
Abstract
The purpose of this meta-analysis was to evaluate the efficacy and safety of the once-daily use of 5 mg tadalafil in the treatment of patients with premature ejaculation. The databases MEDLINE/PubMed, EMBASE, and Cochrane Library from January 1980 until December 2024 were searched to identify randomized controlled trials (RCTs) that referred to the use of tadalafil for the treatment of premature ejaculation. A systematic review and meta-analysis was conducted. Five publications involving 397 patients were included in the meta-analysis. No statistically significant difference was identified between tadalafil and placebo for intravaginal ejaculatory latency time (IELT; mean difference [MD] = 68.43; 95% confidence interval [CI] = [−12.59 to 149.45]; p = .10) and Arabic index of premature ejaculation (AIPE; MD = 11.44; 95% CI = [−11.79, 34.66]; p = .33). Tadalafil appeared to improve the score of the premature ejaculation diagnostic tool (PEDT; MD = −0.30; 95% CI = [−0.57, −0.03]; p = .03). In terms of adverse events, the tadalafil group was significantly higher than the placebo group for headache (odds ratio [OR] = 16.06, 95% CI = [3.80, 67.94], p = .0002), back pain and myalgia (OR = 21.76, 95% CI = [4.17, 113.53], p = .0003), flushing (OR = 6.05, 95% CI = [1.05, 34.92], p = .04), and dyspepsia (OR = 10.27, 95% CI = [1.90, 55.96], p < .007). Our meta-analysis indicates that the once-daily use of 5 mg tadalafil had no statistically significant effect in the treatment of premature ejaculation. Meanwhile, the tadalafil therapy showed a higher risk of complications.
Introduction
The premature ejaculation (PE) is described as the phenomenon that occurs when ejaculation happens persistently sooner than a man or his partner would like during sexual intercourse (Raveendran & Agarwal, 2021). The prevalence ranges from 20% to 30% in sexually active age men (Laumann et al., 2005; Patrick et al., 2005). The International Society for Sexual Medicine (ISSM) defines PE as: (a) ejaculation which always or nearly always occurs prior to or within about 1 minute of vaginal penetration (lifelong PE), or, a clinically significant and bothersome reduction in latency time, often to about 3 minutes or less (acquired PE); (b) inability to delay ejaculation on all or nearly all vaginal penetrations; and (c) negative personal consequences, such as distress, bother, frustration, and/or the avoidance of sexual intimacy (Serefoglu et al., 2014).
Although the exact etiology of PE remains unclear, the leading theories focus on the disturbances in the activities of neurotransmitters, penile hypersensitivity, erectile dysfunction (ED), genetic predisposition, hormonal problems, and prostatic diseases (Culha et al., 2020; Gopalakrishna et al., 2021; McMahon et al., 2016). The treatment of PE includes non-pharmacological and pharmacological treatment. Psychological therapy and various behavioral therapies are also used in the treatment of PE (Raveendran & Agarwal, 2021). Pharmaceutical approaches predominantly comprise the prescription of selective serotonin reuptake inhibitors (SSRIs), tricyclic antidepressants, phosphodiesterase type 5 inhibitors (PDE5-Is), and/or topical anesthetics (Leisegang et al., 2023).
Tadalafil, available in both once-daily and on-demand dosing regimens, is a PDE5-I that has been globally approved for the treatment of ED (Wang et al., 2023). In recent years, clinical trials have explored the once-daily administration of tadalafil for the treatment of PE. Some of these trials have yielded encouraging outcomes, suggesting that daily use of tadalafil may significantly improve PE; however, others have found no significant difference compared to a placebo. Until now, there has been no systematic meta-analysis assessing the efficacy and safety of a once-daily 5 mg dose of tadalafil in the treatment of PE. Consequently, we conducted a comprehensive meta-analysis to evaluate the effects of once-daily use of tadalafil in patients suffering from PE.
Method
Inclusion and Exclusion Criteria
We included randomized controlled trials (RCTs) in which people with lifelong PE according to the ISSM married and in a stable sexual relationship for at least 1 to 6 months. We included studies provided that preliminary results were available. We also included non-English studies in the meta-analysis. RCTs were required to meet the following inclusion criteria: (a) studied the efficacy and safety of once-daily use of tadalafil for the treatment of PE, (b) provided sufficient data for analysis, including primary outcome intravaginal ejaculatory latency time (IELT) and adverse events, and (c) the full text of the study could be accessed. The exclusion criteria were as follows: (a) publications that did not contain original data; (b) duplicated publications; (c) no use of IELT; and (d) studies without merging analysis data.
Search Strategy and Trial Selection
Trials were identified through searches of MEDLINE/PubMed, Embase, and Cochrane Library, as well as gray literature and reference lists of systematic reviews through December, 2024. The following search terms were used: Tadalafil, Premature ejaculation, Phosphodiesterase 5 Inhibitors, and Randomized controlled trials. Abbreviations (PE, PDE5, RCT) were also searched. Two independent researchers screened and assessed for eligibility of relevant RCTs according to the inclusion and exclusion criteria. Researchers resolve disagreements through discussion. The study selection process is presented by a diagram in Figure 1.
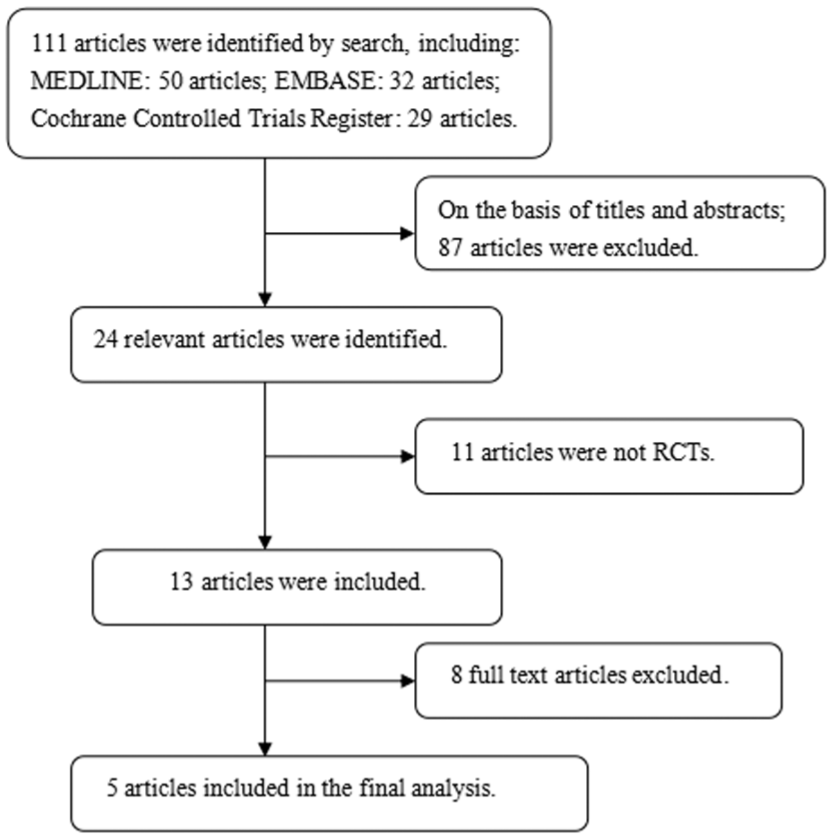
Flow Diagram of the Study Selection Process
The researchers independently performed the data extraction for the meta-analysis, which included the following: (a) the name of the first author and the publication year, (b) the design of the study, (c) the treatment therapy that the patients received, (d) the sample size, (e) the duration of treatment, (f) the outcome measurements, and (g) the eligibility criteria of the study. The characteristics of the individual studies are listed in Table 1.
Characteristics of Individual Study.

Note. RCT = Randomized Controlled Trials IELT = Intravaginal Ejaculatory Latency Time; PEDT = Premature Ejaculation Diagnostic Tool; PE = Premature Ejaculation; AIPE = Arabic Index of Premature Ejaculation; ED = Erectile Dysfunction.
Quality Assessment
The quality of the RCTs was assessed in terms of sequence generation, the concealment of allocation procedures, blinding, incomplete outcome data, selective outcome reporting, and other sources of bias. The studies were then classified qualitatively according to the guidelines published in the Cochrane Handbook for Systematic Reviews of Interventions v.5.1.0 (Higgins et al., 2011). Based on the quality assessment criteria, each study was rated and assigned to one of the three following quality categories: +, low risk of bias; ?, unclear risk of bias; -, high risk of bias. Differences were resolved by discussion among the authors. The bias of all the identified studies that we searched was at low risk in general (Table 2).
ROB for Included Randomized Controlled Trials.

Note. ROB: Risk Of Bias; +, Indicates Low Risk of Bias; ?, Unclear Risk of Bias; -, High Risk of Bias.
Outcome Measurement and Statistical Analysis
Our primary outcome, IELT, was defined as the time from intravaginal intromission until intravaginal ejaculation. The IELT was calculated by female partners using a stopwatch. The secondary outcome was the Arabic Index of Premature Ejaculation (AIPE) and Premature Ejaculation Diagnostic Tool (PEDT). The most commonly reported adverse events are used to assess safety. Regarding the dichotomous outcomes, odds ratio (OR) with a 95% confidence interval (CI) was used where available. Mean difference (MD) with 95% CI was used to report continuous outcomes. The comparative effects were initially analyzed by the traditional pairwise meta-analysis method using Cochrane Collaboration review manager software (RevMan v.5.3.0). We estimated the odd risk for dichotomous outcomes and the MD for continuous outcomes pooled across studies by using the DerSimonian & Laird random-effects model (DerSimonian & Laird, 1986). A “fixed-effects” statistical model was used if there was no conspicuous heterogeneity. A “random-effects” model was used if heterogeneity was detected. The tests for heterogeneity were performed using Chi-square tests with the significance level set at I2 ≥ 50%. A sensitivity analysis was performed to determine whether the heterogeneity was a result of low study quality.
Results
We identified six eligible RCTs (Abou Faddan et al., 2022; Abu El-Hamd, 2018; Al-Shukri et al., 2022; Dell’Atti et al., 2017; Mohamed Gharib et al., 2022; Ozcan et al., 2017); one was excluded for lacking comparison group. Finally, five RCTs involving 397 lifelong PE male patients in a stable sexual relationship were included in our meta-analysis. In these studies, patients were randomized to the treatment group receiving 5 mg tadalafil once daily. The comparison group of four studies was placebo, and one study used the lidocaine spray.
IELT
A total of five studies including 397 patients (204 in the tadalafil group and 193 in the control group) contributed to the analysis of the change of IELT. Heterogeneity was found among the trials (p < .00001, I2 = 100%), and a random-effects model was thus chosen for the analysis. The forest plots reflected an MD of 68.43 (95% CI = [−12.59, 149.45], p = .10). The results revealed that there was no marked difference between the once-daily use of 5 mg tadalafil and placebo in the change of IELT for patients with lifelong PE (Figure 2).

Forest Plot Shows Changes in Intravaginal Ejaculatory Latency Time (IELT; Min)
AIPE and PEDT
Only two studies reported the AIPE and PEDT. When these studies were pooled, the analysis demonstrated that there was no statistically significant variance in the change of AIPE score between the treatment and placebo arms. The MD for AIPE scores was 11.4 (95% CI = [−11.79, 34.66], p = .33), indicating that daily administration of 5 mg tadalafil did not substantially enhance AIPE scores in comparison to placebo. For the change of PEDT scores, the forest plots reflected an MD of −0.30 (95% CI = [−0.57, −0.03], p = .03). The results revealed that once-daily use of 5 mg tadalafil statistically improved the PEDT scores. However, the studies only encompassed a total of 85 patients. This is illustrated in Figures 3 and 4.

Forest Plot Shows Changes in Score of Arabic Index of Premature Ejaculation (AIPE)

Forest Plot Shows Changes in Score of Premature Ejaculation Diagnostic Tool (PEDT)
Adverse Events
All the RCTs which included in the meta-analysis did not report serious adverse effects. The most common adverse events in patients treated with tadalafil included headache, myalgia, back pain, flushing, and dyspepsia. Four studies with available data were included in our analysis. From the analysis, the once-daily use of 5 mg tadalafil was associated with a significantly higher incidence of adverse events (headache [OR = 16.06, 95% CI = [3.80, 67.94], p = .0002], back pain and myalgia [OR = 21.76, 95% CI = [4.17, 113.53], p = .0003], flushing [OR = 6.05, 95% CI = [1.05, 34.92], p = .04], and dyspepsia [OR = 10.27, 95% CI = [1.90, 55.96], p < .007]; Figure 5).

Forest Plot Shows Differences Between the Groups for Adverse Events
Discussion
Due to its highly complex etiology and pathophysiology, PE has seen numerous treatment options proposed and implemented to date. The treatment of PE primarily relies on medications, the majority of which are used off-label, with the exception of dapoxetine, while local anesthetic agents and SSRIs have repeatedly demonstrated their effectiveness in the management of lifelong PE (Asimakopoulos et al., 2012). PDE5-Is are being studied in numerous clinical trials for the potential benefits they offer in the treatment of PE. PDE5-Is increase the activity of cyclic guanosine monophosphate (cGMP) and nitric oxide (NO) in the medial preoptic area. Thus, this leads to a reduction in sympathetic nervous system tone and may ultimately result in delayed ejaculation (Krishnappa et al., 2019; Pfaus, 1999). It is thought that PDE5-Is can delay ejaculation by relaxing smooth muscles in peripheral organs such as the vas deferens, seminal vesicles, prostate, and urethra via the same NO-cGMP pathway (Chen et al., 2007). Besides, PDE5-Is could increase the perception of ejaculatory control, ejaculatory confidence, and overall sexual satisfaction (Raveendran & Agarwal, 2021).
In 2008, Mattos et al. first reported that tadalafil 20 mg on demand significantly improved the IELT compared with placebo (p = .001; Mattos et al., 2008). Previous meta-analyses shown an overall positive effect of the treatment of PE through the use of PDE5-Is (Asimakopoulos et al., 2012; Sun et al., 2015; Zhang et al., 2020). There were very few RCTs involving tadalafil in the previous meta-analyses, and they were all about on-demand use of tadalafil. In 2017, Ozcan et al. first evaluated the effect of 5-mg tadalafil daily use on PE in a single-blind RCT; they found mean IELT values in the PE group showed statistically significant improvement from baseline values (from 40.8 ± 8.1 to 190 ± 19.8 s, p < .05; Ozcan et al., 2017). To our knowledge, this is the first meta-analysis conducted to assess the efficacy and adverse events of once-daily use of 5 mg tadalafil in the treatment of PE.
The studies included in our analysis are all high-quality RCTs involving male patients from various regions, including Russia, Egypt, and Italy, with the aim of exploring the potential of tadalafil in the treatment of lifelong PE. All studies administered a 0.5-mg dose of tadalafil, which is consistent with the commonly used clinical dose. Among the studies, three did not specify whether blinding was employed, while two explicitly mentioned the use of a single-blind design. One study compared tadalafil with the local anesthetic lidocaine, while the others used a placebo, which did not show a significant improvement in ejaculation time, serving as the control. In terms of participant demographics, two studies included young male participants, while the remaining three focused on adult males. Future research could explore the differences in the effects of tadalafil across different age groups by conducting subgroup analyses based on age.
Regarding the results, four studies concluded that tadalafil was effective in prolonging ejaculation time, whereas one study found no significant effect. This finding contradicts the results of our analysis, where we primarily compared the change in IELT between tadalafil and placebo groups relative to baseline values. Our results indicate that tadalafil 5 mg once daily does not have a statistically significant effect on increasing IELT and AIPE, and the incidence of adverse events is higher. The discrepancy may be attributed to several factors, including sample size. Specifically, studies with larger sample sizes tend to produce more reliable results. In order to assess the impact of individual studies on the overall results, a sensitivity analysis was performed by sequentially excluding each study and re-conducting the meta-analysis. The findings indicated that the overall effect remained consistent, with no significant changes observed after the exclusion of any single study. This suggests that the conclusions drawn from this meta-analysis are robust and not unduly influenced by any individual study. Due to the results, the once-daily use of 5 mg tadalafil is not a promising alternative to de novo therapeutic strategies in the treatment of PE.
A number of limitations of the current study were identified. First, only five RCTs with small sample sizes were included in the meta-analysis. Second, in all RCTs included in the meta-analysis, the baseline characteristics of the patients are not completely consistent. Third, the specific components of the placebo in the control group were not clearly stated in some experiments; only two studies pointed out that multivitamin or lidocaine spray as placebo. Fourth, the treatment period and follow-up time of all RCTs ranged from 1 to 3 months. In addition, the findings of this meta-analysis were derived after manipulation of the data, which may also have resulted in bias. Further high-quality RCTs are strongly encouraged to learn more about once-daily use of 5 mg tadalafil in the treatment of PE.
Conclusions
In conclusion, our meta-analysis indicates that the once-daily use of 5 mg tadalafil had no statistically significant effect in the treatment of PE. Meanwhile, the tadalafil therapy showed a higher risk of adverse events.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.