
Abstract
This study aims to evaluate the clinical efficacy of acupuncture and moxibustion in CP treatment and assess the quality of clinical literature. Controlled clinical trials (CCT) and randomized controlled trials (RCTs) from PubMed, Web of Science, NLM, CNKI, and Wanfang (January 2003 to January 2023) were analyzed. Relevant data were extracted and statistically analyzed using RevMan 5.1 software. Twenty high-quality papers (JADAD≥3) involving 1,661 patients were included. Meta-analysis showed a significant difference in the overall response rate between the test and control groups in CP treatment (odds ratio [OR] = 4.08 [95% CI = 3.13, 5.33], p < .001). The National Institutes of Health–Chronic Prostatitis Symptom Index (NIH-CPSI) posttreatment comparison showed significantly better symptom improvement in the acupuncture and moxibustion group (mean difference [MD] = –4.87 [95% CI = −6.145, −3.59]). Acupuncture and moxibustion significantly improve response rates and symptom scores in CP treatment compared with control treatments (drugs, sham acupuncture). This suggests that acupuncture and moxibustion are effective for CP and worth promoting, though further exploration of their mechanisms is needed.
Introduction
Chronic prostatitis (CP) refers to a disease in which the prostate is dominated by symptoms such as abnormal urination, poor urination, and perineal and lower abdominal pain under the action of infectious factors (Andrology Branch of Chinese Association of Traditional Chinese Medicine Information, 2020). Due to its complex etiology and unclear pathogenesis, no uniform treatment is currently available (C. Z. Liang et al., 2009).
The treatment of CP is characterized by long treatment cycles and hefty treatment costs, which bring massive psychological and economic burdens to patients (Trinchieri et al., 2007). Due to the complexity of symptoms, some patients experience changes in sexual function, resulting in anxiety and some difficulties in the clinical treatment of this disease (Trinchieri et al., 2007). In recent years, clinicians have conducted more in-depth clinical studies on acupuncture and moxibustion treatment of CP, confirming that acupuncture and moxibustion boasted advantages in the treatment of CP, and have achieved satisfactory results, showing unique efficacy in improving symptoms and enhancing the quality of life (Chen, Liu, et al., 2016). Therefore, this article collects literature on controlled clinical trail (CCT) and randomized controlled trial (RCT) comparing acupuncture treatment for CP with Western medicine treatment and proposes to perform quality evaluation and meta-analysis, so as to evaluate the efficacy and safety of acupuncture and moxibustion treatment for CP while providing a reference basis for future clinical treatment.
Materials and Methods
Literature Retrieval Strategy
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) instruction manual, databases dated from 1 January 2003 to 1 January 2023 were systematically retrieved, including three English databases, that is, PubMed, Web of Science, and The National Library of Medicine (NLM), and two Chinese databases, that is, China National Knowledge Infrastructure (CNKI) and Wanfang Database. The retrieval strategy as follows: Chronic prostatitis AND (acupuncture OR moxibustion OR electroacupuncture). Chinese: 慢性前列腺炎 AND (针灸 OR针刺 OR 艾灸 OR 电针).
An ethics statement is not applicable because this study is based exclusively on published literature.
Literature Inclusion and Exclusion Criteria
The original literature should be retrieved for relevant CCTs and RCTs that meet the requirements per the examination guidelines established by the International Cochrane Collaboration (Jadad et al., 2000). (a) Randomization method (random number table computer random sequence) is a strict random method, with lotteries, coin flipping, and dice rolling defined as “adequate” random method and other methods like admission order and visit order as semi-random or quasi-random; (b) Allocation concealment includes the use of numbered containers, telephone or fax controlled by the study site, and the sequence number placed in sealed and opaque envelopes as the “correct and adequate” concealment method, with other methods deemed “inadequate or incorrect.” Mentioning the allocation concealment without further description is defined as “unclear,” with neither mentioning nor describing the allocation concealment as “not used”; (c) Whether the patients included in the study are followed up, and whether the follow-up time is long enough; (4) Blinding: blinding should be applied in evaluating the outcome of this type of disease, so as to reduce measurement bias.
Inclusion criteria
(a) Clinical research literature on acupuncture and moxibustion treatment of CP published in well-known medical journals from January 2003 to January 2023; (b) CCTs and RCTs of acupuncture and moxibustion treatment of CP; (c) acupuncture and moxibustion treatment is the main therapy in the test group, while the control group mainly utilizes basic drug treatment, sham acupuncture, or other acupuncture methods; (d) clear diagnostic criteria are available, NIH Chronic Prostatitis Symptom Index (NIH-CPSI) total score > 15 (scale 0–43), and symptoms for 3 months during the previous 6 months (Krieger et al., 1999); (e) efficacy determination indicators: response rate and NIH-CPSI. Sham acupuncture was a therapy protocol included the same number and type of needle, duration, and frequency of sessions as for the acupuncture treatment, but the treatment was delivered superficially at nonacupuncture points 15 mm to the lateral of each corresponding acupuncture point. The points were not stimulated electrically, but the sound of the pulse generator was heard by the participants.
Exclusion criteria
(a) Various reviews, targeted etiologies, mechanisms, and diagnostic studies; (b) case reports, physician experience reports; (c) various dissertations for, conference proceedings; (d) animal research literature; (e) research literature on acupuncture as an adjuvant therapy with other therapies for the treatment of CP; (f) low-quality literature (JADAD score < 3); (g) republished literature.
Literature Screening and Data Extraction
Two researchers independently screened the literature performing preliminary screening through titles and abstracts first, followed by a secondary screening by reading the full text per the inclusion and exclusion criteria. For any inconsistent opinions, the opinions of the third researcher were solicited and discussed to reach a consensus. After literature screening, two researchers independently extracted data from contents as follows: (a) basic characteristics of the included studies: first author, year of publication, country of publication, randomization method, sample size, blinding, baseline comparability, interventions, and efficacy determination criteria; (b) outcome indicators: overall response rate and NIH-CPSI. The outcome indicators we have defined in the article which first is the NIH-CPSI, its total score and pain symptom score: the score index was composed from nine aspects. Items 1 to 4 were used to measure pain or discomfort of patients, with 0 to 21 points, including pain frequency 0 to 5 points, pain site 0 to 6 points, and pain degree 0 to 10 points. Items 5 to 6 are the symptoms of urination, 0 to 10 points; Items 7 to 9 are quality-of-life scores, ranging from 0 to 12 points. A higher total score indicates a more severe condition. The second is “Overall response rate,” it refers to the prostatitis efficacy evaluation criteria in Prostatitis (Y. Guo & Li, 2007). Clinical recovery: score improvement rate ≥ 90%; obvious effect: score improvement rate ≥60% and <90%; effective: integral improvement rate ≥30% and <60%; Invalid: Score improvement rate < 30%. Score improvement rate = [(pretreatment CPSI score – posttreatment CPSI score)! Pretreatment CPSI score] "100%.
Literature Quality Evaluation
The literature meeting the criteria was evaluated with JADAD quality score (Jadad et al., 1996): (a) 2 points for randomization, 2 points for correct randomization, and 1 point for descriptive randomization; (b) 2 points for blinding, 2 points for specific implementation method of double-blind, 1 point for double-blind only described by the author, and 0 points for nonblind; (c) 1 point for withdrawal, and 0 points for not mentioning it. 1~2 points for low-quality literature, and 3~5 points for high-quality literature.
Statistical Analysis Methods
Meta-analysis was performed using Revman 5.3 software. Odds ratio (OR) and weighted mean difference (WMD) were used as the effective index for enumeration data and measurement data, respectively, and each effect size was presented as the point estimate and 95% confidence interval (CI). Moreover, a heterogeneity test was performed with the I2 test to determine the heterogeneity, and the included literature was considered homogeneous if I2 < 50% or p > .1, with the fixed effect model (Mantel–Haenszel) then used for analysis; if I2 > 50% or p≤ 0.1, the included literature were considered somewhat homogeneous, with the random effect model (DerSimonian-Laird) was then used for analysis. The significance level of the Meta-analysis was set as α = .05.
Results
Literature Retrieval Results
A total of 382 relevant papers were retrieved for this study, and after the systematic screening, 20 papers that met the criteria were finally included (W. Chen et al., 2011; D. Chen et al., 2012; Chen, Xiang, et al., 2016; Feng & Lu, 2009; S. Guo & Wang, 2018; Huang et al., 2015; Huo, 2020; S. W. Lee et al., 2011; S. H. Lee & Lee, 2009; B. Li et al., 2023; Liang, 2020; J. Liu et al., 2013; Qin et al., 2018; Sahin et al., 2015; Wang et al., 2014; Xia et al., 2020; Xie et al., 2021; Xu & Xu, 2013; Yang et al., 2018; Zhang et al., 2018) for meta-analysis and systematic review. The flow chart of literature retrieval and screening is shown in Figure 1.

Literature Retrieval and Screening Flowchart
Basic Characteristics of Included Literature
The basic characteristics of the included literature are shown in Table 1. A total of 1,661 subjects were included in 20 papers, including 842 subjects in the test group and 819 subjects in the control group. Of these papers, 18 were from China and two each from Malaysia (S. H. Lee & Lee, 2009) and Turkey (Sahin et al., 2015).
The Basic Characteristics of Included Studies and the Literature Quality Ratings

Note ① = National Institutes of Health-Chronic Prostatitis Symptom Index (NIH-CPSI) Score; ② = Guidelines for Clinical Research of New Drugs of Traditional Chinese Medicine; ③ = Diagnostic and Therapeutic Criteria for Syndrome Differentiation of TCM; ④ = Clinical Diagnosis and Treatment Specification for Chinese Acupuncture and Moxibustion.
Abbreviations: N/M = Not Mentioned; A&M = Acupuncture and Moxibustion; ACU = Acupuncture; TCM = Traditional Chinese Medicine; WM = Western Medicine; S-ACU = Sham Acupuncture; E-ACU = Electroacupuncture; MIC=Microwave.
Interventions
Various acupoint selection methods have been applied in the treatment of chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS), involving 25 different acupoints and eight meridians. These meridians include the bladder meridian of foot-taiyang, ren meridian, kidney meridian of foot-shaoyin, gallbladder meridian of foot-shaoyang, spleen meridian of foot-taiyin, liver meridian of foot-jueyin, large intestinal meridian of hand-yangming, and triple energizer meridian of hand-shaoyang. Some commonalities were observed among acupoint selection studies. The lumbosacral region and lower extremities are the primary targets for acupuncture points. The most frequently used meridians were the bladder meridian of foot-taiyang, ren meridian, and spleen meridian of foot-taiyin. SP6 (Sanyinjiao) was the most frequently used acupoint, followed by BL33 (Zhongliao), BL35 (Huiyang), and BL23 (Shenshu). The acupuncture treatment process is generally standardized among the studies, with each needle performing a rapid twisting maneuver at a frequency of about 200 r/min, adjusted according to the patient’s age, physique, and other conditions. However, the frequency of acupuncture sessions varies, with some studies using treatments 3 times a week for 4 weeks, and others using daily treatments for 12 days per course.
For the test group, there were 15 papers on CP treated mainly with acupuncture alone (D. Chen et al., 2012; Chen, Xiang, et al., 2016; Huo, 2020; S. W. Lee et al., 2011; S. H. Lee & Lee, 2009; B. Li et al., 2023; J. Liu et al., 2013; Qin et al., 2018; Sahin et al., 2015; Wang et al., 2014; Xia et al., 2020; Xie et al., 2021; Xu & Xu, 2013; Yang et al., 2018; Zhang et al., 2018), of which G. Chen, Xiang, et al. (2016) also used acupuncture combined with Western medicine for the treatment of CP; there were three papers on CP treated mainly with acupuncture and moxibustion alone (Feng & Lu, 2009; S. Guo & Wang, 2018; Huang et al., 2015), one paper on CP treated with acupuncture combined with traditional Chinese medicine by W. Chen et al. (2011). Liang (2020) used electroacupuncture combined with Western medicine for the treatment of CP.
The control group mainly used drug therapy and sham acupuncture, and there were three papers on CP treated with traditional Chinese medicine (W. Chen et al., 2011; Huang et al., 2015; Xu & Xu, 2013), seven papers on CP treated with Western medicine (Chen, Xiang, et al., 2016; Feng & Lu, 2009; S. Guo & Wang, 2018; Liang, 2020; J. Liu et al., 2013; Wang et al., 2014; Xia et al., 2020), nine papers on CP treated with sham acupuncture (Huo, 2020; S. H. Lee & Lee, 2009; S. W. Lee et al., 2011; B. Li et al., 2023; Qin et al., 2018; Sahin et al., 2015; Xie et al., 2021; Yang et al., 2018; Zhang et al., 2018), and one paper in which the control group was treated with microwave therapy (D. Chen et al., 2012).
Baseline Comparability
Feasibility results for baseline data were reported in all 20 papers. As shown in Table 1, all included papers were baseline comparable.
Blinding
Of the 20 papers, three did not mention the specific implementation method for blinding (D. Chen et al., 2012; Huang et al., 2015; Wang et al., 2014), with the unclear blinding method for four papers (Huo, 2020; J. Liu et al., 2013; Xu & Xu, 2013; Zhang et al., 2018).
Randomization Method
Of the 20 papers, 16 met the RCT randomization criteria (W. Chen et al., 2011; D. Chen et al., 2012; Chen, Xiang, et al., 2016; S. Guo & Wang, 2018; Huang et al., 2015; S. W. Lee et al., 2011; S. H. Lee & Lee, 2009; B. Li et al., 2023; Liang 2020; J. Liu et al., 2013; Qin et al., 2018; Sahin et al., 2015; Wang et al., 2014; Xia et al., 2020; Xie et al., 2021; Yang et al., 2018) and four met the CCT randomization criteria (Feng & Lu, 2009; Huo, 2020; Xu & Xu, 2013; Zhang et al., 2018).
Literature Quality Ratings
Since papers with a JADAD score < 3 were excluded at the preliminary screening, the ratings of treatment evaluation were between 3 and 5 for the included literature. Of these, eight papers (S. Guo & Wang, 2018; S. H. Lee & Lee, 2009; S. W. Lee et al., 2011; B. Li et al., 2023; Liang, 2020; Qin et al., 2018; Sahin et al., 2015; Xie et al., 2021) scored 5 points, nine (W. Chen et al., 2011; Chen, Xiang, et al., 2016; Feng & Lu, 2009; Huo, 2020; J. Liu et al., 2013; Xia et al., 2020; Xu & Xu, 2013; Yang et al., 2018; Zhang et al., 2018) scored 4 points, and three (D. Chen et al., 2012; Huang et al., 2015; Wang et al., 2014) scored 3 points.
Meta-Analysis Results of Acupuncture and Moxibustion Treatment of CP
Overall Response Rate of Acupuncture and Moxibustion Treatment of CP
A forest plot of a meta-analysis of the overall response rate of acupuncture and moxibustion treatment of CP is shown in Figure 2A. The findings from the analysis of 20 included papers revealed a significant difference in the overall response rate between the test group and the control group (Z = 10.34, p < .001). Moreover, heterogeneity evaluation showed low heterogeneity across studies (I2 = 4%), with the pooled statistics calculated with the fixed effects model. Meta-analysis showed that the test group treated with acupuncture and moxibustion saw a higher overall response rate than the control group (OR = 4.08 [95% CI = 3.13, 5.33]).
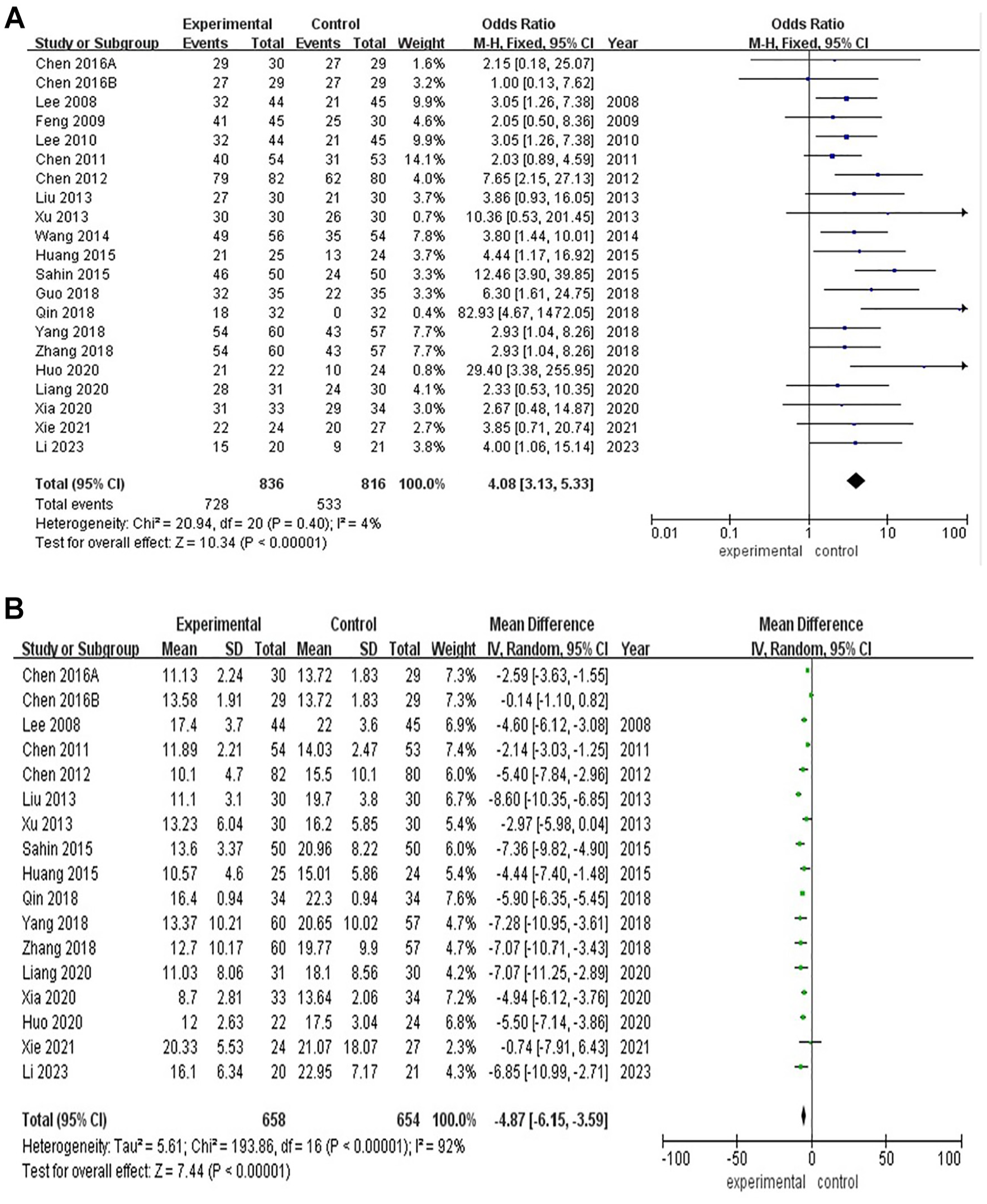
(A) Meta-Analysis Forest Plot of the Overall Effective Rate of Acupuncture in the Treatment of Chronic Prostatitis. (B) Meta-Analysis Forest Map of NIH-CPSI After Acupuncture Treatment of CP
NIH-CPSI Score After Acupuncture Treatment of CP
Figure 2B presents a forest plot of a meta-analysis of the NIH-CPSI score after CP treatment between the test group and the control group in 16 papers. The NIH-CPSI score was analyzed through continuous variable analysis, with the heterogeneity test result of I2 = 92% (χ2 = 193.85, p < .001), indicating that there was robust heterogeneity between the study effect sizes, thus using the random effect model for analysis. MD (mean difference) of the combined effect sizes = −4.87 (95% CI = −6.145, −3.59), Z = 7.44 by Z test, and p < .001. The difference in NIH-CPSI score between the two groups was statistically significant, demonstrating that acupuncture treatment of CP was superior to the control group in terms of symptom improvement.
Publication Bias Analysis
An inverted funnel plot of the overall response rate of acupuncture and moxibustion treatment of CP is shown in Figure 3, which is drawn with the standard error (logarithm of OR) as the Y-axis and OR as the X-axis. Since it can be seen that the right side is a little bit beyond the funnel plot, publication bias may exist in this study.

Inverted Funnel Plot of Total Effective Rate of Acupuncture Treatment of CP
Discussion
As a Traditional Chinese Medicine (TCM) therapy, acupuncture and moxibustion include many different acupuncture therapies, such as standard acupuncture, acupuncture, electroacupuncture, mind-regulating acupuncture, acupuncture combined with Western medicine, and acupoint injection, all of which are classified as generalized acupuncture therapy (AT). Moreover, the evaluation and comparison were conducted for AT with Western medicine and sham acupuncture. Ultimately, 20 papers along with a total of 1,661 subjects were included in the study for a meta-analysis, and the differences in clinical efficacy between the AT and conventional drug therapy (TCM, Western medicine), sham acupuncture, microwave, and other methods in the treatment of CP patients were compared.
This study found that acupuncture and moxibustion treatment of CP is effective and superior to basic drug treatment, sham acupuncture, and other methods in terms of overall response rate. CP belongs to the categories of “turbid sperm,” “gonorrhea,” “white ooze,” and “stranguria due to overstrain” in traditional Chinese medicine. Clinical practice shows that although the symptoms of CP are complex and difficult to distinguish, the root of pathogenesis lies in the primary asthenia-secondary sthenia syndrome, with manifestations of deficiency of spleen and kidney, and damp invasion of lower energizer, or blood stasis due to Qi stagnation. Therefore, the treatment should focus on tonifying the deficiency to eliminate the root cause, supplemented by clearing away heat and dampness, soothing the liver to disperse blood stasis, and promoting blood circulation to remove the meridian obstruction. For the purpose of treating the disease, acupuncture and moxibustion improve the pathological state of the body and pathological tissues through the regulation of meridians, so as to improve the smooth circulation of Qi and blood in the prostate tissues. Among them, methods such as box-moxibustion or moxa-moxibustion come with a large area of action, concentrated heat, and strong penetration, which can warm the meridians and disperse cold while activating meridians to stop the pain. Modern studies have demonstrated that shown that acupuncture at Guanyuan and Zhongji points can significantly increase the serum interleukin-2 (IL-2) content and decrease the tumor necrosis factor-α (TNF-α) content in model rats, indicating an alleviated mediating inflammatory cell infiltration and reduced local inflammatory response after acupuncture treatment (T. Liu et al., 2007), which may be one of the mechanisms of inhibiting prostatitis.
Meanwhile, acupuncture and moxibustion treatment of CP is superior to basic drug therapy and sham acupuncture in terms of symptom improvement, the reasons include mechanisms as follows: first, acupuncture can reduce the expression levels of inflammatory factors such as TNF-α, interleukin (IL-6, IL-8), and prostaglandin E2 (Li et al., 2024). Second, persistent chronic pain can reduce gray matter volume and activation in brain regions such as the anterior cingulate gyrus in CP patients (Bai et al., 2017). Finally, an increase in oxidative stress products leads to nerve terminal sensitization, which serves as a key factor in the development of CP (Bai et al., 2017).
In light of the basic characteristics of the included literature, the findings of this study are relatively reliable. Despite the fact that all included literature is related to RCTs or CCTs, with a high overall quality (JADAD ≥ 3) while presenting the specific efficacy determination criteria and comparable baseline data, some of them either did not specifically report or mention the blinding method for study subjects, making it hard to determine whether there were other essential biases due to the lack of original data.
However, the unsatisfactory overall quality of literature on acupuncture for CP and insufficient multicenter studies with large sample sizes may somewhat impact the evaluation results. Therefore, future clinical study designs should be scientific, standardized, and rationalized, so as to perform clinical efficacy evaluation in a more systematic and objective way. In conclusion, differing from conventional drug therapy (TCM, Western medicine), sham acupuncture, microwave, and other therapies, the efficacy of acupuncture treatment of CP is superior to that of conventional drug therapy (TCM, Western medicine), sham acupuncture, and other methods. However, due to the unclear blinding method of some included literature and certain publication bias, more high-quality RCTs are needed to further confirm their clinical efficacy in the future. It is suggested that in future clinical studies, rigorous, multicenter RCTs with large sample sizes should be designed, and double-blind RCTs with follow-up observations should be followed up for a sufficient period of time, in an effort to evaluate the clinical efficacy of acupuncture and other therapies for CP, while also laying a solid foundation for further demonstrating the superiority of acupuncture treatment of CP.
Footnotes
Author Contributions
Conception and design: F.W. Administrative support: W.S. and D.J.K. Provision of study materials: F.W. Collection and assembly of data: Z.J.Y. and L.X.C. Data analysis and interpretation: F.C.W. and L.Q.G. Manuscript writing: All authors. Final approval of manuscript: All authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
An ethics statement is not applicable because this study is based exclusively on published literature.
Availability of Data and Materials
All data generated or analyzed during this study are included in this article.