
Abstract
On average, American men live shorter, less healthy lives than women. They are more likely to be the victim of a violent crime, die in a car crash, commit suicide, and be injured at work. In addition, men have higher death rates in 9 of the top 10 causes of death, and are less likely to receive routine preventative care, leaving men with a life span that is significantly shorter than women’s. Recently, policy makers and researchers have been paying more attention to health disparities including race, sex, and ethnicity. However, men are still noticeably absent from these discussions despite being significantly harmed by disparities in preventive care, quality of life, and overall health outcomes. Ignoring these disparities is costly in terms of lost productivity, lives lost, and financial costs incurred by the government and employers each year. Premature death and morbidity in men costs federal, state, and local governments in excess of $142 billion annually. It also costs U.S.employers and society as a whole in excess of $156 billion annually in direct medical payments and lost productivity and an additional $181 billion annually in decreased quality of life. As federal and state governments and the private sector struggle with increasing health entitlement burdens—including escalating health care costs—eliminating male health inequities emerges as an important source of savings. This analysis will examine the economic and intangible costs associated with the health disparities that exist between genders and the benefits reaped if these disparities are reduced or eliminated.
Of all the forms of inequality, injustice in health care is the most shocking and inhumane.
There is no time like the present to begin focusing on the goal of health equity—a goal that is not only consistent with the American promise of opportunity, but in our long-term economic interest, as well.
Over the past two decades, we’ve radically revised how we conduct medical research and take care of our female patients. And we’ve made valuable discoveries about how gender helps determine vulnerability to illness and, ultimately, the timing and causes of death. But I now believe that we doctors and researchers may have focused too much on women. . . . It’s time to focus on the unique problems of men just the way we have learned to do with women.
Introduction
With health reform gathering unprecedented national attention, there could not be a better time to address fundamental health disparities in the United States. In addition, because of the significant human cost, we, as a society, have a clear, moral imperative to reduce or eliminate those disparities. Unfortunately, the “social justice” argument—that saving men’s lives is simply the right thing to do—is not always enough to get people to act. Sometimes it is necessary to demonstrate that there are financial incentives for doing the right thing, in other words, a “business case.”
Research from the Institute for Healthcare Improvement defines a business case as the financial return (profit, reduction in losses for a given program or population, or avoided costs) or other positive direct or indirect effects realized by an entity that invests in a health care improvement intervention (Leatherman et al., 2003). The federal government serves as a perfect example of a business case because of the important role it plays in addressing health disparities through its constitutional responsibility to promote general welfare. Recognition as the only entity that can adopt a lifetime perspective on prevention and chronic conditions further underscores the significance of its preservation (Bovbjerg, Hatry, & Morley, 2009). However, recent cost projections of federal entitlement programs such as Social Security, Medicare, and Medicaid reveal that current spending levels are unsustainable over the long term. Barring drastic reductions in public program benefits, closing the deficit gap will require significant cost cutting.
The following analysis provides a compelling business case for a concentrated focus on reducing health disparities in men. As the authors of this analysis will show, these disparities impose enormous costs on society, both in economic and well-being terms. Addressing the health disparities that exist between males and females could result in substantial financial benefits and an overall improvement in quality of life for all Americans. We will estimate the financial benefit that might accrue to individuals, businesses, and the national economy if men had health outcomes similar to those of women.
The Nature and Scope of the Men’s Health Disparity and Health Outcome Data
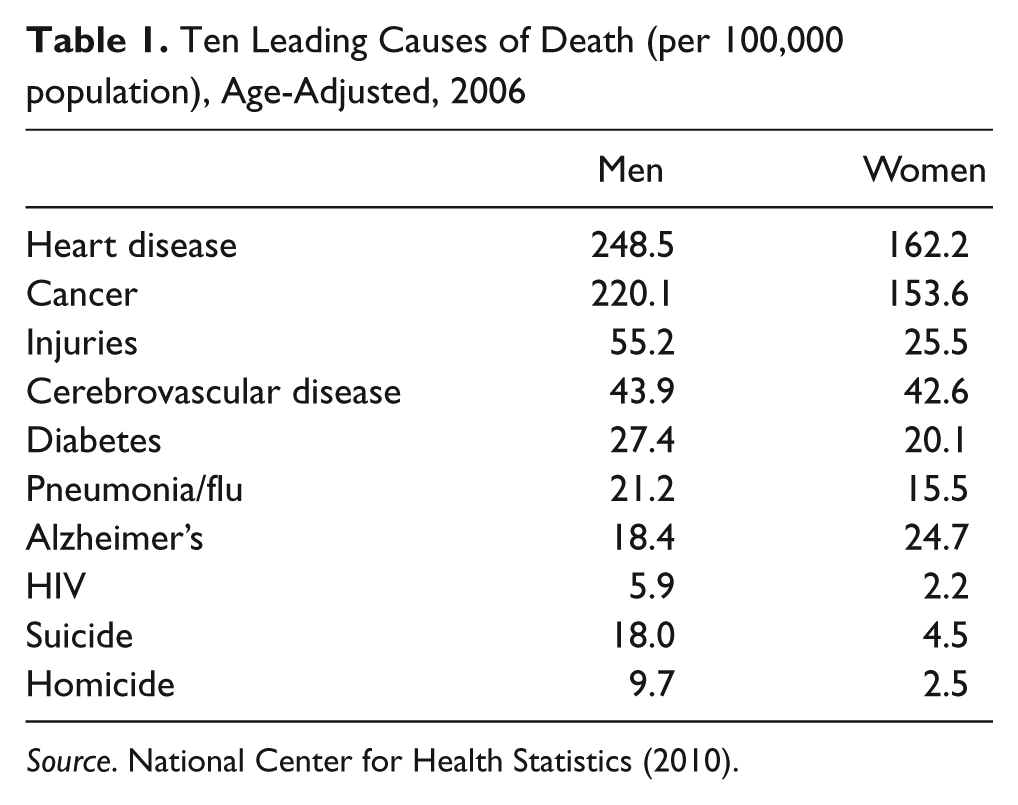
In 1900, women outlived men on average by 2 years. By 1970, that gap had widened to 7 years (see Figure 1). As of 2009, life expectancy for men was 75.7 years compared with 80.6 years for women (Miniño et al., 2011). Men have a higher death rate for 9 of the 10 leading causes of death (see Table 1), and these outcomes become even more pronounced when broken down by race and ethnicity (Sutocky, 2004). According to the U.S. Preventative Task Force (as cited in Courtenay, 2003), at least half of men’s deaths each year in the United States (approximately 600,000 out of a total of 1.2 million male deaths) could be prevented through changes in personal health habits.

Life expectancy at birth by sex: United States, selected years 1900-2007
Ten Leading Causes of Death (per 100,000 population), Age-Adjusted, 2006
There are a number of factors that contribute to men’s shorter life expectancy:
Testosterone. Presence of the hormone testosterone in men is considered by many to be an important contributing factor to men’s elevated risk of cardiovascular disease and stroke. Testosterone is also linked with aggressive and risky behavior, which results in unnecessary fatal and nonfatal injuries (Booth, Johnson, & Granger, 1999).
Socialization. Strongly held beliefs about what it means to be a man have a significant impact on men’s health. “Men are socialized to project strength, individuality, autonomy, dominance, stoicism, and physical aggression, and to avoid demonstrations of emotion or vulnerability that could be construed as weakness. These cultural orientations and structural opportunities combine to increase health risks” (Williams, 2003, p. 726).
Lifestyle choices. Men are also significantly more likely than women to make risky behavioral and lifestyle choices. More men than women smoke (20.7% vs. 16.2%), are overweight (69% vs. 52.2%), binge drink (31% vs. 15%), and use illegal drugs (10% vs. 6%; Williams, 2003). Researcher Williams (2003) identified a number of ways that men’s alcohol and substance abuse negatively affect them, their families, and society. Alcohol, for example, is a significant contributor to suicide, cirrhosis, homicide, and traffic fatalities. Drug use increases risk of car accidents and of contracting HIV/AIDS and hepatitis. Substance abuse is a major financial drain on families and contributes to divorce, family violence, unemployment, psychological problems, and crime. Half of those arrested for or convicted of major crimes, including murder and assault, were under the influence of drugs or alcohol either at the time of their arrest or at the time the crimes were committed (Williams, 2003).
Lack of health care engagement. Dr. Jean Bonhomme (2007), an expert on men’s health issues, points out that women are 100% more likely to obtain preventive care from a physician—even after excluding pregnancy-related visits—when compared with men. In addition, 33% of men (vs. 19% of women) have no regular physician. Twenty-five percent of men (vs. 8% of women) have not seen a doctor in the past year. Only one in five men says that if he were sick or in pain, he would promptly seek medical attention. In addition, nearly 25% of men said that if sick or in pain, they would put off getting medical help as long as possible (Bonhomme, 2007). This aversion to seeking medical attention puts men at a greater risk of late-stage disease and prolonged morbidity (Men’s Health Network, 2009). Thyroid cancer is an example of how this works. According to the American Cancer Society (2011), there will be approximately 48,020 new cases of thyroid cancer in the United States in 2011. Of these new cases, about 36,550 will occur in women and about 11,470 will occur in men. It is virtually the only non-gender specific cancer, other than breast cancer, where incidence rates are higher in women than in men. However, 980 women and 760 men will die of thyroid cancer in 2011. Even though women are more than three times more likely to develop thyroid cancer, they are only about 30% more likely to die of it. This is because of the fact that men are less likely to seek preventative care: They are “more likely to present for treatment at a later stage in the development of their disease and hence with a worse prognosis” (Forman, 2006). When men do eventually seek medical care, they get fewer services, less health information, less advice, and are less likely to talk about the need to change their behavior to improve health (Williams, 2003).
The workplace. Men are often employed in more hazardous occupations than women and account for more than 90% of workplace injuries and fatalities (Courtenay, 2000). Occupational diseases are responsible for approximately 860,000 illnesses and 60,300 deaths in the United States each year (Lax, Grant, Manetti, & Klein, 1998).
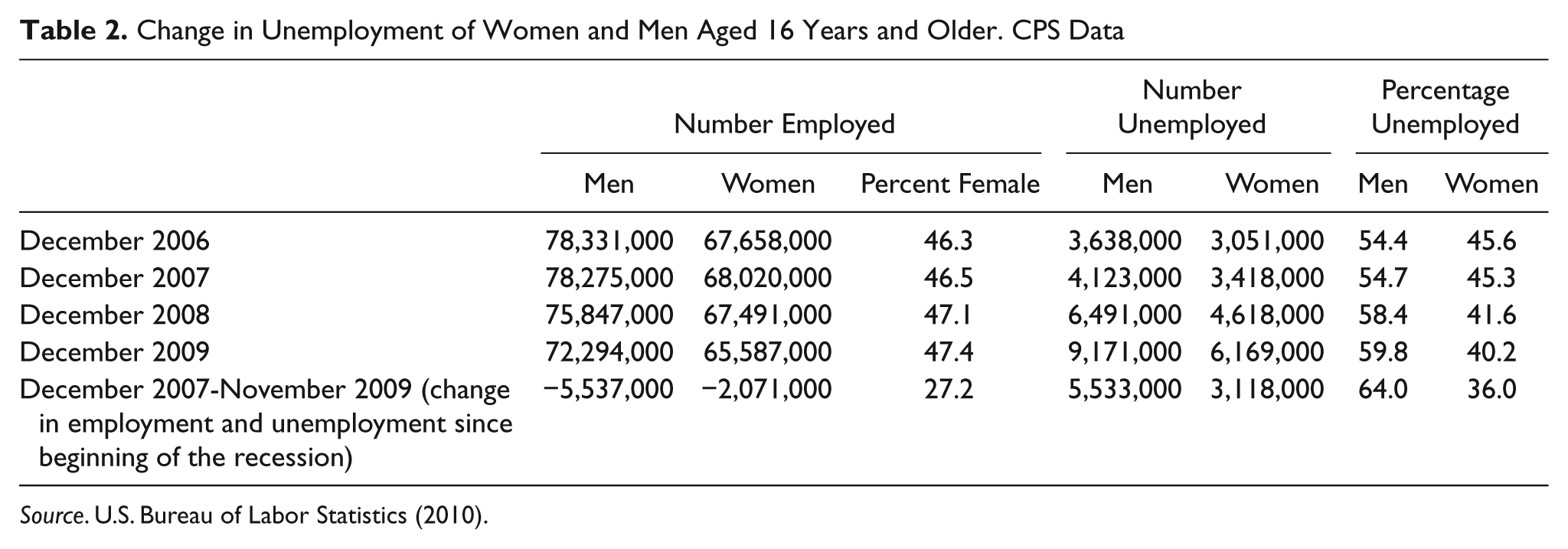
Unemployment. Since 2006, men’s share of the unemployed has risen from 54% to 64% in 2009 (see Table 2). One recent study reported a strong connection between unemployment and increased health risks, including depression, alcohol and substance abuse, lack of exercise, and suicide. “Job loss because of an establishment closure increases the odds of reporting fair or poor health by 54%” (Strully, 2009, p. 233). Compared with those who were continually employed, unemployed workers were also twice as likely to develop a new condition, such as diabetes, high blood pressure, or heart disease (Strully, 2009).
Lack of health insurance. Of the 38.4 million Americans aged 18 to 64 years who lack health insurance, 55% (21.2 million) are men. Of those aged 18 to 34 years, 57.4% of the uninsured are men (Institute for Women’s Policy Research, 2010). People without health insurance have poorer overall health and a higher mortality rate than those with insurance (Kaiser Family Foundation, 2010b). In 2010, a study done by the Centers for Disease Control and Prevention (CDC) reported that uninsured adults with chronic medical problems were three times more likely to skip medical care, compared with those with insurance. In addition, more than 40% of people without insurance who suffer from diabetes, high blood pressure, or asthma skipped getting care because of costs. An American Cancer Society study also reported that people diagnosed with cancer who don’t have health insurance are more likely to die because they are less likely to get screening tests and so are typically diagnosed with advanced disease (Ward et al., 2008).
Research and clinical trials. Contrary to conventional thought, men are underrepresented in clinical trials and research. According to the U.S. Department of Health and Human Services (HHS), National Institutes of Health (NIH) Office of Women’s Health (2009), between 1995 and 2008, women outnumbered men in extramural and intramural clinical research every year. Female enrollment percentage ranged from a low of 51.7% in 1994 to 64.2% in 2002. In 2007, of the 10,914 NIH-funded protocols with human subjects, 1,340 protocols (8.6%) were female only; 517 (3.3%) were male only (U.S. HHS, 2009). Men’s health concerns are also greatly underfunded, particularly when compared with spending on women’s health. A recent report estimated that in 2012, the NIH will spend a total of $3.757 billion on women’s health, including $778 million on breast cancer and $95 million on cervical cancer. In contrast, the NIH is estimated to spend just $337 million on prostate cancer (NIH 2011)—about 43 percent of breast cancer spending—despite the fact that prostate cancer kills nearly as many men every year as breast cancer kills women (National Cancer Institute, 2010). (The American Cancer Society estimates that 33,720 men will die of prostate cancer and 39,520 women will die of breast cancer in 2011).
Change in Unemployment of Women and Men Aged 16 Years and Older. CPS Data
Government Expenditures
Social Security, Medicare, and Medicaid
The social repercussions of men’s poor health are extensive, and the costs to local, state, and federal governments are substantial. Although males have a higher birth rate than females (105 to 100), women outnumber men at every age bracket after age 34 years (U.S Census Bureau 2010). According to the 2000 census, as individuals reach retirement, there are fewer than 85 men for every 100 women. With an anticipated increase of nearly 25 million Medicare enrollees over the next 20 years because of an aging baby-boom population, the U.S. Social Security Administration (2011) projects that its Trust Fund Reserves will be exhausted in 2037.
In 2009, the combined cost of the Social Security and Medicare programs equaled 8.4% of gross domestic product (GDP; 2009 Total GDP equaled $14,003 trillion), which translates to approximately $1.176 trillion (U.S. Social Security Administration, 2009). Social Security’s cost amounted to 4.8% of GDP in 2009 and is projected to increase to 6.0% of GDP by 2084. Medicare’s cost was smaller in 2009—3.5% of GDP—but is projected to surpass the cost of Social Security in 2049. In 2084, the combined cost of the programs would represent 12.4% of GDP (U.S. Social Security Administration, 2009, 2011).
Because men who enter Medicare are in worse health than women, addressing men’s health issues could play a major role in reducing Medicare expenses and the Social Security Trust Fund deficit.
Caring for the Uninsured
Much of the health care administered to the uninsured in hospitals goes uncompensated, and these costs shift to both the public and private sectors. According to the Institute of Medicine (IOM), federal, state, and local governments spend approximately $30 billion per year “to compensate hospitals and clinics for services provided to the uninsured” (IOM, 2004).
However, the IOM (2004) also reports that
the costs to society of having a large uninsured population are not primarily due to the costs of providing health services free of charge to those without coverage. Most of the cost is in the form of poorer health for the uninsured because they frequently receive too little care, too late.
The total benefit to taxpayers of insuring the uninsured is estimated to be between $65 billion and $130 billion per year. Using a ratio of 55% men and 45% women, the estimated total benefit of addressing the male health-insurance disparity is between $6.5 billion and $13 billion per year (IOM, 2004).
As a result of the connection between unemployment and lack of insurance—both of which disproportionally affect men—an increasing number of men are relying on Medicaid and Medicare for their health care needs. This increased burden on the system is further aggravated by men’s unfortunate propensity to delay or forego needed care. That means more late-stage diagnoses, which, in turn, leads to more complicated—and more expensive treatments (Families USA, 2009).
Tax Revenues
Excess morbidity and premature mortality in men affects every aspect of our economy, reducing employer productivity and diminishing family income. Lower earnings translate, of course, to lower revenue from federal, state, and local taxes. Among adults aged 25 to 64 years, there are 1.4 million more women than men (82.726 million women vs. 81.349 million men; U.S. Census Bureau, 2008). Conservatively assuming that 80% of those men would have been in the labor force, with a median household income of $49,777 per year (U.S. Census Bureau, 2010) and a total income tax burden of 9.2% (Cauchon, 2010), these men would have contributed more than $5 billion in combined federal, state, and local income taxes. In addition, employer payroll tax contributions (6.2% for Social Security and 1.45% for Medicare) would have added another $4.2 billion per year. In total, the 1.4 million men in the above calculation would have earned $55.75 billion. Subtracting 9.2% for taxes and 10% for savings (Americans’ savings rate is typically far lower than that), an 81%, or $44 billion, would likely be spent by American consumers. Although not calculated here, the effects of an annual $44 billion infusion into our economy would undoubtedly be substantial.
Social Security
According to the Social Security Administration, in 2009, 7.8 million workers received Social Security disability benefits. The majority of these benefits were paid to men, reflecting their greater exposure to workplace injury and disease risk (412,787 more men than women received disability benefits for conditions such as infectious and parasitic diseases, injuries, circulatory system diseases, digestive system diseases, and genitourinary problems; U.S. Social Security Administration, 2009). Based on an average monthly benefit of $1,134.50, the male health disparity costs the Social Security system $5.9 billion per year (U.S. Social Security Administration, 2009).
Federal Employees
With more than 2 million civilian employees—more than 56% of whom are male (U.S. Office of Personnel Management, 2009)—the federal government is the nation’s largest employer and, as such, suffers the same ill effects as the private sector from excess morbidity and premature death in men. In addition to lost employee productivity because of excess disease and disability, the Federal Employee Health Benefits Program (FEHBP) experiences greater costs due to advanced health problems in men. FEHBP provides coverage to almost 8 million people, with 4 million current and former employees enrolled, and the federal government covers 70% of the plan’s costs (O’Keefe, 2009). FEHBP is facing similar cost containment problems as the private sector, experiencing a growth in annual spending of nearly 8%.
Poverty in Widowhood
In 2009, there were 135 women, 65 years and older, for every 100 men of the same age (U.S. Administration on Aging, 2009). Premature death in men has significant economic consequences for widows and for the government agencies that bear the cost of caring for the deceased’s dependents. The Administration on Aging reports that more than half of elderly widows now living in poverty were not poor before the death of their husband (U.S. HHS, 2001). In all, 20% of elderly widows live in poverty, which is almost five times the overall rate for elderly married women (McGarry & Schoeni, 2002-2003). The onset of poverty is directly related to the husband’s death: The mean income for widowed women drops from $23,284 to $11,121 (Men’s Health Network, n.d). Aside from financial hardship, the descent into poverty also negatively affects women’s health, which, in turn, further increases government costs (Wu & Hart, 2002). In addition, in the first month of widowhood, the risk of death—from all causes—doubles (Bonhomme, 2007).
Government expenditures associated with poverty in widowhood fall into several broad categories: Social Security, Medicaid and Medicare, and other programs (including food stamps and subsidized housing). Each of these categories is briefly discussed below.
Social Security
In 2010, of all those receiving monthly Social Security benefits, 56%—or 30.6 million—were women. Of those, about 17 million received survivor benefits, averaging $12,516 per year (U.S. Social Security Administration, 2009).
The Supplemental Security Income program provides income support to approximately 2 million needy adults aged 65 years or older, 68% of whom are women. In 2008, Supplemental Security Income payments for this age group averaged $4,752 per person, for a total of $6.5 billion in federal dollars (this figure does not include any applicable state supplementation). Lengthening the life span of men by promoting healthy behaviors would not only reduce the need for federal survivor payouts but would also substantially reduce disability payments.
Medicare and Medicaid
Medicare is a federally funded insurance program that covers primarily people more than 65 years, regardless of income, and is funded through payroll taxes. Most Medicare recipients make some out-of-pocket payments for deductibles, medication, and hospital care. Medicaid is a completely different program—funded jointly by the federal government and individual states—that pays for health care services and medication for many low-income people, one fourth of whom are elderly. Medicaid pays Medicare premiums and for most other expenses, such as deductibles and co-pays. Eighteen percent (9 million people) of all Medicare recipients are considered “dual eligible,” meaning that they also qualify for Medicaid (Kaiser Family Foundation, 2007). Elderly duals cost federal and state governments approximately $15,900 per person, per year (Kaiser Family Foundation, 2010a), which accounts for 46% of Medicare spending (Kaiser Family Foundation, 2009). A total of 5.6 million (62% dual eligibles are women (Kaiser Family Foundation, 2010a), who receive a total of $89 billion in Medicaid services and support. After becoming widows, women’s poverty rate nearly doubles, from 14% to 26% (Lee, & Lee, 2006). Using those figures, approximately $47.9 billion of these costs can be attributed to the husband’s premature death.
Other programs
The large amount of Social Security used to support widows is often inadequate and many are forced to seek refuge in other government programs providing food stamps and subsidized housing. Additional expenses in the Supplemental Nutrition Assistance Program (SNAP—formerly called Food Stamps) have been found to total up to $1.2 billion for low-income widows as a result of their husbands’ premature death (Watkins, 2006). These federal expenses will only increase as the life expectancy gap continues to grow. Though outside the scope of this investigation, it is important to note that states bear an enormous burden as a result of excess morbidity and mortality in men, particularly during economic downturns. Medicaid payments for long-term care (for both sicker men and widows), state social security assistance programs, reduced state revenues from lost taxable income (because of disability and premature death), and reduced economic output all place significant strain on local and state government programs.
Costs to U.S. Businesses and the Economy
This article has discussed how much the premature—and largely preventable—death of American men costs federal, state, and local governments in terms of tax revenue. That cost, which this investigation estimates to be between $136 and $142 billion per year (See Table 3), pales in comparison with the enormous toll the poor health of men takes on American businesses and the U.S. economy.
Annual Federal Costs Attributed to Excess Health Disparities in Men

Years of Potential Life Lost
One important measure of the cost of disease and death is to consider the years of potential life lost (YPLL), which is essentially the number of years between death and projected life expectancy (Gardner & Sanborn, 1990). For example, if a person with a life expectancy of 75 years dies at age 52 years, 23 years of potential life are lost. For the 11 most common causes of death in 2007 (the most recent data available), the CDC (2009) estimated 9.17 million YPLL for males, 5.56 million for females. These causes include heart disease, cerebrovascular disease, cancer, chronic lower respiratory disease, influenza/pneumonia, liver disease, diabetes, HIV-AIDS, unintentional injuries, suicide, and homicide. Of course, it is impossible to put a dollar value on the cost of a human life. However, it is possible to estimate the social and economic cost—often a calculation of the value of productivity lost because of death—of a year of life. LaVeist, Gaskin, and Richard (2009) use $50,000 per year—a figure that, according to Braithwaite et al. (2008), is extremely conservative, given the range of $95,000to $297,000 generally used to calculate quality-adjusted life-years. Using $50,000, the value of the 3.61 million excess years of male life (9.17-5.56) that would have been saved if men’s health were on par with women’s is $180.5 billion per year.
Direct and Indirect Costs
Thus far, we have discussed the costs related to death. But what about those men who are still very much alive but suffer from a chronic illness, an injury, or other health issues such as asthma, arthritis, migraines, depression, back pain, gastrointestinal disorders, and diabetes—that may reduce their on-the-job performance (presenteeism) or cause them to miss work altogether (absenteeism)?
About half of the U.S. adult population—133 million Americans—suffer from a chronic condition (Robert Wood Johnson Foundation, 2004) and many suffer from more than one. A recent study by the Milken Institute estimates that seven chronic conditions (cancer, heart disease, hypertension, mental disorders, diabetes, pulmonary conditions, and stroke), which affect more than 109 million Americans, costs the U.S. economy more than $1.3 trillion per year (DeVol & Bedroussian, 2007). Approximately $277 billion of that is direct costs; the remaining $1.1 trillion is lost productivity—nearly 7% of U.S. GDP. (This is a conservative figure because it excludes condition other than the seven examined, the considerable health expenditures of the institutionalized population, and spending associated with follow-up health consequences of the seven listed conditions.) These figures are very similar to those cited by Loeppke and Hymel (2006), who found that for every dollar employers spend on worker medical or pharmacy costs, they have already lost at least $2 to $4 in health-related productivity from absenteeism and presenteeism (see Figure 2). The U.S. Department of Labor Statistics estimates that for all causes (not just the seven in the Milken report), poor health costs American businesses $1.8 trillion (Loeppke et al., 2007).

Top 10 health conditions by annual medical, drug, absenteeism, and presenteeism costs per 1,000 FTEs for Phase 2 companies
Given that 56% of the U.S. civilian workforce is male (U.S. Bureau of Labor Statistics, 2010), it is reasonable to assume that at least 56% of these costs are incurred by men. That puts the excess costs (the amount required for men to achieve health care parity with women) at $156 billion (using Milken’s calculations) to $216 billion (using U.S. Department of Labor Statistic calculations: 56% male/44% female = 12% point gap. $1.3 trillion × 0.12 = 156 billion; 1.8 trillion × 0.12 = 216 billion). At a time when the U.S. economy is struggling and GDP growth is essentially flat, an infusion of $156 to $216 billion (in increased productivity and reduced health care expenses) could spur tremendous growth. It is important to note that these numbers do not include data on all physical and mental conditions, or “intangible costs,” such as work time lost by those providing care to an injured or disabled man, quality of life, emotional problems, or lifestyle changes. These costs are nearly impossible to accurately quantify, but they do have an important impact on individual men, their families, their employers, and their communities.
Return on Investment (ROI)
Clearly, reducing or eliminating the male health disparity can save lives and money. But what would it cost federal, state, and local governments and American businesses to accomplish this goal? Several studies have done cost–benefit/ROI analyses and have concluded that health-promotion programs, whether sponsored by government or business, produce a significant, positive return. For example:
Business ROI
A 1999 study of a comprehensive health management program at Citibank estimated the ROI to be between $4.56 and $4.73 per dollar spent on the program (Ozminkowski et al., 1999).
A cost–benefit analysis performed for The Dow Chemical Company showed that a very small amount of health risk reduction (0.17 percentage points per year) over 10 years would allow the company’s health promotion program to break even, while larger reductions in health risk (1 percentage point per year) over 10 years would yield an ROI of $3.21 for every $1 invested (Goetzel, 2005).
A meta-analysis of work-site health promotion programs found an average reduction in medical costs of slightly more than 25% (Chapman, 2005).
The National Business Group on Health polled 352 human resources or health benefits managers at companies employing more than 1,000 in the United States and Canada. They found that companies with effective health and productivity (H&P) programs experience superior human capital and financial outcomes: 11 percent higher revenue per employee, lower medical trends by 1.2 percentage points, 1.8 fewer days absent per employee and 28 percent higher shareholder returns. High-H&P-effectiveness companies are also more likely to have lower health care costs, lower levels of presenteeism, fewer lost days due to disabilities and lower levels of turnover relative to their industry peers. (National Business Group on Health, 2010)
Government ROI
Local, state, and federal funding of programs to boost awareness of men’s health and to increase men’s participation in health management also have the potential to produce significant net cost savings.
Baltimore City Health Department’s Men’s Health Center (funded by the W. K. Kellogg Foundation) provides no cost medical care to uninsured men aged 19 to 64 years. The Center provides physical exams, screenings for blood pressure, cholesterol, weight, diabetes, tuberculosis, sexually transmitted diseases, and prostate cancer. The men-only aspect reduces embarrassment or feelings of inadequacy that some men feel when seeking care and allows the center to focus on male-oriented outreach and education, as well as clinical issues pertaining largely to men. The results:
By providing culturally sensitive, timely, and appropriate care in a supportive environment, the city would save significantly on uncompensated care delivered in ERs and hospital inpatient settings. The cost of setting up and running the clinic would also be offset by savings in mental health care, drug-related spending, such as rehabilitation and other treatment, and outlays in the legal system. (Alteras & Silow-Carroll, 2005)
Denver’s Men’s Health Initiative (MHI—also originally funded through the W. K. Kellogg Foundation). An ROI analysis found that men who were enrolled in the program showed an increase in primary and specialty care visits and a decrease in urgent care, behavioral health, and inpatient visits. These changes in utilization patterns accounted for a total decrease in charges to the health system of $300,000 during an 18-month period. That includes a reduction in uncompensated care charges by $206,485, despite almost 1,500 additional primary care encounters. After calculating the cost of employing the program staff, purchasing medical supplies, and arranging for patient transportation, the analysis found that every $1 invested in MHI saves the hospital system $3.68—more than $200,000 annually (Alteras & Silow-Carroll, 2005).
Both of the above projects are relatively small. However, these outcomes indicate that similar results can be achieved on a national scale. The Trust for America’s Health (2009) estimates that an investment of $10 per person per year in proven community-based disease prevention programs (The New York Academy of Medicine, 2009)—aimed at improving physical activity and nutrition and preventing smoking and other tobacco use—could yield net savings of more than $2.8 billion annually in health care costs in 1 to 2 years, more than $16 billion annually within 5 years, and nearly $18 billion annually in 10 to 20 years (in 2004 dollars). In ROI terms, these programs would produce a return of $0.96 in the first 1 to 2 years (meaning that the original investment of $10 is recovered, plus an additional 96 cents). Within 5 years, ROI could rise to $5.60 for every $1.00 invested, and to $6.20 within 10 to 20 years. This ROI represents medical cost savings only and does not include the significant gains that could be achieved in worker productivity, reduced absenteeism at work and school, and enhanced quality of life (Trust for America’s Health, 2009). In addition to total dollars saved, the study looked at how this investment could benefit different health care payers. Medicare could save more than $487 million annually in the first 1 to 2 years, more than $5.2 billion annually within 5 years, and nearly $5.9 billion annually in 10 to 20 years. Medicaid could save $370 million annually in the first 1 to 2 years, some $1.9 billion annually within 5 years, and more than $2 billion annually in 10 to 20 years. And, annually private insurers and individuals (through reductions of out-of-pocket costs) could see the biggest savings, with nearly $2 billion annually in the first 1 to 2 years, more than $9 billion annually within 5 years, and more than $10 billion annually in 10 to 20 years (see Table 4).
Net Savings by Medicare, Medicaid, and Private Insurers for an Investment of $10 per Person

Intangible Benefits
A public good is one whose benefits reach across borders, regardless of gender, age, ethnicity, or economic status, therefore benefiting everyone. Because of the public good dimension of health care, benefits from spending to address health care disparities are available not only to the people affected by them but also to others. In other words, benefits are available equally to everyone regardless of who incurs the cost. Public education campaigns about the effects of healthy diets, smoking, stress reduction, and alcohol and illicit drug use are a good example. Once the information is disseminated through public media, it is available to everyone—men and women alike—and there is no increased costs for additional people to access and benefit from it.
“Externalities” or “spillover effects” are another interesting phenomenon of health care. Simply put, externalities are “the cost or benefits of a transaction to parties who do not directly participate in it” (The Free Dictionary by Farlex, n.d.). They can be either negative (such as air pollution, which affects people other than those who produce it) or positive (treating one person’s infectious disease benefits not only the person treated but also other people who happen to come into close contact with the person). Men’s health disparities produce a number of negative externalities, since more men than women smoke, abuse alcohol and drugs, commit crimes, are involved in car accidents, and engage in risky behavior. Reducing or eliminating these disparities would have substantial benefits for men, their families, and society as a whole.
Conclusion and Next Steps
To the best of our knowledge, this is the first analysis of the direct and indirect costs to the government and private sector that are the result of premature morbidity and mortality in men.
Health disparities in men add substantial hardship to their families and the overall health of society. Their premature morbidity and mortality sharply increase government and private sector expenditures. A national commitment to prevention and health promotion—coordinated via the implementation of a Federal Office of Men’s Health—will could curb expenditure growth and create effective social norms aimed at breaking through the paradigm associated with men avoiding health care. A recognized federal focus can act as the apex of lifestyle promotion, workforce safety practices, and male-specific research advocacy.
It is important to recognize that health care spending and outcomes are not a zero-sum equation. Improving men’s health in no way comes at the expense of women’s health by steering funds, energy, and research away from women. The women’s health model includes programs such as WISEWOMAN, which from July 2008 to June 2010 provided health screenings for more than 78,000 women, 89% of which were found to have a least one risk factor for heart disease (CDC, 2011). As a result, 61% of the women screened participated in at least one lifestyle intervention resulting in improvements in weight, blood pressure, cholesterol levels, and smoking habits (CDC, 2011). These improvements have significantly reduced the WISEWOMAN participants’ risk of developing heart disease, which is a major cause of death in the United States (CDC, 2011). The Department of Health and Human Services estimates that through their women’s health initiatives, by the year 2000, approximately 85% of women had received a pap smear within 3 years, and 75% of females aged 50 years and older had received a mammogram, which helped decrease the cancer mortality rate by an average of 2.4% each year (“The role of HHS in improving women’s health,” 2002). These programs and initiatives have prevented millions of unnecessary deaths, improved the lives of millions of women, and should serve as a roadmap toward achieving the same goal for men. As Jean Bonhomme (2007) writes, “A rising tide lifts all boats.” In other words, improving men’s health also improves the health of their spouses, children, neighbors, coworkers, and society as a whole.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.