
Abstract
Preconception health behaviors significantly influence pregnancy outcomes, yet patterns of these behaviors and their determinants have received limited attention, particularly among men. Understanding behavioral profiles is essential for developing targeted interventions to improve paternal reproductive health. We conducted a cross-sectional study examining over 20 guideline-recommended preconception health behaviors among 952 Chinese men. Latent profile analysis was utilized to identify different behavioral profiles. Multinomial logistic regressions assessed associations of profile membership with sociodemographic and medical history characteristics. Four distinct preconception health behavioral profiles were identified: a “Moderate” profile (44.0%) with scores near or slightly above the overall mean on most behaviors; a “Vulnerable” profile (4.5%) showing markedly negative scores across multiple behaviors; and two intermediate profiles “Unmotivated” (33.2%) and “At-Risk” (18.3%) with scores closer to average on some behaviors but notably lower on others (e.g., planning, avoidance of environmental hazards and domestic violence, treating existing diseases). Several behaviors received low scores across all profiles, including preconception check-ups, genetic screening, receiving professional preconception education, physical activity, and immunization. Lower education and unplanned pregnancy were consistently associated with at-risk behavioral profiles. Interventions must combine universal campaigns to elevate systematically neglected behaviors with targeted strategies addressing profile-specific needs. Pregnancy planning emerges as a keystone intervention opportunity. National programs require rebranding to emphasize paternal participation, while all strategies must address underlying social determinants rather than focusing solely on individual behavior change.
Keywords
Introduction
Preconception health comprises the health status of individuals during the period preceding pregnancy (typically 3–6 months), with established associations with fertility, pregnancy outcomes and offspring health (Stephenson et al., 2018). While this field has primarily centered on maternal well-being, a growing body of evidence highlights the critical and often overlooked role of paternal factors (Kotelchuck & Lu, 2017). Men’s preconception health, particularly modifiable behaviors (e.g., substance use, lifestyle choices, and chronic condition management), directly influences fertility and can shape offspring health through mechanisms like epigenetic programming (Day et al., 2016; Stephenson et al., 2018). Evidence indicates that effective preconception care such as nutritional interventions may prevent birth defects and pregnancy-related complications (Dean et al., 2014), making the health behaviors of prospective fathers a key target for health promotion.
Major international health organizations including the World Health Organization (WHO), Centers for Disease Control and Prevention (CDC), and the American College of Obstetricians and Gynecologists have established comprehensive preconception health guidelines (“ACOG Committee Opinion No. 762,” 2019; Johnson et al., 2006; WHO, 2013). These recommendations provide a multifaceted framework for optimizing preconception health, emphasizing nutritional supplementation, substance avoidance, weight management, chronic condition screening, environmental hazard mitigation, medication review, psychological well-being, genetic screening, and other key health domains for both prospective parents (“ACOG Committee Opinion No. 762,” 2019; Johnson et al., 2006; WHO, 2013). However, despite this established consensus, implementation barriers persist (Kandel et al., 2021; Poels et al., 2016). This challenge is particularly significant for men, who represent an underexamined dimension in preconception research and are frequently marginalized in clinical practice (Abed Alah, 2024). Such neglect constrains insight into man-specific behaviors and their determinants, thereby impeding the development of effective, sex-informed interventions.
Current evidence on behavioral predictors has primarily focused on whole-population analyses (Kandel et al., 2021; Toivonen et al., 2018), overlooking the heterogeneity of behavioral patterns and their varying determinants across different subgroups. Research shows behavior adherence varies across different sociodemographic groups (Dott et al., 2010; Toivonen et al., 2017), highlighting the importance of identifying distinct subgroups and providing behavior recommendations tailored to population specific characteristics (Mason et al., 2014). Person-centered approaches offer practical solutions for capturing these diverse behavioral patterns. Unlike traditional methods that examine average patterns across entire populations, latent profile analysis (LPA) identifies distinct subgroups with similar behavioral characteristics (Collins & Lanza, 2009). This methodology enables the detection of subgroup differences that might be overlooked when behaviors are analyzed at the population level.
Given the significant gap in understanding men’s preconception health behaviors, this study aims to apply a person-centered approach to this understudied population. The objective is to identify distinct preconception health behavior profiles and to examine sociodemographic and medical history predictors specifically among reproductive-aged Chinese men. The results are intended to inform the development of targeted preconception health interventions tailored to the specific risk profiles of men, thereby enhancing the implementation of evidence-based practices and ultimately improving paternal contributions to fertility and offspring health.
Method
Study Design and Setting
This study used a cross-sectional design, analyzing survey data collected from July through September 2023 in Zhejiang Province, eastern China. Zhejiang is an ideal location for this study due to its coastal status and diverse population of local residents and migrant workers, which provides insight into varying preconception health behaviors among reproductive-aged men.
Participants and Sampling
This study focused on reproductive-aged men who, together with their partners, had intentions to conceive. The recruitment strategy was designed to capture a sample of men across a spectrum of recent reproductive experiences, defined by the couple’s conception outcome. These outcomes included successful pregnancies (both planned and unplanned) and unsuccessful outcomes (infertility and miscarriage cases).
Multistage stratified sampling was employed. First, Hangzhou and Quzhou cities were purposively selected, representing urban-developed and rural-developing areas of Zhejiang Province. Next, two districts/counties were randomly selected from each city. Within each selected district/county, community health centers and maternal-child hospitals served as recruitment sites. Recruitment used a couple-centered approach and convenience sampling, where women attendees at community health centers and maternal-child hospitals were screened for eligibility; upon consent, they were invited to refer their men partners for participation.
Because population-level, man-specific estimates for conception outcomes and infertility are limited, we based our sampling ratios on well-documented rates among Chinese women, since men’s exposure to these outcome categories is coupled with their partners’ clinical status. This included reported infertility rates of approximately 15% among Chinese couples with regular unprotected intercourse (Z. Zhou et al., 2018) and pregnancy loss rates of about 10% (Peters et al., 2020). To ensure representativity and reduce bias, the sampling plan specified that participants experiencing partner infertility and pregnancy loss should comprise 5% to 15% and 5% to 10% of the total sample, respectively.
Data Collection
The questionnaire was developed based on current Chinese and international preconception health and care guidelines (“ACOG Committee Opinion No. 762,” 2019; Hyperthermie—Gezond zwanger worden, n.d.; Qi & Yang, 2018; WHO, 2013). The questionnaire was pilot-tested with 122 men to identify potential problems and improve their effectiveness.
Surveys were distributed using Wenjuanxing, a leading Chinese online survey platform. Participants were recruited in person at prenatal, gynecology, and reproductive health departments in local health care facilities and completed the questionnaires on their mobile phones. Each questionnaire started with an informed consent form explaining data confidentiality, voluntary participation, and right to withdraw.
Study Variables
Preconception health behaviors were the primary outcome variables. Respondents were asked to recall their behaviors during the 3 months before partner’s pregnancy (for those with successful pregnancies or miscarriages) or report their current behaviors (for those with infertility).
Preconception health behaviors assessed included planned pregnancy, avoidance of advanced maternal age pregnancy, optimal maternal and paternal health status, standard preconception check-up, preconception genetic screening, receiving professional preconception health education, balanced nutritional intake, maintenance of mental health, smoking cessation, alcohol cessation, appropriate physical activity, maintenance of appropriate body weight, maintaining balanced work–life patterns, avoidance of noise exposure, avoidance of domestic violence, avoidance of toxic and harmful substances, avoidance of medication without medical consultation, avoidance of secondhand smoke exposure, avoidance of hyperthermia exposure, immunization, treatment of pre-existing conditions, and infectious disease prevention.
All behaviors were scored on a scale from 0 to 100, with higher scores indicating better adherence to recommended practices. Some behaviors were evaluated through single questions (e.g., prevention of domestic violence, avoidance of toxic substances), whereas others were assessed with multiple questions capturing dimensions such as frequency, volume, and duration (e.g., detailed assessment of alcohol consumption patterns, smoking habits, and physical activity levels).
Sociodemographic characteristics included age, education level, monthly household income, ethnicity, migrant status, and residential area. Medical history variables included self-rated health status, history of miscarriage, history of induced abortion, and self-reported pregnancy planning. Notably, self-reported pregnancy planning should not be confused with the behavioral indicator “planned pregnancy.” In the Chinese context, pregnancy planning (“Beiyun”) emphasizes whether individuals have actively prepared for pregnancy, reflecting a broader concept that includes personal readiness and intentional actions. In contrast, the “planned pregnancy” indicator simply assesses whether the pregnancy was intended, focusing on the individual’s behavioral intention.
Statistical Analysis
Descriptive statistics were employed to describe sociodemographic characteristics and preconception health behaviors. Correlation analyses were completed and visualized in R Studio for preconception health behaviors. LPA was conducted using R Studio’s mclust package to identify distinct preconception health behavior patterns, with subgroups comprising less than 5% of the total sample potentially indicating model instability (Nylund et al., 2007). To standardize variables, Z-scores were calculated for each preconception health behavior by subtracting the mean from each value and dividing by the standard deviation. Models with 1 to 7 profiles were compared using Bayesian information criterion (BIC) to determine optimal profile solutions. A higher BIC mclust value indicates a better model fit. Behavior patterns were visualized using ggplot2. Chi-square tests were used as an initial screen for associations among categorical variables. Every predictor that proved significant, except the methodological factor “sampling location,” was subsequently entered into multinomial logistic regressions in Stata 18.0 to evaluate the relationship between profile membership and sociodemographic or medical history variables, with the healthiest profile set as the reference category. Statistical significance was set at p < .05.
Results
Descriptive Statistics
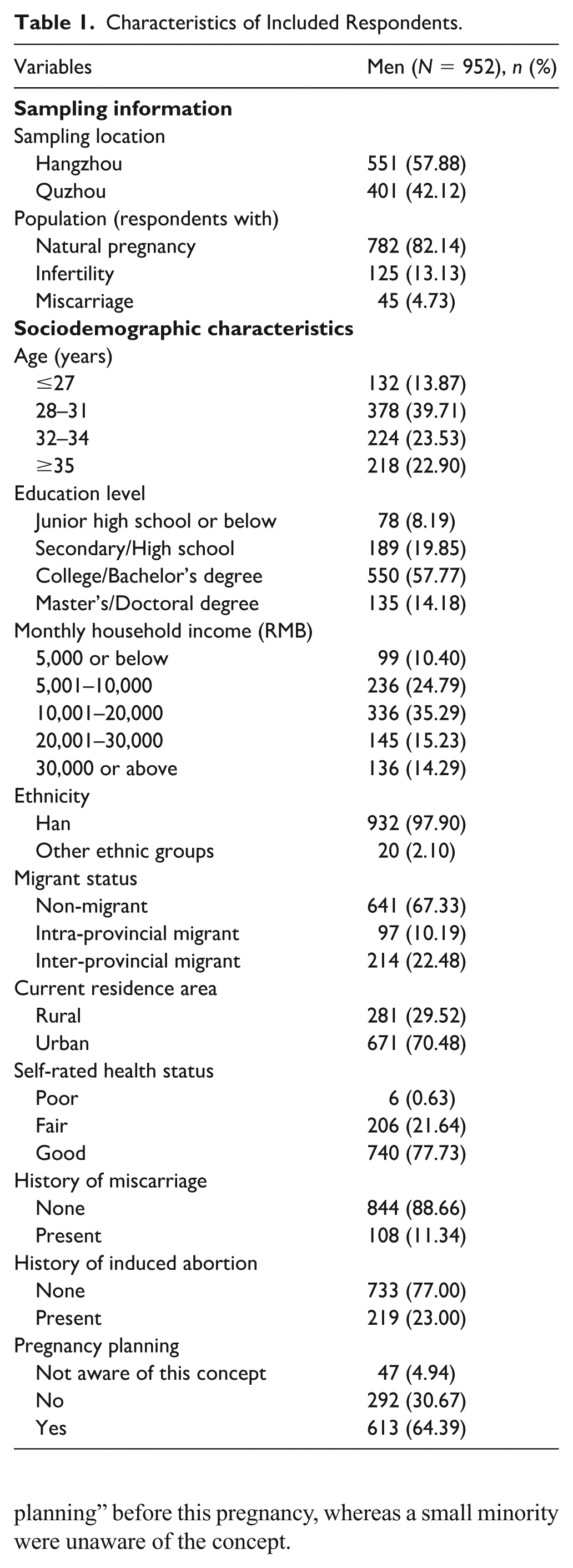
A total of 1,026 questionnaires were collected, with 952 men providing valid responses. Participants were recruited from Hangzhou (57.9%) and Quzhou (42.1%), with the ratio of natural pregnancy cases to infertility cases to miscarriage cases being approximately 82:13:5 (Table 1). Men were predominantly aged 28 to 31, with over half holding college degrees. The sample was primarily of Han ethnicity (97.9%), non-migrant (67.3%), and urban-dwelling (70.5%). Most participants reported good health, though reproductive history revealed prior miscarriages (11.3%) and induced abortions (23.0%). Approximately 64% of men reported that they conducted “pregnancy planning” before this pregnancy, whereas a small minority were unaware of the concept.
Characteristics of Included Respondents.
The descriptive statistics and correlations of the behavior variables are presented in Supplemental Table S1 and Figure 1, respectively. Adherence was generally high (>90) for most preconception health behaviors (e.g., avoiding toxic substances and medication without consultation, treatment of pre-existing conditions), whereas respondents showed the lowest mean scores for standard preconception check-ups, genetic screening, receiving education, physical activity and immunization. Pair‑wise correlations among behaviors were mostly weak to moderate (r < .50), with the strongest positive clusters linking related lifestyle actions, such as “no smoking” with “no drinking” and “work–life balance” with “mental well-being.” In addition, a smaller cluster connected preventive care behaviors, including preconception check-ups, genetic screening, and receiving education.

Correlation Matrices of Preconception Health Behavior Variables (N = 952).
Latent Profile Analysis
Competing models with one to seven profiles were estimated under both EEV (ellipsoidal, equal volume, and shape) and EII (spherical, equal volume) covariance structures. EEV was chosen for yielding the highest BIC mclust in preliminary mclust runs, whereas EII provided the next best, more economical fit. As shown in Table 2, BIC improved up to the four‑profile solution before declining, indicating that four profiles optimally balanced fit and simplicity. Three classes exceeded this 5% threshold (Nylund et al., 2007), whereas the smallest class (4.5%) was retained for its distinct behavioral pattern.
Bayesian Information Criterion (BIC) Values Across Latent Profile Models.

Note. EEV = ellipsoidal, equal volume and shape; EII = spherical, equal volume. Higher BIC values correspond to a better fit. The maximum BIC value occurs for the four-cluster model, which is in bold in the table.
Four distinct latent profiles emerged (Figure 2):
1. Moderate (Cluster 1; n = 419, 44.0%) clustered around the mean on nearly all behaviors, with small positive deviations for pregnancy planning (0.55), avoidance of advanced maternal age pregnancy (0.44), and infectious disease prevention (0.44).
2. Unmotivated (Cluster 2; n=316, 33.2%) recorded the lowest scores on pregnancy planning (−0.57), avoidance of advanced maternal age pregnancy (−0.58), and infectious disease prevention (-0.51). However, they demonstrated better preconception maternal/paternal health status (~0.39) and more successful work–life balance (0.11), suggesting reasonable lifestyle management despite limited attention to specific preconception health practices.
3. At‑Risk (Cluster 3; n = 174, 18.3%) displayed marked deficits in preconception maternal and paternal health status (−1.55 and −1.47, respectively) along with below‑average scores on mental health well-being (−0.47) and maintaining work–life balanced patterns (−0.31). Their main challenges lie in their general health status and life patterns.
4. Vulnerable (Cluster 4; n = 43, 4.5%) showed the lowest engagement overall, with steep negatives for treatment of pre-existing conditions (−3.47), toxin/noise/violence avoidance (−1.85 to −2.05), and maintaining work–life balanced patterns (−0.50). Scores for most other items were also below average.

Z-Score Profiles of Four Distinct Preconception Health Behavior Clusters (N = 952).
Predictors of Profile Membership
Supplemental Tables S2 display sociodemographic and medical history characteristics across behavior profiles. Significant associations included sampling location, population group, age, education, self-rated health, abortion history, and pregnancy planning. Multinomial regressions (Table 3) revealed that participants with miscarriage (vs. natural pregnancy) had significantly higher RRRs for At-Risk (RRR = 7.559, 95% CI = [2.817, 20.286]) and Vulnerable (RRR = 7.643, 95% CI = [2.095, 27.882]) profiles. Men older than 34 (versus ≤27) showed significantly higher RRRs for Unmotivated (RRR = 4.215, 95% CI = [2.341, 7.589]) and At-Risk (RRR = 2.202, 95% CI = [1.013, 4.789]) profiles. Education beyond junior high was a protective factor for Unmotivated (Secondary/High school: RRR = 0.190, 95% CI = [0.075, 0.479]; College/Bachelor’s degree: RRR = 0.141, 95% CI = [0.059, 0.336]; Master’s/Doctoral degree: RRR = 0.138, 95% CI = [0.053, 0.362]) and Vulnerable (Secondary/High school: RRR = 0.141, 95% CI = [0.039, 0.508]; College/Bachelor’s degree: RRR = 0.086, 95% CI = [0.026, 0.282]; Master’s/Doctoral degree: RRR = 0.092, 95% CI = [0.020, 0.421]) profiles, while education beyond secondary/high school was a protective factor for the At-Risk profile (College/Bachelor’s degree: RRR = 0.164, 95% CI = [0.058, 0.459]; Master’s/Doctoral degree: RRR = 0.321, 95% CI = [0.104, 0.991]). Fair health status (versus good) significantly increased RRRs for At-Risk (RRR = 14.002, 95% CI = [8.747, 22.412]) and Vulnerable (RRR = 6.846, 95% CI = [3.285, 14.268]) profiles. History of induced abortion was a risk factor for the At-Risk profile (RRR = 1.670, 95% CI = [1.014, 2.751]). Lack of pregnancy planning (Unmotivated: RRR = 5.260, 95% CI = [3.605, 7.674]; At-Risk: RRR = 3.125, 95% CI = [1.931, 5.058]; Vulnerable: RRR = 3.291, 95% CI = [1.544, 7.011]) or awareness (Unmotivated: RRR = 7.760,95% CI = [2.731, 22.050]; At-Risk: RRR = 3.862,95% CI = [1.080, 13.816]; Vulnerable: RRR = 10.504,95% CI = [2.573, 42.873]) were risk factors for all non-Moderate profiles.
Multinomial Logistic Regression Results Predicting Cluster Profile Membership Among Respondents (N = 952).

p < .05. **p < .01. ***p < .001.
Discussion
Our study examined more than 20 preconception health behaviors among reproductive-aged Chinese men, revealing four distinct behavioral patterns. The largest group (44.0%) demonstrated a “Moderate” profile with behaviors clustering around population averages. The second-largest “Unmotivated” group (33.2%) maintained reasonable lifestyle management but showed poor engagement in pregnancy planning and infectious disease prevention. An “At-Risk” group (18.3%) displayed marked deficits in health status and work–life balance, whereas a “Vulnerable” minority (4.5%) showed the poorest performance across multiple domains, particularly in treating pre-existing conditions and avoiding environmental hazards. Across all profiles, older age (>34 years), lower education, poorer self-reported health, experiencing miscarriage in this pregnancy, and lack of pregnancy planning were associated with membership in the at-risk group(s).
Interpretation of Findings
The weak to moderate correlations between most preconception health behaviors suggest that men adopt these practices independently rather than as part of a cohesive health strategy. This finding implies a fragmented understanding of comprehensive preconception health, which may reflect a broader trend also observed in women (Zhao et al., 2023), suggesting a systemic gap in comprehensive preconception education. For men specifically, this fragmentation could be exacerbated by a general lack of proactive engagement with preventive health care and limited exposure to men-targeted reproductive health information (Abed Alah, 2024). Therefore, effective interventions must not only promote individual behaviors but also build a comprehensive conceptual framework, educating men on how these disparate actions collectively contribute to optimizing fertility and offspring health.
While the “Moderate” group was the largest (44.0%), representing men whose behaviors clustered around population averages, this should not be interpreted as optimal performance. Rather, it reflects a concerning reality where the population “average” for several critical behaviors is itself inadequate, including participation in standard preconception check-ups, genetic screening and education, physical activity, weight management, and immunization. This pattern reveals significant public health challenges despite national policies like the National Free Preconception Health Examination Project (NFPHEP) providing free services (Q. Zhou et al., 2016). Contributing factors include high rates of unplanned pregnancies in China (≈55%–60%) (Bearak et al., 2022), persistent awareness gaps (Abed Alah, 2024), and historically women-focused public health campaigns that create perceptions of man’s irrelevance to preconception care (Abed Alah, 2024). These findings highlight the critical need to rebrand national preconception programs as essential for both partners, with clear messaging on paternal participation benefits and interventions addressing broader lifestyle factors.
The large “Unmotivated” group, who managed general lifestyle but neglected specific planning, reveals a common and dangerous misconception: that being “healthy enough” in daily life automatically ensures optimal reproductive potential (Sharot, 2011; Weinstein, 1984). Interventions for this group must directly target this assumption by providing concrete evidence linking specific paternal behaviors (e.g., nutrition, stress) to reproductive outcomes (Day et al., 2016; Stephenson et al., 2018).
Conversely, the “At-Risk” profile, characterized by poor self-rated health and work–life imbalance, points to the powerful influence of psychosocial stress on men’s health. Chronic stress can disrupt the hypothalamic–pituitary–gonadal axis, impacting testosterone and spermatogenesis, creating a direct biological link between their life pressures and reduced fertility (Nargund, 2015; Odetayo et al., 2024). The “Vulnerable” group, with its deficits in managing pre-existing conditions and avoiding environmental hazards including domestic violence, likely faces a confluence of medical, social, and possibly occupational challenges. This underscores that high-risk men require comprehensive case management that integrates medical care with mental health support and social services.
Our analysis of sociodemographic predictors aligns with findings from other contexts, such as Anakwe et al.’s (2022) study of American men, reinforcing that these behavioral patterns are not merely individual choices but are shaped by structural and social determinants. The strong association between lower education and at-risk profiles is a classic indicator of health inequity. Furthermore, the link between a history of induced abortion and the At-Risk profile suggests that suboptimal contraceptive practices and poor preconception health behaviors may be part of a larger syndrome of risk-taking or limited health literacy. Since unplanned pregnancies were a powerful predictor for all non-Moderate profiles, this underscores pregnancy planning as a critical entry point for improving multiple health behaviors simultaneously. This suggests that promoting family planning awareness and services could serve as a “keystone” intervention, potentially triggering broader preconception health improvements across men.
These findings make it clear that simply encouraging individual men to “make better choices” is insufficient. Effective interventions must be multifaceted: they must provide targeted health promotion and comprehensive reproductive education (including contraception), while simultaneously addressing systemic barriers like limited access to man-friendly reproductive services and cultural norms that discourage men involvement. Only by tackling both individual behaviors and the systems that shape them can we meaningfully improve men’s preconception health.
Strengths and Limitations
This study has several strengths: it focused specifically on men as participants, addressing the significant research gap in paternal preconception health behaviors; it comprehensively analyzed more than 20 guideline-recommended preconception health behaviors; and it incorporated both infertility and miscarriage samples, offering a more comprehensive perspective on men’s reproductive health experiences. However, important limitations should be acknowledged: the cross-sectional design prevents establishing causal relationships between identified factors and preconception health profiles, requiring future longitudinal studies to confirm temporal associations; the single-province sampling limits generalizability to other regions of China or internationally, although our findings may still provide valuable insights for similar cultural contexts; and self-reported behaviors may be subject to recall and social desirability bias, potentially leading to overestimation of positive health behaviors despite our efforts to minimize measurement error through validated instruments.
Conclusion
We identified four preconception health behavioral profiles among Chinese men, highlighting that population averages for key behaviors remain inadequately low, particularly for preconception check-ups, physical activity, and weight management. Interventions must combine universal campaigns to elevate systematically neglected behaviors with targeted strategies addressing profile-specific needs. Pregnancy planning emerges as a keystone intervention opportunity for preconception health improvements. National programs should emphasize paternal participation, while all strategies must address underlying social determinants rather than focusing solely on individual behavior change.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883251400712 – Supplemental material for Preconception Health Behavioral Patterns and Predictors in Chinese Reproductive-Aged Men: A Latent Profile Analysis
Supplemental material, sj-docx-1-jmh-10.1177_15579883251400712 for Preconception Health Behavioral Patterns and Predictors in Chinese Reproductive-Aged Men: A Latent Profile Analysis by Ruyu Sun, Rui Fan, Hanqian Wang, Xin Xu and Lu Li in American Journal of Men's Health
Footnotes
Acknowledgements
The authors gratefully acknowledge the participants who completed the survey and generously shared their experiences and insights on preconception health behaviors.
Ethical Approval
The study protocol was reviewed and approved by two Institutional Review Boards: School of Public Health (ZGL202303-6) and the Women’s Hospital, School of Medicine (IRB-20230245-R) at Zhejiang University.
Informed Consent
Participation was voluntary and participants could withdraw at any time without penalty.
Consent to Participate
Electronic informed consent to participate in this study was obtained from all participants.
Consent for Publication
Not applicable, as no individual person’s data in a form that could identify any individual participant is included in this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be made available upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.