
Abstract
Few studies have investigated paternal characteristics in relationship with adverse pregnancy outcomes, and results are inconsistent. The purpose of this study was to review studies examining associations between characteristics of Black fathers and adverse pregnancy outcomes in the United States. A systematic narrative synthesis was conducted of research studies examining paternal characteristics of Black fathers in association with adverse pregnancy outcomes: preterm birth, hypertensive disorders of pregnancy, gestational diabetes, spontaneous abortion, and maternal mortality. Seven databases (Academic Search Premier, CINHAL, CENTRAL, ClinicalTrials.gov, Embase, PubMed, and Web of Science) were searched for original research articles from inception to February 2023. Articles were excluded if they (a) were in a language other than English, (b) did not describe original research, (c) included a geographic region outside of the United States, (d) did not include adverse maternal outcomes as a study outcome, (e) did not describe race of fathers in the study sample, and (f) did not describe a paternal characteristic of Black fathers. The search resulted in 210 articles. Six studies were included in the final review; five studies examined associations between paternal characteristics of Black fathers and preterm birth, finding significantly increased odds of preterm birth among births with Black fathers. Among births with non-Hispanic Black paternity, the odds of hypertensive disorders of pregnancy were reduced or not significantly associated. Researchers should continue to explore paternal factors that influence pregnancy outcomes in racial/ethnic-specific models to identify optimal intervention strategies to improve disparities in maternal and child health outcomes.
Introduction
Black women in the United States have a two to three times greater risk of dying from pregnancy or childbirth-related complications than their white counterparts (Hoyert, 2023). According to the Centers for Disease Control and Prevention (CDC), from 2019 to 2020, maternal mortality rates for non-Hispanic Blacks increased by a significant 17%, compared with 2.6% for non-Hispanic white women (Hoyert, 2023). Adverse pregnancy outcomes (APOs) such as preterm birth (PTB) and hypertensive disorders of pregnancy (HDoP) are often linked to mortality outcomes and reflect similar racial disparities. Preterm birth, delivery of a live-born infant <37 weeks gestation, impacted roughly 10% of all 2020 births in the United States; in the same year, Black/African American women had a PTB rate of 14.4%, compared with 9.1% in White and 9.8% in Hispanic women (Preterm Birth, Maternal and Infant Health, & Reproductive Health, CDC, 2023; Shapiro-Mendoza et al., 2016). HDoP, including gestational hypertension and preeclampsia, were diagnosed in approximately 15% of U.S. pregnancies and were found in 31.6% of pregnancy-related deaths in 2019 (Ford et al., 2022). Black women account for 21% of all HDoP compared with White women (14.7%; Ford et al., 2022). Gaps in understanding of influencers of racial disparities and the lack of identified appropriate interventions to improve outcomes have catalyzed additional investigation among Black populations.
Maternal risk factors have been heavily studied in pregnancy outcome research. Well-known maternal risk factors for APOs are maternal age, race and ethnicity, substance use, neighborhood composition, and socioeconomic status (De Genna et al., 2017; Hill et al., 2020; Richardson et al., 2019; Salow et al., 2018; Slaughter-Acey et al., 2019). Among some racial minorities and “foreign-born” women in the United States, acculturation may influence pregnancy outcomes (Noah et al., 2022; Premkumar et al., 2020), although no single characteristic is a useful marker for prediction (Bai et al., 2009; Perez-Sepulveda et al., 2014). While maternal factors related to these disparities have been explored and continue to warrant additional research, paternal factors and paternal influences associated with APOs have generally been overlooked. While fathers may not be directly responsible for pregnancy outcomes, their contribution to pregnancy is significant and their participation in pregnancy may influence outcomes. A small number of studies have investigated paternal characteristics in relationship with APOs, such as advanced paternal age (Alio et al., 2012; Tough et al., 2003), race and ethnicity (Simhan & Krohn, 2008), sociodemographic features (e.g.: education), and biometrics (e.g., body mass index; Shah, 2010), reporting potential associations with low birth weight, PTB, and small for gestational age (Goisis et al., 2018; Meng & Groth, 2018; Shah, 2010). A 2008 study of approximately 3 million singleton births in the United States determined that Black couples had twice the odds of APOs compared with White couples (Simhan & Krohn, 2008). Similarly, a study of 16 million singleton births in the United States concluded that non-Hispanic Black paternal race was associated with higher rates of PTB and low birth weight (Simhan & Krohn, 2008) after adjusting for maternal characteristics. A 2021 study of approximately four million singleton births from de-identified live birth records collected through the National Vital Statistics System between 2015 and 2017 reported that paternal Black race/ethnicity was significantly associated with PTB, after adjustments for maternal factors (Green et al., 2021). These findings suggest the importance of understanding influencers of racial disparities when examining fathers’ influences on APOs, in addition to mothers’.
A paucity of literature comprehensively examines paternal characteristics in association APOs, describes potential interventions for including paternal characteristics in future research, or examines how APOs affect fatherhood experiences. Still, it is imperative to understand the landscape of literature in the past 10 years examining paternal factors related to adverse pregnancy outcomes. Identifying these noteworthy gaps may elucidate modifiable paternal factors and pathways to improve future pregnancy outcomes, eliminating racial disparities in the occurrence of APOs and actively including fathers in perinatal care and parenting. Therefore, our objective was to conduct a narrative synthesis of studies examining associations between characteristics of Black fathers and adverse pregnancy outcomes in the United States.
Method
We conducted a systematic narrative synthesis of literature examining paternal characteristics of Black fathers in association with adverse pregnancy outcomes: PTB, hypertensive disorders of pregnancy, gestational diabetes, spontaneous abortion, and maternal mortality. PTB is defined as live birth at <37+0days gestation (Preterm Birth, n.d.; Preterm Labor and Birth, n.d.). HDoP is an overarching term encompassing four types of hypertension (SBP≥140 mmHg and DBP≥90 mmHg) during pregnancy: chronic hypertension, chronic hypertension with superimposed preeclampsia, gestational hypertension, and preeclampsia (Garovic et al., 2022). Gestational diabetes is the onset of glucose intolerance during pregnancy (Gestational Diabetes Mellitus, n.d.; Quintanilla Rodriguez & Mahdy, 2024). Spontaneous abortion (miscarriage) is pregnancy loss <20 weeks gestation (Alves et al., 2024). This review was prospectively registered with PROSPERO (ID#
Search
Seven databases (Academic Search Premier, CINHAL, CENTRAL, ClinicalTrials.gov, Embase, PubMed, and Web of Science) were searched for original research articles written in the English language and published from inception to February 8, 2023. Search terms were categorized into two groups—adverse pregnancy outcome terms and population of interest terms (Appendix A)—to locate articles that matched the study objective.
Selection
Upon completion of database searches, all titles and abstracts were uploaded to Covidence (Covidence—Better Systematic Review Management, n.d.), an online systematic review tool; two stages of study inclusion (title/abstract, full text) and one stage of data extraction were followed. At each stage of study inclusion and data extraction, two trained and blinded reviewers independently evaluated articles against predetermined criteria. Discrepancies were resolved by a third independent reviewer, in consultation with both initial reviewers.
Articles were included for data extraction if they (a) investigated associations between fathers’ characteristics and adverse maternal outcomes, (b) included an adverse maternal outcome of interest (PTB, HDoP, GD, spontaneous abortion, maternal mortality) as a study outcome, (c) described racial characteristics of fathers in the sample, (d) described characteristics of Black fathers, (e) described original research, and (f) included a U.S. population.
Articles were excluded if they (a) were in a language other than English, (b) did not describe original research, (c) included a geographic region outside of the United States, (d) did not include adverse maternal outcomes as a study outcome, (e) did not describe race of fathers in the study sample, and (f) did not describe a paternal characteristic of Black fathers.
Data Extraction
A template form was generated in Covidence to streamline and standardize data extraction (Appendix B). Study characteristics extracted include article title, first author, DOI, study aims, hypothesis, study design and timing, years of data collection, and geographic region. Data extracted from articles include adverse pregnancy outcomes of interest, paternal characteristics, maternal characteristics, data sources, study inclusion/exclusion, statistical analyses and modeling, sample characteristics, quantitative measures of association, and qualitative findings.
Results
Our literature search resulted in 210 articles (Figure 1); 112 were identified as duplicates and removed. Therefore, 98 articles were screened against the title/abstract inclusion and exclusion criteria; 64 studies were excluded for not including adverse pregnancy outcomes of interest or for not including paternal characteristics. The remaining 34 studies were assessed for data extraction eligibility via full-text review. Twenty-eight articles were excluded: 5 were not original research; 1 was not conducted in the United States; 12 did not describe racial characteristics of fathers; 4 did not describe associations with adverse maternal outcomes of interest; and 6 did not describe paternal characteristics of Black fathers. Thus, data were extracted from 6 studies.

PRISMA Diagram of Article Selection.
Of these six studies, five reported on one outcome alone; four considered preterm birth, and one reported on preeclampsia. Palatnik et al. (2021) was the only article reporting multiple adverse birth outcomes: PTB, preeclampsia, and gestational diabetes.
Preterm Birth
Five studies examined associations between paternal characteristics of Black fathers and preterm birth (Table 1). Three studies were secondary data analyses (Getahun et al., 2005; Palatnik et al., 2021; Tullius et al., 2020); one cross-sectional survey (Bamanikar et al., 2021); and one (Johnston, 2014) qualitative case study. Of the four quantitative studies, two (Getahun et al., 2005; Palatnik et al., 2021) utilized the National Centers for Health Statistics (NCHS) linked birth files, and two (Bamanikar et al., 2021; Tullius et al., 2020) used state-specific birth records. Three of the four quantitative studies utilized multivariable logistic regression; Tullius et al. (2020) utilized multivariable log-binomial regression and Poisson distributions.
Articles Describing Associations Between Paternal Characteristics and Preterm Birth

Qualitative Study of Preterm Birth
Johnston (2014) qualitatively described a Black father’s experience with adverse pregnancy outcomes. Emergent themes were identified throughout the three stages of the perinatal period: prebirth, during hospitalization, and postdischarge. Major themes included loss, unmet needs during the birthing experience, and changed perspectives on being a father.
Quantitative Studies of Preterm Birth
In quantitative studies, characteristics described included race, age, education, ethnicity, nativity, employment, substance use, father’s own adverse birth outcomes, exposure to adverse live events, paternal involvement, and racial concordance of parents. Interestingly, besides race, no covariate was uniformly examined across all five studies. Even with these non-standardized analyses, all five studies reported a statistically significant association between characteristics of Black fathers and preterm birth.
Getahun et al. (2005) assessed NCHS birth data from 1995 to 2001 by parental racial concordance, adjusting for maternal age education, and smoking during pregnancy; paternal age; trimester prenatal care initiated; parity; and marital status. As compared with White mother–White father parents, the adjusted relative risk of preterm birth (<37 weeks) for White-mother–Black-father parents was 1.11 (95% CI: 1.10, 1.13); and for Black-mother Black-father parents, this relative risk was 1.71 (95% CI: 1.70, 1.72).
Using the Illinois transgenerational birth file, Tullius et al. (2020) linked parent-infant birth outcomes to estimate the relative risk (RR) of infant adverse birth outcomes. Among Black mothers, the risk of infant PTB was 1.02 to 1.62 times greater in those whose father was born preterm compared with infants born to fathers who were not preterm. Controlling for maternal factors in Black women, the adjusted relative risk (aRR) of PTB in former preterm fathers was 1.19 (95% confidence interval [CI] [0.98, 1.45]).
Bamanikar et al. (2021) used New York birth certificate data and self-report surveys to assess parental involvement in the perinatal and postpartum period. Overall, paternal absence, as compared to presence, was associated with increased odds of preterm birth (Odds ratio [OR]: 2.64, 95% CI 1.23, 5.68), controlling for maternal characteristics. In the sample with paternal involvement, when considering an Adverse Birth Composite Outcome (ABCO, defined by the investigator as the presence of one of the following: small for gestational age, prematurity, or NICU admission), Black dads had higher odds of ABCO as compared with White dads, controlling for paternal factors alone (OR 3.19, 95% CI 1.03, 9.87).
Palatnik et al. (2021) performed a retrospective cohort study analyzing all singleton, live birth data in the United States from the CDC National Vital Statistics System, based on birth certificates and other required reporting, from the years 2013 to 2017, that reported paternal race and ethnicity (N=16,482,745). In the sample, PTB rates were highest among births with non-Hispanic Black paternity (14.8%), compared with 9.8% among births with non-Hispanic white paternity and 10.9% among births with Hispanic paternity. As compared with births with non-Hispanic white paternity, odds of preterm birth were greater in unadjusted models (OR = 1.61, 95% CI [1.60, 1.61], p < .0001), models adjusted for maternal demographic characteristics (aOR = 1.17, 95% CI [1.16, 1.18], p < .0001), and models adjusted for maternal demographics and clinical characteristics (aOR = 1.14, 95% CI, [1.13, 1.15], p<.0001) among births with non-Hispanic Black paternity.
Hypertensive Disorders of Pregnancy
Two studies examined associations between paternal characteristics of Black fathers and hypertensive disorders of pregnancy (Table 2).
Articles Describing Associations Between Paternal Characteristics and Hypertensive Disorders of Pregnancy
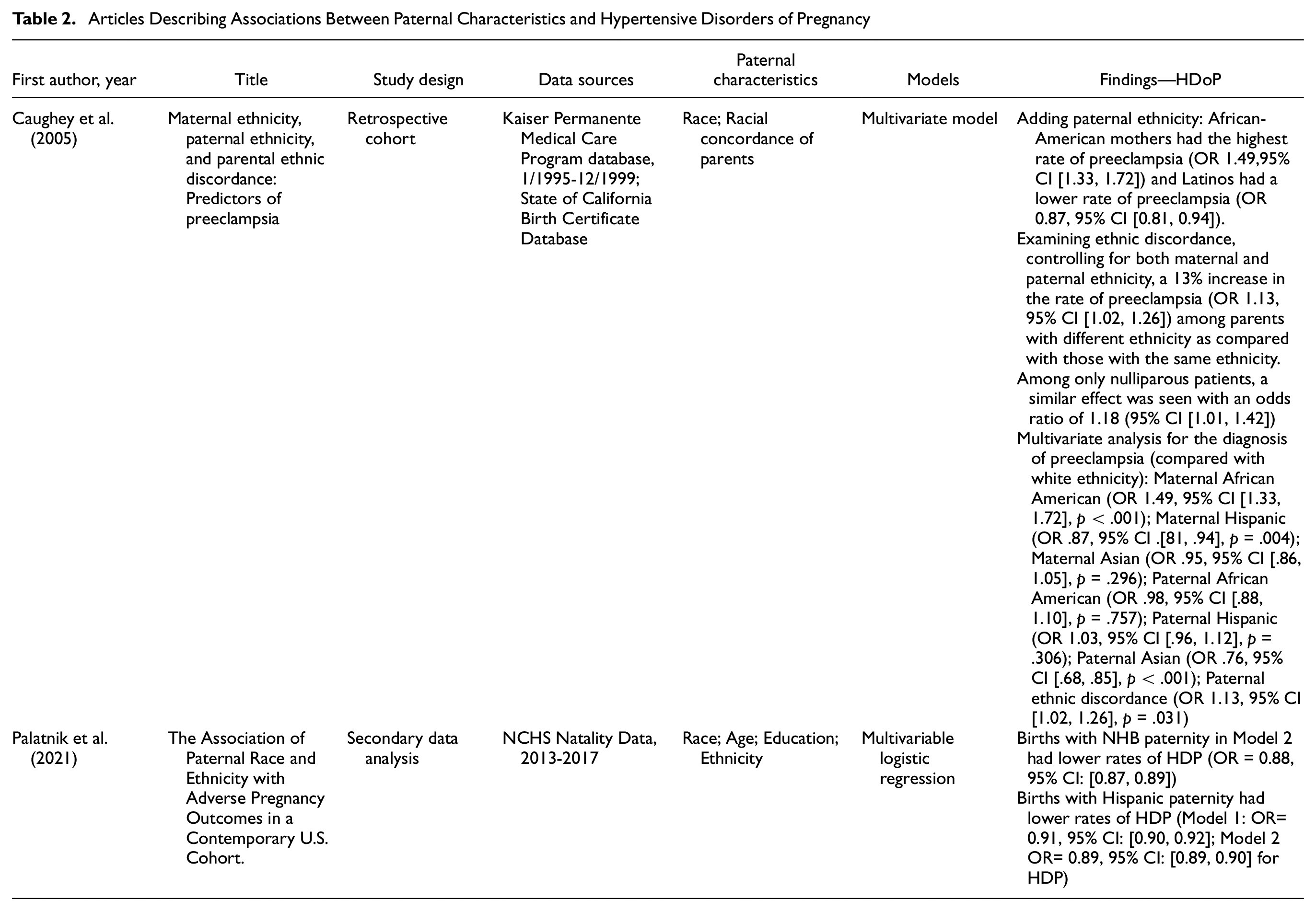
Palatnik et al. (2021; described previously) assessed HDoP, including preeclampsia and gestational hypertension, in association with paternal race and ethnicity. Rates of HDoP were slightly higher among births with non-Hispanic Black paternity (6.9%) compared with non-Hispanic white paternity (6.1%) and Hispanic paternity (4.8%). However, as compared to births with non-Hispanic white paternity, births with non-Hispanic Black paternity were associated with lower adjusted odds of HDoP. After adjusting for maternal demographic characteristics, adjusted odds of HDoP among births with non-Hispanic Black paternity were 0.98 (95% CI, 0.97, 1.00); adjusting for maternal demographics and clinical characteristics, adjusted odds were 0.88 (95% CI 0.87, 0.89).
Contrasting these findings, Caughey et al. (2005) used Kaiser Permanente hospital records from 1995 to 1999 to assess parental racial concordance as a predictor of preeclampsia. Rates of preeclampsia were highest among African American fathers (4.9%) compared with other paternal races. Multivariable analysis indicated that parental racial discordance in the entire sample was associated with greater odds of preeclampsia (OR 1.13, 95% CI [1.02, 1.26]). Black paternal race alone was not associated with any difference in preeclampsia odds.
Gestational Diabetes
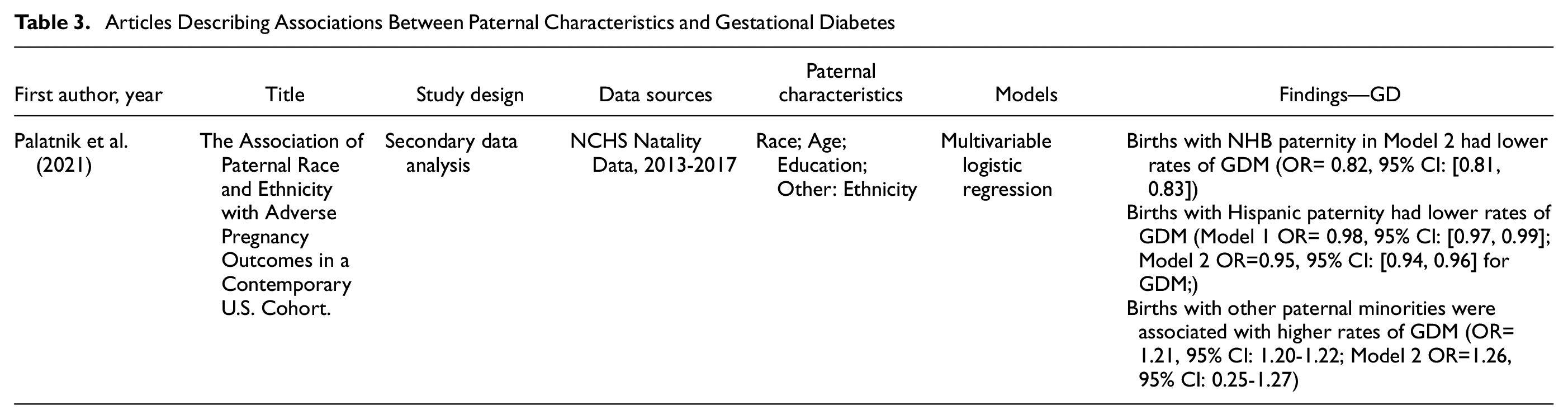
One study examined associations between paternal characteristics of Black fathers and gestational diabetes (Table 3). Palatnik et al. (2021) again determined rates of gestational diabetes among births with non-Hispanic white (5.4%) and Black (5.3%) paternity to be similar; however, among Hispanic (6.4%) and Other (9.2%) paternity, rates were higher. Compared w births with non-Hispanic White paternity, those with non-Hispanic Black paternity had lower odds of gestational diabetes in unadjusted models (OR = 0.97, 95% CI = [0.96, 0.98]) and models adjusted for maternal demographic and clinical characteristics (aOR = 0.82, 95% CI = [0.81, 0.83]).
Articles Describing Associations Between Paternal Characteristics and Gestational Diabetes
Other Adverse Pregnancy Outcomes
This literature review did not return any studies in which outcomes of spontaneous abortion or maternal mortality were examined in association with Black paternal characteristics.
Discussion
There has been a slow but growing interest in the role of fathers in maternal health outcomes (Bond, 2010; Bowen et al., 2022; Griffith et al., 2023). Paternal factors are associated with several maternal and infant outcomes including preterm birth, fetal growth restriction, preeclampsia, maternal stress, and even breastfeeding rates (Alio et al., 2013; Eggermont et al., 2017; Poh et al., 2014; Yargawa & Leonardi-Bee, 2015). Several studies have informed the importance of paternal involvement during pregnancy. For example, Alio et al. suggest paternal involvement has a significantly positive impact on pregnancy and infant outcomes (Alio et al., 2013). When fathers are involved during pregnancy, maternal negative health behaviors diminish, and the risk of pre-term birth, low birth weight, and fetal growth restriction is significantly reduced (Alio et al., 2013), and maternal stress levels are lower (Xue et al., 2018). Individual, family, community, societal, and policy factors significantly facilitate or diminish the involvement of fathers during pregnancy (Alio et al., 2013). When fathers are involved during pregnancy mothers experience higher levels of perceived support associated with lower emotional distress for mothers (Walsh et al., 2023). Father’s support and involvement can also play a protective role in maternal health, and well-being (Walsh et al., 2023). Father and mother interpersonal relationship quality may be positively correlated with mental health and overall health (Walsh et al., 2023).
Examining paternal influencers of pregnancy outcomes is timely and important given the persistent and worsening maternal health outcomes in the United States (Hoyert, 2023; World Health Organization, n.d.). Emerging evidence of the impact of paternal factors on maternal and child health outcomes and the results of this review establish that Black paternal characteristics specifically also influence pregnancy outcomes. This is significant in light of the worsening Black maternal health crisis. Factors such as race, age, education, ethnicity, nativity, employment, substance use, and the father’s own adverse birth outcomes are linked to pregnancy morbidity (Shah, 2010; Simhan & Krohn, 2008; Tough et al., 2003). Results from this review suggest that Black paternity increased the odds of PTB but was inversely related to HDoP. Therefore, there is an urgent need to expand data collection to incorporate fathers in studies of pregnancy outcomes and link paternal characteristics to maternal and infant factors to improve the understanding of the full landscape of influential factors to optimize prevention strategies.
While the results of this review establish relationships between Black paternal characteristics, preterm birth, and hypertensive disorders of pregnancy, mechanisms linking paternal factors to pregnancy outcomes are not entirely clear. This emphasizes the need to further expand the collection of fathers’ health and social data in relation to maternal and child health. Paternal age could influence sperm function (Sartorius & Nieschlag, 2010) and genetic imprinting. For example, paternal imprinting has been suggested to influence placental development, trophoblast migration, subsequent fetal growth, preterm birth, and preeclampsia (Monk, 2015). While paternal age has been well studied (Goisis et al., 2018; Sartorius & Nieschlag, 2010; Tough et al., 2003), additional paternal biological factors that may adversely influence the normal physiology of pregnancy should be explored. Findings from this review suggest that the Black paternal race was protective for gestational diabetes and hypertensive disorders of pregnancy. Studies (Jiang et al., 2022; Morken et al., 2018; Rich-Edwards et al., 2014; Saravanan et al., 2020) have consistently shown women who experience HDoP and gestational diabetes have an increased risk of cardiomyopathies and premature death in later life (Bokslag et al., 2017; Giguère et al., 2012). In neonates, these outcomes are associated with intrauterine growth restriction and macrosomia, PTB, low birth weight, and other adverse late-life outcomes (Hauspurg et al., 2018; Heida et al., 2016; Jiang et al., 2022; Morken et al., 2018; Rich-Edwards et al., 2014). Little is known about the potentially mediating effects of paternal factors on PTB, HDoP, and GD. Narratively reviewing the literature on the relationship between Black paternal factors and APOs establishes significant rationale to identify paternal-influenced pathways for improving maternal health outcomes to reduce the poor burden of maternal health outcomes in the United States.
Existing programs that successfully engage fathers could be expanded to incorporate the necessary data collection to improve understanding of the influence on pregnancy and fetal outcomes. For instance, the Where Dads Matter Initiative (Helping Babies, Parents and Communities Thrive, n.d.), successfully recruits fathers and offers pregnancy support and parenting preparation targeted to both mother and father. Healthy Start, Inc. already indicates that engaged fathers show improvements in psychological well-being, father-mother relationship quality, parenting literacy, economic stability, and overall child behavioral and emotional/social development (Helping Babies, Parents and Communities Thrive, n.d.). This program could be expanded to integrate measurement tools that link paternal characteristics and pregnancy outcomes to include data tools to confirm these suggested protective effects and biological impact (Fleck et al., 2013; Lee & Lee, 2023; Obure et al., 2019). Sustainability for fatherhood initiatives is crucial for longitudinal exploration factors. None of the manuscripts included in the present review included long-term, prospective assessments of paternal influences on the maternal outcomes of interest. While not included in this review for lack of linkage to pregnancy outcomes, there is one existing U.S. cohort prospectively recruiting Black fathers to understand biological and social impacts on Black births (Misra et al., 2023). This study anticipates the recruitment of 400 Black fathers and will link maternal and infant health records to explore family influencers of pregnancy outcomes. This study demonstrates a strong rationale that fathers can be successfully recruited into perinatal studies and highlights the need to incorporate fathers into existing perinatal cohorts to improve and sustain U.S. fatherhood initiatives (Obure et al., 2019; Semlow et al., 2021).
Out of over 90 identified manuscripts, only 6 were eligible to be included in our review, highlighting the limited literature in the field of Black men’s paternal influences on maternal and child health. Despite this limitation, the included publications ranged in design (e.g., qualitative studies and secondary data analyses), sample size, and data source (e.g., birth certificate data and survey self-reports); providing a range of research studies to deduce our findings from.
Conclusion
This study identified six research studies that explored Black fathers’ characteristics influencing adverse pregnancy outcomes. Studies demonstrated Black fathers’ significant association with preterm birth outcomes in several studies, but an inverse impact on preeclampsia and gestational hypertension. Research should continue to explore paternal factors that influence pregnancy outcomes in racial/ethnic-specific models to identify optimal intervention strategies to improve disparities in maternal and child health outcomes.
Footnotes
Appendix
Search Terms Utilized for Database

| Outcomes | Population |
|---|---|
| Preterm birth Preeclampsia Gestational diabetes Spontaneous abortion Miscarriage Hypertensive disorders Maternal mortality Maternal death |
Paternal Father Spouse AND Black African American |
Acknowledgements
We thank Claire Couturier, Maggie Chen, Lindsey DeSplinter, and Ramatu Abdul Hamid Alhassan for their assistance in the review process.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: University of Pittsburgh Office of the Provost Race &. . . Research Collaboratory, Black Fathers Initiative.