
Abstract
This study aims to evaluate the strengths, opportunities, and facilitators in the implementation of the National Policy for Comprehensive Men’s Health Care (PNAISH) in Brazil in response to user demands. A mixed-method approach was applied to residents across Brazil between April and July 2024 through a web survey using a semi-structured questionnaire addressing sociodemographic characteristics, engagement, and critiques of the PNAISH. The qualitative analysis employed the Collective Subject Discourse method. A total of 144 individuals participated, primarily young cisgender men, with 80.5% holding postgraduate degrees and 75.7% engaged in male health initiatives. Progress has been observed in the implementation of the PNAISH, particularly in primary care, yet challenges persist regarding policy dissemination and managerial involvement. Most respondents (77.8%) recognized strengths and facilitators in PNAISH, with 43.8% reporting its implementation at both state and municipal levels. Qualitative narratives revealed that participants perceive PNAISH as a strategic opportunity not only to engage men in preventive care but also to foster reflection on masculinities, self-care, and health promotion. Many highlighted that the policy helps to overcome cultural stigmas that traditionally distance men from health services, especially through educational actions and intersectoral strategies. While the policy has advanced access and male participation in health services, structural barriers and limited visibility still constrain its broader impact and effective engagement.
Introduction
The evaluation of public health policies plays a fundamental role in the sustainability of health systems, directly impacting their ability to respond to population needs while shaping organizational, structural, and budgetary aspects. In Brazil, such assessment is crucial to guide investments and promote equity in access and quality of care, especially within the Unified Health System (SUS) (Machado, 2024; Machado Martins et al., 2023).
Historically, men's health has received less attention in public health agendas, often focusing on chronic diseases and maternal and child health. This neglect has led to concerning rates of preventable morbidity and mortality among men, particularly adults (Baker et al., 2023; Dolgalev et al., 2023). Furthermore, cultural norms of masculinity further discourage men from seeking care, contributing to delayed diagnoses and increased vulnerability to treatable conditions (Baker et al., 2023).
In this context, the National Policy for Comprehensive Men’s Health Care (Política Nacional de Atenção Integral à Saúde do Homem—PNAISH) was established in 2009, to expand access and ensure comprehensive care for men, particularly those aged 20 to 59. The policy considers intersections between health, gender, and masculinity and aims to reorganize services to meet men’s specific needs (Brasil, 2008, 2021).
Since its inception, PNAISH has faced structural and organizational challenges—such as men’s limited engagement in preventive care, insufficient training of health professionals, and fragmented services—combined with restricted investment and an emphasis on secondary prevention. While efforts such as public awareness campaigns and screenings have improved access, deeper evaluations are still needed to understand the policy’s broader impact (Brasil, 2021; Lima & Schwarz, 2018).
Although several studies and technical documents have addressed the status of men’s health and the implementation of PNAISH (Brasil, 2018a, 2018b, 2023; Gomes et al., 2016; Moura, 2012), few have adopted a process evaluation methodology capable of proposing knowledge translation strategies aimed at strengthening public health policies for men in Brazil. This gap underscores the relevance of the present study.
Fifteen years after the policy’s establishment, it is necessary to assess its strengths, opportunities, and facilitators, while also recognizing ongoing challenges and proposing improvements that can guide future efforts (Brasil, 2008, 2021). This study aims to assess the strengths, opportunities, and facilitators in PNAISH’s implementation, investigating its influence on early detection and diagnosis of men’s health conditions, while highlighting progress, challenges, and gaps in the care process.
Methods
This study employed a mixed-methods approach with national coverage, involving participants from all Brazilian states and the Federal District. The design followed the framework proposed by Creswell and Clark (2013), adopting a concurrent embedded strategy with greater emphasis on the qualitative strand. In this configuration, qualitative data guided the interpretation and integration of findings.
Data collection occurred between April and July 2024, using a virtual survey due to the territorial extension of Brazil and logistical barriers to face-to-face access. The online strategy allowed a broader geographic reach and diverse participant engagement. The study adhered to quality standards for mixed-methods research, including the Good Reporting of A Mixed Methods Study checklist (O’Cathain et al., 2008) and the Mixed Methods Appraisal Tool (Hong et al., 2019).
Eligible participants were individuals aged 18 or older (N = 144), from different professional and social backgrounds, with some degree of involvement in men’s health or the Brazilian Unified Health System (SUS). Inclusion criteria focused on a diversity of perspectives—users, healthcare professionals, managers, and activists—while ensuring participants had some familiarity with the policy. Responses with incomplete or inconsistent data were excluded.
The web survey was hosted on the Google Forms® platform, selected for its ease of use and compliance with best practices for online research (Passmore et al., 2002). The data collection protocol was previously pilot-tested internally (research team) and externally (potential participants) to assess the clarity of questions, the average response time, and the suitability of the instrument for the target population. The instrument included semi-structured items comprising blocks on sociodemographic characteristics, open-ended questions aligned with study objectives, and closed-ended questions to complement qualitative exploration.
Participants were recruited through key informant chains, public database access, digital platforms (Facebook®, Instagram®, and WhatsApp®), institutions, and organized social movements or advocacy groups—based on strategies established in the literature (Santos et al., 2024; Sousa et al., 2020a). Snowball sampling was applied as an exploratory theoretical approach using chain referral (Biernacki & Waldorf, 1981). The initial network was composed of professionals, researchers, and activists in men’s health. This method was employed as a non-probabilistic recruitment technique suitable for populations with limited visibility or access through conventional sampling frames. In this process, initial participants—selected based on predefined inclusion criteria—were invited to refer other potential participants from their professional or social networks. This chain-referral process allowed the sample to grow organically, helping to reach individuals with experience or interest in men’s health and PNAISH. While effective for expanding access, this method may have introduced sampling bias due to digital exclusion and the overrepresentation of highly educated individuals.
Security measures were implemented to ensure data protection and confidentiality, including the use of pseudonyms, encrypted storage, and restricted access to the research team.
Quantitative variables used to describe the sample included: sex/gender, age, region, race/color, education level, employment status, marital status, parenthood, and type of healthcare system accessed. To evaluate contact with and participation in men’s health and PNAISH-related activities, self-reported variables included: the male population served; years of experience in men’s health; and involvement in PNAISH activities, such as participation in 2009 and 2021 public consultations and ordinance reformulation processes. Other variables examined participation in specific PNAISH actions, recognition of policy strengths, opportunities, and facilitators with PNAISH implantation at municipal or state levels. Membership in men's health support groups was also assessed, including involvement in political advocacy networks, non-governmental organizations (NGOs) governmental institutions, research network collectives, or other support structures. Engagement in PNAISH’s thematic axes was evaluated, including access and welcoming; fatherhood and care; violence and accident prevention; sexual and reproductive health; and main health conditions/chronic diseases.
An open-ended guiding question was used to collect qualitative data: “What strengths, opportunities, and facilitators do you recognize following PNAISH’s implementation in your city and health services?”
For the quantitative part, simple statistical analysis was employed, considering the descriptive and cross-sectional nature of the study (Lefevre & Lefevre, 2012). Data were analyzed using IBM SPSS software (version 19.0 for Windows; IBM Corp., Armonk, NY, USA), with quantitative variables presented as measures of central tendency and dispersion, and categorical variables as absolute and relative frequencies. Inferential statistics were not applied, as preliminary bivariate tests showed no significant associations, and the non-probabilistic nature of the sample does not support the use of p-values or generalizations.
For qualitative analysis, the CSD technique was adopted.²⁰ Participant responses were imported into Microsoft Word 2019® and analyzed using CSD steps, which include identifying key expressions and central ideas to construct synthetic discourses representing collective perspectives. The coding was conducted manually by the research team, based on the methodological protocol of CSD, through successive readings, extraction of key expressions, and classification by central ideas and anchors. This method facilitated an interpretative and representative analysis of participant narratives.
The two datasets (quantitative and qualitative) were developed and analyzed independently and later integrated using a parallel convergence strategy (Paranhos et al., 2016; Santos et al., 2017). Convergences and divergences were identified and synthesized in tables that enabled comparison and joint interpretation. The policy’s normative and theoretical framework was used to support the interpretation of findings, in alignment with Brazil’s current policy directives (Brasil, 2021).
Artificial intelligence tools were used solely for language editing, translation support, and the creation of infographic images; all scientific analyses were conducted by the research team and subsequently reviewed by human editors. Microsoft Excel® was used to generate descriptive charts and graphs for quantitative data presentation. Interpretative notes were added below each figure to enhance comprehension and contextualize visual representations of the findings.
This study adhered to Resolution No. 466, dated December 12, 2012, issued by the National Health Council (Conselho Nacional de Saúde), for conducting research involving human subjects. All participants provided informed consent by signing the Informed Consent Form (Termo de Consentimento Livre e Esclarecido—TCLE). [Information regarding ethical approval has been removed from this manuscript solely for study evaluation]
Results
This section presents the findings of both quantitative and qualitative analyses, structured around three axes: (a) sociodemographic and regional profile; (b) involvement in men’s health actions and PNAISH implementation; and (c) perceptions of strengths, opportunities, and challenges, as well as data integration through the CSD technique.
Sociodemographic and Regional Profile of Participants (QUAN)
Among the 144 participants, 45.8% (66) identified as cisgender men, while 42.4% (61) as cisgender women. Most participants were young adults (41.0%; 59) or middle-aged adults (37.5%; 54), with a mean age of 42.2 years (±9.96). Regarding race/ethnicity, 45.1% (65) self-identified as White and 42.4% (61) as Brown. Most participants resided in the Northeast (36.8%; 53) and Central-West (20.1%; 29) regions of Brazil. Educational attainment was notably high: 20.8% (30) held a PhD, 25.7% (37) a master’s degree, and 34.0% (49) a specialization certificate. The majority were employed (94.4%; 136) and had children (52.1%; 75). A substantial portion used both public and private health services (54.2%; 78) (Figure 1).
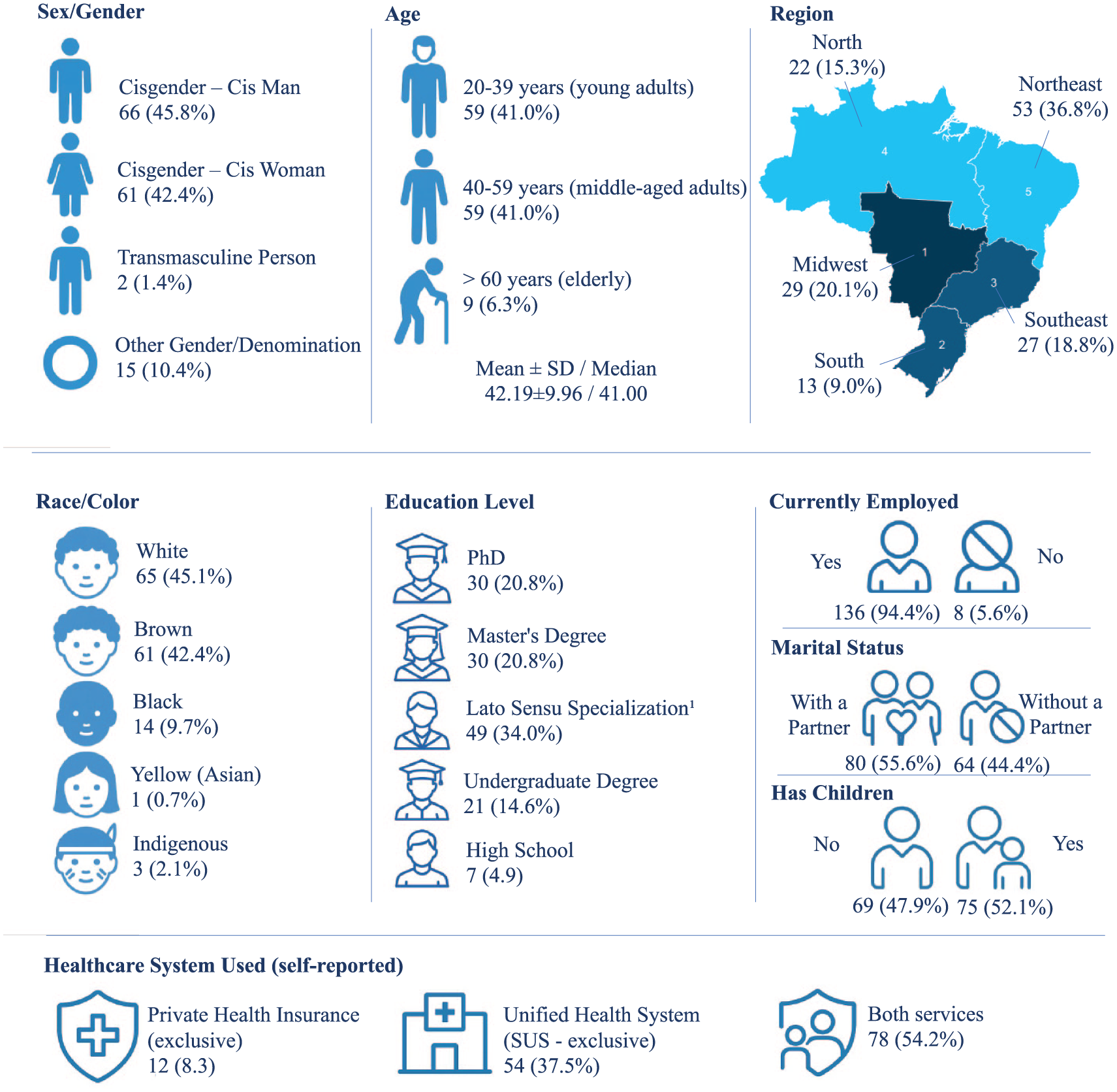
Demographic, Social, and Regional Characterization of the Study Sample
Interpretative note: These data indicate that most participants were highly educated professionals from urban areas, which may reflect selective engagement in PNAISH initiatives.
Involvement with PNAISH: Actions, Perceptions, and Implementation (QUAN)
Most participants (61.1%; 88) reported working primarily with the urban male population, while 31.3% (45) had contact with both urban and rural groups. Regarding professional experience in the field, 32.6% (47) had been involved in men’s health for 1 to 5 years. Most respondents (75.7%; 109) reported having participated in some type of man’s health-related initiative (Figure 2).

Distribution of Contact, Participation in Men’s Health Actions, and PNAISH in Brazil (N = 144). Salvador, Bahia, Brazil
A significant portion, 77.8% (112), recognized strengths, opportunities, or facilitators related to the PNAISH in their municipalities or healthcare services. As for policy implementation, 43.8% (63) indicated that PNAISH was active at both the state and municipal levels, while 19.4% (28) reported implementation only at the municipal level (Figure 2).
Interpretative note: The majority of participants had direct involvement with urban male populations and reported working in men’s health for up to 5 years, highlighting recent and localized engagement with PNAISH.
Participation in PNAISH-related initiatives was limited, with only (33.3%; 48) of respondents reporting involvement in policy-driven actions, while 66.7% (96) indicated no participation. Among those engaged, 17.4% (25) contributed to the 2021 public consultation, and 11.1% (16) participated in the policy ordinance update process that same year (Figure 3).
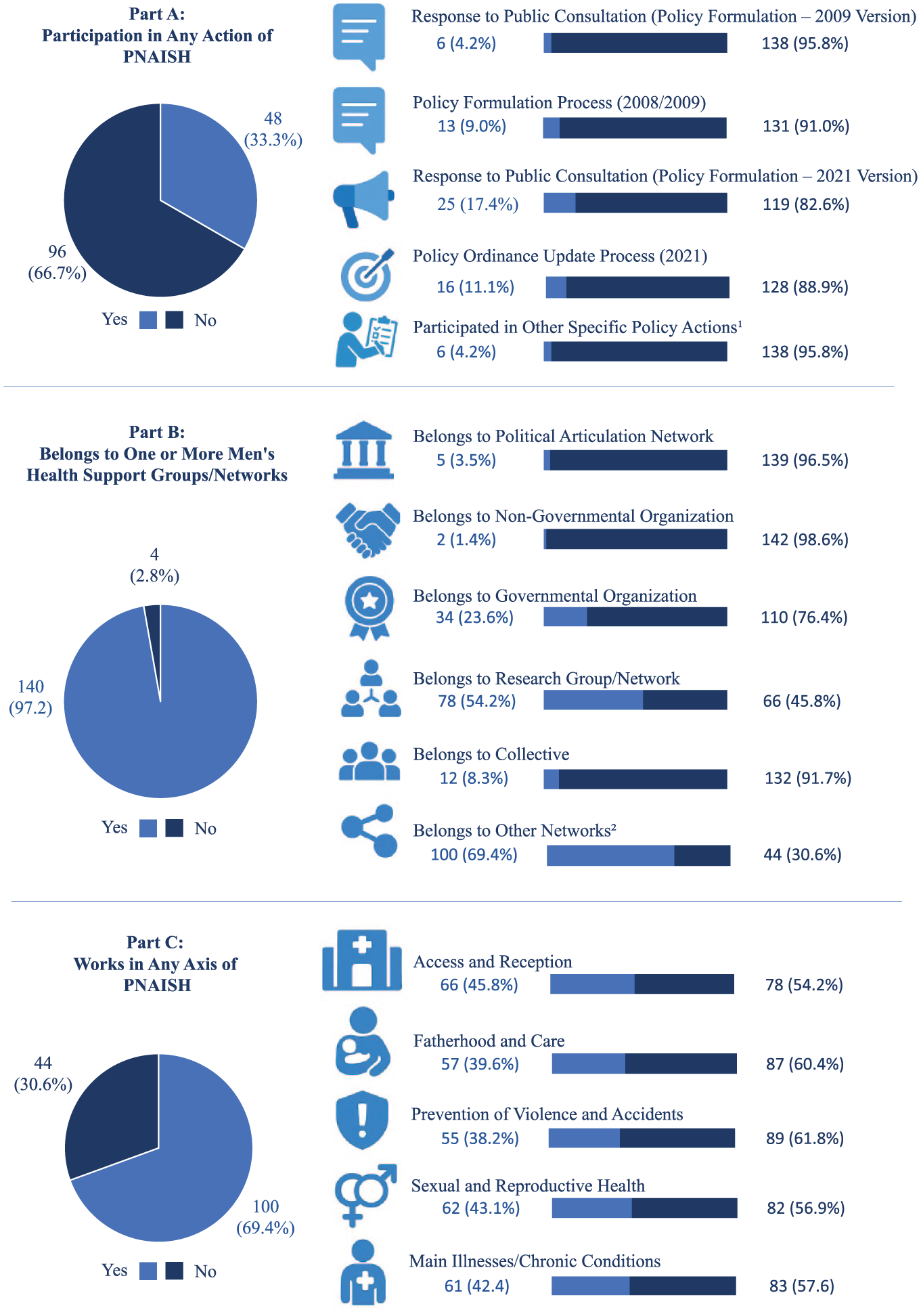
Participation in Actions in PNAISH (Part A), Belonging to One or More Men’s Health Support Groups/Networks (Part B), and Work in Any Axis of PNAISH in Brazil (Part C) (N = 144)
Despite the low level of direct policy engagement, most participants (97.2%; 122) reported belonging to at least one health support group or network. Of these, 54.2% (78) were affiliated with research groups or academic collectives, and 61.3% (88) indicated participation in other forms of organized engagement (Figure 3).
Regarding involvement in PNAISH’s strategic axes, 69.4% (100) reported working in at least one. The most frequently cited areas were Access and Reception (45.8%; 66), Sexual and Reproductive Health (43.1%; 62), and Chronic Diseases (42.4%; 61; Figure 3).
Interpretative note: Although formal participation in PNAISH policy development remains low, the data reveal high levels of engagement in support networks and strategic axes, particularly among individuals linked to research and service delivery. This suggests that practical implementation is being driven by decentralized, professional, and academic efforts, even in the absence of structured governmental articulation.
Perceptions of Strengths, Opportunities, and Implementation Challenges (Qualitative and Mixed Integration)
Quantitative data indicated that PNAISH implementation varies according to sociodemographic characteristics, influencing perceptions of the policy, its territorial reach, and local initiatives. Participants reported involvement mainly through educational activities, health campaigns, and discussions on masculinity in services, schools, and communities (Framework 1).
Distribution of Variables Derived from QUAN Data and Key Expressions from QUAL Participants on the Strengths, Opportunities, or Facilities of PNAISH in Brazil (N = 144). Salvador, Bahia, Brazil.
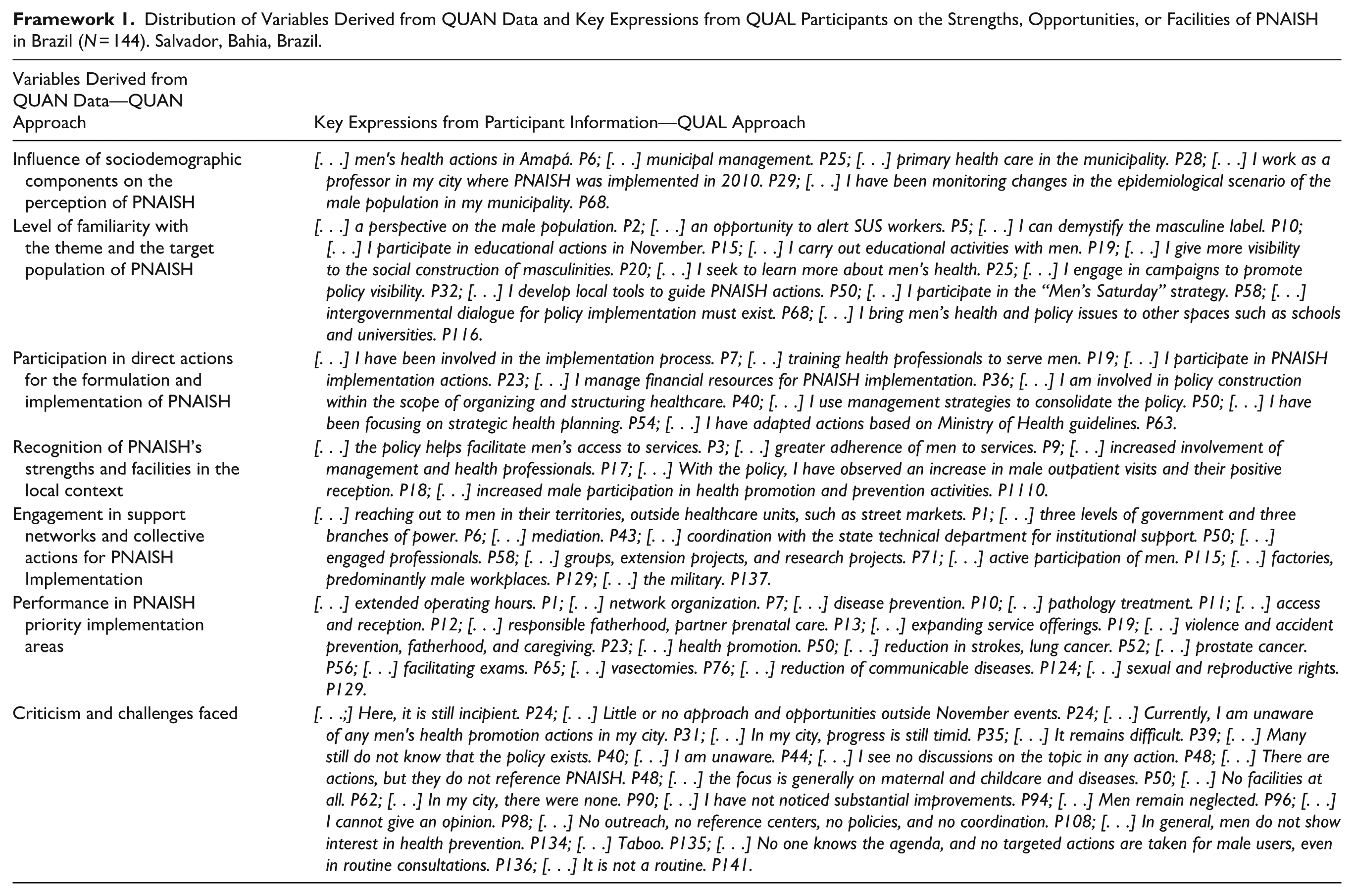
Qualitative data deepened this understanding, revealing engagement in professional training, resource management, health network organization, and the application of ministerial guidelines. Respondents identified facilitators such as improved male access, greater adherence to care, and increased support from managers and professionals. Yet, implementation remains uneven, with persistent challenges and criticisms (Framework 1).
Interpretative note: Framework 1 illustrates the convergence between sociodemographic engagement patterns and participants’ discourses on the perceived value and expansion of PNAISH initiatives at the local level.
The integration of quantitative and qualitative data highlighted key strengths, opportunities, and facilitators of PNAISH implementation over the past 15 years. Based on quantitative findings, six core themes were identified and explored through CSD aligned with PNAISH’s principles.
Quantitative results showed that most men served by health initiatives live in urban areas, and professionals working in men’s health commonly have between 1 and 5 years of experience. Qualitative findings emphasize the need to strengthen bonds between services and men, with educational initiatives like “Blue November” and “Men’s Health Saturdays” cited as key strategies. Training and promotion of self-care were also seen as central to success (Framework 2).
Integration of quantitative and qualitative results regarding the strengths, opportunities, and facilitators of the implementation of PNAISH in Brazil (N=141). Salvador, Bahia, Brazil.
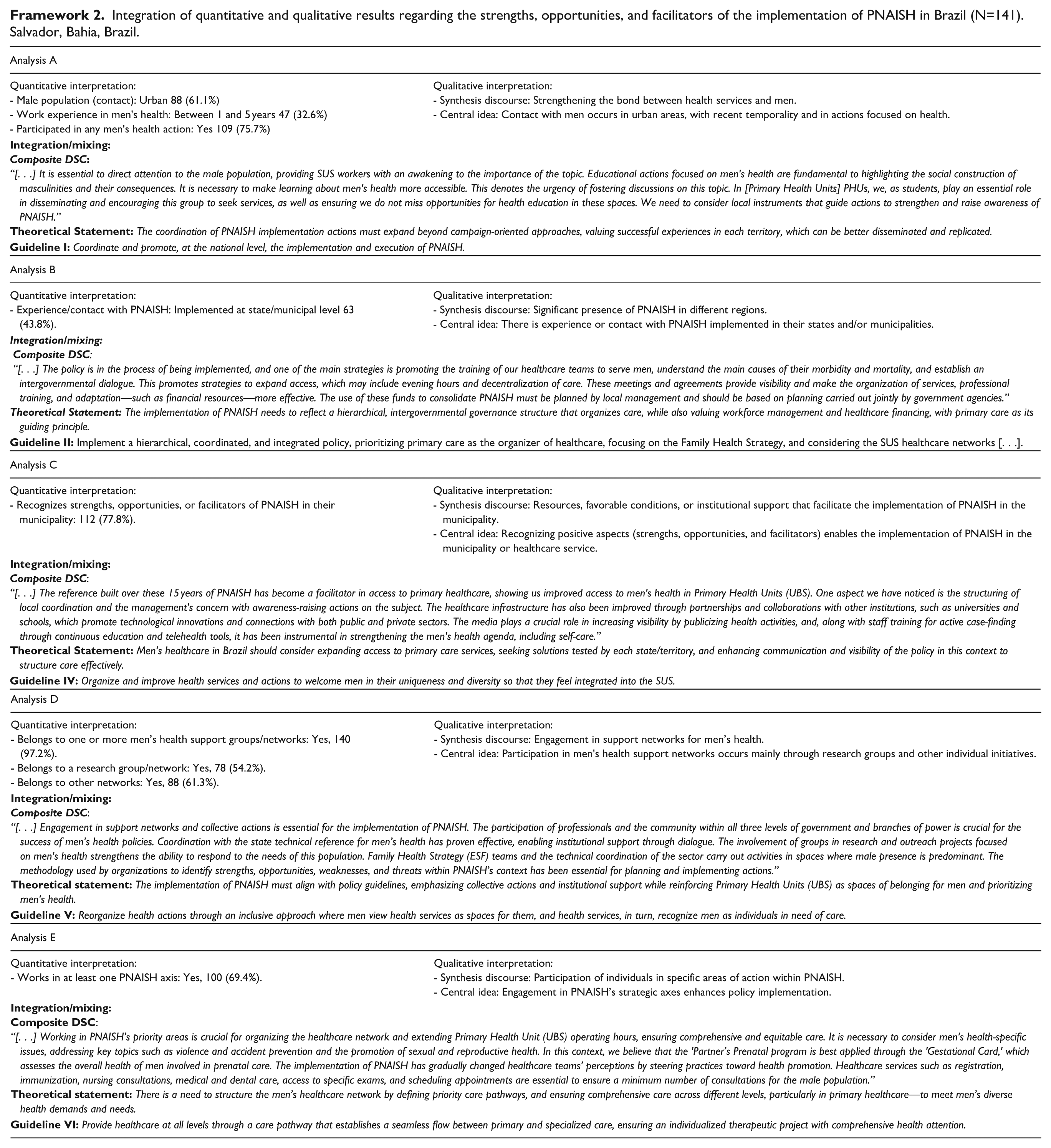
Participants acknowledged improved access and reception in primary care, with expanded service hours and more specialized care, increasing user acceptance. Statements confirmed that PNAISH is in ongoing implementation, supported by training efforts and visibility campaigns (Framework 2).
Most respondents were part of men’s health networks, often combining research and practice. PNAISH was viewed as a pioneering policy using outreach and intergovernmental coordination to meet men’s specific needs. Engagement in strategic axes—especially fatherhood, reception, and chronic disease care—was seen as essential for building equitable, responsive health services (Framework 2).
Interpretative note: Framework 2 illustrates that PNAISH implementation is driven by local actions and professional engagement, even in the absence of strong institutional coordination, revealing opportunities for scaling successful practices.
PNAISH implementation continues to face criticisms and challenges. Quantitative data highlight low participation in its initiatives, while qualitative findings reveal that man’s health promotion remains limited—often restricted to symbolic campaigns “Blue November.” In many areas, actions are still incipient, poorly disseminated, and lack coordination among health services, reinforcing a sense of neglect among the male population (Framework 3).
Integration of Quantitative and Qualitative Results Regarding Criticisms and Challenges Faced in the Implementation of PNAISH in Brazil (N = 141). Salvador, Bahia, Brazil.
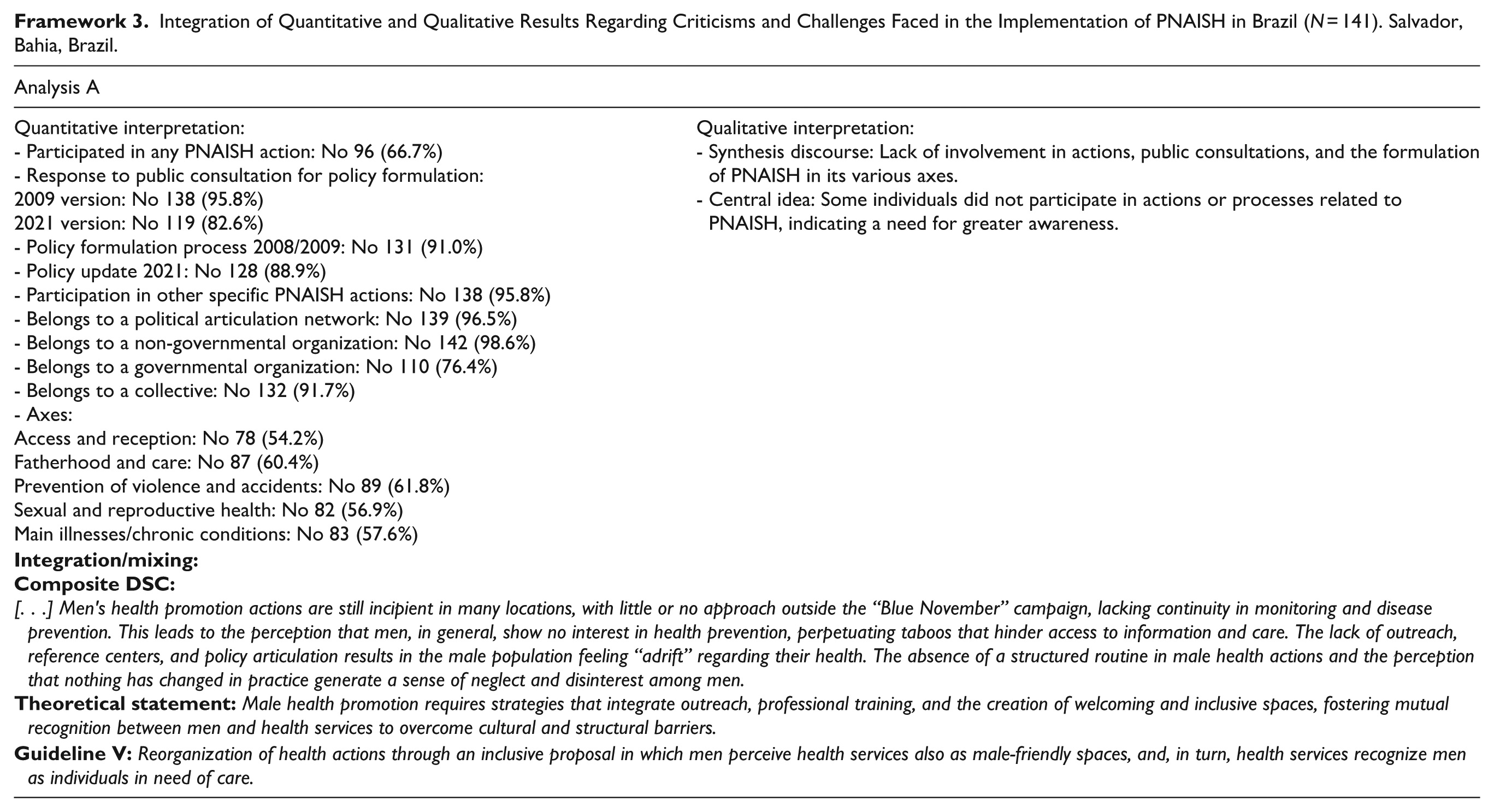
Participants described systemic barriers, including long waiting times in the public system and fragmented care in the private sector. These issues contribute to the perception that men are disengaged from health services, while the lack of targeted, continuous, and structured initiatives limits their participation (Framework 3).
Interpretative note: The data synthesized in Framework 3 reveal critical gaps in policy engagement and execution, especially in terms of participation, continuity, and service organization. These challenges underscore the urgency of strengthening institutional commitment and expanding men’s health initiatives beyond isolated campaigns.
Discussion
The findings of this study revealed a predominance of cisgender men (45.8%) among participants, pointing to the need for more inclusive public health policies that address gender diversity. Most respondents were young adults (41.0% aged 20–39), a group with specific health needs that remain under-addressed. Recognizing these demographic patterns is key to designing responsive, targeted strategies (Szabo et al., 2020).
The high representation of White (45.1%) and Black (42.4%) individuals underscores the importance of addressing racial disparities in healthcare. Race is a known determinant of health service use and perception, often linked to structural inequalities and socioeconomic conditions (Ogungbe et al., 2024; Xiao et al., 2024). PNAISH should consider these disparities more explicitly and promote equity-based strategies in its planning.
With 36.8% of participants residing in the Northeast region, regional inequalities become apparent. This region faces chronic underinvestment and reduced healthcare infrastructure, which can limit the implementation of national policies (Alcântara et al., 2020; Coelho et al., 2023). For the successful implementation of PNAISH, it is necessary to identify these regional particularities and tailor intervention strategies to more effectively address local needs, fostering a more accessible and responsive healthcare system.
The elevated level of education among participants—20.8% with doctoral degrees and 34.0% with specialization—suggests a profile inclined toward engagement with health initiatives. However, as previous studies show, educational level does not guarantee participation (Campmans et al., 2023). The high proportion of employed individuals (94.4%) indicates strong workforce participation, which could facilitate involvement in health programs. However, it also highlights the necessity for health policies to be adapted to the routines and professional environments of these individuals (Campmans et al., 2023).
Urban-centric engagement 61.1% signals an implementation gap in rural areas, where access to care is often more limited. Including rural populations in PNAISH's scope is essential to ensure equitable care and prevent the deepening of existing vulnerabilities (Basu, 2022; Shen et al., 2023).
In recent years, the digitization of healthcare systems, including electronic medical records and telehealth, has facilitated patient monitoring and continuity of care. During the COVID-19 pandemic, telemedicine experienced significant growth, expanding men’s access to healthcare services, particularly in remote areas or where cultural and socioeconomic barriers hindered in-person consultations (Ezeamii et al., 2024). PNAISH's incorporation of telehealth and digital communication platforms has supported continuity of care and broadened male engagement (Balcombe & De Leo, 2022; Lima et al., 2024).
The findings indicate that participants’ perceptions of PNAISH and its effectiveness are shaped by their professional experience, with 75.7% having previously participated in initiatives related to men’s health. This suggests that prior participation enhances connection with health policies and reinforces the importance of permanent education and training (Hahn & Truman, 2015; Silva & Alves, 2024; Sousa et al., 2020b).
The implementation of PNAISH has fostered strategic partnerships with NGOs and social movements, which have brought forward issues such as mental health, responsible fatherhood, drug use prevention, and domestic violence. These collaborations have expanded the policy scope and encouraged a more humanized, less stigmatized approach to men’s healthcare. Joint efforts between government, civil society, and local actors have helped identify and address specific vulnerabilities affecting men (Sousa et al., 2020b; Smith et al., 2016).
The execution of PNAISH at different levels—43.8% at the state level and 19.4% at the municipal level—reflects progress in its dissemination and implementation. However, low engagement in specific actions (33.3%) exposes a significant gap. This limited participation suggests that initiatives remain sporadic and poorly publicized. PNAISH must overcome the perception of being a seasonal campaign and become a permanent part of public health, addressing men’s health comprehensively beyond prostate cancer prevention.
Increasing the frequency and diversity of PNAISH actions, along with effective communication, is essential to advancing its goals. The lack of continuity and visibility underscores the need for broader campaigns that engage both men and healthcare professionals, raising awareness about comprehensive and ongoing care. These actions should be part of the routine health services, following a more accessible and inclusive approach. Collaboration is crucial to overcoming cultural and structural barriers that limit access (Lima & Schwarz, 2018; Sousa et al., 2020b; Etienne, 2018). Furthermore, continuous professional training and the creation of discussion spaces can enhance acceptance and participation, fostering a more equitable and welcoming healthcare environment (Oliveira et al., 2020; Paranhos et al., 2021).
Evaluation of PNAISH’s thematic axes indicates that most participants work in areas such as Access and Reception (45.8%) and Sexual and Reproductive Health (43.1%), reflecting the centrality of these issues in men’s health. Support networks and study groups can foster experience-sharing and strengthen knowledge of male health needs (Nyalela & Dlungwane, 2024; Shand & Marcell, 2021). These collaborative spaces enable locally adapted interventions and promote innovative practices that enhance participation and address the complexity of men’s health (Shand & Marcell, 2021).
The mixed-methods approach enabled a comprehensive understanding of PNAISH’s implementation. While quantitative data revealed trends and patterns, qualitative findings provided insights into participants’ experiences and perceptions. Integrating both strands is essential to inform evidence-based practices that genuinely address men’s health needs.
The qualitative findings emphasize the need to train healthcare professionals to promote clearer and more accessible dialogue in primary care. Proper training enables providers to act as facilitators of men’s health and highlights the value of continuous education, especially on topics like masculinity and self-care (Etienne, 2018; Lima & Schwarz, 2018; Sousa et al., 2020b). These themes help address men's health needs more sensitively, demystifying care and fostering trust between professionals and patients—essential for adherence and engagement. Thus, ongoing training is a key strategy for the success of PNAISH, supporting a more cohesive and responsive approach.
Despite ongoing challenges in Brazil’s primary healthcare system, PNAISH has, over 15 years, helped consolidate strategies centered on primary care. This has expanded men’s access to prevention and health promotion services—areas long underutilized. The policy has played a crucial role in challenging the notion that men’s health is limited to severe illnesses or emergencies, broadening the scope to include prevention and continuous care (Sousa et al., 2020b).
The experiences of “Blue November” and “Men’s Saturday” have emerged as key strategies for promoting men’s health. These events raise awareness but must be expanded through ongoing, year-round actions. Ongoing promotion is vital to ensuring that men’s health remains a permanent part of the public health agenda, rather than being confined to commemorative dates. This integrated approach contributes to demystifying men’s health topics, encouraging men to seek guidance and actively participate in their healthcare. The persistence and expansion of these initiatives are crucial for reshaping perceptions of men’s health and building a more inclusive and equitable healthcare system (Baker, 2022; Etienne, 2018; Sousa et al., 2020b).
The perception of obstacles during PNAISH’s implementation highlights the need for continuous monitoring and adaptation to local realities. Constant evaluation and adaptability of strategies are essential for the policy’s success, ensuring that interventions remain effective and relevant (Sousa et al., 2020b). Furthermore, flexibility in strategies is crucial for quickly responding to shifts in men’s healthcare needs, ensuring that PNAISH remains practical and relevant for men in various social and community contexts.
Participants’ feedback underscores the urgent need to boost awareness and male engagement in PNAISH. A lack of communication and coordination across services remains a barrier to making men feel welcome in care settings (Sousa et al., 2020b). To address these challenges, educational campaigns are essential. They should not only provide information about PNAISH but also create an environment that encourages men’s active participation, fostering a sense of belonging and responsibility for their health. The use of social media, partnerships with community organizations, and in-person events can enhance the impact of these initiatives, making PNAISH a fundamental and constant component of public health.
The limitations of this study stem from the use of pre-existing contact networks and the snowball sampling method for data collection, which may have resulted in a concentration of participants with similar profiles to those in the networks through which the study circulated, potentially introducing selection bias. Additionally, the online survey format may have excluded individuals with limited digital access or literacy, restricting the diversity of perspectives captured. As a result, the findings may not be generalizable to the broader male population in Brazil. The sample’s high educational level and prior engagement with the topic may also have influenced responses, particularly in favor of PNAISH initiatives.
Finally, this research makes significant contributions to the advancement of scientific knowledge by providing original insights into the provision of care and men’s health services within the scope of PNAISH. It highlights key elements that impact men’s health in Brazil, laying the foundation for future research on care strategies and improvements in healthcare services for this population across different social and political contexts.
Conclusions
This study reveals a multifaceted scenario in which the strengths, opportunities, and challenges of PNAISH coexist. The consolidation of this policy depends on the active involvement of healthcare professionals, administrators, and the population itself. Shared responsibility is essential for building a more equitable and responsive healthcare system for Brazilian men.
While PNAISH has significant potential to transform men’s health, its success requires overcoming persistent barriers—especially limited participation, visibility, and coordination. Strengthening communication strategies, investing in professional training, and integrating initiatives into the daily routine of healthcare services are key to advancing its implementation.
Experiences like “Blue November” illustrate how awareness can be generated, but they must evolve into sustained, year-round actions. Health promotion efforts should address a broader range of issues and be rooted in continuous education and inclusive practices. Ensuring that men are recognized as subjects of care—and not only as targets of specific campaigns—is essential to ensure that the goals of PNAISH are fully achieved.
Footnotes
ORCID iDs
Authors’ Contributions
Barreto NMPV; Araújo JS; Souza AR; Gomes DT; Silva AF; Corrêa ACP; Sousa AFL; De La Rosa RN; Ortega J and Pereira A: made substantial contributions to the acquisition and interpretation of data; wrote the manuscript; contributed to data acquisition and analysis for the study; assisted in the interpretation of the results; contributed to writing and critically revised the manuscript for scientific content.
Souza AR: designed the study and supervised the work; made substantial contributions to data interpretation for manuscript preparation and critically revised it for scientific content.
All authors approved the final version to be published.
Ethical Considerations
The study complied with the recommendations of Resolution No. 466, dated December 12, 2012, issued by the National Research Council (Conselho Nacional de Pesquisa), for conducting research involving human subjects. All individuals who agreed to participate in the study signed the Informed Consent Form (Termo de Consentimento Livre e Esclarecido—TCLE). This research originated from an independent initiative of the Center for Adult Health Care and Technology Studies (Núcleo de Estudos de Cuidado e Tecnologia da Saúde do Adulto—NECTA), under the Research Line: Men's Health Care, Masculinities, and Sexualities, affiliated with the School of Nursing at the Federal University of Bahia (Escola de Enfermagem da Universidade Federal da Bahia—UFBA). The project received support from: the Bahia State Health Secretary (Secretaria Estadual de Saúde da Bahia—SESAB), the Bahia State Research Support Foundation (Fundação de Amparo à Pesquisa do Estado da Bahia—FAPESB), scholarship-funded students, and the Men’s Health Coordination Unit of the Ministry of Health (Coordenação de Saúde do Homem do Ministério da Saúde—CS/MS). This study is part of a larger research project approved by the Research Ethics Committee (Comitê de Ética em Pesquisa—CEP), under: CAAE (Certificate of Ethical Assessment)—76017423.3.0000.5531 and approval Nº: 6,603,953.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by postgraduate research scholarships from the Coordination for the Improvement of Higher Education Personnel (CAPES) and the National Council for Scientific and Technological Development (CNPq).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.