men who relied more on their health care providers (OR = 0.62, p = .002, 95% CI = [0.46, 0.84]) and community groups or clubs (OR = 0.55, p = .046, 95% CI = [0.31, 0.99]) for ongoing help and support to improve their health and manage health problems were less likely to have weaker personal agency to manage health.
Discussion
Focusing on the experiences of non-Hispanic Black and Hispanic men living with T2D in the United States, the present study used self-reported data to identify the levels of personal agency to manage health, the sources of social support to manage health based on personal agency levels, and the factors associated with lower personal agency to manage health by race and ethnicity. Irrespective of race and ethnicity, most participants reported the highest level of personal agency by strongly agreeing with the statement “I am the person who is responsible for taking care of my health.” For men with the strongest level of personal agency, health care providers and the internet were the main sources for ongoing help and support with improving their health and managing their health problems. Men with weaker personal agency levels indicate relying more on a wider variety of sources of social support, mainly their spouse or partner, friends or relatives, faith-based organizations, and people with similar health problems.
These differences in the main sources of social support by personal agency level may be explained by the support/efficacy framework (Antonucci & Jackson, 1987). According to this framework, similar supportive behaviors carried out by different support providers may be perceived differently by the target person (i.e., recipient of support) and have varying levels of effectiveness (Antonucci, 1985). The support provider’s belief in the target person’s ability or effectiveness may be a crucial factor in prompting them to engage in suitable and effective supportive behaviors, which, in turn, may positively impact the target person’s sense of self-efficacy or perceived capability to achieve the desired behavior (Antonucci & Jackson, 1987). For non-Hispanic Black and Hispanic men with the strongest personal agency to manage health, the above may translate into relying more for ongoing help and support on sources that are both knowledgeable and sensitized to the difficulties of managing chronic conditions like T2D, such as health care providers. For men with the strongest personal agency to manage health, health care providers may be perceived as appealing sources of support given their role in increasing awareness, managing health behaviors, and motivating patients to be screened for diseases (Vega et al., 2009), actions that may further reinforce notions of self-efficacy on individuals with the strongest agency.
Similarly, the support/efficacy framework may help explain why non-Hispanic Black and Hispanic men with the strongest agency rely more on the internet even in the absence of other support providers (Allen et al., 2019). The internet can be perceived as a source conducive to the internalization of efficacy beliefs (Allen et al., 2019). Put differently, lacking support from interpersonal relationships within close-knit groups, or deciding not to use support from those sources, may be compensated by seeking care from health care professionals or practical help from online sources, reinforcing personal agency among non-Hispanic Black and Hispanic men with T2D.
Overall, men living with chronic conditions accept that they need help and cannot manage their health alone, but they differ in the sources they turn to for support. Additional differences by race and ethnicity merit further attention. Specifically, non-Hispanic Black men with a weaker agency had more reliance on their spouses and less reliance on the internet. These findings may be an artifact of the lower SES of non-Hispanic Black men in this sample. Compared with Hispanic men, non-Hispanic Black men reported lower annual household income, educational attainment, and labor force participation, thus potentially reducing their ability to use the internet for ongoing health and support with improving their health and causing them to turn to reciprocal relationships to managing their health problems, that is, their spouse or partner. Hispanic men with a weaker agency relied more on their coworkers and faith-based organizations but less reliance on health care providers and community groups or clubs. An argument could be made that there are cultural differences regarding how these two groups of men seek external support in managing T2D.
Although both non-Hispanic Black and Hispanic men tend to be socialized into a type of masculinity that emphasizes the appearance of strength, control, and a sense of invulnerability to illness, which can present a barrier to health seeking (Hawkins et al., 2017; Rivera-Ramos & Buki, 2011), our findings suggest that these groups of men differ in their support sources depending on their levels of personal agency. As mentioned previously, non-Hispanic Black men with weaker agency rely on their spouse or partner and those with the strongest agency rely on the internet to manage their health, which indicates that significant sources of support for men of this racial group vary from intimate reciprocal relationships (i.e., spouse or partner) to distant and impersonal ones (i.e., the internet) based on agency. For Hispanic men, the range of significant sources of support to manage their health is not as wide as that of non-Hispanic Black men; instead of extending from the intimate to the impersonal, it lingers in the realm of secondary groups. For Hispanic men, differences in significant sources of support to manage health by personal agency level may be a function of passive versus active choice (Helzer, 2012). Support might be anticipated within faith-based organizations and work environments given the normative or contractual nature of the interpersonal relationships; the fact that one could anticipate such support could explain why Hispanic men with weaker personal agency rely on such sources more. The role of friendships in community groups or clubs can be hypothesized to be one of choice, not obligation, and thus more aligned with the strongest personal agency type. In addition, and similar to the results for the model including all men, relying on health care providers aligns with the strongest personal agency as it affirms its distinctive attributes, like the ability to plan, regulate courses of action, and reflect on their efficacy (Bandura, 2006), which can be exercised in the patient–medical staff relationship.
Compared with those with the strongest agency, non-Hispanic Black and Hispanic men with weaker agency were less likely to feel they get the help and support needed to improve their health and manage health problems. Thus, having less agency may indicate needing others to provide functional support or lacking abilities to use the available resources to overcome obstacles to chronic disease self-management. Interventions and linkages to resources and services to improve the personal agency of men with diabetes may be beneficial not only for its direct effects in the form of an increased sense of self-efficacy but also as a mechanism to improve perceived support provision (Bahari et al., 2019; Choi, 2020; Helliwell & Putnam, 2004; Thoits, 2011). To bolster personal agency, nationally available and cost-effective interventions such as the Diabetes Self-Management Program (DSMP) are promising strategies that effectively help participants manage their diabetes and associated symptomatology in clinical and community settings (Lorig et al., 2009, 2010, 2016; Smith et al., 2017). Targeted and culturally sensitive DSMPs like ¡Sí, Yo Puedo Controlar Mi Diabetes! for Hispanic and Wisdom, Power, Control for non-Hispanic Black and multi-ethnic people with diabetes are further avenues to strengthen knowledge, skills, and confidence to self-manage diabetes while encouraging greater personal agency among these populations (Peña-Purcell et al., 2011, 2015, 2019).
Rural residence was significantly associated with weaker agency for all men, in general, and non-Hispanic Black men, in particular, suggesting that it may be challenging to have stronger agency when resources are more dispersed or less prevalent in the community. The prevalence of diabetes and its associated problems are worsened by a lack of adequate health care options and insufficient availability of other support resources for disease management within rural communities, leading to disadvantages compared with urban areas (Lepard et al., 2015; Massey et al., 2010; Ross et al., 2015). In a subset analysis of the current sample, participant characteristics were compared by rural/urban residence. Beyond having weaker agency, men residing in rural areas had lower education levels and relied less on friends/relatives, people with similar problems, health care providers, faith-based organizations, and the internet for ongoing help/support to improve their health and manage health problems, relative to those residing in urban areas. Despite only 5.6% (n = 38) of the current sample residing in rural areas, this subset analysis may suggest the presence of important differences in social networks and support structures in rural versus urban communities, which warrants further investigation.
Consistent with previous literature on the link between psychosocial and physical factors (Schneiderman, 2004), men with weaker personal agency overall had worse general health status. The latter was also the case for Hispanic men with weaker personal agency compared with those with the strongest level, which may suggest actual or perceived worse health compounded by the lower self-efficacy associated with weaker agency (Infurna et al., 2011). Men with the strongest personal agency and non-Hispanic Black men reported taking more daily medications, but the relationship between agency and medication use was not significant despite likely indicating a more complex multimorbidity.
This study is not without limitations. Data were self-reported and cross-sectional, which may have introduced reporting bias (i.e., under- or overreporting) and limited the ability to draw conclusions about causality. Data were collected through an online questionnaire, which may have biased the results toward individuals with higher SES and access to the internet and excluded those without access. Gathering data using internet-based data collection may limit the generalizability of these findings to those without internet access. Not all survey items and scales in the parent study were formally pretested or pilot-tested specifically with non-Hispanic Black and Hispanic men with diabetes prior to their selection or use. The majority of men in this sample reported the strongest agency level (69.1%), which led researchers to dichotomize the dependent variable to identify factors associated with weaker agency. While the decision to collapse response categories was justifiable, it may have resulted in a loss of information. Future studies should consider using multi-item measures to assess agency such as the PAM (Hibbard et al., 2005). While the study provided information on chronic conditions that co-occur with diabetes, it did not provide details on the diagnosis, treatment, and complications of these conditions over time. Likewise, the study did not contain any longitudinal data on participants’ social networks, nor did it document any changes in the availability and reception of social support. Additional analyses are recommended to continue examining and conceptualizing the relationships between levels of personal agency to manage health, sources of social support, and racial and ethnic identity. A better understanding of the concordance of patient/physician racial and ethnic identities and its role in promoting personal agency among Black and Hispanic men is also needed (Street et al., 2008; Takeshita et al., 2020).
Conclusion
This study aimed to identify social supports and other factors associated with lower personal agency to manage health by race and ethnicity. Findings from this study contribute to the existing literature by contextualizing personal agency and support sources among non-Hispanic Black and Hispanic men with T2D. Generally, the men in this sample reported high levels of personal agency and strong social supports, which are important for T2D self-management. However, additional research is needed to determine whether stronger agency actually results in better T2D regulation (e.g., HbA1c levels) and self-management behavior among non-Hispanic Black and Hispanic men. While health care professionals were the most frequently reported source of support to improve health and manage health problems in this sample, sources of support differed by levels of personal agency and across race and ethnicity, suggesting the importance of culture, affluence, and social network composition among these men. Efforts are needed to better understand the role of passive versus active choice for social supports among men living with T2D, and the level and types of support these men receive from each source relative to their personal agency levels. Findings from this study may be helpful to prepare health care professionals and community-based organizations to engage men in practical, culturally appropriate diabetes self-management strategies. Additional research is needed to better understand the nuances social supports and networks of non-Hispanic Black and Hispanic men, how they influence (or are influenced by) personal agency, and how they contribute to diabetes self-management and control.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Texas A&M University through their Texas A&M Triads for Transformation (T3) initiative (#246357-00000).
Ethics Statement
The study was conducted in compliance with federal regulations governing protection of human participants and was reviewed and approved by the Institutional Review Board (IRB) at Texas A&M University (IRB2018-1684M).