
Abstract
Men’s pregnancy intention is associated with a host of positive outcomes for families, yet this topic remains understudied. Because unintended pregnancies are more likely to occur at suboptimal parental health, this study aimed to examine the extent to which men improve their preconception health in the context of future fertility planning. This study used pooled data from the 2011–2019 National Survey of Family Growth for a final sample size of 10,223. Latent class analysis (LCA) was used to identify distinct classes of men’s preconception health. Eight preconception health risk factors were used to determine class membership. A classify-analyze approach was used to create the preconception health phenotype (PhP) exposure variable. The outcome of interest was men’s fertility intentions. Multinomial regression models were used to examine the association between the exposure and the outcome. Three unique PhPs were identified (lowest risk, substance users, and sexual risk-takers) from the LCA model. Men in the substance users’ group (22.9%) were characterized by high-risk alcohol use and drug use, while sexual risk-takers (8.1%) were characterized by having multiple sexual partners. Belonging in the phenotypes of substance users or sexual risk-takers was associated with increased odds for definite no fertility intention than definite yes intentions (adjusted odds ratio [aOR]: 1.47, 95% confidence interval [CI]: [1.18, 1.84] and aOR: 1.51, 95% CI: [1.13, 2.01], respectively). Results provide new insights on how preconception health can be measured and fills a knowledge gap on its relationship to men’s future fertility planning. Findings can be applied to preconception care intervention frameworks, and guide family planning interventions and contraceptive counseling.
Keywords
Background
Men’s pregnancy intentions, that is, whether their partners’ pregnancy occurred when it was wanted (intended), too soon (unplanned/mistimed), or when it was not wanted (unwanted), are a strong determinant of father involvement before, during, and after pregnancy (Almeling & Waggoner, 2013; Bronte-Tinkew et al., 2007; Combs et al., 2021; Lindberg et al., 2017). From 2006 and 2010, about 40% of men in the United States between ages 15 and 49 years reported having an unintended pregnancy with their partner (Lindberg et al., 2017), a phenomenon that is seldom reported in the research literature. In a population-level cross-sectional study of the U.S. male population ages 15 to 44 years, Choiriyyah and colleagues (2015) reported that about 60% of these men needed preconception care through their exposure to risk factors including existing health conditions, behavioral risks, and substance use (Choiriyyah et al., 2015). Pregnancies that occur at suboptimal parental health are associated with numerous adverse outcomes for children and families, and these adverse outcomes are more likely to occur when pregnancies are unplanned or unwanted (Barker, 2007; Dott et al., 2010; Fleming et al., 2018; Johnson et al., 2006).
Despite evidence suggesting that men’s preconception health affects child outcomes (Kasman et al., 2020, 2021) and recommendations for men to optimize preconception health (Frey et al., 2008; Kotelchuck & Lu, 2017), the greater proportion of this work focuses on women. Men are more likely to engage in risky behaviors and less likely to modify these behaviors overtime, are less aware of the health behavior changes they need to make or how these health states and behaviors can impact their offspring, and are less inclined to seek health care (Besera et al., 2016; Goossens et al., 2019; Marcell et al., 2016; Mitchell et al., 2012; O’Brien et al., 2015). A better understanding of how men improve their health in the context of future fertility planning can inform how interventions are developed, retooled, and targeted.
Studies that utilized a preconception health lens to examine future fertility planning disproportionately focused on people living with specific underlying risk factors or health conditions (e.g., diabetes and HIV/AIDS) and couples exploring Assisted Reproductive Technologies (ART). With the advent of and success rates in antiretroviral therapies, many people living with HIV/AIDS seek opportunities to fulfill their desire to become parents. Because of the health impact HIV exposure can have on future generations, researchers make concerted efforts to model the fertility intentions of this population to optimize their health, reduce the risk of vertical transmission to infants, and minimize the burden of unintended pregnancies in this population (Bai et al., 2017). Similar attempts are being used to optimize the preconception health status of couples seeking ART to ensure maximum positive outcomes. These studies are based on the underlying premise that the health status of an individual can be an important consideration for fertility planning and gives credence to predicting fertility intentions among men based on their preconception health profile. These studies underscore the need to improve men’s health prior to pregnancy to ensure that all pregnancies are planned and wanted, optimize men’s biological and genetic contribution, and advance men’s capacity for fatherhood (Kotelchuck & Lu, 2017).
Theoretical Underpinning
To further conceptualize and examine the multifaceted factors associated with men’s preconception health and their future fertility intentions, the Theory of Conjunctural Action (TCA), an adaptive life course framework, was used to guide this study. The TCA posits that fertility intentions are a function of deliberative and nondeliberative cognitions. It emphasizes the role of social structures such as the social relations within classes, races, cultures, and traditions in creating behaviors and shaping social action. The term “conjuncture” implies a “coming together” of circumstances, including materials (objects or resources in one’s environments) and schemas (i.e., ideas, values, beliefs, norms) that form or shape actions and outcomes (Johnson-Hanks et al., 2011, p. 99).
The TCA integrates both proximal and distal frameworks that have over the years been applied to understand fertility factors including micro- and macro-level processes, life course perspectives, sequential decision–making, and period effects (Johnson-Hanks et al., 2011). It is also useful for examining nonbinary fertility concepts, such as ambivalence toward fertility intentions. This framework, though complex and still developing, has been applied to several studies exploring fertility intentions and behaviors (Pearce & Davis, 2016; Shreffler et al., 2019). By applying the TCA framework in this study, the individual and collective experiences of men on preconception health and fertility intentions will be better understood.
Men’s preconception health was conceptualized as the totality of their physical, mental, and social well-being beginning from pubarche and continuing throughout the reproductive years (Centers for Disease Control and Prevention [CDC], 2022; World Health Organization, 2022). Based on this conceptualization, the observed preconception health status indicates a coming together of the schemas (i.e., men’s ideas, social norms, beliefs, and values) and materials (i.e., resources and environments such as policies, legislations, neighborhoods, and family relations that exist outside the schema) that have interacted over their life course to create the structures in which these health states and behaviors are formed. Men’s preconception health was, therefore, operationalized as a latent construct characterized by unobserved social structures and mechanisms (Figure 1). We assumed that (a) men who experienced similar structures will exhibit similar preconception health profiles and will differ from men who experienced other structures and (b) men with better preconception health profiles will have higher odds for future childbearing.
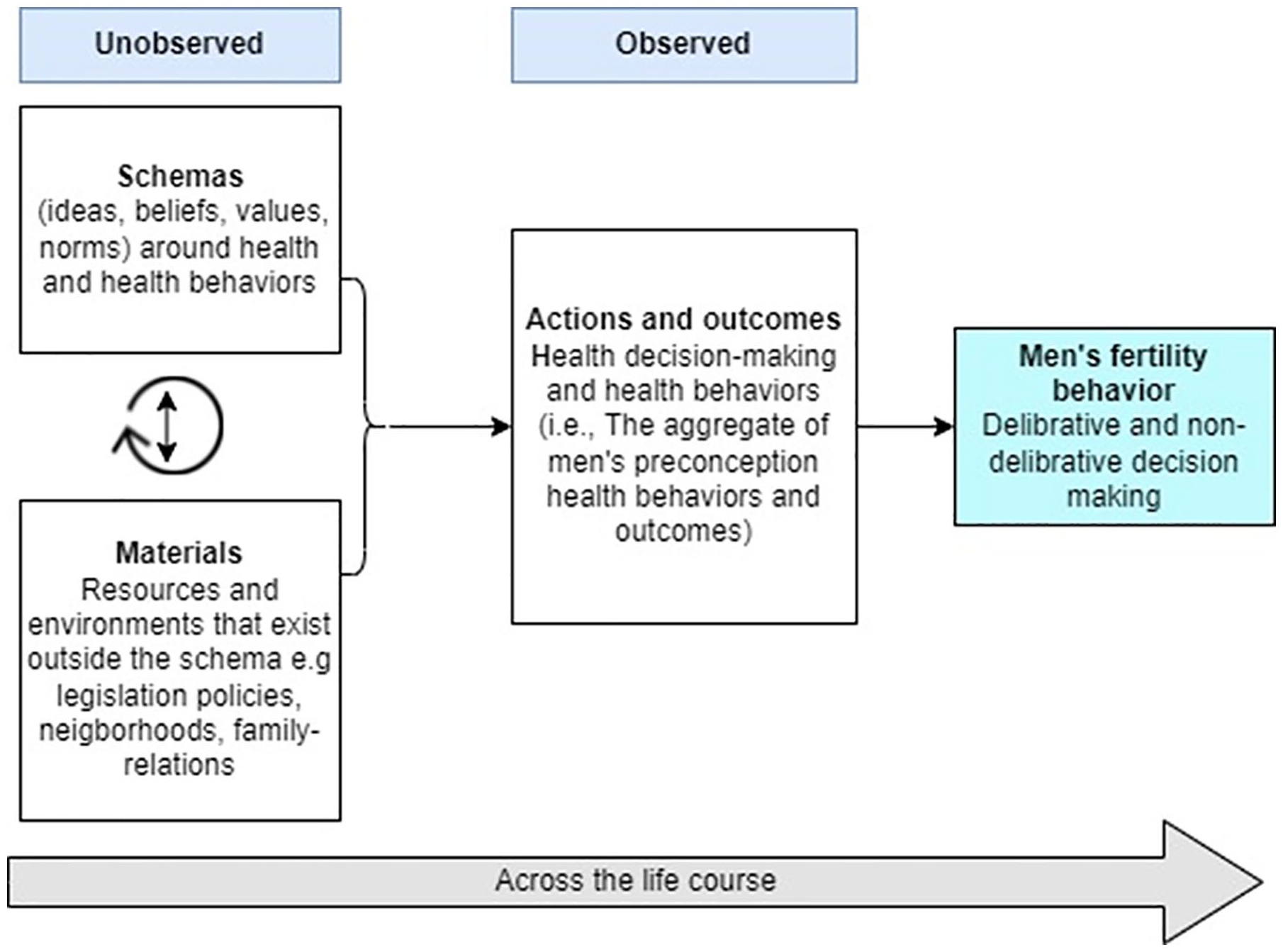
Theory of Conjunctural Action Applied to Conceptualizing Men’s Preconception Health and its Relationship to Fertility Behavior
Preconception risk factors such as risky sexual behaviors and substance use or chronic disease and poor nutrition often co-occur (Parkes et al., 2020; Toivonen et al., 2017). Although emerging evidence suggests that men’s exposure to multiple preconception risk factors increases the likelihood for poorer reproductive outcomes (Kasman et al., 2020, 2021), most epidemiological studies focused on preconception health often measure the effect of an individual risk factor (e.g., environmental exposures, substance use and sexual risk behaviors) on an outcome. These approaches that examine the independent effects of preconception risk factors on an outcome, despite their co-occurrence, preclude the opportunity to examine their interdependencies and limit our understanding of the collective effects of these factors. Guided by the TCA framework, this study therefore aimed to (a) examine the constellation of factors that constitute men’s preconception health status and (b) measure the association between men’s preconception health status and childbearing intentions.
Method
Study Participant and Data Source
Pooled data from the 2011–2019 National Survey of Family Growth (NSFG) male respondent file were used. The NSFG is a multi-stage, stratified, nationally representative probability sample of the noninstitutionalized U.S. population aged 15 to 44 years (extended to 49 years in the 2015–2017 cycle). Details on data collection methods are reported elsewhere (National Survey of Family Growth, 2018). Men included in this study were 20- to 44-year-olds who were sexually experienced (i.e., if they ever had vaginal intercourse) with a female, fecund, and had at least one fecund partner (Casey et al., 2016; Choiriyyah et al., 2015). Those who reported a current pregnant partner were excluded. These criteria were selected to identify those who, at the time of data collection, were at risk of experiencing a pregnancy with their partner (von Elm et al., 2007) (Figure 1). The study was exempt from review by the Institutional Review Board Saint Louis University because only publicly available de-identified data published by the National Center for Health Statistics were used.
Measures of Men’s Preconception Health Status (Manifest Variables)
Using the preconception health indicators recommended by the CDC, men’s preconception health was measured using eight lifestyle preconception health variables—number of sexual partners, sexual risk-taking behavior, condom use consistency, general health status, alcohol, drug use, exposure to sexually transmitted infections (STI), and body mass index (BMI). For a detailed description of these manifest variables, see eTable 1 in the Supplemental Material.
The number of female sexual partners was assessed with the question, “How many female partners in the last 12 months?” and was recoded as 1 = none or one female partner and 2 = more than one female partner (Choiriyyah et al., 2015). Condom use was measured with the question, “In the last 12 months, how often did you use a condom with your partner or partners?” and was recoded as 1 = used consistently and 2 = inconsistent use to no use (Casey et al., 2016). STI and HIV risk-taking behaviors were measured using five questions that asked whether a man (a) had sex with a female intravenous drug user, (b) gave money or drugs to a female for sex, (c) took money or drugs from a female for sex, (d) had sex with an HIV-positive female, and (e) had any other sexual experience with another man. These variables were used to create a single STI/HIV risk dummy variable (1 = no, 2 = yes) (Choiriyyah et al., 2015). General health status was measured using the question “In general, how is your health?” and was dichotomized as 1 = excellent to good and 2 = fair to poor.
Alcohol use was measured using three questions that assessed the frequency and quantity of alcohol use. These variables were recoded as “no drinking” if no alcohol use was reported in the past 12 months and 30 days, “low risk” if alcohol use was reported in the past 30 days but not at binge levels, “medium risk” if they binge drank less than 5 times in the past 30 days, and “high risk” if they binge drank 5 or more times in the past 30 days (National Institute on Alcohol Abuse and Alcoholism, n.d.). For analytical purposes, these risk categories were further recategorized into two risk groups: 1 = no to low-risk drinking and 2 = medium- to high-risk drinking.
Six questions on drug use inquired about marijuana, cocaine, crack, methamphetamine, and injection drug use in the past 12 months. These variables were recoded into a single “any drug use” category with a binary (yes/no) response. Five questions measured the presence or absence of sexually transmitted diseases. These questions asked whether the respondent was told that he had gonorrhea, chlamydia, herpes, genital warts, and/or syphilis in the last 12 months. Reponses were dichotomized (yes/no) to create a single STI status dummy variable.
Body mass index was collected as a continuous variable and was categorized into four distinct groups—underweight (less than 18.0), normal weight (19 to <25), overweight (26 to <29), and obese (30 or higher) (CDC, 2020). These measures were dichotomized into “under to normal weight” and “overweight to obese.” Variables were dichotomized following sensitivity analysis, which showed no significant differences between the categories by sociodemographic variables.
Fertility Intentions (Outcome Variable)
Future childbearing intentions were assessed by participants’ response to the following two questions: “Do you intend to have (more) children?” with response options 1 = intends to have more, 2 = does not intend to have more, and 3 = does not know intent. The second question was: “If you got (your wife or partner / a female) pregnant now, how would you feel?” with response options 1 = very upset, 2 = a little upset, 3 = a little pleased, 4 = very pleased, and 5 = wouldn’t care. These variables were recoded to indicate 1 = definite no, 2 = definite yes, 3 = far/contingent intention, and 4 = indifferent/ambivalent intentions (Bernardi et al., 2015; Philipov et al., 2015; Yoo et al., 2014).
Covariates
Covariates were sociodemographic characteristics that were independently associated with the exposure, outcome, or both and relevant to the literature. These included residential status (urban, suburban, and rural), insurance status, reproductive wellness (no doctor’s visit, nonreproductive health doctor’s visit, and reproductive health visit), employment stability, poverty income ratio, educational attainment, race/ethnicity, immigration status, union type (married, separated/widowed/divorced and never married), age, number of children they ever fathered, and age of sexual debut.
Statistical Analysis
Latent Class Analysis
Latent class analysis (LCA) is a latent variable framework that utilizes categorical data to measure underlying unobserved quantities (Lanza et al., 2012) and was applied to this study in an exploratory capacity (Bartholomew et al., 2011). This method was used because of the heterogeneity in preconceptional behaviors, interrelatedness between these risk factors, and the utility of this method to identify unique dimensions of preconception health from these variables. An iterative maximum likelihood method was used to identify the prevalence of latent classes (Gamma), representing the proportion of mutually exclusive groups within the classes, and the item response probability representing the probability of endorsing a particular item within each class.
The LCA model was fitted starting with the two-class model with one-unit increment in the number of classes (three-, four-, and five-class models). The model of best fit was determined based on the Bayesian Information Criterion (BIC), entropy, mean posterior probabilities and class size (Lanza et al., 2012), the interpretability of the solution, parsimony of the model, and relevance to the literature. The smaller BIC value indicates better model fit. Entropy denotes how accurately a model defines a class with values closer to 1 considered ideal (Collins & Lanza, 2009). Mean posterior probabilities are presented in matrix with probabilities of membership in each class on the diagonal. Diagonals close to 1 (0.8 and above) and off-diagonals close to zero are considered more reliable models. Analyses were completed using the PROC LCA procedure in SAS 9.4 (SAS Institute, 2013). The combined 8-year weight for the 2011–2019 period was applied to all analyses.
Analysis of Missing Data
To ensure that the latent class solution was robust to missingness, sensitivity analysis was performed, and multiple imputation techniques were applied. The PROC MI technique with the fully conditional specification (FCS) statement using the discriminant function method (Van Buuren, 2007; Yuan, 2011) was used to create five imputed data sets. Each of these data sets was subsequently used to fit independent LCA models which were compared with the final solution (i.e., the model derived using the full-information maximum likelihood [FIML] technique) (eFigure 1 in the Supplemental Material).
A classify-analyze approach was subsequently used to create a preconception health phenotype (PhP) variable which was used as the exposure variable to fit multinomial regression models with the fertility intentions outcome variable. Although “phenotype” is a biological term that refers to the physical expression of genes, it was applied to this study to denote the set of observable characteristics that distinguished members within a specific latent class from those in other latent classes. Regression models estimated odds ratios (ORs) with corresponding 95% confidence interval (CI). Statistical significance was placed at p value <.05% and 95% CIs not overlapping 1.0.
Results
Descriptive Statistics
A total of 10,223 men were included in the final sample and had an average age of 30.7 years. Most men were non-Hispanic White (n = 5,219, 57.4%; non-Hispanic Black: n = 2,097, 14.1% and Hispanic n = 2,221, 21.3%), never married (n = 6,155; 55.4%) had some college education (n = 3,320; 32.0%), and had stable employment (n = 7,073; 72.4%). More than 80% (n = 7,116) of men reported inconsistent to no condom use, 61.9% (n = 6,279) reported being overweight or obese, and 18.6% (n = 2,378) reported having two or more sexual partners. About a third (n = 3,464; 32.2%) used drugs and 41.8% (n = 3,669) used alcohol at medium- to high-risk levels.
Latent Class Analysis
The three-class model represented an optimal solution for the data given 50 random start values, highest entropy values, and separation into distinct classes based on posterior probabilities of class membership (probability ranging from .84 to .97 within the class) (eTable 2 in the Supplemental Material). In addition, as a classify-analyze technique was applied to create a PhP variable, it was important to have high mean posterior probabilities to reduce random error (eTable 3 in the Supplemental Material).
Most men (n = 6,652; 69%) belonged to Class 1 “lowest risk group.” This class was characterized by high endorsement probability of inconsistent/no condom use (82%) and overweight/obese (65.3%); all other prevalence estimates for each manifest variable was low. Class 2 “sexual risk takers” had the lowest prevalence of latent classes (n = 1,092; 8.1%) and was characterized by high endorsement probability for multiple sexual partners (94.2%), inconsistent/no condom use (68.2%), medium/high alcohol use (54.1%), and overweight/obese (63.8%). Approximately 23% (n = 2,479) of men belonged to Class 3 “substance users” and were characterized by high endorsement probability for inconsistent/no condom use (79.6%), medium-/high-risk alcohol use (66.9%), drug use (98.8%), and overweight/obese (50.8%) (Figure 2). Item response probabilities >.50 were selected to facilitate interpretation of class membership.
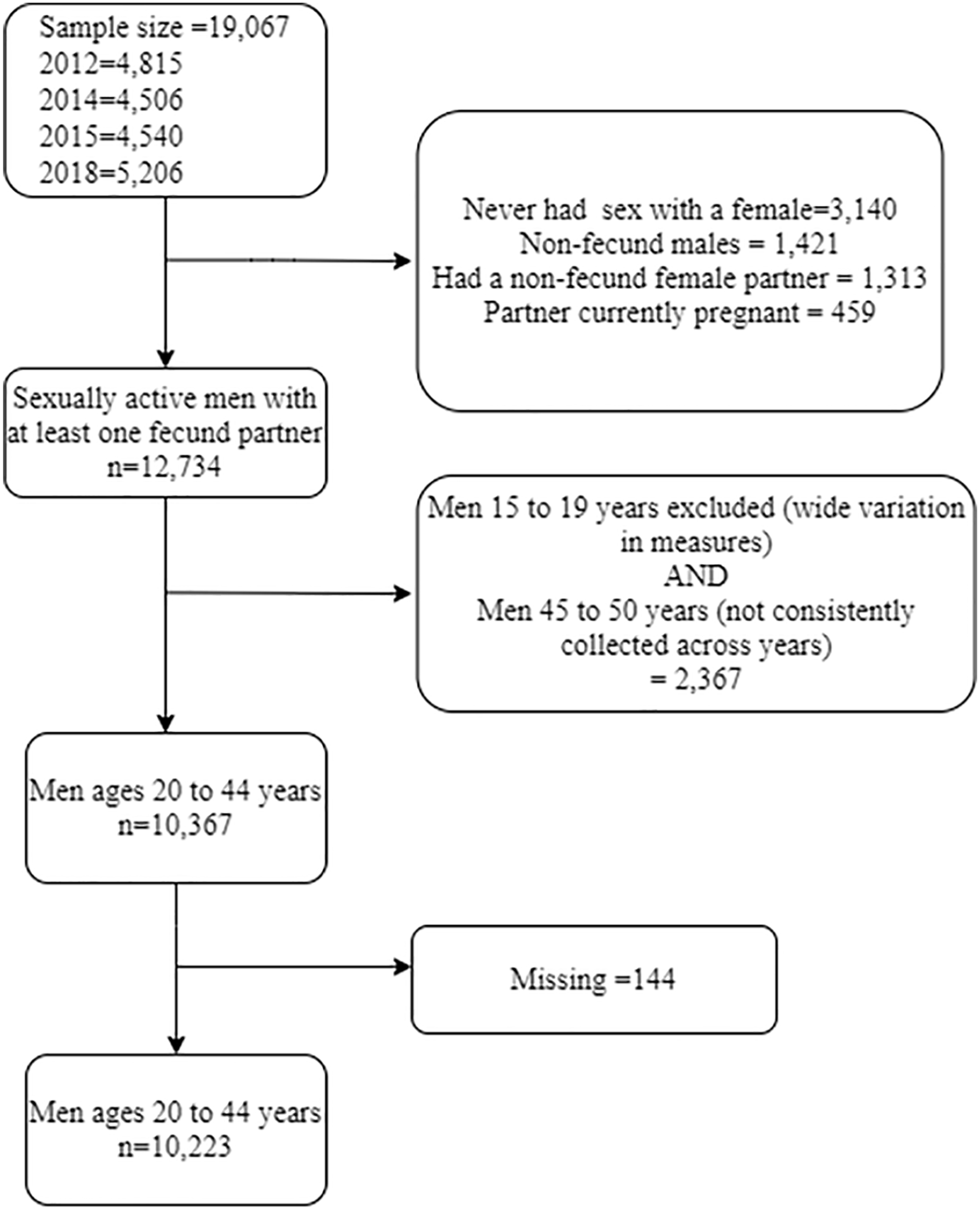
Consort Diagram for Study Inclusion and Exclusion Criteria.
Multinomial Regression with PhP Predictor
Most men belonged to the “definite yes” group (n = 4,393; 43%) followed by the far/contingent intention category (n = 3,970; 38.8%). Across all fertility intention categories, most men were in the “lowest risk” class (between 66.4% and 74% of men). Most men in the lowest risk class had “definite yes” intentions (n = 2,993; 74%), whereas 22.9% (n = 429) of substance users had “definite no” fertility intentions, 25.9% (n = 1,045) had “far or contingent intentions,” and 22.1% (n = 26) had “indifferent or ambivalent” intentions. Most (11.3%) “sexual risk-takers” had “indifferent or ambivalent intentions (Figures 3 and 4).

LCA Results From the Three-Class Model Showing Preconception Health Phenotypes

Weighted Percentage Distribution of PhP by Future Fertility Intentions
Table 1 provides the crude and adjusted estimates of the multinomial regression analysis for fertility intentions and preconception health status. “Substance users” had increased odds for “definite no” and “far or contingent” intentions than “definite yes” intentions (adjusted OR [aOR]: 1.47, 95% CI: [1.18, 1.84] and aOR: 1.48, 95% CI: [1.25, 1.76], respectively). “Sexual risk-takers” had increased odds for “definite no” fertility intentions (aOR: 1.51, 95% CI: [1.13, 2.01]) than “definite yes” intentions. No statistically significant differences were observed in the association between PhPs and “indifferent/ ambivalent” intentions.
Crude and Adjusted Estimates of the Effects of Preconception Health Status on Fertility Intentions.

Note. The adjusted model controlled for the effect of insurance coverage, employment consistency, poverty income ratio, education status, race/ethnicity, union status, number of children, and age.
Bold indicates statistically significant associations at p <.05.
Discussion and Conclusion
Summary of Results
This population-level study identified an association between men’s preconception health and their future fertility intentions. Based on the assumptions of the TCA framework guiding this study in which we hypothesized that men who experienced similar structures will exhibit similar preconception health latent profiles, we identified three distinct subgroups of men’s preconception health: lowest risk, sexual risk-takers, and substance users. Men who exhibited poorer preconception health (i.e., belonging to the substance users and sexual risk-takers categories) had reduced odds for desiring a future pregnancy. The science on measuring preconception health and fertility planning and their relationship remains a challenge in family planning research. Our results provide (a) new insights on how preconception health can be conceptualized and measured, (b) fills a knowledge gap on the relationship between men’s preconception health and fertility planning by identifying complex combinations of preconception risk factors as they relate to reproductive planning, and (c) provides initial evidence on the utility of modeling future fertility intentions using a preconception health lens.
Across all latent classes, men were very likely to be overweight/obese. As the evidence on the risks for adverse birth outcomes due to poor paternal preconception health including chronic metabolic diseases becomes better established (Kasman et al., 2020, 2021), our findings emphasize the need to address obesity among all men independent of fertility intentions. Inconsistent condom use was also prevalent across all latent classes and underscores the need to examine individual and structural factors influencing this phenomenon, especially for substance users and sexual risk-takers. With the increasing prevalence of STIs, it is necessary to identify the factors at the intrapersonal, interpersonal, community, and society levels (e.g., beliefs and attitudes toward condom use, knowledge of its benefits, improper use, partner characteristics and condom use conversations, timely access to condoms, and reproductive health care) that continue to contribute to inconsistent use.
One in six men belonged to the “definite no” fertility intentions category, yet their preconception health status indicated high substance use and sexual risk-taking. In other words, men in this category were not actively preventing pregnancies, thereby increasing the risk of pregnancies occurring at suboptimal paternal health. This finding is consistent with previous studies (Campbell et al., 2019) and emphasizes the need for family planning in this population. This study provides additional insight on how male population subgroups may benefit from different interventions to manage reproductive health at the population level including long-term reversible contraceptive methods and/or educational interventions. Health professionals need to proactively assess men’s fertility intentions (within and outside clinical settings) and offer counseling on health behaviors or consistent contraception. Further studies are needed to understand the social conditions that interact over the life course to create these preconception health profiles and their impact on fertility planning. Although the current study adjusted for the effects of social factors (such as educational attainment, access to and utilization of reproductive health care, and racial/ethnic belonging) that can influence the relationship between preconception health and fertility planning, the authors have noted elsewhere that these social determinants of health may impact men’s preconception health in ways that differ from conventional understanding (Anakwe et al., 2022).
“Far/contingent” intentions were positively associated with belonging in the substance user’s subgroup but not in the “sexual risk-takers” category. While this group, in the short term, may benefit from substance use interventions, longitudinal studies that examine how fertility intentions change overtime vis-à-vis their preconception health may provide better insight to the intervention needs of this population. Because more than 30% of the sample belonged to this category, it is imperative to monitor their fertility planning and health behaviors as they transition through different life stages. Men may be more hesitant to utilize long-lasting contraceptive methods because their pregnancy intentions may change overtime (Campbell et al., 2019).
Most studies on fertility intentions suggest that ambivalent intentions are associated with higher risk-taking, particularly among males (Higgins et al., 2012). This study observed a null association which may be attributed to the small sample size of those who had ambivalent or indifferent intentions. Nationally representative data sets that measure pregnancy ambivalence are sparse, which poses serious data constraints on exploring this intention category further. There is a need for data that measure fertility ambivalence more robustly.
Study Implication, Strengths, and Limitations
Applying LCA to the study provided a nuanced understanding of the preconception health needs of men and how it factors into their fertility planning behaviors which have utility for maternal and child populations. Our study demonstrates that men in the “sexual risk-takers” category have different risk profiles from “substance users,” which suggests that these independent groups may benefit from different types of preconception and reproductive planning interventions.
With more than 80% of men in this study reporting inconsistent condom use, conversations with men about condom use remain important because this practice can simultaneously protect against STIs and pregnancy when used correctly and consistently. Trends in men’s inconsistent condom use have increased and correspond with the increasing incidence of STIs in the United States (CDC, 2021; Lindberg et al., 2021). Although men are less likely to seek or utilize health care in general, and reproductive health care more specifically, (Besera et al., 2016; Goossens et al., 2019), there are a plethora of factors that contribute to men’s inconsistent condom use including beliefs and attitudes toward condoms, lack of knowledge, partner and relationship dynamics, and social networks (Flood, 2003; Fortenberry, 2019; Hubach et al., 2014). Some studies have also reported a disconnect between men’s knowledge of the value of condoms for both STI and pregnancy prevention (de Visser, 2005; Flood, 2003), which necessitates more strategic efforts toward understanding how men navigate their sexual and reproductive health in the context of fertility planning. Approaches that ask men about these conversations with a (potential) partner can provide nuanced insight on how public health practitioners and health care providers can support men in developing their reproductive health agency. Exposure of males to formal sex education has been positively associated with dual contraceptive method use (i.e., both male condom use and a female pregnancy prevention method; Jaramillo et al., 2017). Tailored interventions that educate and support men in understanding and managing their sexuality are needed.
Interventionist and health care practitioners will find value in this study as it identifies and provides insights on the unique preconception health and family planning needs for this population, which can guide how interventions are designed and how conversations should be directed. For instance, sexual and reproductive health education that is tailored toward men can be co-created with families, schools, community-based organizations, and local health departments. Program content should include conversations on reproductive planning such as actively preventing STIs and unplanned pregnancies, and the importance of optimizing health prior to pregnancy. As noted by Maas and colleagues (2022), men with unhealthier preconception lifestyle are less likely to utilize preconception care–related information. However, men valued information that was provided by their health care provider (Maas et al., 2022). More needs to be done to make clinics more male-friendly, decrease provider bias toward men’s reproductive health, and routinely engage men in reproductive wellness (Hogg et al., 2019; Robbins et al., 2016). Preconception health for men is typically not discussed in health care settings and should be part of men’s health care training. Pipelines for male-specific providers, which complement the obstetrics and gynecology field, should be created to administer preventive reproductive health services. Inequitable systemic barriers, such as lack of access to free reproductive health screenings, should be eliminated for men. Men’s fertility intentions should also be routinely assessed and resources that can support them to plan for or prevent pregnancies should be provided.
This study utilized nationally representative data and applied an advanced statistical technique to explore a phenomenon that was hither-to unexplored, hence providing much needed information on the role of preconception health on future fertility planning. This is the first study to our knowledge that utilizes this approach to examine men’s preconception health. It also applies a multidimensional fertility intentions construct providing a more nuanced perspective to reproductive planning.This study was limited by its utilization of cross-sectional data and restriction of causal inferences. Using self-reported data on a limited number of preconception risk factors was also a limitation. For instance, measures on smoking and high blood pressure were not utilized because they were either not measured at all or were inconsistently measured across the survey years. Preconception risk factors could, therefore, be underreported. A high prevalence of inconsistent condom use was reported in this study, which may not necessarily indicate poor preconception health, but a limitation of the data source to comprehensively capture participants’ contexts including partners’ condom use or actively trying to become pregnant. However, the NSFG data were well suited to answer the questions posed by this study, and findings have utility for clinicians and practitioners.
This study lays the foundation for utilizing an approach that models future fertility from the preconception health status of men and demonstrates that concerted efforts are needed to better engage men in preconceptional health care more holistically. Furthermore, it can guide intervention frameworks that seek to optimize the health of men prior to conception.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883221135764 – Supplemental material for Men’s Preconception Health and Fertility Intentions: A Latent Class Analysis Approach
Supplemental material, sj-docx-1-jmh-10.1177_15579883221135764 for Men’s Preconception Health and Fertility Intentions: A Latent Class Analysis Approach by Adaobi Anakwe, Rhonda BeLue, Hong Xian and Pamela Xaverius in American Journal of Men's Health
Footnotes
Author Contributions
AA: Conceptualized and designed the study, analyzed data, and drafted initial manuscript. RB: Contributed to study conceptualization and design, analysis, and critical manuscript revisions. HX: Contributed to data analysis and interpretation. PX: Contributed to study design and critically revised the manuscript for intellectual content.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was received through the Society for Family Planning Research Fund (Grant Number: SFPRF14-ES2).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.