
Abstract
Treatment of urethral stricture is a complex reconstructive urology treatment. Previous surgery in the treatment of urethral stricture increases the risk of urinary incontinence. Therefore, this study aimed to assess the outcome of comparing two preservative or nonsurgical methods, clean intermittent catheterization (CIC) or hydraulic urethral dilatation (HUD). Forty-eight patients diagnosed with symptomatic urethral stricture were enrolled in the study. Patients were randomly divided into two groups: Nelaton-based dilatation and HUD treatment. Patients were assessed using patient-reported outcome measure for urethral stricture surgery (USS-PROM) through direct clinical interview and were followed up for 12 months. The rate of urinary infection, the need for surgical intervention, and the patient’s quality of life were considered as outcomes of the interventions. SPSS software, version 20.0, was used for statistical analysis. Overall, 23 (47.9%) patients underwent HUD of stricture and Nelaton-based dilatation of stricture was done in 25 (52.1%) patients. We found that surgical intervention was required in four patients in the HUD group, but 15 patients in the CIC group required surgical intervention. Also, the need for surgical intervention and urinary tract infection (UTI) was significantly greater in the CIC group compared with the HUD group. With respect to the patient-reported outcomes, the mean Peeling’s voiding picture (Q8) and EQ-VAS score (Q16) in the HUD group (p = .02) were significantly greater than those in the CIC group (p = .02). We obtained excellent results by using an HUD catheter. This safe, simple, well-tolerated, home-based procedure reduced the need for hospital admission to operate for repeat.
Introduction
The term urethral stricture refers to the narrowing of urethra that affects three of every 1,000 men. The main causes of urethral strictures include iatrogenic urethral injury, trauma, and infection (Jackson et al., 2014; Komplikasyon & Darlık, 2016; Mirzazadeh et al., 2017). Managing urethral stricture is a challenge for urologists (Hosseini & Tabassi, 2008). Urethral reconstructive techniques include direct visual internal urethrotomy (DVIU; Pal et al., 2017), laser ablation (Razzaghi et al., 2018), urethroplasty (Hosseini & Tabassi, 2008) and the Optilume drug-coated balloon (DCB)(Elliott et al., 2022) which are selected based on the site and length of stricture, the extent of spongiofibrosis, and the surgeon’s skills (Hosseini et al., 2018). Because the treatment of proximal bulbar or membranous urethral stricture with surgeries such as transurethral prostate resection, laser prostatectomy, open simple prostatectomy, or radical prostatectomy increases the risk of urinary incontinence, clean intermittent catheterization (CIC) and hydraulic urethral dilatation (HUD) are suggested as conservative therapy in urethral stricture management.
DCB includes a combination of urethral dilation with circumferential delivery of an antiproliferative agent that hinders fibroblast growth and stricture recurrence. It is a successful method in the management of male urethral stricture (Elliott et al., 2022). However, it is impossible to do it in all conditions due to the need for patients in the operating room.
Dilatation of urethral stricture with boogies and the metal catheter has been used in practice for a long time (Lauritzen et al., 2009). Feeling of discomfort and pain, urethral injury, urinary extravasation, and secondary spongiform fibrosis persuaded urologists to abandon this procedure (Vyas et al., 2013). There are some attractive alternative techniques for the dilatation of stricture such as balloon dilatation. The main mechanism of dilation by a hydraulic catheter is gradual radial pressure to the urethral stricture sites and shearing forces made by a rigid catheter are avoided. Then, the dilation of stricture under local anesthesia may be more acceptable and less painful for patients. Moreover, less damage to the urethral wall may hypothetically reduce extravasation and subsequent spongiofibrosis and potentially lead to improved therapeutic results (Levine & Engebrecht, 1997; MacDiarmid et al., 2000; Vyas et al., 2013). Most studies on balloon dilatation are anecdotal studies and non-follow-up studies (Vyas et al., 2013). Therefore, this study aimed to assess the outcome of comparing two conservative or nonsurgical methods, CIC or HUD.
Method
Population
In December 2016, 48 patients diagnosed with a symptomatic urethral stricture, who were previously subjected to ductal dilatation (DVIU) in the operating room or other manipulations, were enrolled in the study. Patients were randomly divided into two groups: Nelaton-based dilatation and HUD treatment. After explaining the objectives of the study to patients and obtaining their informed consent, sealed envelopes were randomly provided to the patients by the secretary of the urology department. Pediatric patients, patients who were unwilling to participate in our study, those suffering from strictures immediately after distraction injury, previous radiotherapy, lichen sclerosus, malignant strictures, patients with urethral false passage or fistula, hydronephrosis, and handicap patients who were unable to perform CIC properly were excluded from the study.
Evaluations
Before dilation, all patients were evaluated with a complete urological history and physical examination. Parameters include demographic characteristics (Table 2), duration of catheterization, and previous intervention documented in the questionnaire. The cause, location, and length of the stricture were determined by retrograde urethrogram and cystoscopy.
Patients were assessed using the patient-reported outcome measures (PROMs) questionnaire for the treatment of urethral stricture with a direct clinical interview and demographic characteristics questionnaire. This questionnaire was developed and approved for the first time by a British scientist (Jackson et al., 2011). The original version of the questionnaire has been translated into several languages and its validity and reliability were confirmed (Kluth et al., 2016; Önol et al., 2017). Evaluation of the psychometric properties of the Iranian version was performed by Taybi Azar in 2020 (Fallah-Karkan et al., 2020). Content validity ration (CVR) and content validity index (CVI) were checked. CVR (0.61) (because the number of specialists was 15, this number is appropriate and acceptable according to the Lavche table) and CVI (0.97) were reported. To evaluate the reliability, two methods of determining internal consistency through Cronbach’s alpha were .84 and stability with an intracluster correlation coefficient (ICC) of .79 was used. The present questionnaire consists of 16 questions; the first six questions are about the lower urinary tract symptoms (LUTS); the seventh question is about how the LUTS affect the patient’s daily life; in the eighth question, the patient marks the number that shows her urine flow capacity in the last month; and the ninth and 10th questions show satisfaction with the outcome of the surgery. For Questions 11 to 15, the following options known as the best description of their current health status include average mobility, self-care, daily activity, pain/discomfort, and anxiety/depression. For each question, zero indicates the best and one indicates the worst status. Finally, the 16th question reports a scale (similar to a thermometer) showing the best imaginary health conditions with 100 and the worst imaginary health conditions with zero.
Urethral Balloon Catheter Dilation Protocol
In this study, patients started self-dilation with a hydraulic catheter or a catheter Nelaton after 7 to 14 days of catheter removal that was placed due to previous surgery. The reconstructive urology fellowship guided how to use a self-balloon catheter.
Self-dilation was initiated by inserting the balloon catheter in the deflated state 14 Fr unfilled (28 Fr filled), 40 cm, coudé tip, 15-cm urethral balloon catheter (Uromed industry) after applying the sterile lubricating jelly. Using a Luer-Lok 10-mL syringe, the balloon was filled with distilled water up to a maximum diameter of 28 Fr. The stopcock mechanism was engaged for inflation. The fluid was then aspirated and the device was removed from the urethra, washed with soapy water, and allowed to dry. Patients were instructed to first perform home urethra dilatation on a daily basis. The frequency of dilation was then decreased to 2 to 3 times a week by 2 to 4 weeks and then every 2 weeks for 2 to 4 months. Depending on the amount of improvement, the frequency of dilation was further decreased, increased, or terminated if necessary. The protocol of Nelaton is that first surgical dilatation is performed for patients up to 18 Fr. Then, after removing the surgical catheter, the patient begins to self-dilatation with the Nelaton 18 Fr. Each time, depending on the patient’s tolerance, the catheter stays in the urethra and then it is removed (Table 1). If the patient felt difficulty with the 18-Fr catheter, the size of the catheter would be reduced. If the catheter size was reduced to 14 Fr, the treatment would be considered a failure, and the patient would need to prepare for another surgery. The median follow-up was 12 months. Patients were initially evaluated for 1, 3, and then 12 months. A urine culture was performed if the patient became symptomatic .The success or failure of the interventions was defined based on the need for surgical interventions, the rate of urinary tract infection (UTI), and the patient’s quality of life. The primary outcome was considered based on the need for surgical interventions, the rate of UTI, and the secondary outcome of the patient’s quality of life.
Category of Home Catheterization With CIC or HUD

Note. CIC = clean intermittent catheterization; HUD = hydraulic urethral dilatation.
Statistics
SPSS software, version 20.0, was used for statistical analysis (IBM corp., Chicago, IL, USA). Data were presented as mean and standard deviation for quantitative variables and as frequency and percentage for qualitative variables. Chi-square and t tests were used to compare the dichotomous and continuous variables between the two groups, respectively. A p value less than .05 was considered significant.
Result
Our study consisted of 48 patients suffering from recurrent bulbomembranous urethral stricture disease (USD). Overall, 23 (47.9%) patients underwent HUD of stricture and Nelaton-based dilatation of stricture was done in 25 (52.1%) patients. The mean ages of patients in HUD and CIC groups were 62.43 and 65 years, respectively (Table 2).
Demographic, Treatment, and Surgical Characteristics of Patients Who Underwent HUD or CIC

Note. HUD = hydraulic urethral dilatation; CIC = clean intermittent catheterization; DVIU = direct visual internal urethrotomy; BMG = Buccal Mucosa Graft.
Transurethral manipulation was associated with the etiological factor of urethral stricture in 32.4%, and it was due to trauma in 35.1%. Other etiologies included idiopathic and infectious diseases. The mean stricture length was 1.59 and 1.72 cm in the HUD and the CIC groups, respectively (p = .56, Table 2). The most common intervention was stricture dilatation in the operating room in both treatment groups. Four and 15 patients required a surgical intervention in the HUD and the CIC groups, respectively. The need for surgical intervention and UTI was significantly greater in the CIC group compared with the HUD group (Tables 2 and 3).
Need for Surgery and the Possibility of UTI During Treatment by HUD or CIC
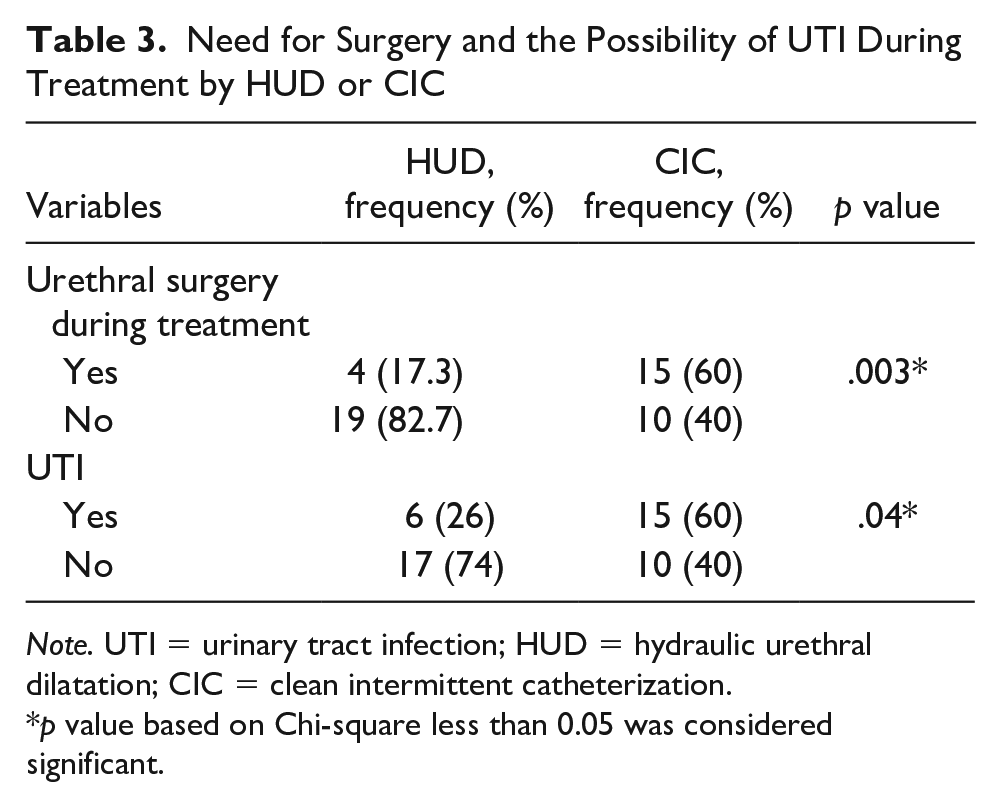
Note. UTI = urinary tract infection; HUD = hydraulic urethral dilatation; CIC = clean intermittent catheterization.
p value based on Chi-square less than 0.05 was considered significant.
The difference of six items of LUTS scores between the two treatment groups was not statistically significant (p = .1). There were statistically significant differences with regard to the mean Peeling’s voiding picture between the two groups. Seven (30.4%) patients in the HUD and 5 (20%) in the CIC groups reported that interference of urinary symptoms was not serious in their lifetime (Table 4). There were no differences with regard to EQ-5D index scores between the HUD and the CIC treatment groups (0.21 vs. 0.28). The EQ-VAS score was more significant in the HUD group (67.70% vs. 56.20%).
Patient-Reported Outcomes

Note. USS-PROM = patient-reported outcome measure for urethral stricture surgery; HUD = hydraulic urethral dilatation; CIC = clean intermittent catheterization; LUTS = lower urinary tract symptoms.
p value based on Chi-square less than 0.05 was considered significant.
Discussion
Numerous approaches are available for managing USD such as dilation with a balloon, filiform and followers, urethral sounds, or self-dilatation with catheters (Komplikasyon & Darlık, 2016). However, this is associated with high recurrence rates (Yurkanin et al., 2001).
Major risk factors for recurrence are the length and severity, which are characterized by the depth of scar tissue and spongiform fibrosis, etiology, and location of the stricture (Steenkamp et al., 1997). According to different researchers, previously treated, long, and multiple strictures with penile or pendulous areas have a higher recurrence rate (Tunc et al., 2002). A low recurrence rate with intermittent self-catheterization following surgical intervention has been reported by several authors (Levine & Engebrecht, 1997).
Using a balloon dilator in urology represents an additional endoscopic USD and bladder neck contracture (BNC) treatment. Older studies describing this technique reported up to a 41% recurrence rate (Ramchandani et al., 1994). A more recent study used a high-pressure balloon catheter, dilating the vesicoureteral stricture to up to 30 F at 30 atm with a recurrence-free rate of 80% with a 24-month median follow-up (Ishii et al., 2015). The researchers reported balloon dilation as an alternative to cold knife transurethral incision and cystoscopy dilatation which has less invasiveness and bleeding complications (Cotta & Buckley, 2017).
Steenkamp and colleagues (Steenkamp & Heyns, 1997) showed that urethral dilatation and optical internal urethrotomy under local anesthesia are successful as initial outpatient treatment. Regarding the successful performance of the procedure itself, multiple, longer (>2 cm) post-traumatic, and previously untreated strictures are better managed with dilatation, whereas patients with complications or retention are better managed with internal urethrotomy.
Several authors have found advantages for radial forces directed perpendicular to the mucosa accomplished by balloon dilation (Niesel et al., 1995). Stretching prevents contraction of the incised mucosal edges and probably increases the blood flow around the incision site, increases tissue oxygenation, and finally decreases the levels of several cytokines, such as transforming growth factor-beta, which has been shown to play a major role in the pathogenesis of fibrosis (Border & Ruoslahti, 1992). Considering this point, several authors have studied balloon dilation and its use in the management of urethral stricture, which seems to be effective and well tolerated (Levine & Engebrecht, 1997). Fishman examined 58 patients who had “excellent compliance” with balloon self-dilation and were followed up by uroflowmetry and if necessary, urethrograms (Fishman, 1992).
We used a urethral balloon catheter that provided sufficient dilation against an USD. In this study, balloon dilation led to a high success rate (80%), where recurrent strictures could be controlled by performing repeated balloon dilation. However, no patients required further treatment. Transurethral balloon dilation is simpler and less invasive than a cold knife incision. Balloon dilation also has the benefit of reducing the risk of urethral vascular damage. However, no complications were reported in our study, except for exacerbation of urinary incontinence in one (10%) patient.
In the study of Elliott et al., 2022, the Optilume DCB method was reported as a successful method. DCB includes a combination of urethral dilation with circumferential delivery of an antiproliferative agent that hinders fibroblast growth and stricture recurrence. It is a successful method in the management of male urethral stricture (Elliott et al., 2022). However, it is impossible to do it in all conditions due to the need for patients in the operating room. But in this study, we tried to reduce the need for resurgery and presence in the operating room by patient participation in the treatment process.
In this study, we proposed a urethral dilation protocol (Table 1) for treatment of recurrent bulbomembranous urethral strictures with the aim of reducing or eliminating the need for additional DVIU and/or open surgical reconstruction. Frequent dilations during the early weeks, as suggested in our protocol, help prevent early post-urethrotomy recurrences which are more resistant to endoscopic treatment alternatives (Heyns et al., 1998).
A limitation of our study was the difficulty in obtaining the patient’s hydraulic catheter due to market shortages. However, we were able to overcome this obstacle through effective coordination.
Conclusion
We demonstrated excellent short-term results by using this new catheter, which is a safe, simple, tolerable, office-based procedure that significantly reduces the need for consecutive DVIUs as well as surgical reconstruction in the management of recurrent urethral stricture. Balloon dilation appears to be a viable option for managing USD in inoperable patients.
Its efficacy should be further investigated to confirm any practical benefit of this little change in the treatment protocol for the patients. Further investigations are required in which larger sample populations should be evaluated. Individuals should be followed up for a longer period of time. Using uroflowmetry is recommended to evaluate the performance of urinary excretion and its lifelong cost-effectiveness.
Footnotes
Acknowledgements
The authors would like to thank all the contributors to this project. They would also like to thank the staff of Shohada-e-Tajrish Hospital and the selected Social Security Hospital (12th Bahman) who assisted us in this study.
Authors’ Contribution
JH, RSH, and AMM contributed to the conceptualization and design, interpretation of data, literature search and drafting, review, and editing of the manuscript for publication. KSG, SA, and RT were responsible for the conceptualization and design, data acquisition, formal analyses, interpretation of data, literature search and drafting, review, and editing of the manuscript for publication. JH supervised the study. All the authors have read the manuscript and approved the final version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
This article is taken from a disease registry titled “Establishment of a national registry system for patients undergone reconstructive urology procedures” and a project with the Ethics Committee code IR.SBMU.REC.1397.121 that was supported by the Deputy of Research and Technology in Shahid Beheshti University of Medical Sciences (![]() ). The authors would like to thank the patient for their sincere collaboration. Participation in the survey was voluntary as participants could decline to participate at any time during the study.
). The authors would like to thank the patient for their sincere collaboration. Participation in the survey was voluntary as participants could decline to participate at any time during the study.
Consent for Publication
Not applicable.
Availability of Data and Materials
The data sets used and/or analyzed during this study are available from the corresponding author upon reasonable request.