
Abstract
Our aim is to investigate the prevalence of clinically significant prostate cancer (Gleason score 3+4 or higher) on fusion biopsy for Prostate Imaging Reporting and Data System (PI-RADS) 3–5 lesions based on ethnicity. A retrospective analysis was conducted on patients who underwent fusion biopsy between 2016 and 2022 at two institutions. The prevalence of Gleason score 3+4 or higher within each ethnic group (Caucasian, African American, and Hispanics) was assessed. Possible correlation between PI-RADS lesion score and race was also assessed. Among the 918 patients included in the analysis, 54% were Caucasian, 29% were African American, and 17% were Hispanic. A total of 1,384 lesions were identified (PI-RADS 3—34%, PI-RADS 4—40%, and PI-RADS 5—26%). The prevalence of clinically significant prostate cancer by PI-RADS score and ethnicity was similar: (PI-RADS 3—Caucasian 13%, African American 13%, and Hispanic 9%, p = .45; PI-RADS 4—Caucasian 42%, African American 34%, and Hispanic 38%, p = .29; PI-RADS 5—Caucasian 63%, African American 64%, and Hispanic 51%, p = .38). In conclusion, the prevalence of clinically significant cancer did not significantly differ across PI-RADS 3–5 among different ethnicities on image-guided fusion biopsy.
Introduction
Prostate cancer remains one of the most common cancers among men in the United States with 288,300 new cases diagnosed in 2023 (American Cancer Society [ACS], 2023). The disease has been well described as having heterogeneous presentation and prognosis across different racial and ethnic groups. A disproportionate number of prostate cancer diagnoses are associated with worse outcomes for non-Hispanic Black men and men from certain Latin American ethnic backgrounds, likely as a result from a combination of genetic and socioeconomic factors (ACS, 2023; Chinea et al., 2017; Smith et al., 2017). Prostate cancer literature in general tends to be under-representative of racial and ethnic minorities (Owens-Walton et al., 2022). With the shift in clinical practice to incorporate magnetic resonance imaging (MRI) into more domains of prostate cancer diagnosis, surveillance, and treatment, further emphasis should be placed on understanding parameters of the use of prostate magnetic resonance imaging (MRI) in a racially diverse population.
Previously, it has been demonstrated that clinically significant (CS) prostate cancer is detected more frequently in non-Hispanic Black men undergoing MRI-guided fusion biopsy (Eklund et al., 2021; Hines et al., 2021; Shin et al., 2017). Supplementary to this information would be to determine if there exists any significant correlation between Prostate Imaging Reporting and Data System (PI-RADS) lesion score and race or ethnicity, and if any differences in PI-RADS lesions with lower scores have any higher probability of detecting a CS prostate cancer in patients of certain racial or ethnic backgrounds.
Method
Retrospective analysis was performed on patients across two high-volume institutions. Inclusion criteria were patients 18 years or older found to have elevated prostate-specific antigen (PSA) or abnormal digital rectal examination, who underwent fusion prostate biopsy between 2016 and 2022, and who provided a self-reported race or ethnicity documented in their health record. Patient demographics, including the racial or ethnic identity of the patient, were assessed through retrospective chart review. Patients identifying as Black, Hispanic, or White were included in the study as the three most common identifiers of race or ethnicity. Patients underwent three-phase (T2-weighted imaging [T2W], diffusion-weighted imaging [DWI], and dynamic contrast-enhanced imaging [DCE]) biparametric or multiparametric 3T MRI Prostate MRI imaging and PI-RADS v2 scoring prior to intervention. Of note, while the PI-RADS scoring system was revised between eras in 2019, no significant difference is appreciated between scoring versions 2 and 2.1 (Rudolph et al., 2020).
PI-RADS score of 3, 4, or 5 on MRI was considered suspicious. All patients underwent image-guided biopsy for the suspicious areas, and standard systematic biopsies. The platform used for fusion biopsy was UroNav™, Philips Health care. CS disease was defined at Gleason grade group 2 (GG2) or higher.
To determine a correlation between PI-RADS lesion score and race, Fisher’s exact test was performed comparing total number of PI-RADS 3 lesions across three categories of patients identifying as Black, Hispanic, or White. The same was performed for cohorts of PI-RADS 4 and 5 lesions. Significant level was determined as p < .05. All tests were double-sided. Analysis was performed with SAS 9.4.
Results
The racial identity of patients is described in Figure 1. A total of 918 eligible patients were included in the study. Of these, 271 patients (29%) identified as Black, 153 (17%) identified as Hispanic, and 494 (54%) identified as White.
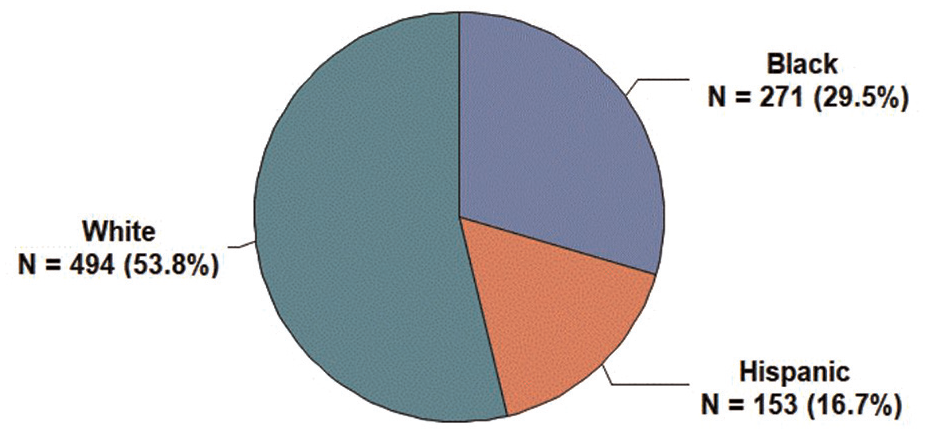
Racial or Ethnic Identity of All Patients Meeting Inclusion Criteria (n = 918)
A total of 1,384 PI-RADS lesions with score 3–5 were analyzed. Of these, 469 (34%) were PI-RADS 3, 554 (40%) were PI-RADS 4, and 361 (26%) were PI-RADS 5. A median of 3 scores (IQR 3–4) were taken per lesion. Median age of the patients was 65 (IQR 60–69) years with a mean PSA of 9.6 (SD 7.9). CS disease was detected in 494 (36%) of these lesions. Details of detected lesions and biopsies are described in Table 1.
Descriptive Characteristics of All PI-RADS Lesions Included in the Analysis (n = 1,384 Total Lesions)

Among Black patients, CS prostate cancer was found in 13% of PI-RADS 3, 34% of PI-RADS 4, and 64% of PI-RADS 5 lesions. Among Hispanic patients, CS prostate cancer was found in 9% of PI-RADS 3, 38% of PI-RADS 4, and 51% of PI-RADS 5 lesions. Among White patients, CS prostate cancer was found in 13% of PI-RADS 3, 42% of PI-RADS 4, and 63% of PI-RADS 5 lesions. These results are summarized in Table 2. There was no significant difference in the detection of CS cancer among PI-RADS scores 3–5 across all races (p-value .45, .29, and .38 for PI-RADS 3, 4, and 5, respectively), as shown in Table 3 and Figure 2.
PI-RADS Lesions With CS (GGG2 or Higher) Prostate Cancer Biopsy Results

Correlation of CS (GGG2 or Higher) Prostate Cancer to Patient Race or Ethnic Identity by Fisher’s Exact Tests, Stratified by PI-RADS Scores
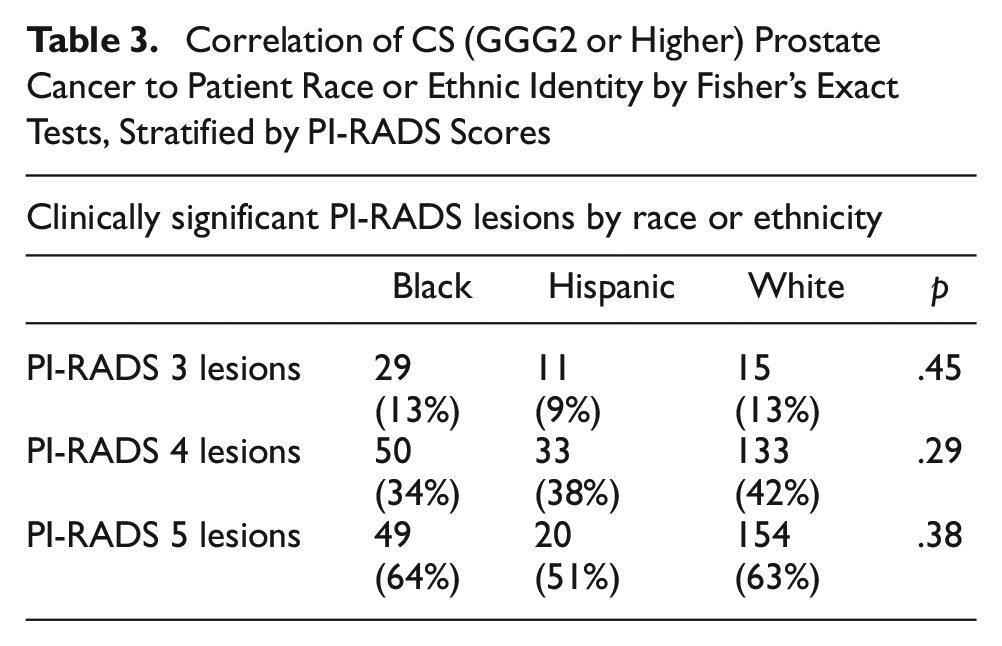

CS Prostate Cancer Detected in PI-RADS Lesions 3, 4, or 5 Shows No Significant Correlation to Patient Race or Ethnicity (p =.45 for PI-RADS 3, p=.29 for PI-RADS 4, and p=.38 for PI-RADS 5 by Fischer’s Exact Test)
Discussion
The findings of our study demonstrate that the yield of CS prostate cancer on image-guided fusion biopsy of PI-RADS 3, 4, and 5 was similar when stratified by patient race or ethnic identity. The significance of this finding becomes most relevant when considering that the validation of the PI-RADS system was performed in a population of predominantly White men, and has since been applied to a more diverse population of patients based on assumption and not clinically representative data (Leapman et al., 2022). As such, this study and those like it aim to correct for this inherent racial disparity in validating diagnostic and therapeutic tools as widely incorporated into clinical practice as prostate MRI has become. Any attempts to close the gap in health care delivery across racial and ethnic minorities can be justified when obtaining prostate MRI, even if supporting medical literature does not explicitly publish data on racial and ethnic minorities.
There is an emerging need to diversify racial representation in prostate cancer literature as previously novel technologies are quickly emerging as standards of care. Indeed, the last several decades have demonstrated increasing clinical applications for the role of prostate MRI in the detection, characterization, and management of prostate cancer. As interpretation of MRI results became more clinically relevant, prostate MRI interpretation became more standardized with the development of the PI-RADS scoring system in an effort to simplify and objectify radiologists’ interpretation of results (Turkbey et al., 2019). Prostate MRI’s role in the detection of prostate cancer gained widespread recognition with the Prostate MR Imaging Study (PROMIS) and PRostate Evaluation for Clinically Important Disease PRECISION trial suggesting that multiparametric MRI allows an increased detection of CS prostate cancer while avoiding over-detection of clinically insignificant cancers compared with standard TRUS-biopsy protocols (Ahmed et al., 2017; Kasivisvanathan et al., 2018). Emerging applications include follow-up MRI for patient on active surveillance, preoperative planning in demonstrating disease in relative proximity to the neurovascular bundle, mapping for focal therapy or radiation treatment, or prognostic predictors of recurrence (Fernandes et al., 2022; Tricard et al., 2020).
Although transitioning these data support the ubiquitous use of prostate MRI into clinical practice, providers should confirm these applications in an ethnically heterogeneous population. Unfortunately, this is often not the case—racial and ethnic minorities are overall under-represented in urologic oncology clinical trials across cancer types and studies of various funding sources, including prostate cancer (Owens-Walton et al., 2022). Certain studies have even suggested that the probability of detecting a CS cancer on MRI-guided biopsy may be even higher for Black men compared with White men (Hines et al., 2021). Similar disparities have been suggested for certain subgroups of patients of Latino/Hispanic descent, particularly of Puerto Rican background, although overall the Latino/Hispanic population are largely under-represented in published prostate cancer literature (Chinea et al., 2017). Further complicating this racial disparity is patients of Hispanic/Latino background who may be misrepresented as Black or White patients if the literature does not specify Non-Hispanic Black (NHB) or Non-Hispanic White (NHW). Our findings aim to correct this disparity in finding that fusion biopsy is just as likely to detect CS disease in patients identifying as Hispanic compared with those identifying as Black or White.
In addition to the lack of racial representation in prostate MRI literature, there also exist patient-specific socioeconomic barriers to obtaining MRI that are often tied to race and ethnicity. Indeed, it has been previously established that more barriers to obtaining prostate MRI exist for Black patients compared with White patients (Walton et al., 2019). This observation is particularly concerning given that Black patients tend to have higher risks of prostate cancer–related mortality, thought to be attributed to a combination of biological and socioeconomic factors (Nair et al., 2022; Smith et al., 2017). When considering that patients of racial or ethnic minority backgrounds may experience additional barriers to treatment for prostate cancer, it seems even more pertinent to be assured that the medical literature advocating for more frequent use of prostate MRI should be representative of racial and ethnic minorities. The burden of obtaining any additional workup prior to diagnosis or treatment should be weighed heavily against the additional benefit the MRI will provide.
The practical adoption of MRI in the clinical setting is not without certain pitfalls, including variability in MRI’s positive predictive value across imaging centers, inter-reader variability, and applications of the majority of current clinical data derived from treatment-naïve organs (Westphalen et al., 2020). These variables affecting the interpretation of prostate MRI further emphasize the necessity to validate the interpretation on MRI findings across a widely diverse patient population. The findings of this study support the use of the PI-RADS scoring system across a diverse population despite these pitfalls.
Although we should not disregard the vast body of literature delineating the use of prostate MRI in patients with prostate cancer, we can attempt to rectify such racial and ethnic disparities by demonstrating consistency in imaging results across racial groups. Our findings supporting the use of the PI-RADS scoring system across racial and ethnic minorities can maximize the emerging applications of prostate MRI in clinical practice. This is one attempt to demonstrate that our body of literature can—and should—be more generalized across a racially and ethnically diverse group of patients.
Limitations of our investigation include the retrospective nature of the study, and a limited number of institutions providing patient data. Further limitations include patients from only White, Black, and Hispanic backgrounds; patients of Asian, Native Hawaiian/Pacific Islander, or American/Alaska Native descent are not included in the study given low enrollment numbers that would not have been significant for the investigation. An important caveat to our study is the inclusion of patients with PSA > 20, which may confound our results given that patients with such high PSA levels are more likely to have CS prostate cancer detected on MRI. However, we feel that due to the low number of patients within this category distributed across all races, this category is unlikely to confound our overall conclusion that no race or ethnicity is more or less likely to have a CS cancer detected on MRI. Finally, limitations inherent to prostate MRI include up to 15% of prostate cancers “invisible” to prostate MRI, including the aggressive subtypes of ductal, intraductal, and cribriform cancers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
This project was classified as exempt by our institution’s Institutional Review Board.