
Abstract
Fathers’ mental health and behaviors influence child development and partner well-being, yet paternal stress and well-being are frequently overlooked; especially in non-Western settings. The aim of this mixed-methods study was to quantitatively assess the impact of parenting stress on fathers’ overall well-being in Ghana, West Africa; while qualitatively delving into their lived experiences as fathers. We used a qual/quant mixed-methods approach in this study. The study was conducted in three distinct locations in Ghana (a) Ada, a rural community on the Southeastern coast; (b) Kumasi, an urban setting in upper Southern Ghana; and (c) Sunyani, a peri-urban setting in West-central Ghana. Paternal stress was measured with the Aggravation in Parenting Scale (APS) and well-being was assessed using the Secure Flourishing Index (SFI). Textual data from focus group interviews were sorted using inductive coding and aggregated into overarching themes. Thirty-eight Ghanaian fathers ages 21 to 74 years participated in the study, average age 43 (±12.12 SD), median 39.5. Correlation analyses showed a strong, negative association between paternal stress and well-being (R = −0.63; p < .0001), which was supported in linear regression models (β = −1.04; 95% CI: −1.62, −0.45; p<.0001). Emergent themes of fatherhood stress included financial (employment, food, education, and health care), social (norms and expectations), and psychological (mental work, discipline, relationships, and coping strategies) stressors. A fourth overarching theme of pride and joy in parenting permeated the interviews. Ghanaian fathers with higher parenting stress experience lower overall well-being. Identified stressors could guide interventions that bolster the well-being of fathers and their families.
Introduction
Over the past three decades, there has been increasing focus around the globe on the role of fathers within Maternal and Child Health (MCH) (United Nations Population Fund [UNFPA], 1995). Paternal factors directly impact MCH outcomes in a multitude of ways (Barker et al., 2010; Bond, 2010; Garfield, 2018; Teitler, 2001). Paternal involvement increases breastfeeding rates and the likelihood of appropriate prenatal care. In low-resource settings, it is associated with improved maternal mental health and increased utilization of skilled birth attendance and postnatal care (Garfield, 2018; Yargawa & Leonardi-Bee, 2015). The field of child development has extensively documented how paternal characteristics and behaviors can affect children’s development (Bögels et al., 2008; Lamb, 2010). Children of those positively engaged in fatherhood demonstrate higher academic achievement, self-esteem, and stress tolerance (van der Gaag et al., 2019). Conversely, paternal depression is associated with child conduct problems and internalizing behaviors (Kane & Garber, 2004; Ramchandani et al., 2005). Paternal health and well-being, which in turn impacts paternal behaviors, play a critical role in the paradigm of human development, impacting not only fathers but also their children and families.
Despite growing evidence demonstrating fathers’ influence on the health of their families throughout pregnancy and childrearing, men continue to be underrepresented in MCH research; we continue to leave the “F”-for fathers- out of “MCH.”(Lu et al., 2010) In our gendered world in which women frequently occupy socially marginalized roles and carry much of the burden of reproduction and unpaid domestic labor, the focus on women and children is justified (van der Gaag et al., 2019). Nevertheless, by undervaluing the pivotal role of fathers, the field falls short of fully addressing the sociocultural context within which reproductive and maternal and child health are embedded.
The demands of parenting are stressful (Barroso et al., 2018). The challenges of managing children’s behavior in chaotic homes are further exacerbated by limited economic resources (Crnic & Greenberg, 1990; McQuillan et al., 2019). Parenting stress remains largely undocumented in sub-Saharan Africa and previous studies have focused predominantly on mothers (Barroso et al., 2018; Kanter & Proulx, 2019; Mark et al., 2021; McQuillan et al., 2019). Despite a scarcity of data exploring how parenting impacts fathers, initial studies conducted predominantly with Western populations suggest the experience of fatherhood can elicit psychological distress including depression and anxiety (Garfield et al., 2014; Paulson & Bazemore, 2010). Fathers in underresourced settings may have greater stress than that reflected in this literature. Literature from Ghana has highlighted men’s authority in household decision-making and allocation of resources (Fuseini et al., 2019; Ghana Statistical Service [GSS], Ghana Health Service [GHS], & ICF International, 2015). In Ghana, fathers are heads of households and, within the context of child care, men are financial providers and decision makers (Fuseini et al., 2019; GSS, GHS, & ICF International, 2015). Men are considered affectionate and loving when they provide material resources for their families (Coe, 2011). Women often assume the majority of the direct child care responsibilities, with studies indicating that both genders view men as less able to assume these direct caretaking roles than women (Adama et al., 2017; Dumbaugh et al., 2014). Active male involvement in child care is only recently (i.e., within the last decade) becoming popular and sociocultural expectations of men as providers are often cited as barriers to male involvement in child care. On one hand, Ghanaian men’s roles as primary providers and decision makers has the potential to improve maternal and child health outcomes and begs for more paternal involvement in MCH endeavors (Ameyaw et al., 2016; Ganle et al., 2015). On the other hand, the responsibility of being primary breadwinners and decision-makers may also add additional stress. To our knowledge, no research has explored the impact of parenting on Ghanaian fathers’ overall well-being.
The aim of this mixed-methods study was to quantitatively assess the impact of parenting stress on fathers’ overall well-being in Ghana; while qualitatively delving into the lived experiences of fathers in this low-resource setting. The primary hypothesis of our quantitative analyses was that fathers with higher levels of parenting stress have lower overall well-being. We then used qualitative grounded theory to allow fathers the opportunity to use their own words to contextualize their parenting experiences.
Method
Setting and Participants
Following approval from the University of Institutional Review Board (IRB) and Ghana’s Council for Scientific and Industrial Research (RSRB # 00003844), we conducted a survey and focus group interviews with fathers (n = 38) in three areas of Ghana in November and December 2019 (Figure 1). Participants were recruited through snowball sampling in collaboration with the Women and Children Health Advocacy Group (WaCHAG)-Ghana, a non-governmental agency working to reduce maternal mortality and advocate for better health conditions for Ghanaian families. Participant eligibility requirements were: (a) being male, (b) being 18 years or older, (c) residing in Ghana, and (d) self-identifying as a father. Study recruitment was done in person or by phone. Our snowball sampling scheme began with WaCHAG identifying men in their network who fit the study’s eligibility criteria and contacting them in person or via telephone to explain the study’s objective to them. These men then identified and recommended other potentially study participants within their own networks for WaCHAG to contact and screen for eligibility. This snowball sampling technique was followed until a quorum was gathered in each of the three communities of interest. The three communities were (Figure 1): (a) Ada, a rural community on the Southeastern coast; (b) Kumasi, an urban setting in upper Southern Ghana; and (c) Sunyani, a peri-urban setting in West-central Ghana (United Nations Department of Peacekeeping Operations Cartographic Section, 2005). We chose these three sites because we wanted to reflect the experiences of a heterogeneous mix of Ghanaian fathers whose lives span a range of lifestyles in rural, urban, and peri-urban settings, and who would have a range of family sizes, educational attainment, and employment statuses. In the coastal community of Ada, for example, men tend to have lower educational attainment, have large families, and rely on fishing for their livelihood. Home to 76,411 people, Ada is considered a “paradise town” for its serene beaches and getaway lifestyles (City Population, 2022a; Ghana Tourism Authority, 2022), although the socioeconomic status of fathers in this community tends to be lower than those in more urban Kumasi and Sunyani. Kumasi, the “Garden City” is the capital city of the Ashanti Region, strategically located in south-central Ghana where all major roads converge at the city center. It is Ghana’s second largest city after the capital city, Accra, and home to 2,035,064 people. Kumasi is an important educational center, boasting 649 public pre-primary, primary and junior high schools, two top public universities, one of the nation’s premiere medical schools and a polytechnic (City Population, 2022b; Millennium Cities Initiative, 2022). North of Kumasi is Sunyani, the capital of the Brong Ahafo Region of Ghana and home to 74,240 people. Known as the “food basket” of Ghana, Sunyani serves as a transit for travelers from the South to the Northern part of Ghana. Although considerably smaller than Kumasi, Sunyani is growing rapidly and serves as an important hub for the distribution of the country’s natural resources between the southern and northern parts of the country. The peri-urban city is home to several higher education institutions as well and a domestic airport (Britannica, 2013; City Population, 2022b, 2022c). Whereas travel to Ada is completed via road transport, reaching Kumasi or Sunyani can be accomplished via road or domestic aircraft to the Kumasi or Sunyani airports respectively.
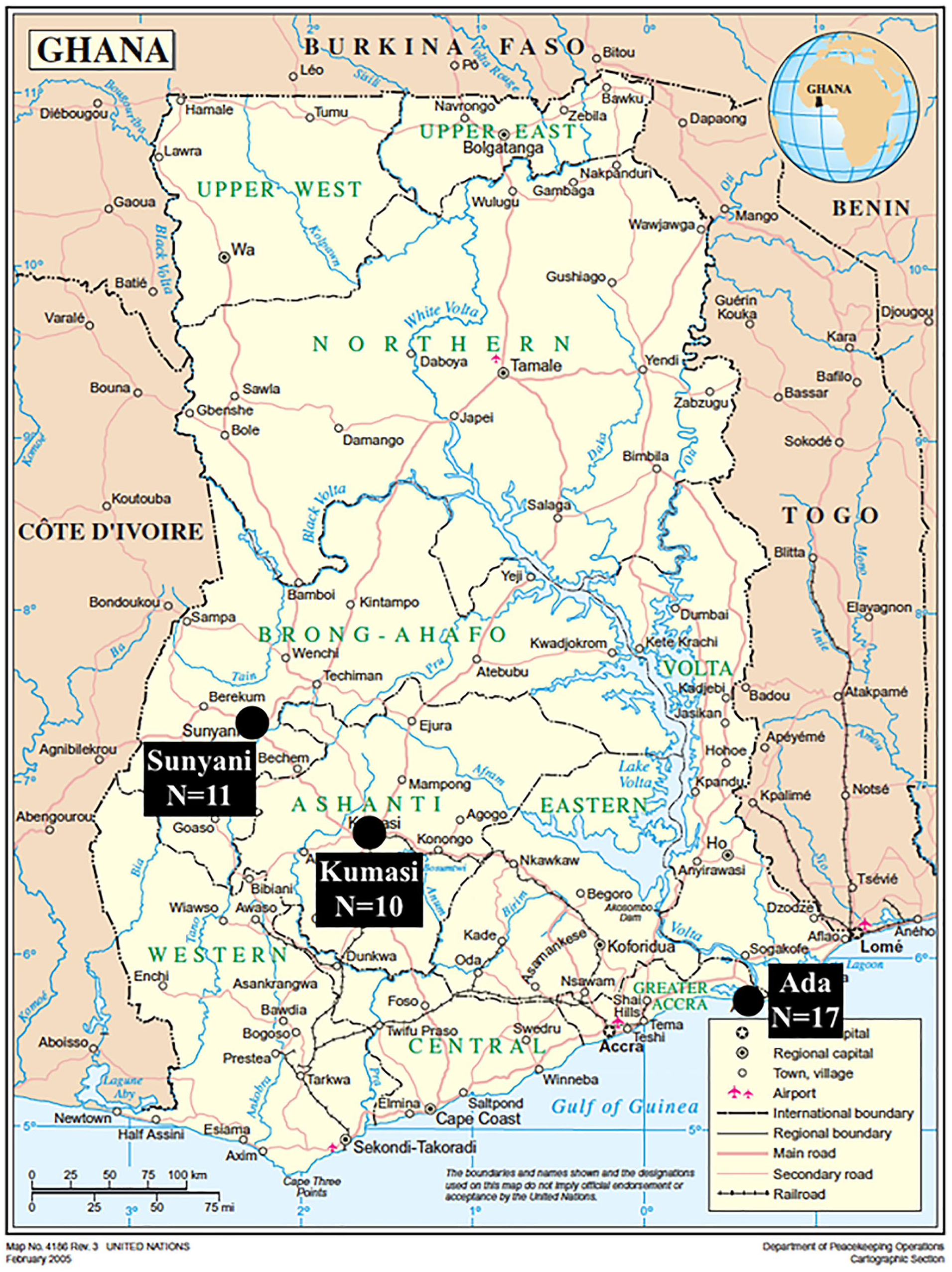
Map of Ghana, With Study Sites Labeled.
Procedures
Data collection included an individual survey and follow-up focus group interviews in each study site. Written informed consent was obtained from all participants. The process of gaining consent, the survey, and the focus group processes were conducted in-person, with trained interpreters. Co-author J.O.A. supervised and verified all interpretations for accuracy. All study participants were provided information sheets detailing the study procedures, monetary incentivizes, and refreshments. Participants were explicitly informed about the research purpose and motivation, the primary interviewer’s (A.B.) experience with Ghanaian and other African community-oriented research, that of the co-authors, and then offered opportunities to ask questions. Participants were also provided the contact information for the researchers both locally and internationally. No participants dropped out or refused participation.
Paternal stress, the predictor of interest, was evaluating using the Aggravation in Parenting Scale (APS) (Ehrle & Moore, 1997). The APS has been used to assess parental stress in various ethnic, racial, low-income, and immigrant populations; and has been reported to have strong psychometric properties (Bendheim-Thoman Center for Research on Child Wellbeing, 2018; Yu & Singh, 2012). Although the APS is sometimes modified to be a three or four question survey, this study maintained the full nine question scale as developed and outlined by the Fragile Families and Child Wellbeing Study, derived initially from the Job Opportunities and Basic Skills Training Program Child Outcomes Study and Panel Study of Income Dynamics (Bendheim-Thoman Center for Research on Child Wellbeing, 2018; Moore et al., 2005; Murphey et al., 2014). The survey has nine items, each scored on a 4-point Likert-type scale that ranges from 1 (strongly disagree) to 4 (strongly agree) on questions asking how often in the last month the caregiver felt the child was harder to care for than expected, did things that bother them, and how much the caregiver feels they are giving up much more of life to be a parent than expected. As in the Fragile Families study (Bendheim-Thoman Center for Research on Child Wellbeing, 2018), scores from all items were summed (resulting in scores ranging 4–36) then divided by the total number of items to generate the reported mean score ranging from 1 to 4. Higher values were indicative of greater parental aggravation (Moore et al., 2005).
Fathers’ well-being, the outcome of interest, was evaluated with the Secure Flourishing Index (SFI), which assesses well-being beyond physical and mental health (VanderWeele, 2017). The concept of flourishing recognizes humans as complex social beings and health as more than simply the absence of pathology (VanderWeele et al., 2019, 2020). The SFI assesses six domains: (a) happiness and satisfaction, (b) mental and physical health, (c) meaning and purpose, (d) character and virtue, (e) social relationships, and (f) financial and material stability (VanderWeele, 2017). The questions were developed from prior validated measures with frequent use in literature and further validated in five culturally distinct settings, including low-resource sites across the globe (Weziak-Bialowolska et al., 2019). The scale contains 12 items, each scored on a numeric scale ranging from 0 to 10 with 0 (least favorable response) and 10 (most favorable). The Secure Flourishing Index score is obtained by summing the scores from the twelve questions in all six domains and results in a score from 0 to 120. Often, for purposes of interpretation, the secure flourishing score is reported as an average of the questions (rather than sum) so that all scores are on a scale of 0 to 10. Higher scores are indicative of greater flourishing (VanderWeele et al., 2019, 2020).
The lived experience of fatherhood for participants was explored through semi-structured focus group interviews. The interview guide was face and content validated by key informants on the research team and co-authors, R.S.K. and J.O.A., both of whom are Ghanaian nationals, and was pretested with a subgroup of Ghanaian fathers to ensure cultural validity prior to study commencement. R.S.K. is a nurse midwife and founder of WaCHAG. WaCHAG is a non-governmental organization whose main focus is on reducing maternal mortality and advocating for better health conditions for Ghanaian women and their children. Her work focuses on improving the quality of life of children and women through advocacy and public education. She served as the in-country supervisor for the project, and was involved in all stages of the study’s development from inception, recruitment, data validation and manuscript preparation. J.O.A. is a founding member WaCHAG. He holds a Bachelor’s degree in Psychology from the University of Ghana, and is a community health advocate and active volunteer. He doubles as a radio broadcaster for one of Ghana’s national radio stations. His radio health programs focus on improving health care delivery for pregnant women and their families. He has been at the forefront of using the power of radio to inform interested participants about WaCHAG’s public education initiatives. A multi-lingual, well-respective professional and father, J.O.A. facilitated all the interviews and was involved in all stages of the study’s development from inception to recruitment to data validation and manuscript preparation.
Four focus group interviews were conducted in Kumasi (1), Sunyani (1), and in two distinct communities in Ada (2). Focus groups were facilitated by A.B., first author and experienced interviewer who was doing a 1 year research clerkship in Ghana as part of her medical school training; under the supervision of M.A.O., a Ghanaian native. The interviews were conducted in dedicated community spaces in Ada and Sunyani, and in a university conference room in Kumasi. Only researchers and study participants were present for interviews. Interviews lasted no longer than an hour. Interviews were audio-recorded, and non-English elements of the interviews were translated by J.O.A. and other trained interpreters. A.B. took field notes during and after each interview. Interviews were subsequently transcribed in English. Questions guiding the conversations included: “Tell me about parenting. What is it like?” “What does “stress” mean to you?” “How do you feel that your stress levels were affected when you became a father?” “How was your stress level before you were a father?” “How do you cope with the stress of being a father?” “What is something that you would like to see implemented within your community to assist fathers in coping with parenting stress? For expecting fathers? New fathers? Experienced fathers?”
We used a concurrent triangulation mixed-methods study design for this project, where both the quantitative and qualitative data were collected concurrently, but separately, with equal priority and are “mixed” during the interpretation or analysis phase of the study to verify or substantiate the overall findings (Creswell & Plano Clark, 2011; Creswell et al., 2008).
Analysis
Analysis of the mixed-methods study addresses the relationship between stress and well-being of fathers. First, to examine the relationship between paternal stress (APS) and well-being (SFI), we used Stata® software to perform correlation and linear regression analyses to examine the relationship between APS and SFI scores. We estimated a correlation between the variables, and used linear regression models to determine an effect size. Covariates were chosen based on potential confounders identified in prior studies and included age, marital status, educational attainment, employment status, household size, and location (Ehrle & Moore, 1997; Schieve et al., 2011; Weziak-Bialowolska et al., 2019; Yu & Singh, 2012). A cutoff of p < .05 was used to determine statistical significance. We prioritized the father’s lived experiences and the context of their parenting experiences rather than the number of respondents. Thus, the study’s sample size was not driven by statistical significance, but rather saturation of themes in the qualitative design and the clinical and contextual significance of the findings. Following the quantitative analyses, transcripts and field notes were analyzed by the research team using Dedoose™, a web-based software that facilitates multi-layered qualitative data organization, enabling meaningful analysis (SocioCultural Research Consultants, 2020). Directed content analyses were performed in which recurring topics were coded and an iterative codebook was generated (Hsieh & Shannon, 2005; Pope et al., 2000). Salient themes were validated by community members (both by study participants and nonparticipant community contacts) in addition to research team members. As an iterative code tree was generated, and codes were removed or consolidated if not used. Codes were aggregated into overarching themes and sub-themes. Codes showed that saturation had been reached in the four focus groups. After preliminary coding and theme identification, data was presented to study participants via study site meetings and via handouts. This study followed Consolidated Criteria for Reporting Qualitative Research (COREQ) reporting standards (Tong et al., 2007).
Results
Sociodemographic Characteristics
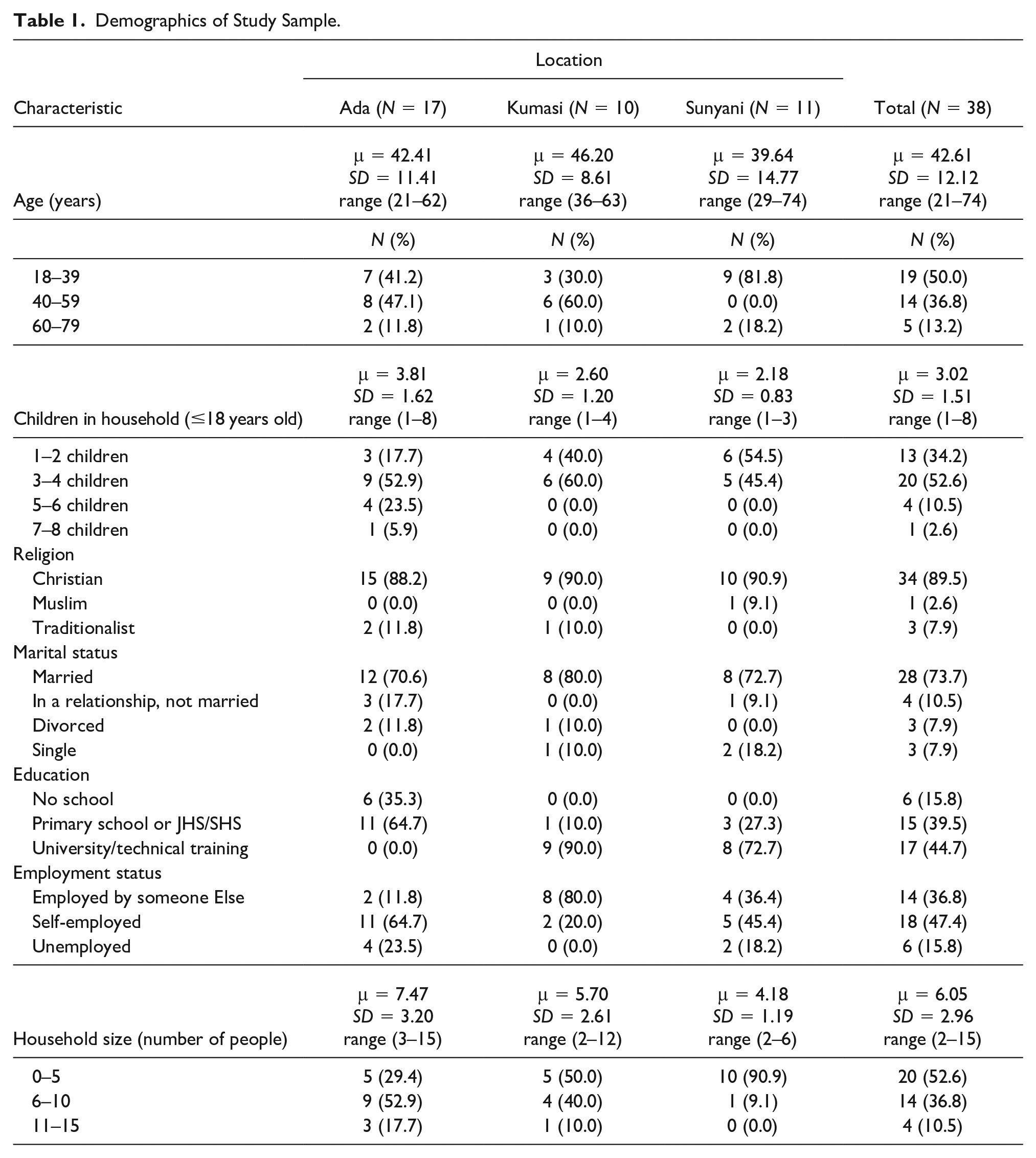
A total of 38 fathers participated in the study. Table 1 reports selected sociodemographic characteristics of the sample population. The mean age of fathers across the sites in this study was 43 (±12.12 SD, range 21–74, median 39.5). Participants in Kumasi (n = 10) and Sunyani (n = 11) tended to be more educated than those in Ada (n = 17), where a third of the fathers had no formal schooling. Across all sites, 73.7% (n = 28) of participants were married or in a relationship. The majority of fathers (84.2%, n = 32) were employed, and the average household size was 6 (±2.95 SD, range 2–15). The mean number of children ≥ 18 years old living in the participants’ households was highest in Ada (3.81 ± 1.62 SD, range 1–8) as compared with Kumasi (2.60 ± 1.20 SD, range 1–4) and Sunyani (2.18± 0.83 SD, range 1–3). At the time of the study, seven of the 38 participants (18.4%) were expecting another child.
Demographics of Study Sample.
Quantitative Findings
The mean APS and SFI scores were 2.67 (±0.65 SD, range: 1–3.67) and 7.03 (±1.22 SD, range: 5.09–10). Correlation analyses showed a strong, negative association between paternal stress and well-being (R = −0.63; p < .0001, Figure 2), which was supported in linear regression models (β = −1.04; 95% CI: −1.62, −0.45; p < .0001, Table 2). Fathers with higher levels of parenting stress had worse overall well-being.

Relationship Between Paternal Stress (Aggravation in Parenting Scale) and Overall Well-Being (Secure Flourishing Index).
Linear Regression Effect Estimates of Changes in Paternal Well-Being Associated With Increasing Paternal Parenting Stress a .
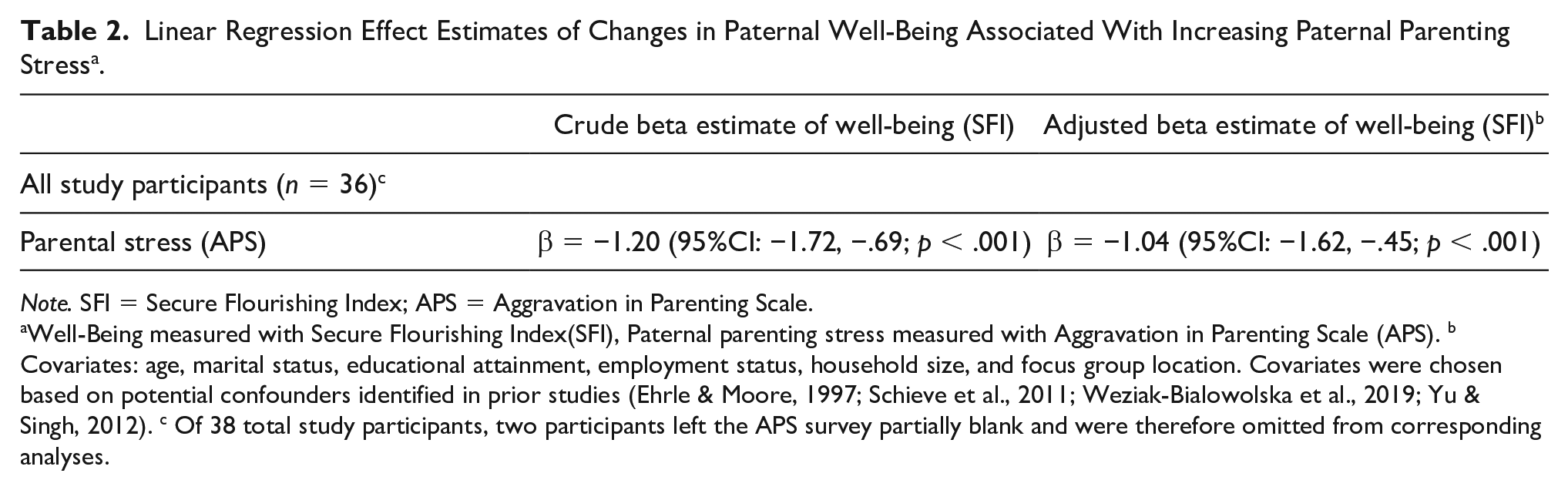
Note. SFI = Secure Flourishing Index; APS = Aggravation in Parenting Scale.
Well-Being measured with Secure Flourishing Index(SFI), Paternal parenting stress measured with Aggravation in Parenting Scale (APS). b Covariates: age, marital status, educational attainment, employment status, household size, and focus group location. Covariates were chosen based on potential confounders identified in prior studies (Ehrle & Moore, 1997; Schieve et al., 2011; Weziak-Bialowolska et al., 2019; Yu & Singh, 2012). c Of 38 total study participants, two participants left the APS survey partially blank and were therefore omitted from corresponding analyses.
Qualitative Findings
Three focal themes related to parenting stress emerged from the analysis focus group interviews: financial, social, and psychological stressors. A code tree was generated from correlated subthemes (Figure 3) and a fourth overarching theme of pride and joy in parenting permeated the interviews. Findings from the focus groups capture the perceptions and experiences of stress and well-being of the participant fathers.

Qualitative Code Tree Displaying Themes and Sub-Themes That Emerged Textual Data to Guide Analysis.
Financial Stressors
Fathers’ stress related to securing employment and steady income, mitigating food insecurity, and supporting children’s education and health care emerged across all focus groups. Nearly 50% (n = 18) of participants described themselves as self-employed. The relationship between precarity of self-employment and the risks to securing a steady income was a common stressor and the first mentioned by each focus group. One participated stated: Everything will become a problem . . . [Look] at the cost of things and, remember, as the time goes on, there is an inflation going up and your salary remains the same . . . How are you going to meet your [family’s] needs? (Sunyani)
In the farming communities of Ada, where economic success is driven by agricultural yields and subsequent sales, concerns over land degradation, production limitations during the dry season, and related access to water for irrigation were frequently raised. One father highlighted this stating: Anything that could help [us] do farming and get [any] amount of money is very good. [We] have a source of water over here but the bill that comes . . . is also another source of worry . . . If this basic thing about life, a job, is resolved, it [would] go a long way to resolve [our] issues. (Ada)
When later asked about possible interventions that participants could foresee alleviating their fatherhood-related challenges, respondents again returned to the topic of employment: The stress [comes] from people not really having good jobs to take care of their children so if job creation should be created, it [would] limit to a very high extent the kind of stress that comes with childbearing. (Ada)
The stress of securing employment and its connection to land and food security was contextualized as participants described the “needs” they were concerned about meeting, often as fundamental as providing food. A common refrain from the fathers was that they felt responsible for the daily survival of their children and families: A father . . . has a responsibility of ensuring that the mother and the children have food on the table. So, on a daily basis, a father is on the run, . . . [always] looking for something for the family. That’s fatherhood in this community. (Ada)
This struggle to afford food creates dilemmas for fathers, who must decide between feeding their children or paying for school or recreational activities. Small daily choices to provide entertainment or recreation may be impactful on well-being: Sometimes you have to sacrifice . . . for a child to attend . . . sports. But . . . when you take that [5 cedis] from your pocket it means that whole week, the whole family will not eat. Let’s say you have three children. They are all going for that same sports activity. See that kind of stress? (Sunyani)
As a participant stated, the way we acquire education is by money (Ada) and the father’s desire to provide good education for their children was of major financial concern. School fees were often cited as enormous, and sometimes insurmountable, financial burdens.
Because of poverty and lack of funds, you are unable to take care of your children as you wish to, and it may cause the children to stop schooling. (Ada)
Another stressor was health care-related stresses, which frequently arose in the context of unforeseen circumstances that create unexpected financial burdens: You may be unfortunate and . . . give birth to a sickle cell child or a child with a special kind of disease and you try to treat that sickness, but you waste a lot of money on that and later you lose the child. It’s a very big difficulty and challenge. (Ada)
Participants perceived interventions that specifically targeted health care costs as alleviating fatherhood stress: In this community, we have the traditional birth attendants . . . We don’t end up wasting a whole lot of money at the hospital [because] the traditional birth attendants help so it helps to minimize troubles that come with fatherhood. (Ada)
Social Stressors
Integral to Ghanaian communities is the understanding that “every man needs to be a father.” Participants described fatherhood as a societal expectation and an essential aspect of one’s masculine identity: Every man needs to have the mind that one day he will not be alone, . . . he will have to marry . . . [and] take care of the children. (Kumasi)
Norms surrounding childbearing incited feelings of pressure prior to having children, stress and shame about infertility, and feeling “pitiful for those who do not have children.” With the attitude that “[if you are] unable to bear a child, it is a trauma in our Ghanaian society . . . [you] become a laughingstock,” participants described their stress leading up to the birth of their first child and the subsequent relief once the child was born and “all the pressure had gone”: In our community, sometimes when a man and woman get married, . . . people psychologically are expecting children within some amount of years so if there is no child, they begin to ask questions. So, when . . . your wife gets pregnant and then gives birth for the first time, you have some inner fulfillment . . . that you have satisfied community demand. (Kumasi)
Even when not feeling prepared to have children, interviewees stated there was no choice but to have children as the “social obligation” overshadowed the stress of supporting children: If you are an African man and you are not able to give birth, count yourself out of many things. [It] is a whole stress in our life. People will be pointing their fingers on you, [saying] this is the man who is not able to give children. (Sunyani)
Psychological Stressors
Although fulfilling the expectation of reproduction brings relief, participants emphasized that parenting brings forth a host of familial, marital, and relationship challenges. Fathers in each group noted a significant shift in perspective when they became fathers, as they could not “think as an individual any longer, you think about other people and take responsibilities for other people.” Participants did not lament the need for this new mind-set, in fact perceiving it as a positive change that “makes you learn a lot of senses” and generally “go up in life.” Fundamental to participants’ definitions of fatherhood was the role as head of house and leader of the family: It brings up new kind[s] of responsibilities trying to counsel, trying to put them on the right path and also meeting with their mother regularly to think about the progress of the child. Even when there isn’t money, how do you think through . . . things. So, fatherhood comes with stages of thinking or different mindset. (Ada)
Participants advocated for family planning to limit the psychological burdens that come with this new mind-set, however Sometimes you wake up late in the night and you really wish to sleep but you can’t sleep because you have to think about certain things at the end of the day . . . and when it happens so, you think “Oh, I don’t really need to be giving birth to a lot of children because it means more stress, so I have to reduce the number of children I have. (Ada)
Reverberating through each focus group was discussions of the tension in marriage and co-parenting when children arrive. Participants noted the challenges of marriage, expressing that it is “the women who are spoiling the children,” and noting the challenges of being the household’s main decision-maker, as “all those demands are coming to a single person as a man.” In addition to the burdens of being the sole breadwinners who are “providing everything,” fathers expressed feeling as though their children felt more cared for by their mothers, who tended to be home more often: Sometimes you will sacrifice and . . . the children will not appreciate [it] . . . You pay school fees . . . Their mother will just give them chop money . . . but they will appreciate that one more than you. (Sunyani) Sometimes we even wake up at dawn. Your kids will not see you as a father. You are gone, you have to go and work . . . They will always be with their mother, so they have love for their mothers. (Sunyani)
Participants did occasionally appreciate the role their partners play in child-rearing, particularly with respect to monitoring children’s behavior and discipline, and acknowledged the stress associated with teaching children to behave well: If you are responsible father, you really feel what women go through. One day I decided to go to church with my little boy without the mother. That day I didn’t hear anything, in fact I realized that when our women go to church, mostly they don’t hear anything because of the childcare. It’s very very stressful, you just give all your attention . . . You want to be inside; they want to be outside . . . By the time they say “amen,” you also say “amen,” without hearing anything. Yes, so the stress comes in various levels the closer you are to the children, sometimes emotionally. (Kumasi)
Mental health care was identified as a helpful resource, though no one expressed having access and several groups described the personal resistance and stigma associated with seeking care: Sometimes you need guidance, planning. You need somebody to guide you in life whether you like it or not. And we lack these things . . . We need counseling centers. (Sunyani)
Participants emphasized the importance of coping mechanisms to combat the mental stressors, citing personal examples such as walks in nature or distractions in the form of movies, books, music, sports, or friends. Their stories relay a belief in the perceived downstream effects of this psychological stress: You have to strategize and find a defensive mechanism to relieve you of the pressure that is coming. If you . . . continue to be harboring all those things you may fall sick and die. (Ada)
Pride and Joy in Fathering
Interwoven into the dialogue of each focus group interview, alongside the challenges, was an overarching theme of pride and joy intrinsic to fatherhood. The men interviewed reported a deep sense of satisfaction and solidified respect within their communities as a direct consequence of their fatherhood status: At least somebody sees you as a hero, [is] attached to you, wants to go out with you, feels comfortable and safe with your bosom. It’s a kind of feeling that you can’t explain. You see, some of these fulfilling moments you can only get through fatherhood and not through any other thing. (Kumasi) In our tradition when a man doesn’t have a child and the man is dead, we say he’s gone but if the person has a child and he’s dead we say he’s left. It means you left something behind. But when you don’t have a child and you die, you are gone . . . So, I’m happy I have a child because tomorrow they will say that I have left something. (Ada)
Often the participants’ children themselves and the countless moments of joy while spending time with them were considered some of the best ways to relieve the stress of fatherhood. From the moments after work when “they see you [and] run to you,” or when “they come and embrace you,” to “the way they talk,” or “crack jokes”; the men offered these as some of the “most fulfilling moment[s]” that filled them with joy: I’ve always wanted to have a child of my own to pass down that kind of care, so when I became a father it was a joy. It was a joy for me and since then I have not looked back. (Kumasi)
Discussion
Fatherhood research consistently suggests higher parenting stress in low-income settings, though the literature disproportionately represents Western populations (Perzow et al., 2018). To our knowledge, this is one of the first studies to evaluate the stress, well-being, and lived experiences of fathers in the African region, filling a much needed gap and enriching the field’s understanding of fatherhood in this non-Western setting. We found evidence to support our hypothesis that Ghanaian fathers with higher levels of stress (APS) have lower overall well-being (SFI). Our results align with the conceptual framework of the Socio-Ecological Model (SEM), used for decades in public health to place individuals within their multi-layered social and ecological contexts (Kilanowski, 2017). In this study, fatherhood can be viewed as existing in complex conjunction with: (a) individual factors, (b) interpersonal factors within the family and close social network, (c) community factors, and (d) public policy factors (McLeroy et al., 1988). Each of these four layers both impacts and is affected by each other layer; and to effectively address public health issues, interventions should act across multiple layers simultaneously (Alio et al., 2010; Centers for Disease Control and Prevention, 2020). For example in our study, fathers identified three main sources of parenting stress in the Ghanaian context: financial, social, and psychological. Study participants described how fatherhood challenges their mental health, relationships, and financial stability, each of which contributes to one’s ability to flourish (VanderWeele et al., 2019). All four focus groups cited challenges with employment opportunities, health care and education costs, and food insecurity. They identified additional sources of paternal stress from social pressure, relationships, and the mental shifts that accompany fatherhood. These stressors, although experienced at the individual level, are impacted by interpersonal, community and public factors that are often outside of the individual’s control. Participants identified immense stress arising from their financial obligations as parents. This “sole breadwinner” stress was exacerbated by the fact that most fathers were self-employed in a strained Ghanaian economy. When fathers express distress over the increasing cost of goods and food insecurity, they are also aware of government policies and environmental stressors that trigger and/or exarcebate these situations. In the Ghanaian setting, where providing material resources for one’s family (Coe, 2011; Ezeugwu & Ojedokun, 2020) is synonymous with being a “good” husband and provider, these exacerbating factors may leave men feeling powerless and out of control in their roles as fathers; prompting behavioral or emotional exhaustion, and decreasing their psychological wellbeing (Amarachi et al., 2020; Kaya et al., 2019).Within the qualitative accounts, psychological stress was prevalent and is consistent with emerging data suggesting fatherhood can negatively impact paternal mental health. A 2010 U.K.-based study concluded that 21% of fathers experienced depression by the time their children were 12 years old (Davé et al., 2010). Studies indicate that paternal depression increases during the first five years of fatherhood;(Garfield et al., 2014) and stress and anxiety have been associated with the transition to fatherhood (Baldwin et al., 2018). In a study by Fast et al. examining masculine idealogies in Tanzania and Kenya, the authors reported increased rates of depression and suicidality among men who were unable to fulfill their expected roles and responsibilities as “financial providers” (Fast et al., 2020). These men, the authors posit, experienced prolonged periods of depression, anxiety, and stress, which had been entrenched and deepened by economic, political, and social uncertainty; before succumbing to taking their own lives to avoid the shame of being “too poor to provide for their families.” Even though there are changes in the fatherhood role in the new African dual-earner families, an adult male is still considered a husband (e.g., with one wife or more), a father (with or without children), an uncle (with responsibilities to others within the extended families), an employee or a manager (fulfilling their job role to the organization), and can also occupy a city or village chieftaincy position within their age grade (Ezeugwu & Ojedokun, 2020; Kelly, 2018). The pressures placed on African men can seem insurmountable and yet an overarching theme that emerged from our study was the sense of pride and joy that fatherhood brings to these men, counter-balancing the stress-related findings. Being a father earned them homage among their peers, re-affirmed their “manhood,” elevated their status in society, and made them heroes in the eyes of their children. Ghanaian men want to, and enjoy being, fathers and must be supported in this role to combat the external stressors. Our study participants emphasized the importance of mental health resources, including counseling, to alleviate the psychological stressors of fatherhood. Such interventions are needed now even more so, in the post-pandemic era, as World Bank forecasts predict that at least 29 million people in the African region will be pushed into extreme poverty by the end of 2021 due to the economic ramifications of the COVID-19 crisis (Human Rights Watch, 2021). Inflation (especially food prices) has risen sharply in Ghana, and its West African neighbors Nigeria and Senegal (Anyanwu & Salami, 2021), prompting the Ghanaian finance minister to request financial interventions from the World Bank and International Monetary Fund (Ofori-Atta, 2020). As sociocultural norms dictate, fathers, deemed heads of households, will bear the brunt of this COVID-induced financial burden. Given the interrelatedness of paternal health to the health of mothers, children and families as a whole, gender researchers should pay close attention to the impact that masculine norms have on paternal health (and by default maternal and child health) in this post-pandemic era (Courtenay, 2002). Interventions that span the interconnected layers of the SEM model to address gender norms, community expectations, and employment policies may alleviate some of the “sole breadwinner” stress imposed on not only fathers, but Ghanaian men overall.
Strengths and Limitations
Although studies have examined paternal involvement in obstetric care in Ghana, to our knowledge this is one of the first studies to document the lived experiences of Ghanaian fathers in a broader parenting context (Aborigo et al., 2018; Craymah et al., 2017; Story et al., 2016). The study’s strengths stem from its mixed-methodology, with narratives from Ghanaian fathers guiding analyses and participants themselves validating the results. Our sample was heterogeneous, spanning from rural to urban, across a wide range of ages, family sizes, educational attainment, and employment statuses. Crucial to the success and impact of this study was the partnership with Ghanaian collaborators at WaCHAG.
This study’s limitations include its small sample size, which made it difficult to conduct more rigorous statistical analyses. Despite the modest sample size, several results were statistically significant, alluding to the salience of the research question. Future studies should recruit larger samples for higher-level regression estimates. It would be worthwhile for such studies to evaluate whether fathers with higher stress levels have increased co-morbidities such as hypertension, coronary heart disease, myocardial infarction, and sudden death, thought to be associated with high-stress lifestyles (Dimsdale, 2008; Steptoe & Kivimäki, 2012). Evaluating the longitudinal impacts on morbidity and mortality would shed light on the implications of parenting stress on men’s overall health. Findings could also be compared with higher-resources settings where fathers may be under less stress. The study limitations illustrate the need for further study of the experiences of Ghanaian and sub-Saharan African fathers, as they are grossly under-represented across the literature.
Conclusions
The well-being of fathers transcends their individual health to impact partner well-being and child development. Our findings call for effective MCH promotion to include fathers, as impactful players and as individuals shaped by their families and experiences. Paternal well-being, particularly in resource-limited settings, is underrepresented in MCH research and warrants investigation. Sources of stress and joy identified by Ghanaian fathers should guide research and interventions to bolster the well-being of not only fathers, but families and communities overall.
Footnotes
Acknowledgements
The authors sincerely thank the Ghanaian communities of Ada, Kumasi, and Sunyani who participated in this study and enabled the authors to learn about their personal experiences as fathers. The authors particularly appreciate the community contacts who helped coordinate focus group interviews and served as liaisons between the fatherhood communities and researchers as well as the chiefs and community leaders who granted access to the focus group populations. The authors also give enormous thanks to the Women and Children’s Health Advocacy Group Ghana for this fruitful collaboration, their vital insights, and the inspiring public health work they are engaged in.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors acknowledge the University of Rochester’s Susan B. Anthony Center, Susan B. Anthony Institute, Office of Global Engagement, Office of Medical Education, and Department of Emergency Medicine for contributing funding to make this Medical Student Year-Out project possible. At the time of press, Dr. Anto-Ocrah was funded by NIH NINDS Grant# K01NS121199.