
Abstract
The application of Botulinum toxin (Masport) in urology has a long history. We aimed to assess the effect of local Masport on improvement in patients with urethral stricture by reducing the recurrence of urethral stricture. This pilot study conducted was a double-blind randomized clinical trial with code IRCT20191222045852N1 on patients suffering from urethral stricture. Finally, 28 patients were allocated to intervention and control groups. Twelve patients received intralesional injection with Masport in addition to internal urethrotomy, while 16 patients underwent internal urethrotomy with normal saline. The Cox regression hazard model was used to evaluate the effect of treatment status on recurrence time adjusted for the age, length, and location of the stenosis, cause of the stenosis, and history of previous operations. The effect of treatment type was significant at the .05 level. The past medical history and cause of urethral stricture had a significant impact on relapse-free survival. Also, the improvement in the mean score of the EuroQol Visual Analogue Scale (EQ-VAS), International Prostate Symptom Score (IPSS), and Q-max in the group with Masport was significantly different from the group with normal saline. The internal urethrotomy with intralesional injection of Masport has a better survival prognosis than internal urethrotomy with normal saline group. Therefore, the authors suggest that, given this successful initial clinical trial, consideration be given to future studies involving the use of botox in the management of urethral strictures in conjunction with internal urethrotomy.
Introduction
Urethral strictures are caused by biopsy, urethral manipulation, catheterization, diathermy, external trauma, hypospadias surgery, radical prostatectomy, other prostate surgeries, congenital stricture, or it may occur for unknown reasons (Palminteri et al., 2013; Sögütdelen et al., 2016). During the repair of urethral injuries, extravasation of urine under the epithelium leads to an increase in scar tissue in the urethra as well as spongiofibrosis (Ayyildiz et al., 2004). Various methods such as urethral dilatation, internal urethrotomy, laser, stent implantation, and open surgery with different success rates are used for the treatment of urethral stricture (Ferguson et al., 2011; Hosseini et al., 2023). Although urethroplasty is regarded as the gold standard, it cannot be conducted in all centers due to the need for expertise, so the most common treatments include internal urethrotomy and urethral dilatation (Gallegos & Santucci, 2016). The success rate of the direct vision internal urethrotomy (DVIU) depends on the length and extent of spongiofibrosis. Internal urethrotomy is used for stenosis less than 1.5 cm in the bulbar urethra. In the postoperation dilatation, the chance of recurrence is high if it is used for a long time (for 1 year or more) (Dey et al., 2014). Low success rate, high risk of recurrence of stenosis, need for a long-term catheter, urethral stent and CIC (Clean Intermittent Catheterization) emphasize the need for new treatments (Gallegos & Santucci, 2016). The healing process of a scarring urethral stenosis can be affected by corticosteroids (such as triamcinolone), herbal medicines, transforming growth factor (TGF)-β, oligodeoxynucleotides, recombinant adenovirus, and using mitomycin (Farrell et al., 2017; Gupta et al., 2022; Li et al., 2013). The use of Botox in urology has a long history including neurogenic hyperactivity of the detrusor muscle, chronic pelvic pain syndrome, detrusor dyssynergia, urinary incontinence with sensory and motor causes. Numerous mechanisms for the effect of Botox injection have been reported in studies (Schurch & Reitz, 2004). One of them is that it directly inhibits fibroblast-to-myofibroblast differentiation in vitro and indicates its potential for use in treating wounds expected to develop into hypertrophic scars after burn or surgery. It also relaxes the scar tissue and then establishes blood flow, enabling the process of remodeling (Antunes et al., 2007; Jeong et al., 2015). Since the main cause of urethral stenosis after manipulation is scar formation, the hypothesis is that Botox injection prevents this event. We aimed to investigate the effect of topical Botox on improving or reducing the recurrence of urethral stricture in patients who tolerate internal urethrotomy.
Materials and Methods
Study Design and Participants
This pilot study was a double-blind and randomized clinical trial with code IRCT20191222045852N1. After receipt of the Ethics Committee code IR.SBMU.RETECH.REC.1397.1366 from the Deputy of Research and Technology in Shahid Beheshti University of Medical Sciences, we included men aged 19–70 years with the diagnosis of urethral stenosis who were internal urethrotomy candidates. Of total, 60 patients with urethral stenosis, who were referred to Shohada-e-Tajrish hospitals in Tehran, Iran, from April 2019 to April 2020, were included in this study. These participants were selected by availability sampling. Inclusion criteria included men over 18 years of age diagnosed with urethral stricture who were candidates for surgery for bulbar stricture. Of these, only 38 had the inclusion criteria for this study. A total of 10 patients were excluded because they did not want to participate in the study due to the lockdown by COVID-19. A total of 28 patients between aged 20 and 58 years were considered as internal urethrotomy candidates based on their history, physical examination, and radiography and cystoscopy findings. Patients were divided into two groups. A total of 12 patients underwent internal urethrotomy plus intralesional injection of Masport, and 16 patients underwent internal urethrotomy plus normal saline. At the end of the study, two patients were excluded from the control group because of lack of access. Patients who were dissatisfied with participating in the study, stenosis length of more than 1.5 cm, spongiofibrosis, acute retention, multiple stenosis, stenosis due to lichen sclerosis, active urinary tract infections, neurogenic bladder, stenosis in the penile urethra or membranous, and a history of benign prostatic hyperplasia, prostate cancer, pelvic radiotherapy, urethroplasty, more than one internal urethrotomy, and hypersensitivity reaction to any of the components of Botulinum Toxin Type A (MASPORT®500, MDPC, Iran) were excluded (Figure1).

Flowchart of the Study Step
Biographical and Clinical Assessment and Measurements
Before the operation, the patient was asked about the demographic information, history of previous operations, risk factors for stenosis, and the cause of the stenosis. Length and location of the stenosis, International Prostate Symptom Score (IPSS), voiding Q-max, and EuroQol Visual Analogue Scale (EQ-VAS) was measured and recorded in all patients. The validity and reliability questioners were confirmed in previous studies (Feng et al., 2014; Wong et al., 2017). IPSS is based on the answers to seven items about urinary symptoms and one item about the quality of life. Scores of each item are assigned points from 0 to 5. The total score range is from 0 to 35 (score 1–7 = mild, 8–19 = moderate, and 20–35 = severe).
First, the patients were examined by a reconstructive urologist, and then a list of patients who met the inclusion criteria was prepared. Patients were informed about the objectives of the study, and informed consent was obtained from them. Patients were divided into two intervention and control groups by simple random method. In this way, the type of intervention of people who wanted to participate in the study was placed in sealed envelopes. These envelopes were given to the secretary of the urology department. The envelopes were given to the patients at their choice. After hospitalization, the questionnaires were completed by a reconstructive urology fellowship student with an interview. Patients underwent spinal anesthesia and dorsal position lithotomy and underwent DVIU after cystoscopy with radial incisions by cold knife and star-like technique by a surgeon (Figure 2). Patients’ urethra was examined after dilation by a 22-inch French cystoscope. A total of 50 IU of Masport was mixed with 3 cc of normal saline and then injecting was conducted using a 22-Gauge needle at three different points in the submucosal site (12, 5, and 7 o’clock position) in the intervention group. A similar procedure was performed by injecting normal saline at the site of the urethrotomy in the control group. After surgery, an F18 silicone catheter was implanted for 10 days. After 1 month, patients were evaluated for symptoms with IPSS, voiding Q-max, and EQ-VAS. Abnormal results were considered (Q-max <15, IPSS >5, and decrease EQ-VAS). Retrograde urethrography (RUG)-voiding cystourethrography (VCUG) and ureterocystoscopy also if necessary for the required treatment were performed. Recurrence was defined as patients’ need for treatment such as dilatation or the need for catheterization. Patients were followed up for about 10 months to evaluate the duration of relapse-free survival (RFS) (Figure 3).

Radial Star-Like Incision of Urethral Stricture

Survival Curves for Botulinum Toxin and Normal Saline Groups
Statistical Analysis
The data are presented as mean ± standard deviation (SD) and percentage for continuous and categorical variables, respectively. The normal distribution of data was checked using the Kolmogorov–Smirnov test. An independent t-test was used to compare the mean of continuous variables, and the chi-square test was used to compare the distribution of qualitative variables between two groups at baseline. The Cox regression hazard model was applied to evaluate the possible effect of treatment status on recurrence time adjusted for the age, length, and location of the stenosis, cause of the stenosis, and history of previous operations and to estimate an adjusted survival curve that compares the survival time in patients who undergo intralesional injection of Masport or saline groups. A repeated measurement analysis was used to determine whether the mean score of IPSS, the mean score of EQ-VAS, and the mean score of Q-max are different before the internal urethrotomy, 1 month, and 6 months after the internal urethrotomy, significantly and to check does undergoing treatment of Masport or normal saline play any role here? All statistical analysis was performed by SPSS software (version 26.0. 2018, IBM SPSS), and the statistical significance was set at p < .05.
Results
The mean ±SD age of patients and length of urethral stenosis in the Masport group and the normal saline group were, respectively, 33.67 ± 11.15 and 38.88 ± 18.20 years and 10 ± 3.65 mm and 11.25 ± 3.11 mm (p = .349). There was no statistically significant difference between ages in the two groups (p = .39). The difference between length of urethral stricture was not significant, either (p = .349). As shown in Table 1, there were no significant differences between the two groups regarding the history of DVIU (p = .378), stricture location (p = .948), and etiology of stricture (p = .415). Moreover, complications for patients after surgery included bleeding and infection which did not differ significantly in both groups (p = .228).
Descriptive Statistics of Baseline and Postoperation Characteristics and Comparison of Characteristics Between Two Groups

Of the 12 patients who were undergoing treatment in the Masport group, three patients relapsed during the study period, whereas the nine patients were censored. Of the 16 patients who were in the normal saline group, six patients have relapsed.
The effect of treatment type was significant at the .05 level (p = .017). Figure 3 shows the estimated survivor curves for the two groups. The graph shows that the survivor function for the Masport group consistently lies above that for the normal saline group; this difference indicates that the treatment appears effective at all points of follow-up for Masport.
Notice, however, that the two functions are somewhat closer together in the first few weeks of follow-up, but thereafter are quite spread apart. This gap suggests that the treatment is more effective later during follow-up than it is early on. The average hazard rate is 0.019 and 0.022 in the Masport group and normal saline group, respectively.
According to Table 2, the hazard ratio for normal saline injection is calculated to be 2.900 times greater than the hazard ratio for Masport injection.
Results of Cox Proportional Hazards Model

The results indicate that the effect of past medical history and the cause of urethral stricture are significant at the 0.05 level. The hazard ratio for the effect of past medical history (no vs. yes) adjusted for the other variables is 0.080 (p = .000). Furthermore, after adjusting for other variables, the hazard ratio for the effect of a straddle versus other causes of urethral stricture is 0.098 (p = .002). These mean that the hazard for subjects with past medical history is higher than the hazard for subjects without past medical history, and the hazard for subjects with urethral stricture caused by straddle is lower than the hazard for subjects with urethral stricture caused by other causes.
A repeated measures analysis of variance (ANOVA) test determined that the mean score of IPSS differed statistically significantly between time points (p = .000) (Table 3). The post hoc analysis with a Bonferroni adjustment revealed that the mean score of IPSS was statistically significantly decreased from preintervention to 1-month postintervention (mean difference = 9.46, 95% CI for difference = [8.249, 11.042], p = .000) and from preintervention to 6 months postintervention (mean difference = 6.316, 95% CI for difference= [5.490, 7.142], p = .001) and increased from 1-month postintervention to 6 months postintervention (−3.33, 95% CI = [−4.747, −1.913], p = .000). The analysis of the IPSS score showed a significant interaction between time and treatment (p = .002) (Figure 4).
The Difference in the Mean Score IPSS in the Two Groups Pre- and Post-Intervention

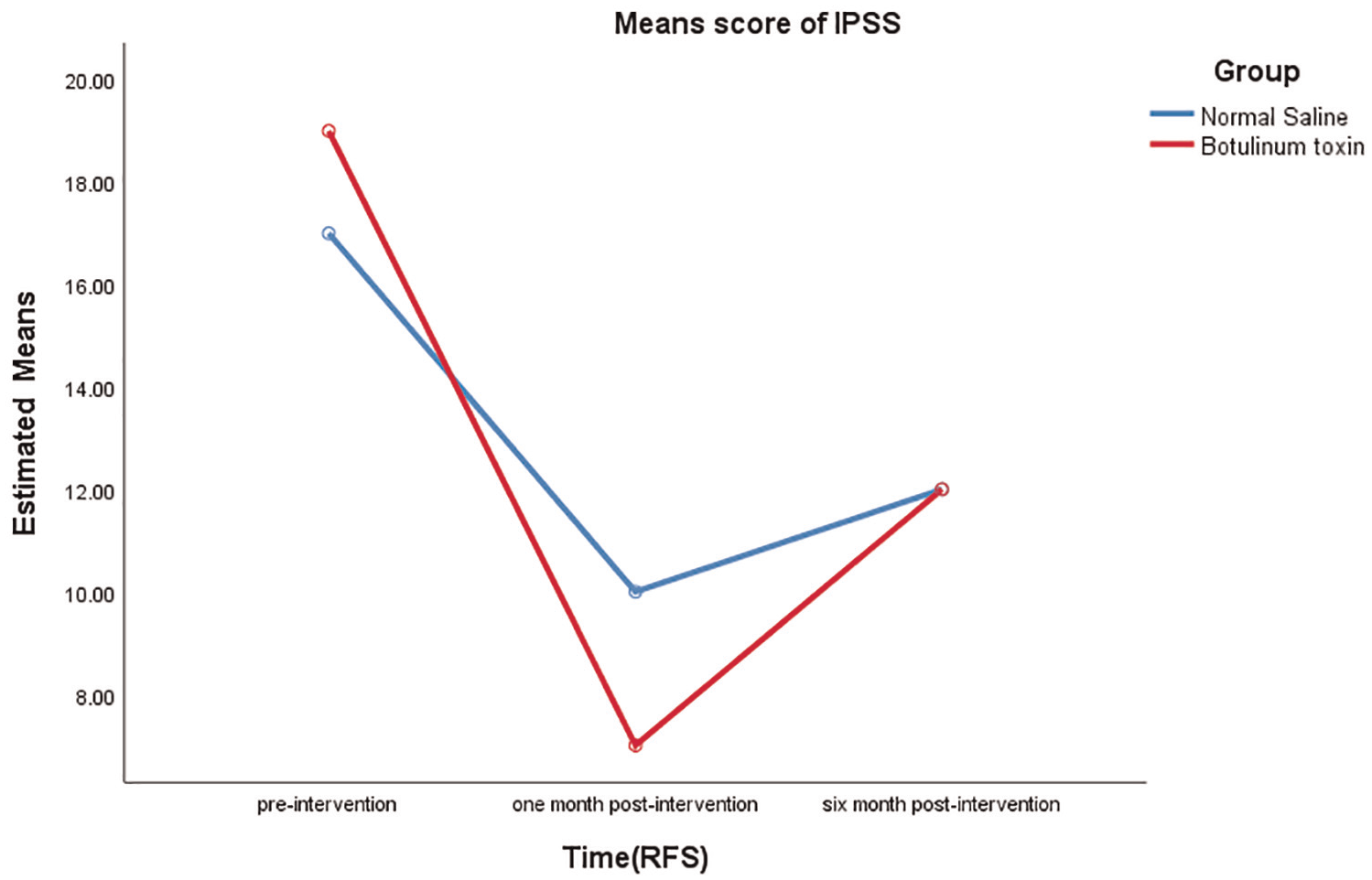
Mean Score of IPSS During the Study
The mean score of EQ-VAS also differed significantly between time points (p = .000) (Table 4). It was statistically increased from preintervention to 1-month postintervention (mean difference = −37.073, 95% CI for difference = [−41.879, −32.267], p = .000) and from preintervention to 6-month postintervention (mean difference = −22.734, 95% CI for difference = [−27.798, −17.671], p = .000) and decreased from 1-month postintervention to 6-month postintervention (14.339, 95% CI = [8.405, 20.272], p = .000). Based on the analysis, it was found that the interaction between time and treatment was significant (p = .000). After the intervention, patients who received the Masport treatment had higher EQ-VAS scores compared to those who received the normal saline treatment (Figure 5).
The Difference in the Mean EQ-VAS Score in the Two Groups Pre- and Post-Intervention


Mean Score of EQ-VAS During the Study
There is a difference between Q-max at time points, significantly (p = .000) (Table 5). Post hoc analysis with a Bonferroni correction showed that there was a significant difference between Q-max for each pair of time points. Q-max increased by 14.695 between preintervention and 1-month postintervention (p = .000) and then reduced by 6.735 between 1-month and 6-month postintervention (p = .002). The Q-max analysis showed that the interaction between time and treatment was significant. In general, patients who underwent Masport had higher Q-max than those who underwent normal saline, except at the beginning of the study (Figure 6).
The Difference in the Mean Score Q-Max in the Two Groups Pre- and Post-Intervention


Mean Score of Q-Max During the Study
Discussion
Our study examined whether injecting botulinum toxin (Masport) after an internal urethrotomy could affect the time to recurrence in patients with bulbar urethral stenosis. We compared the outcomes with those who received a normal saline injection. The results of this study showed that the degree of complication after surgery was not different in the two groups (bleeding and infection). The improvement of patients in terms of mean scores EQ-VAS, IPSS, and Q-max was higher in the group with Masport than in the group with normal saline. Also, the number of cases without recurrence and the duration of RFS during 6 months in the Masport group were higher than in the normal saline group. Shirazi and colleagues found that Captopril gel was a safe, effective agent for decreasing the recurrence rate of the urethral stricture after internal urethrotomy (Shirazi et al., 2007). This study was consistent with our study in that stenosis has a length of between 1 and 2 cm. Mitomycin C combined with DVIU is a promising way to reduce the long-term recurrence rate of a short-segment anterior urethral stricture. It is an excellent antifibrosis antigen that has been used in many fields (Xu et al., 2021).
Recently, DVIU is one of the most common methods of treating urethral stricture (Gallegos & Santucci, 2016). The success rate of this method depends on the location of the stenosis and its length, which is the best answer for stenosis in the bulbar region with a length of less than 1 cm (Pogula et al., 2021). In stenosis with a length of more than 2 cm or stenosis of the penile urethra, the success of this method is much lower, and it is not a suitable method for these patients. There are various methods to prevent recurrence and increase the success of urethrotomy, such as injecting steroids into the lesion or intermittent catheterization, where intermittent catheterization has worked better. Dilatation of the urethral by intermittent catheterization by the patient is one of the methods that is sometimes recommended to prevent the recurrence of stenosis. Other existing strategies aim to prevent scar formation (Gallegos & Santucci, 2016). One study showed that Masport prevented the increase in collagen content during urethral wound healing (Sahinkanat et al., 2009). In this study, in addition to the fact that the Masport group had a longer survival without recurrence than the normal saline group, a significant improvement in the condition of EQ-VAS, IPSS, and Q-max was also observed. Consistent with the results of this study, another study reported an improvement in the visual analogue scale after 6 months to 2 years after urethroplasty surgery (Jackson et al., 2013). Postoperative intermittent self-dilatation of a urethral stricture, primarily treated by internal urethrotomy, significantly reduces the stricture recurrence rate as well as delays the time until recurrence (Lauritzen et al., 2009). As a consequence, the authors recommended periodic dilatation and intermittent catheterization for at least 6 months in the stenosis of less than 2 cm of the bulbar urethra. Recently, two studies have been performed in Iran on the role of steroids in preventing the recurrence of urethral stenosis following internal urethrotomy. According to the initial study, injecting steroids directly into the scar tissue located at the stenosis site not only decreases the chance of stenosis recurrence but can also delay its reappearance (Mazdak et al., 2007). In the second study, injection of triamcinolone significantly reduced stricture recurrence after internal urethrotomy (Mazdak et al., 2010). Consistent with this study, the mean Q-max was increased postoperatively in another study (Isen & Nalçacıoğlu, 2015). Along with internal urethrotomy, botox injection can be considered an effective treatment option to prevent recurrence in the short term.
The strength of the study is that it is novel. This sets it apart and makes it a valuable contribution to the field. One of the limitations of this study was the dropout of patients in the follow-up phase due to their unwillingness to visit health centers due to the lockdown of COVID-19. This study required patients with specific conditions, making it challenging to find suitable participants. As a result, the method was introduced as a pilot.
Conclusion
Internal urethrotomy is a successful method for the treatment of stenosis less than 1.5 cm, the success rate of which depends on factors such as the length of the stenosis and the degree of fibrosis of the corpus spongiosum tissue. Given this successful initial clinical trial, using Masport during internal urethrotomy to improve patients’ quality of life and reduce the recurrence of stenosis, the need for CIC and dilatation after internal urethrotomy is suggested as an appropriate method. Although the study had a limited follow-up time and a small sample size, it is suggested that further research be conducted to compare the effectiveness of Masport injection followed by internal urethrotomy with urethroplasty. In addition, long-term follow-up is recommended for a more comprehensive understanding of the outcomes.
Footnotes
Acknowledgements
The authors thank all the contributors to this project. The authors also thank the staff of Shohada-e-Tajrish Hospital and the selected Social Security Hospital (12th Bahman) who assisted us in this study.
Author Contributions
HS, JH, and MFK contributed to study concept and design. RSH, AM, and SA contributed to data acquisition. EAB and KS contributed to data analysis. NN and NI contributed to drafting of manuscript. KS, JH, and AM contributed to critical revision of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
This article is taken from a disease registry titled “Establishment of a national registry system for patients undergone reconstructive urology procedures” and a project with the Ethics Committee code IR.SBMU.RETECH.REC.1397.1366, that was supported by the Deputy of Research and Technology in Shahid Beheshti University of Medical Sciences (![]() ). The authors thank the patient for their sincere collaboration. Participation in the survey was voluntary, as participants could decline to participate at any time during the study. Also, we obtained informed consent from all participants. All methods were carried out in accordance with relevant guidelines and regulations.
). The authors thank the patient for their sincere collaboration. Participation in the survey was voluntary, as participants could decline to participate at any time during the study. Also, we obtained informed consent from all participants. All methods were carried out in accordance with relevant guidelines and regulations.
Consent for Publication
Not applicable.
Availability of Data and Materials
The data sets used and/or analyzed during this study are available from the corresponding author on reasonable request.