
Abstract
Deciding when to become a father for the first time is shaped by personal and social factors, yet little is known about the determinants of men’s age at first childbearing. This study examines the key personal and social predictors with men’s age during their first transition to fatherhood. This descriptive-analytical, cross-sectional study examined 290 men who, with their wife’s first pregnancy, were referred to health centers in Mashhad, Iran for pregnancy care in 2023. Cluster sampling was used. The data-collection tools included the Enrich Marital Satisfaction questionnaire, the Quality of Life questionnaire, the Multidimensional Scale of Perceived Social Support, the Snyder Hope Scale, and demographic characteristics. The outcome variable of interest is the age of the men. Data analysis was done using univariate and multiple linear regression models in SPSS 26, with statistical significance set at p < .05. A total of 290 men who became fathers for the first time participated in the study, with a mean age of 29.73 years and a standard deviation of 6.28 years. Among the variables included in the multiple linear regression analysis, the indicators of marital satisfaction (p = .001), marriage span (p = .001), occupation levels (p < .05), some economic status levels (p < .05), and the person who decides the number of children (p = .008) had a significant effect on men during their first transition to fatherhood. The duration of marriage, marital satisfaction, and economic factors are determinants during men’s first transition to fatherhood. Governments and policymakers should include men in education and fertility planning by providing them with appropriate solutions.
Introduction
Childbearing decisions represent one of the most significant transitions in the human life course, shaping family structures, demographic patterns, and individual well-being. Early research in fertility behavior primarily emphasized women’s roles in reproductive decisions, reflecting their biological and social centrality in the process of childbearing (Bell, 2016; Zabak et al., 2023). However, contemporary scholarship increasingly recognizes the crucial influence of men in shaping reproductive outcomes (Ku et al., 2025). Despite men’s equal partnership in conception and parenting, their perspectives and contributions to fertility decision-making remain comparatively underexplored (Harlow et al., 2020; Seth et al., 2022).
In the context of global demographic transitions, the trend toward delayed parenthood including an increasing number of men becoming fathers after age 35 underscores the importance of understanding the psychosocial, economic, and relational factors that shape the timing of first-time fatherhood (Mu et al., 2025; Wood & Goriely, 2022).
Declining fertility rates and delayed childbearing are defining features of modern demographic change (Thompson & Lee, 2011). In Iran, these trends have been particularly pronounced. The total fertility rate decreased from 6.5 children per woman in the 1980s to 1.8 in 2011, increased slightly to around 2.0 in 2016, and then declined again to approximately 1.6 by 2023 (Safdari-Dehcheshmeh et al., 2023). This rapid decline, coupled with shifting marriage and employment patterns, has led to a demographic situation where the cohorts born in the 1980s and 1990s once the largest reproductive groups are moving beyond typical childbearing ages. Consequently, Iran’s demographic capacity for population replacement is diminishing (Hashemzadeh et al., 2022).
While demographic policies largely focused on encouraging higher fertility, most studies have centered on women’s attitudes and circumstances, leaving men’s economic, occupational, and relational determinants of fertility timing underexamined (Miettinen & Jalovaara, 2020). Understanding how these factors influence men’s age at first birth is therefore critical for addressing both delayed parenthood and persistently low fertility (Wei et al., 2018).
A review of existing literature reveals several key limitations: (1) Most fertility studies either overlook men’s perspectives or treat male factors as secondary to women’s determinants. (2) The relationship between men’s economic and occupational stability and their timing of first childbearing has not been comprehensively analyzed within a coherent theoretical framework. (3) The mediating role of marital satisfaction and intra-couple decision-making patterns in shaping fertility timing among men remains insufficiently explored.
Thus, there is a clear need to investigate how men’s socioeconomic conditions, marital dynamics, and decision-making authority interact to influence the timing of their first fatherhood specially in the context of countries experiencing fertility decline, such as Iran, which emphasizes that major life events, such as marriage, employment, and parenthood, are interconnected and shaped by their timing within the broader social context. From this perspective, men’s age at first birth reflects the alignment (or misalignment) of economic, relational, and social trajectories throughout their life course.
The purpose of this study is to examine the economic, marital, and decision-making factors associated with men’s age at first birth in Iran. By focusing on men’s roles and perspectives, the study seeks to fill an important gap in fertility research that has traditionally prioritized women’s determinants. The findings aim to contribute to the development of gender-inclusive population policies that address declining fertility rates and promote family well-being within diverse socioeconomic contexts.
Methods
Study Design and Participants
In this descriptive-analytical, cross-sectional study, a random sample of 290 men, along with their wives, who were referred to health centers in Mashhad, Iran for pregnancy care in 2023, was selected. The ages of the men participating in this study ranged from 18 to 46 years. The inclusion criteria for the study were Iranian men who were married, had no history of infertility in their couple, and were having their first child. The exclusion criterion was incomplete completion of the questionnaire. In this study, seven subjects completed the questionnaire incompletely and were excluded from the study. G-power software was used to calculate the sample size. Considering α = 0.05, power = 0.9 (β = 0.1), the effect size of 0.15 (Cohen’s suggested medium effect size) and the presence of 20 independent variables in the study, the sample size was estimated to be 191 people. Considering that cluster sampling was used in this study and considering a design effect of 1.5, the final sample size was estimated to be 287 people.
Sampling
Cluster sampling was used. First, three health centers were randomly selected from all the health centers in Mashhad. Then, according to the list of names of individuals registered in the Integrated Health System (SIB), each eligible man was assigned a code based on the study entry criteria, and 96 individuals from each health center were selected by simple random selection using random numbers in Excel software. After identifying individuals eligible to participate in the study, the subjects were contacted by phone. The objectives of the research were explained to them, and they were invited to attend the health center on a specified day if they were willing to participate. At the center, further explanations were provided in person regarding the study’s aims and the method for completing the questionnaire. Participants were assured that all their information would remain confidential. After obtaining informed consent, each individual completed the questionnaires privately in a designated room.
Data-Collection Instrument
The data-collection tools included the Enrich Marital Satisfaction questionnaire, the Quality of Life questionnaire, the Multidimensional Scale of Perceived Social Support, the Snyder Hope Scale, and the demographic characteristics questionnaire included age, education of the wife and husband, occupation, place of residence, length of the marriage, appropriate spacing between children, history of illness, family economic status, interest in having children, housing status, access to contraceptive methods, the person who decides when to have children, the person who decides the number of children, the person who decides the method of contraception, and membership in a charitable association. The outcome variable of interest is the age of the men.
Enrich Marital Satisfaction Questionnaire
This questionnaire has 35 questions and has four dimensions: ideal distortion, marital satisfaction, communication, and conflict resolution. Cronbach’s alpha coefficient of the questionnaire in the Asoodeh study (2010) with 365 couples (730 people) was found to be 0.68, 0.78, 0.62, and 0.77, respectively (Asoodeh et al., 2010). The validity and reliability of this questionnaire were evaluated and confirmed in this study. The content validity index (CVI) for the entire questionnaire was 0.88. The reliability of the instrument was assessed using Cronbach’s alpha, and Cronbach’s alpha for the entire questionnaire was 0.80. For the repeatability of the questionnaire, the intraclass correlation coefficient (ICC) was calculated and was 0.78 for the whole of the questionnaire.
Quality of Life Questionnaire
The quality of life questionnaire is derived from the World Health Organization’s quality of life questionnaire. The World Health Organization’s summarized quality of life questionnaire includes 26 questions in four dimensions: physical, psycho-emotional, social, and environmental. Usefy et al. (2010) determined the reliability of the quality of life questionnaire using Cronbach’s alpha of 0.70. The validity and reliability of this questionnaire were evaluated and confirmed in this study. The CVI for the entire questionnaire was 0.82. The reliability of the instrument was assessed using Cronbach’s alpha, and Cronbach’s alpha for the whole of the questionnaire was 0.76. For the repeatability of the questionnaire, ICC was calculated, and 0.81 was obtained for the whole of the questionnaire.
Multidimensional Perceived Social Support Scale Questionnaire
Zimet et al.’s (1988) Multidimensional Perceived Social Support Scale is a 12-item instrument designed to assess perceived social support from three sources: family, friends, and important people in life. Its Persian version was developed by Salimi and Bahrami in 2009 (Zimet et al., 1988). The validity of the Multidimensional Perceived Social Support Scale (Zimet et al., 1988) questionnaire has also been estimated through content analysis using the appropriate principal components method, and the reliability of the questionnaire in various studies using Cronbach’s alpha has been reported to be between 0.86 and 0.9 for the dimensions of the questionnaire, and 0.86 for the entire questionnaire (Bruwer et al., 2008; Salimi et al., 2009). The validity and reliability of this questionnaire were evaluated and confirmed in this study. CVI for the entire questionnaire was 0.94. The reliability of the instrument was assessed using Cronbach’s alpha, and Cronbach’s alpha for the entire questionnaire was 0.89. For the repeatability of the questionnaire, ICC was calculated, and 0.91 was obtained for the entire questionnaire.
Snyder Hope Scale
The Snyder Hope Scale is a scale that assesses a person’s hope as a relatively stable personality trait. This 12-question hope scale was designed by Snyder (2000) for ages 15 and up and includes two dimensions: agentic thinking and strategies. The standard version of the Snyder Hope Scale consists of 12 items: four items assess agency thinking, which reflect an individual’s belief in their ability to pursue and achieve their goals. Four items assess pathways thinking, which evaluate an individual’s ability to generate different routes or strategies to reach their goals. Four items are filler items, which are not included in scoring and are used solely to reduce test transparency and prevent response bias. The items are typically scored on a 4- or 5-point Likert-type scale. In general, higher scores indicate a higher level of hope. The validity estimate of Snyder Hope Scale has also been mentioned through appropriate content analysis, and its validity has been reported to be above 0.7. Snyder (2000) reported the reliability of this tool through retesting after 3 weeks as 0.85, 0.81 for the factorial thinking dimension, and 0.74 for strategies (Snyder, 2000). Ghobary et al. (2007) reported the reliability of this instrument in the Iranian student population through Cronbach’s alpha as 0.82 for the total scale, 0.79 for the factorial thinking subscale, and 0.88 for the strategies. The validity and reliability of this questionnaire were evaluated and confirmed in this study. CVI for the entire questionnaire was 0.88. The reliability of the instrument was assessed using Cronbach’s alpha, and Cronbach’s alpha for the entire questionnaire was 0.86. For the repeatability of the questionnaire, ICC was calculated and was 0.90 for the entire questionnaire (Ghobary et al., 2007).
Data Analysis
Demographic characteristics were summarized using statistical measures such as mean ± standard deviation and frequency (percentage). Total scores (calculated as the mean of all items per instrument) were used for each questionnaire in the analyses. Variables showing a correlation with age at first childbirth (p value < .2 in univariate linear regression) were included in a multiple linear regression model. Data analysis was conducted using SPSS 26, with statistical significance set at p < .05.
Results
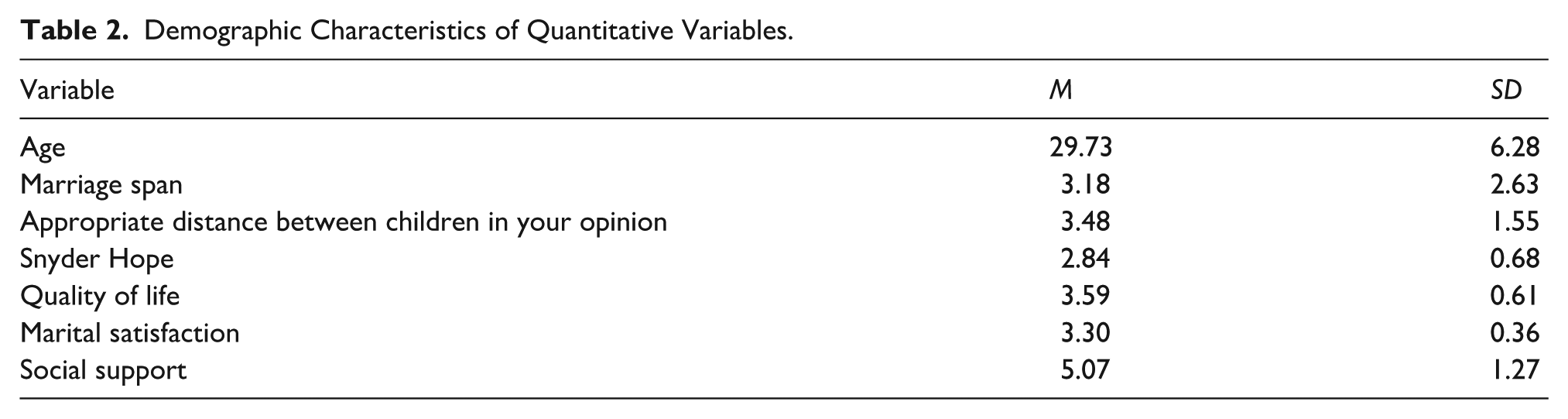
A total of 290 men who had their first child participated in the study, with a mean age of 29.73 years and a standard deviation of 6.28 years. Information and statistics on qualitative demographic variables are reported in Table 1, and statistics on quantitative variables and the four questionnaires they completed are reported in Table 2.
Demographic Characteristics of Qualitative Variables.

Demographic Characteristics of Quantitative Variables.
Initially, univariate regression analysis was performed on individual variables to identify those most strongly associated with the age at first childbirth. Subsequently, variables with a p value < .2, such as ideal spacing between children, marital satisfaction index, marriage span, occupation, family economic status levels, history of illness, access to contraceptive methods, and the person who decides the number of children included in the final multiple linear regression analysis. A model with the highest R² value was determined (R² = 0.256). The results of the univariate linear regression analysis are not reported.
Among the variables included in the multiple linear regression analysis, the indicators of marital satisfaction, duration of marriage, occupation levels, some economic status levels, and the person who decides the number of children had a significant effect on the age of first childbearing. Interpretation of variable for marital satisfaction means that for every 1 unit increase in marital satisfaction, 3.6 years are reduced from the age of first childbearing. This indicates an inverse relationship between marital satisfaction and age at first childbearing. Interpretation of variable for marriage span means that for every 1 unit increase in marriage span, 0.8 years are increased from the age of first childbearing, which is logical and obvious. The interpretation for the occupation is that the age at first childbirth in the worker class is approximately 2.9 years higher than the unemployed class. The interpretation for the status of the family economy is that the age at first childbirth in the very poor economic class is approximately 4.3 years higher than the good economic class. This indicates that the better the economic status of men, the lower their age at first childbirth. The results of the multiple linear regression analysis are reported in Table 3.
Multiple Linear Regression Model for Factors of Men’ Age at First Childbearing Decision.

Unstandardized coefficients, b confidence interval, c reference category (R2 = 0.256, F = 7.95, p < .001).
Discussion
This study identified key determinants influencing men’s age during their first transition to fatherhood in Iran, emphasizing marital satisfaction, duration of marriage, occupational and economic status, and decision-making dynamics within couples. The influence of these factors in various dimensions’ shapes and interacts with an individual’s decision-making during the childbearing years. The results of our study showed that relationship factors, such as marital satisfaction, have a greater impact on fertility, with higher satisfaction being associated with earlier childbearing. Testa and Bolaño’s (2021) study reported that greater relationship harmony increased reproductive motivation among couples, which is consistent with the results of our study. In a similar study, Faghani Aghoozi et al. (2020) found that men’s satisfaction with their marital life has a direct impact on their desire to start having children and shows that emotional stability facilitates early family formation. Probably, higher marital satisfaction significantly shortens the age of fatherhood for men. Parallel research on men is scarce, or existing work is often limited to descriptive surveys.
While, in different communities, the duration of marriage tends to increase, and the age of childbearing rises for both women and men, the results of this study indicated that the duration of marriage was positively correlated with men’s age at first fatherhood. With longer marriages, this finding often indicates a delay in childbearing, which aligns with the findings of Datta et al. (2023), suggesting that couples tend to prioritize stability before conception. Conversely, earlier marriages may accelerate family planning, highlighting the interrelation between relational maturity and reproductive timing. In addition, prolonged marital duration may reflect changes in social norms and life-course expectations (Berrington & Pattaro, 2014), where couples devote more time to strengthening emotional bonds and achieving personal or professional goals before entering parenthood.
Economic and occupational status was also significant predictors of first-time fatherhood. Based on scientific evidence, socioeconomic status (SES) plays a critical role (Lazzari et al., 2023). The results of the study by Šprocha and Fitalova (2022) indicated that financial security often precedes the decision to have children. At the national macroeconomic level, economic conditions, including employment status, occupational stability, and income levels, are directly associated with fertility behavior (Vignoli et al., 2020). According to the study by Tavousi et al. (2016), the reluctance of couples to become parents is associated with the family’s financial situation and the broader economic conditions at the national level. Men with lower economic resources or precarious employment tended to delay childbearing. Whereas those with stable or higher-income occupations became fathers earlier. Similar associations have been observed across diverse settings, where financial security is perceived as a prerequisite for parenthood (Šprocha & Fitalova, 2022; Vignoli et al., 2020). These findings underscore the critical role of socioeconomic stability in fertility decisions, particularly in cultural contexts where men are viewed as primary providers (Queisser et al., 2023). Social and economic factors are significant in men’s childbearing decisions. In a study examining the factors influencing the decline in fertility interest among married Iranian adults by Haerimehrizi et al. (2017), concerns about the child’s future (76.1%) and economic challenges (71.0%) were reported as primary factors. Vahdani et al. (2017) demonstrated that Poor economic status, increased literacy rates, and cultural activities are inversely related to fertility.
Based on the results of our study, the age of childbearing was higher among employed individuals. Employed men often experience greater fatigue and longer working hours due to economic pressures, leaving couples with less time for sexual relations. As a result, the average age of fatherhood in men was approximately 3 years higher. Dual-earner couples may also face additional challenges related to child care and the cost or availability of hiring a baby. Many studies have shown that men with higher occupational status (such as jobs with higher education or managerial responsibility) delay childbearing (Zwier et al., 2024). An analysis of the NLSY79 data found that men who become fathers later in life (i.e., after the age of 30) typically possess greater human capital (higher levels of education and occupational status) and work longer hours (Astone et al., 2010). Job-related pressures and the pursuit of career stability are key factors contributing to this delay. Furthermore, studies examining fatherhood and work patterns suggest that men with higher incomes, or those whose spouses have lower incomes, are less likely to reduce their working hours after becoming fathers, which may introduce additional economic and occupational pressures (Weinshenker, 2015).
As we know, the decision to their first transition to fatherhood a pivotal moment in the life course of individuals and couples, carrying profound demographic, social, and psychological implications. Based on the result of this study, the finding that shared decision-making couple about the number of children reduces men’s age at first fatherhood highlights the importance of shared reproductive autonomy. This is consistent with the results of Kaboudi et al. (2013) who emphasized that shared decisions increase readiness and confidence for parenthood. Which partner decides on the number of children to have affects fertility outcomes; in a way that joint decision-making between men and women about having children is associated with a lower age of first fatherhood compared to unilateral decision-making by women (Duvander et al., 2020). These findings are consistent with the results of our study. This is while, government incentives in Iran for the first childhood have failed, resulting in a halt in population growth and a decrease in the birth rate. Furthermore, the effective implementation of economic policies within families can have a positive impact on the childbearing intentions of young couples (Hosseinpoor et al., 2016). Understanding men’s perspectives is essential, as their economic circumstances, occupational stability, marital dynamics, and agency in decision-making collectively contribute to the timing and willingness to embark on parenthood (Wei et al., 2018). In the study by Hashemzadeh et al. (2022), the creation of a safe environment, the facilitation of work–life balance for couples, the implementation of health promotion programs, the presence of child have centered social support, and the enhancement of socio-cultural relationships was considered part of these policies (Hashemzadeh et al., 2022). Such partnership-based approaches to fertility planning can strengthen couple communication and lead to more timely childbearing decisions. Future research using longitudinal designs is recommended to explore how these factors evolve and interact over time.
Collectively, these results indicate that psychosocial and economic determinants interact to shape men’s readiness for parenthood. Strengthening marital relationships, improving economic stability, and promoting couple-based fertility counseling could facilitate healthier and more timely family formation.
Strengths and Limitations of the Study
Strengths of the study include the innovative nature of the topic, its focus on the male target population, and the large sample size. Data collection was conducted over a defined period in 2023 using cluster sampling across health centers, which enhanced population coverage and minimized selection bias. However, recruiting and accessing newly expectant fathers presented logistical challenges, and reliance on self-reported questionnaires may introduce response bias. The cross-sectional design limits causal inference, preventing analysis of temporal dynamics and long-term trends in fertility decision-making. Importantly, the study was unable to evaluate macro-factors and dynamic socioeconomic variables. These could include shifts in national parental leave policies, changes in housing costs or availability, inflation rates, or health insurance coverage, each of which may substantially affect fertility decisions at the societal level. For example, empirical evidence suggests that extending parental leave and improving social policy benefits can advance both the timing and likelihood of childbirth in certain populations, while adverse economic shocks or restrictive policies may delay family formation. Longitudinal investigation of such impacts in Iran and similar contexts remains a critical unmet need. Future research should leverage cohort or longitudinal designs to capture the effects of policy shifts, economic volatility, and evolving social norms over time. Extending study populations to include those with subsequent pregnancies as well as diverse household structures (such as unwed or, where culturally relevant, same-sex couples) would also expand understanding of fertility determinants. Comparative analyses between urban and rural settings and inclusion of stress and mental health measures could further illuminate mechanisms underlying parental decision-making.
Conclusion
The results of this study demonstrate that men’s initial decisions to have children are influenced by the dynamic interplay of marital age, SES, relationship quality, and joint decision-making between partners. By emphasizing men’s perspectives, this research contributes novel insights to public health and reproductive sciences. Given the significant role of men in fertility decisions, it is imperative for governments and policymakers to design and implement targeted reproductive education and family planning programs that actively involve men. Such efforts should address known barriers including cultural taboos and insufficient educational resources, tailoring interventions to be culturally sensitive and accessible, especially in rural areas where knowledge gaps are more pronounced (Hoseini et al., 2025; MirzaiiNajmabadi et al., 2019). Policymakers should prioritize comprehensive fertility awareness campaigns, promote couple-based counseling services, and invest in training male health care providers to support men’s reproductive health needs. These strategies are essential for enabling informed decision-making by couples and may contribute to reversing declining fertility trends in Iran.
Footnotes
Acknowledgements
This study was the result of a project at Mashhad University of Medical Sciences. The authors appreciated the cooperation of the honorable Research Deputies at the University of Mashhad, as well as all couples who participated.
Ethical Considerations
This study was approved by the Ethics Committee of Mashhad University of Medical Sciences with code IR.MUMS.NURSE.REC.1400.043. Written informed consent to publish the clinical data was acquired from each participant before enrolment. For illiterate participants, we provided informed consent from their legal guardian/a legally authorized representative.
Author Contribution
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be made available on request. The data sets used and/or analyzed during the current study are available from the corresponding author (