
Abstract
This study explores aspects that men consider when deciding whether to participate in a prostate cancer screening program and how the information in the invitation letter contributed to their decision. Semi-structured interviews were conducted with 50- to 62-year-old men invited by letter to a population-based prostate cancer screening program. Data from transcribed interviews were analyzed using qualitative content analysis using manifest and indicative approaches. Eighteen men were interviewed, 10 whom chose to be tested, and 8 who declined screening. The information in the invitation letter was not decisive for whether men chose to be tested or not. The aspects that the men valued in their personal decision to participate or refrain from screening were categorized as (a) the expectation that authorities should take responsibility and provide guidance; (b) fear, which was described as both a driving force and a barrier; (c) reliance upon intuition combined with seeking social and emotional support; (d) the perception of one’s own risk of being affected. Men who relied on risk assessment mentioned difficulties in evaluating the information about the potential disadvantages of screening. Our findings suggest that the intention of informed decision-making for prostate cancer screening is difficult to fully realize. Further research is needed to understand how the individual decision-making process is influenced by factors such as assessment of personal risk, perception of advantages and disadvantages, and cultural background, and to optimize the information to the invited men.
Introduction
The question of whether men should undergo screening for prostate cancer is the subject of extensive scientific investigation and debate. For the past three decades, prostate-specific antigen (PSA) testing has been a key tool in the early detection of prostate cancer. However, elevated PSA levels can also result from benign conditions such as prostatic hyperplasia, contributing to overdiagnosis, particularly of low-grade cancers (Hugosson et al., 2019). This challenge has driven the development of complementary diagnostic methods, such as magnetic resonance imaging (MRI), which have improved accuracy and mitigated overdiagnosis by refining risk stratification and reducing unnecessary biopsies (Bratt et al., 2023). These methods are currently being assessed in randomized screening trials, further evaluating their impact on prostate cancer detection and management (Auvinen et al., 2017; Hugosson et al., 2022; Kohestani et al., 2021).
In 2018, the Swedish Ministry of Social Affairs commissioned regional cancer centers to develop standardized and more effective testing for prostate cancer. This resulted in the start of population-based regional organized prostate cancer testing (OPT; Alterbeck et al., 2022). The Swedish OPT programs agree well with the European Union’s 2022 recommendation to evaluate the feasibility and effectiveness of organized screening programs for prostate cancer (European Union Council, 2022).
Traditionally, men’s decision to test their serum PSA and possibly initiate an investigation for an early diagnosis of prostate cancer has been made in consultation within a shared decision-making context with healthcare professionals as discussion partners (Dasarathy & Rajesh 2020). In such personal decision-making, the individual considers the different options and chooses an action based on personal preferences, values, or goals (Van den Berg et al., 2006). Previous studies have shown that shared decision-making with a healthcare professional helps men navigate and reach a personal decision about PSA testing (Bell et al., 2014; Lin et al., 2008).
A central part of Swedish OPT is to offer all eligible men brief, neutral, easy-to-understand, written information about the possible advantages and disadvantages of being tested for early detection of prostate cancer. This means that men are meant to make their decisions on their own rather than in consultation with a healthcare professional. This contrasts with the general principle of shared decision-making in healthcare and the U.S. Preventive Services Task Force’s (2018) recommendation that decisions about PSA testing should be made in consultation with healthcare professionals based on individual values. Eldh et al. (2008) emphasize the importance of patient participation in healthcare decisions but also describe nonparticipation as a lack of recognition, information, and security in patient-provider interactions.
A survey study from two regional Swedish OPT programs showed that almost all respondents held a positive attitude about making a personal decision about PSA testing, but that some considered the described disadvantages difficult to understand (Svensson et al., 2023). Previous studies of men’s decision-making have shown that they often base their decision about PSA testing on the presence or absence of symptoms from the urinary tract (Rai et al., 2007), a belief that a healthy lifestyle can prevent prostate cancer (Ferrante et al., 2011), increasing age, that healthcare professionals recommend PSA testing (Li et al., 2018) and an active discussion with a healthcare professional about the advantages and disadvantages of PSA testing (McCormick & Haile 2023). It has not previously been reported which aspects influence men’s personal decision-making about PSA testing in a population-based screening setting where information and an invitation are sent home. The aim of this study was to explore this in depth.
Methods
Setting
The first two Swedish OPT projects started in 2020 in Region Västra Götaland and Region Skåne (Alterbeck et al., 2022). These two regions together have three million inhabitants and include urban, semi-urban, and rural areas. In Region Skåne, an initial pilot project included 1,000 randomly selected men who the past few months, had been invited to OPT, aged 50, 56, and 62. The Region Västra Götaland project began by inviting all 12,000 men born in 1970 (i.e., 50 years old).
The invitation letter contained a brief (12 sentences), neutral summary of the advantages and disadvantages of testing for early detection of prostate cancer (Supplemental Material) and a description of the diagnostic procedures for individuals with an elevated PSA value, MRI of the prostate and, for some, transrectal ultrasound with a biopsy. The text about the advantages and disadvantages of testing was written by the National Working Group for Organized Prostate Cancer Testing and had been reviewed and endorsed by several professional organizations, the National Prostate Cancer Patient Organization, and men without prostate cancer. In both regions, the men could have a PSA test free of charge after receiving the invitation, without making an appointment either at a primary care center or any of the public hospitals in the region.
Participants and Recruitment
In the fall of 2020, an invitation to participate in a telephone interview and a copy of the OPT invitation letter were sent out to 400 men invited to the OPT program. Men who were interested in sharing their experiences through an interview were asked to email the first author of this article (LS, oncology specialist nurse) to arrange for a date and time. To achieve a balanced representation of men who chose to have a PSA test within OPT and those who declined, an additional 200 interview invitations were sent separately to men who had not undergone PSA testing within the OPT program. These 600 interview invitations were positively responded to by 24 men, of whom 18 were interviewed. Of these, 6 later chose not to be interviewed for personal reasons, leaving 18 men for interview. Before the interview began, men were asked about sociodemographic factors (Table 1).
Demographic Characteristic

Note. PSA = prostate-specific antigen.
Nonacademic-Primary school (9 years), secondary school (3 years). Academic: high school/university.
Data Collection
After verbal approval, semi-structured interviews were conducted by LS with the support of an interview guide (McGrath et al., 2019). The interviews were conducted between March and May 2020, lasting between 12 and 25 min, and were recorded and saved as audio files. Each session began with a brief explanation of the study’s purpose and time for questions before recording started. The interview started with an introductory question, followed by the interviewer guiding the conversation according to the guide (Table 2).
Semi-Structured Interview Guide

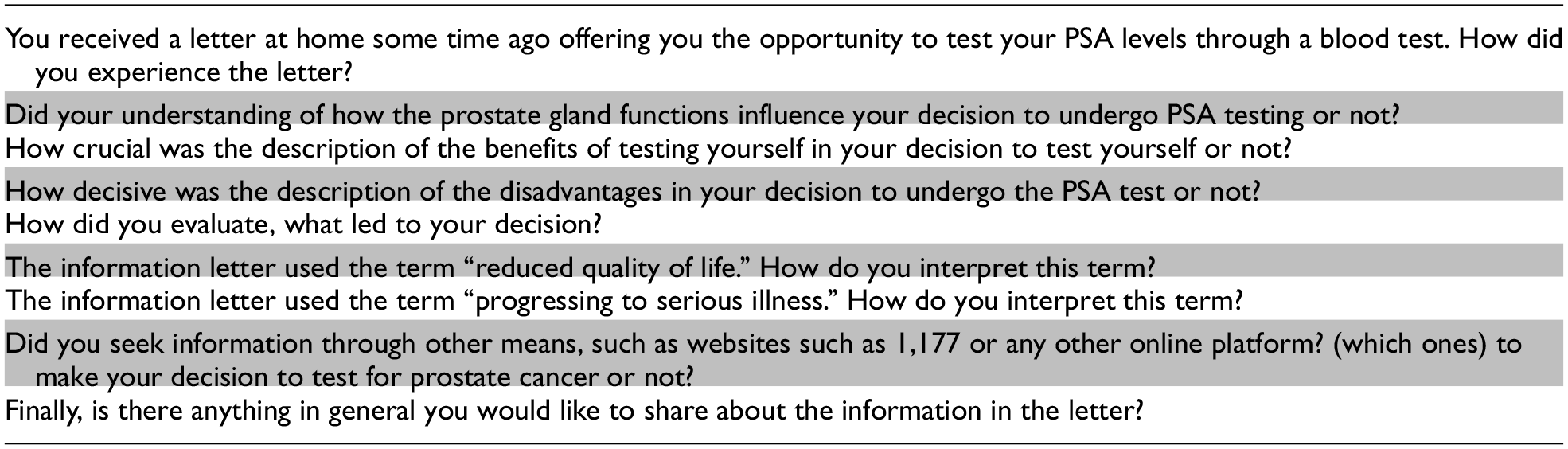
Note. PSA = prostate-specific antigen.
Ethics
Verbal consent was obtained just before the start of the interview. The men were informed that their interview data would be pseudonymized before it was published, that they could withdraw their information before it was published, and that they could interrupt the interview anytime during the interview session. The study was approved by the Ethics Review Authority (2020–00699).
Data Analysis
Data were analyzed using qualitative content analysis. The inductive method was used because it is used to describe phenomena within an area where the knowledge is limited, and the data provide a direct analysis of the individual’s description of the phenomena (Graneheim et al., 2017; Stenfors et al., 2020). Initially, the anonymized transcribed material was read several times by the LS to become familiar with the data. It was then broken down into meaning units that contained sentences relevant to the study, which were organized in Microsoft Excel. These meaning units were further condensed into denser units, which meant removing unnecessary words while preserving the core content. In both steps, this condensation was done with minimal abstraction and interpretation to preserve the participants’ own phrases. The condensed units were further shortened into codes consisting of single words or short phrases and organized into subcategories where similar topics were discussed. The subcategories were organized by colors to facilitate recognition of patterns that could be used when constructing categories (Graneheim & Lundman 2004; Graneheim et al., 2017; Lindgren et al., 2020). The analysis was initiated by LS which the condensation at each step; the coding and the interpretation were discussed with the last author (KS, behavioral scientist), who enriched the analysis and discussion to consensus.
Results
The average age of the 18 interviewed men was 52 years (range 50–62 years). Ten of the men had chosen to take a PSA test in the OPT program, and eight had declined testing. Four categories were identified from the content analysis that answered the research question. To highlight the study results presented below, we have selected representative participant quotes.
Expectations That Authorities Should Take Responsibility
Men described a collective image and a belief that the healthcare provider has the ultimate knowledge and should provide guidance as the basis for the decision; the decision should not be left to the individual man. One aspect that was evaluated was the risk of suffering from prostate cancer later in life and then “finding yourself in a difficult situation” if they now declined the offer of a PSA test. Some men described their experiences, such as annual health checks or the presence of chronic illness, as having a significant impact on their personal decisions. Prior experience from healthcare was valued and described as a sense of security that neutralized the question of testing one’s PSA or abstaining. The men appreciated the invitation to organized testing and that the healthcare system considered PSA testing to be an important measure to detect prostate cancer in time. The fact that the healthcare system offered testing and thereby showed that this was prioritized was valued as a reason in itself to be tested. Several men described feeling “called upon and chosen” and in regard to the decision, this trumped the information in the invitation letter, which described advantages and disadvantages. Men described that the invitation, in combination with pre-assigned healthcare centers, made it more likely that men chose to get tested.
Interview 5: Want to… I don’t care about the pros and cons of… But I just wanted to be informed that I don’t have it, or that it is discovered in time.
Men described a high level of trust in the healthcare system and the belief that they would receive adequate care and treatment if prostate cancer would be diagnosed. Some men felt that no disadvantages of the PSA test should be described in the invitation letter without also describing how the research is progressing and reassurance that, in the case of a prostate cancer diagnosis, they’d be taken care of.
Fear: A Driving Force and a Barrier
Fear was described as both a driving force and a barrier in the screening decision. The uncertainty aspect about the possible future threat of a late detected, advanced prostate cancer was valued in some men’s personal decisions. The fear of missing their chance of curative treatment was a driving force, whereas the fear of an unpleasant or painful physical examination (e.g., biopsy) was a barrier. Most men, on the other hand, described the frame of reference as how bad things can get if you don’t find cancer in time, and that this was a driving force.
None of the men mentioned that their decision was affected by an increased risk of prostate cancer due to family history. Men valued the fear of losing masculinity and physical sexual function because of treatment side effects in the decision-making process, as these possible consequences were seen as a threat to their quality of life.
Interview 18: As I also understood it, it is the romantic relationship with the girl that can deteriorate… but it could be explained a little more clearly perhaps…. Maybe you don’t dare to ask that either…without feeling ashamed. Interview 17: This relates to male ideals, where the expectation is that the penis must function properly; otherwise, one is not considered a real man.
The fear of cancer in the absence of a PSA test was assessed and weighed against the fear of abnormal test results. For men who valued the disadvantages more than the advantages as described in the OPT invitation letter, the decision was also driven by a fear of getting a “no-treatment-requiring prostate cancer” and “living with it.” The thought of having to face possible negative news about prostate cancer was disheartening.
Intuition and Social Support
Men who felt insecure in the decision-making process described methods of seeking social and emotional support from people close to them. Those who lived with a partner valued their partner’s opinion as a rich source of discussion. Single men sought support by discussing with friends or colleagues, and were influenced by how these people said they would have acted in the same situation.
The men described their approach to the PSA test decision as following a pattern similar to that of other decision processes involving complex dilemmas.
Men who had strong confidence in their own decision-making described their “gut feeling” guiding them. They already had a firm idea of what was right and wrong about screening and had made their decision without evaluating the available information.
Interview 14: I think that was the decisive factor in the end, so to speak…. I don’t know where I would have landed if I hadn’t discussed it with my wife.
Some men described an avoidance strategy. The thoughts were based on a wishful thinking pattern of not being affected by prostate cancer. Reasoning such as “you don’t feel bad about what you don’t know” was valued in their personal decision. The men who held a positive attitude toward PSA testing and possible subsequent examinations for prostate cancer held an attitude of “attack is the best defense strategy.”
Interview 16: Yes, it was more of an approach, so to speak, to life, and it’s generally about the fact that it doesn’t work with an ostrich mentality. But as a person who has my need for control, it usually ends with wanting to lift as many stones as possible.
A few men highlighted their way of thinking about one thing at a time. First, about the PSA test, then any further investigation, and finally, the later consequences were described in that order. This meant they were now focusing on the PSA test instead of any subsequent consequences.
Accessing Information and Evaluating One’s Personal Risk
Men described a complex picture where different layers of information, general and detailed, were important for a complete understanding of the information in the invitation letters. A prominent aspect of the decision to refrain from testing was that the information about advantages and disadvantages was perceived as unclear and difficult to evaluate on a personal level. Some of the men wanted the information presented in percentages and shares to be able to assess their own risk of being affected. These men described a habit from their working life of interpreting and making decisions based on such types of data.
Most men perceived the information about disadvantages, especially the information about overdiagnosis, as difficult to understand. Also, men considered it common knowledge that it is desirable to find cancer at an early stage.
Men who felt they understood the information about advantages and disadvantages expressed confidence in their decision. Men who had previously taken a PSA test did not describe any deep understanding of the term overdiagnosis but rather a certainty that they had made the right choice.
Interview 9: Also, cancer in all its forms, is surely something where the prognosis becomes more favorable the earlier you discover and can take measures. Interview 8: I sort of understand that this can be good as well and I’m in favor of screening, I think it’s a good idea in general. It was just that this just…. Yes. It raised questions in me and I didn’t really understand and then I did nothing.
Some men described that the limited research-based knowledge and the negative attitude of health authorities toward a full-scale screening program made it particularly difficult to know what decision to make. This also contributed to doubts about whether OPT was reliable.
Discussion
Our study is the first to describe which aspects men value in their personal decision-making process when invited to a population-based prostate cancer screening program without a healthcare provider as a discussion partner. Our findings indicate that the information provided in the invitation letter was not decisive in the men’s decision to undergo testing or to abstain. Instead, their choices were primarily influenced by personal experiences and values.
The organized approach and the interpreted clear signal from the healthcare provider played a decisive role in the men’s decision-making process. Men described relying on the healthcare provider’s expertise and preferred guidance in making decisions about PSA testing. Men preferred that healthcare had taken a more active role in the decision to screen, especially for complex and potentially life-changing tests such as the PSA test.
Professional organizations advocate shared decision-making, weighing the advantages and disadvantages of screening for PSA testing. Where the recommendation emphasizes shared decision-making (U.S. Preventive Services Task Force, 2018). In line with this, men in the interviews described the offer of a PSA test as an expression of the healthcare provider’s recommendation, which made them feel “selected” and therefore more likely to undergo the test. Furthermore, these men, particularly those with previous positive experiences of the healthcare system, tended to have a higher level of trust in medical recommendations. The purpose of providing information about the potential advantages and disadvantages of screening is to enable individuals to make an informed decision, which is a core principle of the Swedish OPT and similar programs. The healthcare provider’s view that men’s decision whether to be screened is based on an informed decision is merely an illusion if, in reality, personal values trump rational weighing of the objective advantages and disadvantages against each other (Jepson et al., 2005; Marteau & Dormandy 2001). Similar results have been reported in European studies where the invitation to screening is seen as an assurance that the test is both important and recommended by the healthcare system (Jauernik et al., 2023).
An aspect that weighed heavily in the men’s decision-making process was their fear of the clinical examinations required in the case of elevated PSA levels, and the concern that an undetected cancer could develop into an incurable disease if not detected early. Similar reasoning has been observed in a study on colorectal cancer screening, which showed that fear of cancer can influence the decision to participate in screening, and that expectations of physical discomfort can be a barrier to participation (Vrinten et al., 2015). In our study, men expressed concern about the physical discomfort associated with a rectal examination and reluctance to expose private parts of their bodies, which led some to opt out of the testing. At the same time, men expressed concern about a potential future cancer diagnosis as a motivating factor for participation in OPT, where the decision to participate was seen as a way to seek reassurance and reduce fear of prostate cancer, both now and in the future.
An American study with participants from different ethnic backgrounds reported that both low and high fear of prostate cancer were associated with lower participation in PSA testing (Consedine et al., 2006). Similar findings have been observed among women facing the choice of breast cancer screening, where cancer was described as the greatest health fear, and this fear promoted participation in screening (Consedine et al., 2004). Research has shown that the fear of cancer is widespread in the Western world and is deeply rooted in society, particularly since cancer has become one of the leading causes of death (Smith et al., 2018; Svendsen et al., 2013). Considering this, it seems reasonable that fear may play a role as both a driving force and a barrier.
Men who were unsure about testing actively sought support from a trusted person, as previous research on social support in health decisions also describes: the partner’s opinion often becomes crucial due to emotional support within the relationship (Shaw et al., 2023). Our findings emphasize the need to understand how interpersonal relationships influence screening decisions and suggest that including partners in discussions can aid the decision-making process. Men in relationships saw their partner’s opinion as central, likely because of the natural environment for discussion that partnerships provide. Single men sought advice and support from friends or colleagues, suggesting that social networks play an important role for this group. Men sought discussions focused on past screening experiences and their outcomes. A stepwise approach to decision-making was described, focusing on one aspect at a time.
First, they considered the PSA test, then any further investigations, and finally, the long-term consequences. When implementing a screening program that advocates personal decision-making (Jepson et al., 2005), care is needed to address the fact that long-term considerations are not necessarily related to the initial decision. This stepwise decision-making process means that decisions are initially focused on the test itself, while potential future consequences receive less attention. Men who felt they understood the information about advantages and disadvantages expressed confidence in their decision. Those who had previously undergone a PSA test did not show a deep understanding of overdiagnosis but were confident in their decision and had made the right choice. This is consistent with the concept of confirmation bias (Nickerson, 1998). Once a decision, such as whether to undergo screening or not, has been made, individuals tend to dismiss or undervalue information that contradicts their choice, focusing instead on that which confirms it. In contrast, some men expressed that they let their intuition guide them and had a preconceived, fixed idea of what was right for them. Similar results have been reported from a colorectal cancer screening study in the Netherlands (Douma et al., 2020).
Several men found the information about the advantages and disadvantages of screening unclear and difficult to assess personally, especially regarding the risk of developing prostate cancer requiring treatment, which influenced their decision to decline testing. The information on overdiagnosis was particularly difficult to understand. The men referred to the generally accepted belief in society that early cancer detection is of great importance, as described in a similar study (Smith et al., 2018; Svendsen et al., 2013). Men who were used to interpreting information based on percentages and numbers, often based on work experience, expressed a desire for such formats to be used in information materials to better assess their own risk.
Our previous survey within the same OPT program also showed that men with higher education (university level) found the description of the disadvantages of PSA testing less clear compared to men with less education (Svensson et al., 2023). A possible explanation could be that men with higher education more often base their decisions on data presented in numerical form.
Another factor that contributed to the uncertainty was the limited research-based knowledge and the restrictive attitude of the Swedish health authorities to a full-scale screening program. This casts doubt on the reliability of organized prostate cancer screening, further complicating the decision for some men. Other studies show how decision-making is influenced by the individual’s understanding of the information, how it is presented and how the decision-making process takes place (Bell et al., 2014; Lin et al., 2008).
Strengths of our study include the recruitment of men from a population-based program, where participants had an equal chance of being invited to interviews. This ensured that the sample was representative in terms of age, previous PSA testing experience, and marital status. Another strength is the rich data obtained from the interviews, which provided a high level of informational power (Malterud et al., 2016).
The study has some weaknesses as well. Participants had to respond to the invitation via email, which may have limited participation due to language barriers or a lack of email access. The results may therefore not be representative of the entire target population for prostate cancer screening, which includes men from various cultural backgrounds. The low proportion of men who responded positively to the interview request may also have reduced the representability of the interviewed men. Furthermore, we did not stratify the interviewed men by their cultural background or educational level. A limitation is that OPT is not a nationally implemented screening program, which might have led men to feel they needed to “seize the opportunity” to get a PSA test. In a national screening program, men would know that the test would be offered regularly. Our findings are also limited to countries with cultural and healthcare systems similar to Sweden’s, as the type and amount of relevant information, as well as trust in the healthcare system and authorities, may vary between countries and cultural contexts.
Conclusions
In this Swedish OPT program, men did not view the information in the invitation letter about the potential advantages and disadvantages of PSA testing as decisive for their decision. Instead, they many based their decision on intuition and personal factors, and social support. Our findings show a need for further research into men’s various decision-making strategies. As a potential national screening program would target all men of certain ages, it is crucial to explore how men from diverse cultural backgrounds respond to this invitation to better understand how the individual decision-making process is influenced by factors such as assessment of personal risk, perception of advantages and disadvantages, and cultural background, as well as how to optimize the information to the invited men.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883251344563 – Supplemental material for Prostate Cancer Screening Decisions: Which Aspects Do Men Value Most? An Interview Study With Men Invited to a Population-Based Program
Supplemental material, sj-docx-1-jmh-10.1177_15579883251344563 for Prostate Cancer Screening Decisions: Which Aspects Do Men Value Most? An Interview Study With Men Invited to a Population-Based Program by Linda Svensson, Ola Bratt, Jonas Hugosson and Karin Stinesen in American Journal of Men's Health
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was conducted by the Märta and Gustaf Ågrens Foundation at the Department of Urology, Sahlgrenska University Hospital, and by the Swedish State under an agreement between the Swedish government and the county councils (the ALF agreement). The sponsors played no role in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.