
Abstract
There is a need for tailored smoking cessation programs specifically for Indigenous fathers who want to quit smoking.The aim of this study was to engage Indigenous men and key informants in guiding cultural adaptations to the Dads in Gear (DIG) cessation program. In Phase 1 of this qualitative participatory study, Indigenous men were engaged in group sessions and key informants in semistructured interviews to gather advice related to cultural adaptations to the DIG program. These data were used to guide the development of program prototypes. In Phase 2, the prototypes were evaluated with Indigenous fathers who were using tobacco (smoking or chewing) or were ex-users. Data were analyzed inductively. Recommendations for programming included ways to incorporate cultural values and practices to advance men’s cultural knowledge and the need for a flexible program design to enhance feasibility and acceptability among diverse Indigenous groups. Men also emphasized the importance of positive message framing, building trust by providing “honest information,” and including activities that enabled discussions about their aspirations as fathers as well as cultural expectations of current-day Indigenous men. That the Indigenous men’s level of involvement with their children was diverse but generally less prescriptive than contemporary “involved fathering” discourse was also a key consideration in terms of program content. Strategies were afforded by these insights for meeting the men where they are in terms of their fathering—as well as their smoking and physical activity. This research provides a model for developing evidence-based, gender-specific health promotion programs with Indigenous men.
Keywords
While acknowledging significant limitations with population health data among Indigenous people (Lovett, Thurber, & Maddox, 2017; Smylie & Firestone, 2015), estimates indicate that smoking prevalence is high in comparison to other groups. For example, current cigarette-smoking rates among Indigenous Canadians 1 are, on average, twice as high as those of non-Indigenous Canadians (33% vs. 17%; Wardman & McKennitt, 2017). Similar disparities in smoking prevalence have been reported among Indigenous populations in Australia (41.4% vs. 14.5%), New Zealand (35% vs. 15.7%), and the United States (31.8 % vs. 15.5%; Jamal et al., 2018; Lovett, Thurber, Wright, Maddox, & Banks, 2017; Ministry of Health, 2017). With a few exceptions, men are more likely to smoke than women (Ng et al., 2014), a pattern that generally prevails among Indigenous men (Lovett et al., 2017; Physicians for a Smoke-Free Canada, 2013). High rates of tobacco use have been directly linked to poorer health and lower life expectancy in Indigenous populations than in the general population (Carson et al., 2014). Results from Canada’s 2012 Aboriginal Peoples Survey identify that 61% of off-reserve First Nations people, 60% of Métis, and 42% of Inuit aged 12 years and older reported being diagnosed with at least one chronic condition (Statistics Canada, 2015). Cigarette smoking is the single greatest avoidable risk factor for cancer, heart disease, chronic obstructive pulmonary disease, and other chronic diseases (Canadian Cancer Society, 2016; World Health Organization, 2016). Although smoking cessation (SC) at any age lowers mortality from smoking-related disease, quitting before age 40 is estimated to reduce the risk of death associated with smoking by about 90% (Jha et al., 2013).
Intensified effort to support SC among Indigenous people is recognized as a global priority (Minichiello, Lefkowitz, Firestone, Smylie, & Schwartz, 2016). Multifaceted and tailored interventions have been developed to reduce tobacco use among Indigenous people (Chamberlain et al., 2016; Minichiello et al., 2016) as well as to support cessation among Indigenous women during pregnancy (Bovill et al., 2017; Gould, Lim, & Mattes, 2017; Greaves, Hemsing, Poole, Bialystok, & O’Leary, 2016). However, no gender-specific and culturally sensitive SC programs have been developed for Indigenous men or fathers. The role of gender-related factors in tobacco use and cessation has been recognized (Bottorff, Haines-Saah, Oliffe, & Sarbit, 2012; Bottorff et al., 2014; Knott, Gilligan, Maksimovic, Shen, & Murphy, 2016) and provides a useful framework for designing tailored approaches to cessation.
Background
The majority of SC interventions focusing on pregnancy, postpartum period, and parenting have targeted women. Less often addressed is men’s smoking, which when continued in fatherhood, reduces the chances of female partners’ SC (Mullen, 2004) and can negatively impact the health of their children as well as their own health. There are also intergenerational connections to smoking. For example, children who grow up with fathers (and grandfathers) who smoke are at increased risk of smoking later in life and often exposed to environmental tobacco smoke (Escario & Wilkinson, 2015). The adverse health effects of children’s exposure to secondhand and thirdhand smoke are well known (DiFranza, Aligne, & Weitzman, 2004; Gurkan, Kiral, Dagli, & Karakoc, 2000; Moshammer et al., 2006; Tebow et al., 2008).That said, there is strong evidence suggesting most fathers want to stop smoking but lack the ways and means to initiate and/or sustain a quit (Blackburn et al., 2005; Bottorff, Oliffe, Kalaw, Carey, & Mroz, 2006; Bottorff, Radsma, Kelly, & Oliffe, 2009; Johnson, Oliffe, Kelly, Bottorff, & LeBeau, 2009; Oliffe, Bottorff, Kelly, & Halpin, 2008). Presenting the incompatibility of smoking and fatherhood affords an important window of opportunity for men-centered approaches to SC. A brief review of SC programs revealed few men-specific SC interventions (Okoli, Torchalla, Oliffe, & Bottorff, 2011). To address this gap, a novel program was designed specifically for fathers who want to reduce and quit smoking.
Dads in Gear (DIG) is a highly innovative group program, supplemented with Web-based resources, that focuses on integrating three critical components: SC, fathering, and physical activity (Bottorff et al., 2017). DIG breaks with the well-worn traditions of focusing on women who smoke in pregnancy/postpartum period by directly messaging men about their health and the connectedness of their smoking practices to the well-being of their family. The design and content of DIG is based on men’s health promotion principles drawn from previous research (Bottorff et al., 2006; Bottorff et al., 2009; Johnson et al., 2009; Oliffe et al., 2008) and best practices related to SC and has been refined with the input of fathers. Physical activity was included to facilitate SC (Roberts et al., 2015) and strengthen engagement in the program by recognizing men’s interest in staying healthy and fit to fulfill their responsibilities as fathers. Accordingly, DIG is the first integrated lifestyle program specifically designed for men that has the advantage of reducing several risk factors simultaneously. The DIG program combines creative, strength-based approaches with knowledge and skills related to fatherhood, smoking, and masculinity. Activity-based, interactive, and themed sessions focus on men being healthy and smoke-free as requisites to being the best dads they can be.
The DIG program involves cofacilitated, weekly face-to-face group sessions over 8 weeks. Each session provides peer support, education, and skill building. Trained male facilitators are provided with a manual, describing the objectives and activities for each session, and supplemental Web-based resources that have been optimized for easy access on mobile platforms. DIG implementation strategies are infused with masculine themes (e.g., hockey, fishing) and men’s preferences related to health promotion (e.g., autonomous decision making, humor). Short information sessions are combined with interactive scenario-based activities to solicit men’s opinions and questions. This program was designed to meet the needs of larger Euro-centric male populations.
To assess the acceptability of the DIG program among Indigenous fathers who smoke cigarettes, the program was offered in one urban and one rural (off-reserve) community in British Columbia, Canada, to 12 Indigenous fathers and one Indigenous grandfather as part of a larger feasibility study. Trained Indigenous male facilitators were provided with the DIG program materials and invited to make culturally appropriate adaptations. Men who self-identified as Indigenous (First Nations or Métis), who had children in their lives under the age of 5 years, and who were interested in SC were recruited through community-based organizations offering services to families via posters and word of mouth. Although the delivery of DIG followed the program protocol, some adaptations were made. Facilitators invited Elders as guest speakers, provided information on traditional tobacco and its use in ceremonies and rituals, and discussed values related to family life and father roles in Indigenous families. Participant feedback at program completion indicated that men valued these adaptations, along with the emphasis on positive fathering, and the opportunity to learn more about fathering and smoking in a men-friendly environment. At the end of the program, 28% reported they were abstinent and 43% had reduced their smoking. These observations and findings supported the acceptability of the DIG program model for Indigenous men. However, the feedback from facilitators and participants indicated a need for cultural adaptations to the DIG program prior to delivery to Indigenous fathers. These included (a) incorporating specific information and discussions on the topic of traditional tobacco use among Indigenous peoples; (b) integrating support for stopping the use of chewing tobacco; (c) including options for physical activity and healthy eating that are feasible in Indigenous communities and reflect Indigenous men’s preferences; (d) extending fathering competencies to include children of all ages; and (e) expanding the focus on fathering to include grandfathers to adequately reflect family life in Indigenous communities (e.g., multigenerational households). This small pilot supports recommendations that a range of factors need to be taken into account in planning health programs for Indigenous people that extend beyond evidence-based SC approaches (Ivers, 2004). The findings suggest that a DIG program designed for Indigenous men who use commercial tobacco products holds potential for engaging men in SC while strengthening their roles as fathers and grandfathers. In addition to promoting men’s health, the program holds potential to afford other positive impacts. As men reduce and quit smoking, exposures to secondhand and thirdhand smoke are also reduced, creating healthier individuals, families, and communities, linking to holistic visions of well-being in Indigenous communities. In addition, by focusing on fathers’ positive parenting, men’s involvement in supporting healthy child development is supported.
Despite the limited evidence base on effective approaches for fatherhood programs, some promising practices for the development of programs for fathers have been identified (Bronte-Tinkew, Burkhauser, & Metz, 2012; Reilly & Rees, 2018). Included among these is the need to design programs in ways that are appropriate for fathers and tailored for cultural groups. Despite this priority, the experiences of Indigenous fathers have garnered limited attention until recent years. In the first study of Indigenous fathers in Canada, fathers were reported to have large, complex families (Ball, 2013). Although all fathers wanted to be positively involved with their children (regardless of their current involvement), opportunities to learn about fathering were impacted by the effects of colonialism and residential schools, the lack of childhood experiences of positively involved fathers, and problems with substance use and mental health that created difficulties in maintaining relationships with partners and other family members. The fathers also pointed to their exclusion from support provided by community organizations and health services where mother and child protection were the dominant focus. Indigenous fathers expressed a desire for male-led, father-friendly programs to support them in assuming positive involved roles as fathers. Based on findings of recent systematic reviews, there remains a critical lack of community-based programs for Indigenous children and families that engage fathers (Dozois, Wells, Exner-Cortens, & Esina, 2016; McCalman et al., 2017; Morgan et al., 2017). There is emerging evidence that programs focusing on fatherhood need to acknowledge the situation of Indigenous men and their families and incorporate a respect for Indigenous culture to support men’s capacity to embrace their roles as fathers and promote the well-being of their children (Rossiter et al., 2017).
The purpose of this study was to inform the development a DIG program specifically for Indigenous fathers who want to quit smoking cigarettes and chewing tobacco. The project began with a commitment to design a program with the involvement of Indigenous people. The research objectives were to (a) consult Indigenous DIG facilitators, Elders, and key informants to gather advice to guide the development of a DIG Indigenous program, (b) develop program prototypes and design features for the DIG Indigenous program and pretest these in consultation groups with Indigenous fathers, Elders, and grandfathers, and (c) develop recommendations for development of the DIG Indigenous program based on findings. The research was based on an understanding of the diversity among Indigenous peoples of Canada and focused in particular on First Nations and Métis fathers residing in British Columbia, Canada.
Methods
A qualitative participatory design, informed by an epistemology of constructivism, was used to enable potential knowledge users to inform the design of the DIG program. This approach recognizes the value of engaging those whose lives are the focus of the research and that there are multiple, socially constructed understandings of reality that are influenced by social, cultural, and historical contexts. The research protocol was approved by the UBC Behavioural Research Ethics Board (#H16-01974). The project involved two phases.
Phase 1: Preliminary Consultations for Program Development and Implementation
First, a group consultation session was held with two DIG Indigenous male facilitators (who offered the DIG program to fathers in their communities in a previous pilot study; 39 and 40 years old), a 69-year-old Elder (who participated in the DIG program as a guest speaker), and a 40-year-old Indigenous DIG program participant to provide direction and advice to guide the development of an Indigenous DIG program. Following informed written consent, participants were invited to share experiences and provide feedback on preliminary findings from the DIG participants and offer suggestions for additional cultural adaptations to the program. Participants received an honorarium ($75 CDN) and travel expenses. The consultation session was digitally recorded and transcribed verbatim.
Individual consultations were also held via telephone or in person with 16 other key informants who were supporters of Indigenous fathers and family health to seek their advice for supporting Indigenous men’s SC and health promotion. Key informants were identified by the research team and recruited via e-mail invitations. The key informants included an Elder, an Aboriginal cultural safety educator, Indigenous and non-Indigenous health professionals who provided health services to Indigenous people (n = 6), experts in Indigenous sports and recreation (n = 2), individuals with experience in leading men’s groups in Indigenous communities (n = 3), and Indigenous community leaders (n = 3). Using a semistructured interview guide, key informants were asked for their advice about what resources and support should be included in an SC program tailored for Indigenous fathers as well as advice related to how Indigenous men’s roles as fathers could be supported through the program. Finally, their suggestions for physical activity that would be of interest to Indigenous men were also invited. An inductive content analysis of these data was completed by reviewing narratives, identifying data related to important topics, and coding these data by topic. Drawing on the expertise within the research team, data related to each topic were reviewed to compare comments, summarize key findings, and develop recommendations for the design of the DIG Indigenous program, including its content, resources, and “look and feel.”
Phase 2: Protocol Development and Evaluation
This phase involved creating program prototypes to illustrate DIG program adaptations for Indigenous fathers and to seek men’s feedback. The following prototypes were developed: (a) infographics related to traditional tobacco and the use of SC aids, (b) two interactive activities to engage men in discussions about the process of quitting, (c) a question/answer activity to engage men in talking about being dads and changing expectations, (d) options for physical activities that could be adapted based on program location, men’s preferences, and available resources, and (e) ways for DIG participants to stay in contact with each other and facilitators between sessions. These resources and accompanying interactive activities were shared with men in two consultation group sessions, emulating their use in a typical DIG session. As resources and interactive activities were shared, open-ended questions were used to invite men’s feedback. In addition, men were invited to evaluate the inclusion of Indigenous content and the effectiveness of the prototype activities in building a sense of camaraderie and peer support. Finally, men’s suggestions for further program development were invited. A convenience sample of participants was recruited using posters, brief presentations to individuals attending organizations offering services to Indigenous families, and word of mouth. Eligibility criteria were that men were currently using tobacco (smoking or chewing) or were ex-users, were fathers or primary caregivers for children in their lives, and self-identified as Indigenous. The sample included nine Indigenous fathers (First Nations or Métis), of whom five were also grandfathers. The average age of fathers was 43.75 years (SD ± 12.91) and the mean age of grandfathers was 55.4 years (SD ± 9.35). On average, men had four (SD ± 1.71) children ranging from newborn to adults. Grandfathers had on average 3.8 grandchildren (SD ± 1.92). Five men were currently smoking, and four were ex-users. All provided written informed consent. The sessions were facilitated by three members of the research team using an iterative semistructured discussion guide that included the prototype interactive activities. Based on responses from the first consultation session, questions and activities were further refined for use in the second consultation group to verify and extend emerging findings. Dinner was provided and an honorarium ($40 CDN) was given to each participant. Audio recordings and field notes were reviewed to identify and highlight main topics and responses to each of the program prototypes. Responses to each program prototype were compiled and reviewed by the research team to analyze men’s responses and suggestions for improvement. These data were considered alongside the advice received from stakeholders in Phase 1 by the research team. Through a process of reflection and discussion of these data, the team developed recommendations for inclusion and, where necessary, revision of the prototypes presented in the consultation group sessions, along with recommendations for tailoring the overall program design specifically for Indigenous fathers.
Results
Phase 1: Preliminary Consultations for Program Development and Implementation
The consultation group discussions and key informant interviews generated a range of suggestions related to program content and activities to guide the development of the DIG Indigenous program. In relation to program content, there was general agreement that it was important to design a program that was both culturally relevant and easily adapted to meet the needs of Indigenous men in diverse communities. Suggestions for Indigenizing a program targeting men included incorporating an Indigenous “look and feel” (e.g., using the medicine wheel), honoring ceremonial traditions (e.g., drumming/singing or ceremonies such as smudging), respecting the use of traditional tobacco, incorporating Indigenous role models (e.g., using local leaders, Indigenous male athletes, and important historical figures), and recognizing the importance of family and the collective culture that characterizes Indigenous communities. Also discussed was the value of incorporating a holistic approach to represent the intersection of multiple domains (mental, emotional, spiritual, and physical) of health and well-being (Panter-Brick et al., 2014) as well as traditional activities to advance men’s cultural knowledge. There was a lack of consensus on how much cultural knowledge to include. Pointing to the influence of colonialism and residential schools on tobacco use and Indigenous communities in general (Wardman & McKennitt, 2017), participants highlighted the general lack of knowledge of traditional activities, ceremonies, and practices and stressed the necessity for fathers to obtain this knowledge in order to model and teach these customs to their children. Other participants strongly believed that Indigenizing the program too much would deter some fathers from participating.
The need to balance the use of traditional talking circles and storytelling within a structured program like DIG, while creating an informal, casual atmosphere, was brought forward by participants. It was suggested that men participating in a DIG program be invited to establish guidelines for group discussions in order to honor storytelling, while being mindful of the timeline for program activities. Based on experience, one key informant suggested the use of a word or an object to signal when it was time to move on. It was also recommended that extra sessions be added to the beginning and end of the program to provide important opportunities for traditional celebrations and practices.
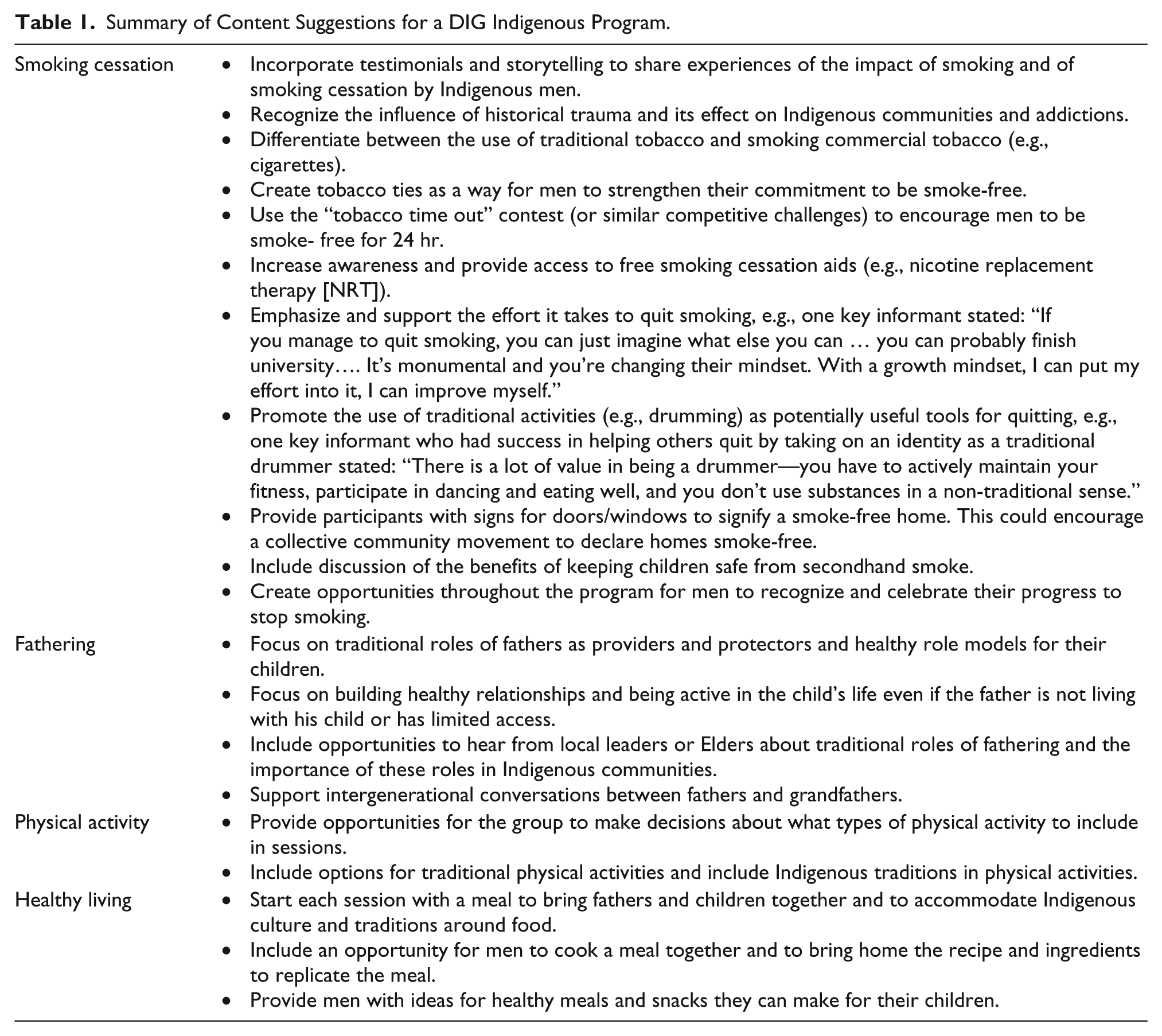
In launching the DIG Indigenous program, it was suggested that partnering with “trusted” local community groups/individuals would be important as well as enabling men’s participation with the provision of food, childcare, and, in some cases, transportation. Although some people suggested that incentives that fit with the goals of the program be considered to encourage participation (e.g., draws for fruit/vegetable basket that could be shared with family), others thought that serving food during the program would be an effective motivator for attendance. There were also suggestions about specific program content for a DIG Indigenous program. A summary of these suggestions is provided in Table 1.
Summary of Content Suggestions for a DIG Indigenous Program.
Phase 2: Prototype Evaluation
The men in the consultation groups responded positively to prototype activities and resources that incorporated Indigenous content. For example, during the opening activity that focused on introductions and a discussion about their given names and the names of their children, some men told stories about their Indigenous names, while others acknowledged that they were just given “White man” names. This led to much joking, bantering, and camaraderie among men who had previously not known each other. Another example of building comfort levels with Indigenous knowledge came about during a discussion around traditional tobacco use, motivated by a draft infographic on this topic. At both consultation sessions, the men suggested that it was important to provide information about traditional tobacco for Indigenous groups, where this was a common practice, and helped frame messages about its use, suggesting statements such as “Traditional tobacco is used in ceremony, given as a form respect, used in exchange for a gift—mostly knowledge” and “Traditional tobacco is used to heal the mind, body, and spirit.” The men were satisfied that within any given group of Indigenous men, the amount of information presented would lead to appropriate discussions about traditional tobacco knowledge and practice. The men’s responses also highlighted the importance of using culturally relevant images in the program that were likely to resonate with Indigenous men. For example, one image shared with participants unexpectedly triggered experiences associated with historical trauma. A participant stated, “The only people who wear shirts like that are ones in Indian [residential] school.”
In terms of supporting SC efforts, the men emphasized the importance of positive message framing. Fathers suggested shifting language from “quit smoking” to “stop smoking,” reasoning that a slip might lead to feelings of failure. One man explained: I never quit, I just stopped, I hate quitters … because quitting, when you say quit that is a long, long, long time that’s forever you know, like you’re convincing yourself that you’re gonna do this forever, so if you start [smoking] you’re going to automatically think you’re a failure.
The consultation sessions also provided an opportunity to introduce men to the idea of “practicing stopping smoking” based on the rationale that practice is required to become skillful in many pursuits (e.g., sports, hunting, drumming). The men were enthusiastic about this approach to cessation and identified ways to practice that would work for them. The most popular suggestions were related to practicing self-motivation tactics (e.g., practice breathing slowly and telling yourself reasons you want to quit smoking) and diversion activities. The men also suggested that ready access to cessation aids such as nicotine replacement therapy be provided within the program, along with information from a health professional about the benefits and side effects of the use of these aids. Men firmly believed that this provision of honest information would help to rebuild trust with health professionals. As one participant explained: “It shows that they really care about us.”
In relation to fathering, the participants offered positive feedback on a prototype activity that encouraged them to reflect on and share their aspirations as fathers and grandfathers as well as societal expectations of modern Indigenous men. In response to questions about what types of physical activity should be incorporated into the program, previous findings were verified. The men’s suggestions extended beyond traditional activities (e.g., drumming, lacrosse) to include outdoor activities (e.g., hiking, biking, nature walks), individual sports (e.g., weightlifting, workout stations, swimming, running or walking on a track), team sports (e.g., soccer, baseball, basketball, badminton), organized games (e.g., dodgeball, tag, kick the can), and community service (e.g., yard work, garbage pickup, raking leaves).
Finally, the men were asked to provide feedback on ways facilitators and other participants could keep in touch between weekly DIG sessions. Preferred methods of contact were via a social media support group (Facebook or twitter), text messaging, telephone, or meeting in person midweek. E-mail was the least popular channel to keep in contact.
Discussion
This study is the first to explore and describe Indigenous fathers’ perspectives and preferences for men-centered and culturally sensitive programming to support men’s SC. The findings add to the field of gender studies, especially related to Indigenous men’s health, which is still very much underdeveloped. There is a general lack of community programs that are tailored specifically for Indigenous men or Indigenous fathers. At a community level, most parenting and child welfare practices remain mother-centric (Panter-Brick et al., 2014), despite recognition of the separate and different needs of fathers (Pfitzner, Humphreys, & Hegarty, 2017), and in particular the potential benefits of supporting positive parenting among Indigenous fathers (Dozois et al., 2016). Nevertheless, there is growing interest in developing and evaluating tailored programs to support Indigenous fathers’ involvement with their children (Ball & Moselle, 2015; Dozois et al., 2016; Fletcher et al., 2017; Hammond, 2010; Moselle & Ball, 2013; Northern Health, 2015; Reilly & Rees, 2018; Rossiter et al., 2017; Stuart, May, & Hammond, 2015). Indigenous men experience unique challenges related to the interactional impacts of masculinities, colonization, and other social hierarchies (racialization, income, education, sexual orientation, etc.) on gender roles (including fathering) as well as their health and social outcomes (Anderson & Innes, 2015). This research provides a useful model for developing evidence-based, gender-responsive programs for Indigenous men based on their preferences and perspectives that acknowledge historical factors and contemporary changes influencing men’s gendered roles and cultural connections. For example, while Indigenous men have experienced trauma and marginalization, culturally sensitive group programs hold promise for aiding healing and building resilience. Affirming and norming the strength for men to connect with one another to garner mutual benefit and to aid their communities more broadly holds much appeal for Indigenous men. DIG has always been a strength-based program in that it focuses on the strengths men bring and their potential to improve their lives and those around them. In the specific context of Indigenous men, palpable in experiences during the consultation groups were the additional benefits of camaraderie and humor, in forging positive change among the men and group more broadly.
It is important to consider the DIG Indigenous program within the context of health inequities, given the findings drawn from the current study. That Indigenous men have high and rising rates of smoking can be reasonably argued, at least in part, as a by-product of unregulated supply and in some cases discounted or subsidized tobacco being made available to this vulnerable group. Coupled with trauma related to colonization, low socioeconomic status, and ongoing discrimination, it is entirely reasonable to expect additional culturally sensitive SC programs as key to reducing the harms of smoking in these vulnerable communities. With these multiple issues in mind, it is imperative that the DIG Indigenous program is informed and offered by trusted, reliable persons, and “wise practices” gained through experiences and traditional teaching (Wardman & McKennitt, 2017). In terms of authenticity and potential for sustainability and scale, the involvement of Indigenous communities in championing change around SC through DIG holds much promise as a lynchpin for the feasibility of the program. Together these findings indicate how health inequities can be attended to, in part, with internal resources, innovation, and trusted partner collaboration.
The findings of both phases of this study need to be considered in relation to study limitations. Despite including a wide range of stakeholder perspectives in Phase 1, their direct experiences with SC and Indigenous communities varied. Further, it is important to recognize that Indigenous men are diverse in terms of their culture, their experiences as fathers, and their use of commercial and traditional tobacco. Although study participants acknowledged this diversity and represented different Indigenous groups, their perspectives are not espoused as representative of all Indigenous men or family structures. Nevertheless, Indigenous team members aided the research team in being mindful of diversities among Indigenous peoples, particularly during data analysis and interpretation. This exploratory study provided much-needed information concerning intervention development for a vulnerable, understudied population; however, it did not evaluate smoking behavior changes. Further research to test the effectiveness of this novel program with Indigenous fathers is warranted.
Despite these limitations, important insights were gained to guide the development of gender-sensitive SC programs for Indigenous men and add to the approaches described by others (Wardman & McKennitt, 2017). Given the success of the interactive activities with men in the original DIG program, various core activities were designed and adapted for the Indigenous program. These activities proved successful in keeping participants active, interested, and engaged. For example, the men were receptive to the idea that stopping smoking takes practice, after participating in a game of hacky sack (juggling a bean ball with their feet). This activity also proved to be a successful way for men to bond with each other through friendly competition and humor. Respectful brainstorming activities provided an opportunity for men to share experiences and proved a positive way to foster peer support.
The positive response of Indigenous men to these prototype activities provided important insights into ways to effectively engage Indigenous fathers in a targeted SC program. Based on the findings of this study, several recommendations can be made to guide the development of a men-friendly and culturally safe DIG program to support SC among Indigenous fathers.
The look and feel of the program along with its images and activities need to be culturally sensitive and appropriate to resonate with the target group.
Offering the program in a group format mirrors Indigenous community cohesion in that it reemphasizes the importance of relationships for emotional, spiritual, physical, and mental health.
Addressing traditional tobacco and its ceremonial use is meaningful for Indigenous men regardless of their individual knowledge on the topic.
Support for SC should include framing cessation as “stopping smoking” and activities to support practice in stopping; narratives from fathers immersed in the process of stopping smoking as well as narratives from fathers who have succeeded in stopping; and the use of traditional activities (e.g., tobacco ties) to support commitment to stop smoking.
Engaging respected Elders and community leaders in some of the program activities respects their knowledge and experience and acknowledges their importance as positive community roles models for fathers.
Providing opportunities for men to discuss historical influences and the changing roles and expectations for modern Indigenous fathers supports men in defining the type of fathers they aspire to be.
Including options for physical activity allows for programs to be guided by men’s preferences and available resources in Indigenous communities.
These recommendations reflect many of the promising practices for fatherhood programs suggested by Bronte-Tinkew and colleagues (2012). For example, the findings indicated that a DIG Indigenous program would be enhanced with trained male facilitators who are experienced in working with community groups, the use of engaging and interactive teaching materials and methods, and a focus on three core integrated topics (SC, fathering, physical activity). In addition, a DIG Indigenous program could offer a promising way to mobilize men’s interest in cessation as fathers (and grandfathers), whether absent or present in their children’s lives; recognize the distinct contributions, experiences, and assets that fathers bring to the lives of children, families, and communities; and address the systematic marginalization of fathers that has been evident in many community-based programs (Panter-Brick et al., 2014). Furthermore, there is the potential through the program to encourage younger men to be mentors and advisors themselves for future DIG groups in their community. Key questions related to implementation need to be explored within communities to determine how best to address barriers to fathers’ and grandfathers’ engagement in this program as well as how to enable community-wide changes to support cultural shifts to involved fathering and reductions in tobacco use.
While much of the gender work in men’s health has focused on Western White middle-class masculinities, in the current study, much-needed insights were offered to what might constitute Indigenous men’s health-related masculine values. Men’s alignments to collectivist cultures were included, whereby the “group” emphasis of DIG offered a familiar way for men to connect with one another. The camaraderie and meaningful connections that can be generated through a group program like DIG are foundational to supporting family networks and community cohesion in Indigenous communities and commensurate with Indigenous views on well-being in that health and wellness radiate from the individual to family to the broader community. This suggested a good “fit” with the group delivery mode of the DIG program. That the Indigenous men’s level of involvement with their children was diverse but generally less prescriptive than current contemporary “involved fathering” discourse was also a key consideration in terms of the program context and content. Strategies were afforded by these insights for meeting the men where they are in terms of their fathering—as well as their smoking and physical activity.
Conclusion
The findings of this study have been used to inform the development of the DIG Indigenous program, resources, and a program website (www.dadsingearindigenous.ca). Although the DIG Indigenous program is the first group program to support Indigenous fathers in their efforts to quit smoking cigarettes and chewing tobacco, an investment of resources to implement and evaluate this culturally tailored and gender-sensitive cessation program is needed to demonstrate its effectiveness. The DIG Indigenous program provides a novel approach to advancing men’s health and well-being and provides an evidence-based prototype for other community-based programs for Indigenous men in Canada. The findings may also be relevant for supporting SC among Indigenous men in other countries who have experienced a similar history of colonization and tobacco use.
Footnotes
Acknowledgements
We gratefully acknowledge the insight and expertise of Kym Howay and Jeff Conners during our consultations with Indigenous men.
Version Date: June 21, 2018
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported with a grant from Interior Health, British Columbia, Canada [Grant #: IHRGC_2016-04].