
Abstract
This study compares the clinical efficacy of electrical pudendal nerve stimulation (EPNS) with pelvic floor muscle training (PFMT) in treating post-radical prostatectomy urinary incontinence (PRPUI). A total of 26 patients with PRPUI were divided into a treatment group (14 cases) and a control group (12 cases) based on their choice of therapy. The control group underwent PFMT, while the treatment group received EPNS. The number of pads used, 24-hr pad test and the International Consultation on Incontinence Questionnaire Short Form (ICI-Q-SF) were observed and scored for both groups before treatment and at 8 weeks of treatment, and the clinical efficacy was evaluated. Pelvic floor neuroelectrophysiology indicators of pudendal somatosensory evoked potentials, pudendal skin sympathetic reflex, bulbocavernosus reflex, and needle electromyography were also collected from 11 out of 26 patients. Compared with pretreatment, scores of the number of pads used, 24-hr pad test, ICI-Q-SF, and sum scores in both treatment and control groups decreased significantly after treatment (p < .05); the treatment group showed significantly higher differences in the pre- and post-treatment scores of the number of pads used, 24-hr pad test, ICI-Q-SF, and sum scores compared to the control group (p < .01). The improvement rate in the treatment group was significantly higher than that of the control group (59.60% vs. 21.98%, p < .01). Pudendal nerve damage was implicated through pelvic floor neuroelectrophysiology. These findings suggest that EPNS can significantly improve the clinical symptoms of PRPUI (Trial Registration Number: ChiCTR2200055461).
Keywords
Introduction
Radical prostatectomy (RP) is the standard treatment for localized prostate cancer (Gu & Zhu, 2022; Mottet et al., 2021). However, urinary incontinence (UI) remains one of the most common complications following RP, severely affecting the patient’s physical and mental health. The incidence of UI within the first 3 months after RP ranges from 34% to 46%, with persistent UI affecting 8% to 25% of patients (Trofimenko et al., 2017). A clinical trial in the United Kingdom reported a 19% incidence of moderate to severe UI at 6 months post-surgery, which reduced to 13% after 6 years (Bhatt et al., 2024). Effective strategies for promoting the recovery of post-radical prostatectomy urinary incontinence (PRPUI) are thus a major clinical challenge and a subject of ongoing research.
Pelvic floor muscle training (PFMT) is a widely recognized first-line treatment for PRPUI (Sandhu et al., 2019). This therapy involves the patient’s voluntary contraction of the pelvic floor muscles, primarily the levator ani muscles, to strengthen their strength. However, PFMT is highly dependent on patient factors, including age and cognitive ability. Many elderly patients fail to perform PFMT correctly due to limited educational background and cognitive challenges, and their poor compliance often hinders the achievement of desired outcomes.
Electrical pudendal nerve stimulation (EPNS) was first applied by Chinese scholar Wang Siyou as a conservative method for the treatment of female stress urinary incontinence (SUI) (Wang & Zhang, 2012). EPNS involves deep needle insertion combined with electrical stimulation near the pudendal nerve (confirmed by CT imaging at the coccyx level), inducing rhythmic contractions of the pelvic floor muscles to strengthen them (Wang et al., 2016). This approach addresses limitations in voluntary PFMT, such as improper contraction or inability to maintain consistency. Previous studies have demonstrated promising therapeutic effects of EPNS in treating SUI (Wang & Zhang, 2012, 2013; Wang et al., 2016). In this study, we applied EPNS for the treatment of PRPUI and compared its efficacy with PFMT as a control group.
Materials and Methods
Clinical Data
This study included 26 patients from the inpatient and outpatient departments (Acupuncture and Moxibustion and Urology Department) of the First Affiliated Hospital of Zhejiang Chinese Medical University. Participants were recruited between June 2022 and December 2022 and were assigned to different groups based on their choice of therapy. Fourteen patients who received EPNS formed the treatment group, while 12 patients who underwent PFMT served as the control group. The study was approved by the Ethics Committee of the First Affiliated Hospital of Zhejiang Chinese Medical University (2021KL-040-02), and all participants provided written informed consent.
Inclusion and Exclusion Criteria
Inclusion Criteria
(1) Patients with UI symptoms at 1 month or more after RP, with a positive 24-hr pad test (i.e., the weight of the pad increases by more than 4 g within 24 hr) (Dalela et al., 2017); (2) Meeting the diagnostic criteria for SUI or SUI-predominant mixed urinary incontinence (MUI) (Heesakkers et al., 2017); (3) Age between 45 and 90 years.
Exclusion Criteria
(1) Urge urinary incontinence-predominant MUI; (2) Overflow incontinence; (3) Pre-existing UI or other conditions causing UI, such as Parkinson’s disease, multiple sclerosis, spinal cord injury, dementia, or diabetes; (4) Urethral stricture, urinary tract obstruction, refractory urinary tract infection, hydronephrosis, urinary system stones; (5) Severe dysfunction of major organs (heart, lungs, liver, and kidneys).
Methods
The control group received PFMT, and the treatment group received EPNS.
Pelvic floor muscle training
Patients in the control group performed PFMT using Kegel exercises. A physiotherapist guided the training, explaining how to contract the pelvic floor muscles and providing instructions. Patients were instructed to contract their pelvic floor muscles as strongly as possible for 3 to 10 s, depending on their ability, and then relax for an equal duration. This contraction-relaxation cycle was repeated 15 times to complete one set. Patients were instructed to perform three sets daily in each different position (supine, sitting, and standing) at home for a duration of 8 weeks.
Electrical pudendal nerve stimulation
Four specific points on the sacrococcygeal area, namely “Sacrococcygeal Four Points.” The upper two points are located 1 cm beside the sacrococcygeal joint (bilaterally symmetrical), and the lower two points are located 1 cm beside the coccygeal tip (bilaterally symmetrical). The patient took a prone position, exposing the puncture site with strict local disinfection. For the upper two points, a needle measuring 0.40 × 100 mm (Suzhou Shenlong Medical Apparatus Factory, Suzhou, China) was inserted perpendicularly with a depth of 75 to 90 mm, making the needle sensation reach the urethra or anus; For the lower two points, use a needle of the same length as mentioned above to puncture obliquely outward (toward the ischiorectal fossa), with a depth of 90 to 95 mm, making the needle sensation reach the perineal area (root of the penis). After the needle sensation reached the above areas, the needle handle on the same side of the body was connected to a pair of electrodes of the G6805 electroacupuncture device (Shantou Medical Equipment Factory, Shantou, China), which was set to produce a continuous wave with a frequency of 2.5 Hz and intensity (45–55 mA) within patient’s tolerance lasting 60 min each time. During the EPNS treatment, the pelvic floor muscles must maintain a rhythmic strong contraction upward (toward the head) centered on the root of the penis. The treatment time was once a day, 3 times a week. Eight weeks was defined as one observation cycle for both groups.
The EPNS was performed by an acupuncturist with a licensed physician qualification at the hospital, while the PFMT was guided by a licensed physiotherapist.
Evaluation and Outcome Measures
The scores of the number of pads used, 24-hr pad test, International Consultation on Incontinence Questionnaire Short Form (ICI-Q-SF), and sum scores were recorded before and after treatment.
Primary Indicator
The improvement rate was calculated using the formula:

Secondary Indicator
Number of pads used (Kulseng-Hanssen & Borstad, 2003): Different scores were given according to the number of pads: those who do not need pads, 0 points; 1 to 3 pads/week, 1 point; 4 to 6 pads/week, 2 points; 1 to 4 pads/day, 3 points; more than 4 pads/day, 4 points.
24-hr pad test (Soto González et al., 2018): The pad weight increasing within 24 hr was measured, and severity was graded and scored: 0 points (less than 4 g), 2 points (5–20 g), 4 points (21–74 g), 6 points (greater than 75 g).
ICI-Q-SF score (Timmermans et al., 2013): Including three parts: the number of urine leaks, the amount of urine leakage, and the impact on daily life. The total score ranged from 0 to 21 points, with higher scores indicating more severe UI.
Statistical Analysis
Data were analyzed using IBM SPSS version 26 software. Quantitative data conforming to normal distribution were presented as mean ± standard deviation. Intra-group comparisons were performed using paired sample t-test, while inter-group comparisons were made using two independent sample t-tests; for quantitative data that did not follow a normal distribution, values were represented as median (upper, lower quartiles) (M [P25, P75]), and rank sum test was applied. Categorical data were described using rates (%), with the Chi-square test used for comparisons. Rank data were compared using the Wilcoxon two-sample rank sum test. A p value <.05 was considered statistically significant.
Results
Baseline Characteristics
The baseline demographic and clinical characteristics of the patients, which could influence urinary control, are summarized in Table 1. Statistical analysis showed no significant differences between the treatment and control groups in terms of age, disease duration, type of UI, Gleason score, endocrine therapy, radiotherapy, or surgical methods (p > .05).
Baseline Demographics and Clinical Characteristics (n = 26)

Note. Mean
Comparison of Pre- and Post-Treatment Scores
Compared with pretreatment, the scores for the number of pads used, 24-hr pad test, ICI-Q-SF, and sum scores decreased significantly in both groups after treatment (p < .05) (Table 2). The treatment group demonstrated significantly greater improvements in these scores—namely, the number of urinary pads used, 24-hr pad test, ICI-Q-SF, and sum scores—compared to the control group (p < .01) (Table 3).
Intra-Group Comparison of Scores of Number of Pads Used, 24-Hr Pad Test, ICI-Q-SF, and Sum Scores Before and After Treatment

Note. M (P25, P75). ICI-Q-SF = International Consultation on Incontinence Questionnaire Short Form.
Comparison of pre- and post-treatment within the group showed a statistically significant difference (p < .05).
Inter-Group Comparison of Differences in Scores of Number of Pads Used, 24-Hr Pad Test, ICI-Q-SF, and Sum Scores Before and After Treatment

Note. M (P25, P75). ICI-Q-SF = International Consultation on Incontinence Questionnaire Short Form.
Compared with the control group, p < .01.
Improvement Rate
The improvement rate in the treatment group was 59.6%, while the control group showed an improvement rate of 21.98%. The difference in improvement rates between the two groups was statistically significant (p < .01) (Table 4).
Improvement Rates Between Two Groups
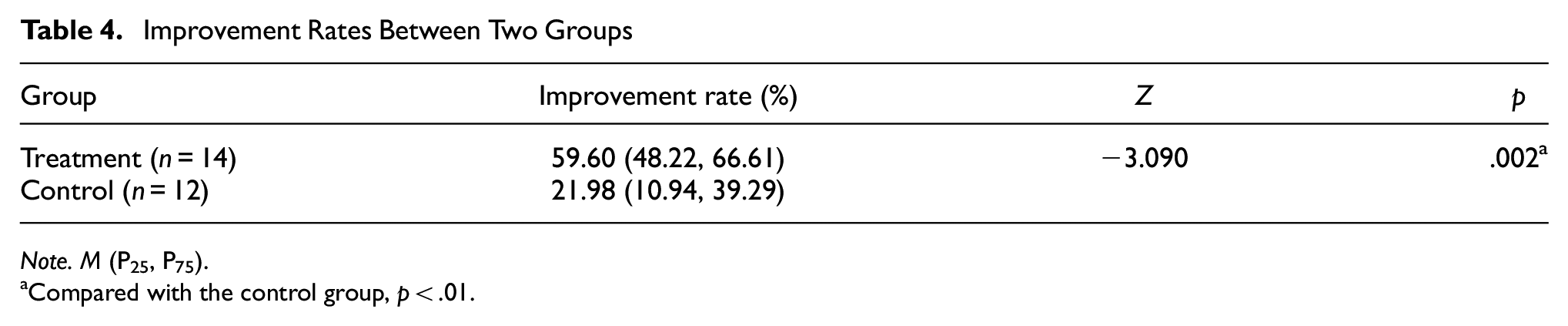
Note. M (P25, P75).
Compared with the control group, p < .01.
Pelvic Floor Neuroelectrophysiology Data
Pelvic floor neuroelectrophysiology data were collected at baseline from 11 out of the 26 patients with PRPUI. The indicators assessed included pudendal somatosensory evoked potentials (P-SEP), pudendal skin sympathetic reflex (P-SSR), bulbocavernosus reflex (BCR), and needle electromyography (EMG). A high rate of abnormalities was observed, with 72.7% of patients showing abnormal P-SEP results, 72.7% showing abnormal P-SSR, 45.5% showing abnormal BCR, and 36.4% showing abnormal EMG findings (Table 5).
Results of Pelvic Floor Neuroelectrophysiology (n = 11)

Note. P-SEP = pudendal somatosensory evoked potentials; P-SSR = pudendal skin sympathetic reflex; BCR = bulbocavernosus reflex; EMG = electromyography.
Discussion
During RP, damage to the urethral sphincters and the supporting structures of the urethra is inevitable, leading to UI, which significantly affects patients’ quality of life. The urethral sphincters, particularly the external sphincter, and the levator ani muscle, which is innervated by the pudendal nerve, are key structures involved in urinary control (Onishi et al., 2023). The recovery of these muscles is critical for patients with PRPUI.
In our study, there were no statistically significant differences in age, disease course, types of UI, Gleason score, endocrine therapy, radiotherapy, and surgical methods between the two groups (p > .05). Compared with pretreatment, the scores for the number of pads used, 24-hr pad test, ICI-Q-SF, and sum scores decreased significantly in both groups after treatment, which meant EPNS and PMFT were both effective for PRPUI patients.
Although statistical differences were observed in the indicators (number of pads used, 24-hr pad test, and sum scores), except for ICI-Q-SF, before treatment (p < .05), direct comparisons before treatment were not feasible due to the small sample size and greater data variability. Therefore, the changes in each indicator after treatment between the two groups were analyzed, and the treatment group showed significantly better outcomes than the control group.
EPNS is a novel physiotherapy technique that combines the benefits of PFMT, nerve electrical stimulation therapy, and acupuncture’s deep needling technique. Noninvasive and nonimplantable, it facilitates passive and efficient pelvic floor muscle contraction, thereby simulating pelvic floor exercises (Feng et al., 2022). Its good acceptance, compliance, and persistence among patients may contribute to the superior efficacy of EPNS over PFMT in terms of symptom improvement rate.
There is growing evidence suggesting a link between pudendal neuropathy and female SUI (Castelán et al., 2018). However, the impact of pudendal nerve dysfunction on PRPUI remains less understood. The pudendal nerve, originating from the S2 to S4 spinal segments, gives rise to the inferior rectal nerve, the perineal nerve, and the deep dorsal nerve of the penis, innervating key structures such as the external anal sphincter, external urethral sphincter, levator ani muscle, bulbospongiosus, and ischiocavernosus (Shafik, 2000). P-SEP provide insights into the integrity of the sensory pathway from the pudendal nerve to the central nervous system (Markers, 2023), while P-SSR evaluates the autonomic regulation of pelvic structures (Valles-Antuña et al., 2009). The BCR is used to assess the integrity of the S2 to S4 spinal segments and pudendal nerve (Markers, 2023). Needle EMG evaluates the neuromuscular function of pelvic floor muscles (Khatri et al., 2017). Our findings suggest that PRPUI patients may experience pudendal nerve damage, leading to pelvic floor disorders such as UI, erectile dysfunction, and pelvic pain. These findings imply that EPNS could restore pudendal nerve function through direct electrical stimulation, highlighting a promising new treatment strategy for PRPUI. While our study provides postoperative insights, the absence of preoperative assessments for pelvic floor dysfunction or pudendal nerve injury remains unresolved. We recommend that future work incorporate baseline functional measurements to strengthen causal inferences.
This study does have limitations. First, the sample size was small, and during the data collection, the COVID-19 pandemic in China severely limited patient visits and follow-ups. Second, patients were not randomly assigned to treatment or control groups. Grouping was based on the way they chose, as a considerable number of patients preferred practicing PFMT at home. Moreover, the pandemic reduced the number of patients seeking medical care. Long-term efficacy data were also unavailable due to difficulties in follow-up during the lockdown period. Future research should involve multicenter, large-sample studies to address these limitations.
In conclusion, EPNS significantly improves the clinical symptoms of PRPUI patients when compared to PFMT.
Footnotes
Acknowledgements
We would like to thank Jianhua Li and Hong Jiang for their guidance on rehabilitation and neuroelectrophysiology.
Ethical Considerations
This study was approved by the Ethics Committee of the First Affiliated Hospital of Zhejiang Chinese Medical University, Zhejiang Provincial Hospital of Traditional Chinese Medicine (approval number: 2021KL-040-02). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Consent to Participate
All the participants were well informed about the purpose of the study and signed a written informed consent before enrollment.
Consent for Publication
All the authors gave their consent for publication.
Author Contributions
Y.C. performed data analysis and wrote the manuscript; X.J. and F.W. screened participants; Q.H. collected data and conducted follow-up; S.C. took part in data analysis and provided overall guidance.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Zhejiang Provincial Administration of Traditional Chinese Medicine (grant numbers 2021ZA056; 2024ZL830), Zhejiang Provincial Health Commission, Zhejiang Provincial Medical and Health Science and Technology Program (grant numbers 2024KY136; 2023RC043), and National Administration of Traditional Chinese Medicine (grant number GZY-KJS-ZJ-2025-017).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.