
Abstract
Type 2 diabetes is on the rise globally, and previous research has identified gender as one known risk factor for developing this disease. Gender has also been reported to affect patients’ experiences of managing type 2 diabetes. However, little is known of men’s specific experiences with type 2 diabetes, as research with a gendered focus has concentrated more on women’s experiences with the disease. This scoping review explores how research has addressed men’s experiences of managing type 2 diabetes and their encounters with health professionals. The review consists of an iterative process, involving six steps: identification of the research questions, identification of relevant studies, study selection, charting the data, collating and summarizing results, and consultation with external stakeholders. Through the process, 28 publications were identified, which indicate a gap in research on patients’ experiences with type 2 diabetes. The majority of the identified studies focuses on men from an ethnic minority due to their poorer health outcomes. However, a knowledge gap regarding men belonging to an ethnic or racial majority warrants further attention, as studies indicate that men who share similar social economic status face similar barriers to improving the management of type 2 diabetes. There is little discussion of how the gendered dynamics in encounters between patients and health professionals affect the management of type 2 diabetes. This review suggests a need for further research that explores how practices of masculinities, that is, the normative practices guiding men’s behavior, intersect with men’s experiences with type 2 diabetes in a broader perspective.
Introduction
Type 2 diabetes (T2D) is on the rise globally. A World Health Organization (WHO) report estimated that 422 million adults were living with diabetes in 2014 (WHO, 2016). Research identifies risk factors related to the increase in T2D as ethnicity, gender, age, socioeconomic factors, and health behaviors. A social gradient has also been noted in the development of T2D and the uptake of treatment. While most studies have focused on the social determinants of T2D and on how the risks of developing T2D reflect social stratification, Wiedman (2010) emphasizes how T2D is a general problem related to a rise in global chronicity following conditions of modernity. The increase thus reflects a complex interplay between human biology and changing structural, cultural, and social conditions of human living.
Research has emphasized men’s greater risk of developing diabetes (White et al., 2011), but less attention has been paid to how gender affects patients’ management of T2D. Chronic illnesses have been regarded as gender-neutral although the management of chronic illness reflects gendered differences (Thorne et al., 1997). The same can be said of research on T2D, where patients identifying as female comply with physicians’ advice and complete treatment more often than those identifying as male. The gendered differences also stand out in research literature on how social support affects patients’ management of chronic illness, reflecting a gendering of care practices in relationships (August & Sorkin, 2010). However, an initial search for literature on men’s experiences of managing T2D led to a finding of only a handful of studies (Hawkins et al., 2016, 2018; Liburd et al., 2007; Sherman & Fawole, 2016).
A WHO report from 2018 addresses men’s general health and highlights the need for a gender perspective to effectively include men in health services and health promotion initiatives (WHO, 2016). Following up on our interest in men’s experiences of managing T2D and the call for a gendered perspective on men’s health, we conducted a scoping review of how research has addressed (a) men’s particular experiences of managing T2D, (b) how gender affects encounters between men with T2D and health professionals (HPs), and (c) how men experience social support in relation to management of T2D.
This review is theoretically informed by an understanding of gender as a set of social and cultural practices, which pervades performances in all situations (West & Zimmerman, 1987). We draw on a theoretical approach of masculinities as multiple in recognition of a social order including hegemonic and subordinate masculinities (Connell, 1995; Connell & Messerschmidt, 2005). Adopting a gendered understanding of how research has addressed men’s experiences with managing T2D, and their experiences of encounters with HPs involves a particular focus on how varying forms of masculinity intersect with health. This will in turn promote HPs’ engagement with patients and direct future research in the field.
Design and Method
This review is conducted as a scoping review of how research has addressed men’s everyday experiences of managing T2D and their encounters with HPs. Following scoping review methodology (Arksey & O’Malley, 2005), this study consists of mapping and identifying relevant studies to determine how a broad research theme has been explored (see also Levac et al., 2010). The subsequent aim is to summarize established knowledge and identify potential research gaps. A scoping review consists of an iterative process, involving six steps: identification of the research questions, identification of relevant studies, study selection, charting the data, collating and summarizing results, and consultation with external stakeholders. As an alternative to external stakeholders, a reference group of researchers with experience of research in gender and chronic illnesses was involved.
The Research Questions
This scoping review included three research questions:
The research questions are situated within the field of health promotion as this approach focuses on patient perspectives and patient resources such as networks and health literacy in the context of living with chronic disease.
While gendered practices have been identified as shaping how we come to engage with a position in society, this review explores how these insights inform research on men’s experiences of T2D and their encounters with HPs. Studies including a patient perspective are thus central to the inquiry.
Identifying Relevant Studies
The search was conducted in relevant databases that span across disciplines within medical and social sciences, such as PubMed, Embase, CINAHL, Anthropology Plus, PsycINFO, Sociological Abstracts, and Web of Science. The strategy involved identifying keywords using thesauruses such as MeSH terms and CINAHL Subject Headings. This resulted in six search terms focusing on different aspects of the research questions: (a) gender, (b) T2D, (c) health promotion, (d) experiences, (e) encounters with HPs, and (f) social network.
Each term was supplemented with synonyms and associated concepts such as male, diabetes mellitus, prediabetes, knowledge, perspectives, treatment, care, spouse, partner, and social network.
Supplementary searches identified relevant gray literature from the websites of health authorities and patients’ organizations; furthermore, manual searches of references from selected publications were conducted to identify additional relevant studies. The search was narrowed to include adult studies (18+) in databases with this particular exclusion option (e.g., PubMed and Embase).
The Selection Process
The search was conducted in September and November 2020 and resulted in 2,855 unique publications. Thirty-one additional publications were identified in gray literature, and references in selected publications were included.
The selection process consisted of two steps: first, the title and abstract were screened, followed by a screening of the full text. The first step involved identifying studies that focused on gender in relation to T2D or that produced results reflecting the importance of gender in this context even if gender was not explicitly within the defined scope of the study.
The first inclusion criterion (Figure 1) implies that gender as a topic must be stated in the abstract, providing actual insights into gendered issues including barriers and dynamics. Similarly, studies focusing on encounters between men and health professionals must include gender, either by focusing on the role of gendered practices and gendered dynamics in medical encounters or by providing analytical results on the importance of gender in relation to T2D.
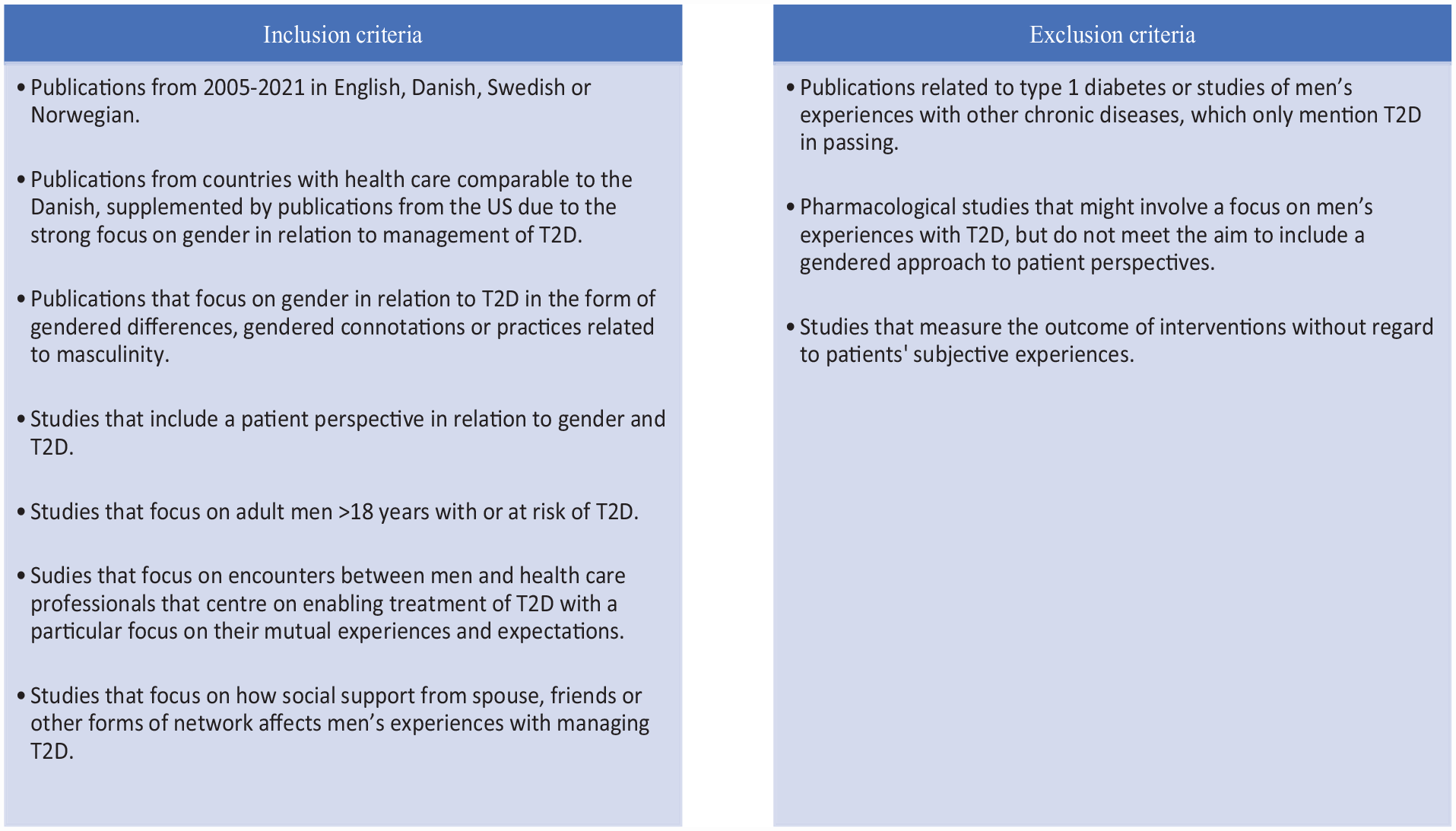
Inclusion and Exclusion Criteria
We limited our scope to countries with health care comparable to the Danish. Although health care in the United States differs from the Danish regarding equity and access, publications from the United States were included because of their strong research focus on gender.
Two of the authors (Pihl and Thualagant) validated the selection by checking whether the stated criteria were followed and subsequently comparing the selected publications. This led to the exclusion of studies that, despite a gendered focus, mostly provided insights into women’s experiences with T2D. Studies evaluating participants’ satisfaction with interventions were also excluded if they did not include further reflections on the role of gendered practices. Finally, studies that compared gendered differences in quality of life or experiences of social support for patients with type 1 diabetes and T2D were excluded, as these focused more on the management of the disease rather than the gendered differences. This process resulted in the inclusion of 93 studies in full-text screening.
The second step consisted of thorough readings of the 93 studies. This was performed by two authors independently (Pihl and Thualagant), with the first author reading all the studies. In this assessment, a decision was made to include or exclude according to the criteria, leading to a final selection of 28 studies (see flowchart, Figure 2).

Flowchart
Charting the Data
Following the selection process, the publications were categorized according to aim, design, population or informants, type of publication, and results. We also included a brief reflection on the gendered focus on T2D and whether the study addressed men’s experiences in particular, their experiences of encounters with HPs, and how social support affected men’s experiences with managing T2D.
Results
A total of 93 publications were included in the full-text screening. Out of these 93 studies, 28 were eligible according to the criteria.
Publication Characteristics
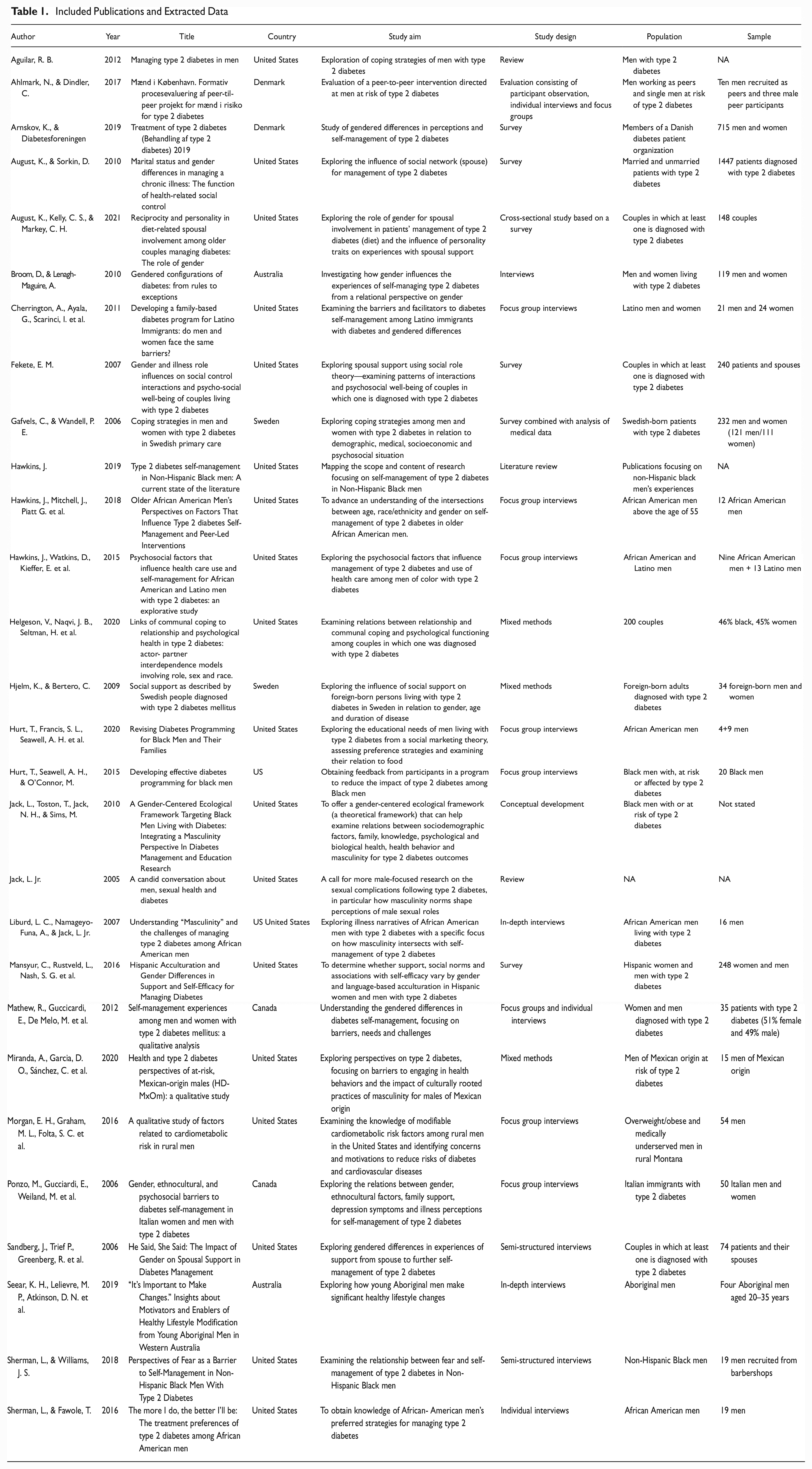
Of the 28 publications, we found that 24 (86%) included an empirical scope. Three (11%) publications are review-based while one involves developing a conceptual framework. Apart from one doctoral dissertation and three (11%) reports, all were published in peer-reviewed journals. Most (22/79% studies) were published since 2010. One third (33%) were published within the last 3 years (2018–2021), indicating a growing interest in men’s experiences with T2D. Seven (25%) publications are from before 2010 (Table 1).
Included Publications and Extracted Data
Geography
Most publications stem from research in the United States. We found that no publications from Europe outside the Nordic region fitted the criteria of the second selection, that is, contributing insights into men’s specific experiences. Thus, four (14%) Nordic studies were included, two (7%) from Denmark and two (7%) from Sweden.
Journals of Publication
Papers were published in diverse journals, focusing on diabetes (3/11%), gender (2/7%), relationships and couples (2/7%), patient education (2/7%), nursing (2/7%), general practice (3/11%), public health (2/7%), and race, geriatrics, family, and community health (5/18%). One journal has published three (11%) of the included studies: the American Journal of Men’s Health.
Research Methodologies
Most studies use qualitative methods (15/54%) publications are based on individual interviews or focus groups). Fewer than one third (21%) involve only quantitative methods. The four (14%) publications employing mixed methods combine interviews with a survey or clinical data. Four studies (14%) include a conceptual framework (Jack et al., 2010) or a synthesis of existing studies (Aguilar, 2012; Hawkins, 2019; Jack, 2005). The study designs reflect how qualitative methods are often employed in research on patient experiences with the qualitative studies providing in-depth knowledge of men’s experiences of diabetes from a particular position, that is, African American or Hispanic men with a specific regional affiliation and socioeconomic status.
Synthesis of Results
The following section shows how the included studies relate to the research questions by presenting the identified findings and research gaps. In addition, the synthesis considers how conceptualizations of masculinity figure in the studies.
Men’s Knowledge and Experiences of Managing T2D
The selected studies point to a gap in knowledge of men’s experiences with managing T2D. While gendered differences have been observed, little attention has been given to explaining why gendered differences appear in relation to outcomes of T2D and how the gendered differences unfold in patients’ lives and experiences with managing T2D (see, for instance, Broom & Lenagh-Maguire, 2010; Mathew et al., 2012).
Most publications focus strongly on the experiences of men from a racial or ethnic minority background or men as immigrants, given the fact that men from these groups often have poorer health outcomes. Studies from the United States form the majority (21/75%) of the selected 28 publications, providing insights into the experiences of African American, non-Hispanic Black, or Latino men (Hawkins, 2019; Hawkins et al., 2015; Jack et al., 2010). A central theme in these publications is cultural and gendered barriers to men’s self-management of T2D with a focus on how practices associated with hegemonic masculinity counteract men’s effective management of T2D (Broom & Lenagh-Maguire, 2010; Hawkins, 2019; Hawkins et al., 2015; Liburd et al., 2007; Seear et al., 2019; Sherman & Williams, 2018). Hawkins et al. conclude that non-Hispanic Black and Latino men refrain from seeking medical help due to norms associated with hegemonic masculinity including men exercising control over their bodies, which become challenged by physicians’ advice. The studies of African American, non-Hispanic Black, and Latino men thus conclude that norms associated with masculinity such as staying in control, being autonomous and engaging in risk-taking discourage men from seeking medical help and improving glycemic control, and adoption of health-promoting lifestyles.
Gendered roles such as males assuming the status of breadwinner in the family lead to a prioritization of work over health. A study of Latino men living in the United States repeated the finding of men’s working lives as challenging the management of T2D, as the obligation to work long hours in hazardous jobs (construction, farming, lumber, and chemical production) increased negative stress. The study highlighted how a lack of flexibility at work produces work-related stress, which negatively affects men’s health behaviors (Cherrington et al., 2011). Drawing on Connell’s theorization of masculinity, Hawkins (2019) refers to these practices and the gendered role of the male breadwinner as associated with performances of hegemonic masculinity.
Although these studies indicate a need for future research on African American or Latino men in the United States due to their poorer health outcomes, a study by Morgan et al. (2016) of White men with T2D residing in the rural west of the United States led to a similar conclusion. In similarity to Hawkins (2019), Morgan et al. discuss how practices of rural masculinity are at odds with healthy behaviors such as seeking medical help as well as how obligations to work long hours in farming discourage men from taking up exercise. Male sociality in the rural community involves drinking and smoking, and thus men’s social interactions represent a barrier to managing T2D (see also Mathew et al., 2012).
A study of patients with T2D in Canada reflected a gendered pattern in relation to preferred self-management practices, leading women to reveal their diagnosis sooner than male patients, who often concealed their T2D from family members and their colleagues at work (Mathew et al., 2012). While these studies include different ethnic groups of patients, they present somewhat similar experiences in relation to gendered roles. Drawing on theories of masculinity and on Liburd et al. (2007), Mathew et al. characterized men’s decision to conceal T2D as a reflection of gendered norms requiring men to perform autonomy, representing a barrier to the effective management of T2D.
Studies also address men’s experience of coping strategies affecting self-management revealing gender differences (Aguilar, 2012; Gåfvels & Wändell, 2006), with women favoring social support and emotional strategies and men relying more on an instrumental approach to T2D (Gåfvels & Wändell, 2006). Aguilar (2012) points out that men with T2D exert less effort in coping, are less informed about treatment strategies, and are less likely to use health care services. In this way, a need to take account of cultural differences emerges across the studies of men’s coping strategies and experiences of managing T2D.
Studies indicate conflicting findings on the role played by men’s knowledge in the management of the disease. Miranda et al. (2021) find that men of Mexican origin at risk of T2D lack sufficient knowledge of risk factors. Lifestyle changes are challenged by a fatalistic approach to life and an adherence to work (see also Mansyur et al., 2016). In contrast, Seear et al. (2019) identify how young Aboriginal men with or at risk of T2D successfully change their lifestyles through diabetes education and the belief that their actions can help mitigate the progression of the disease. Therefore, while studies of men’s experiences suggest a need for education about health behavior, the effects of knowledge on men’s managing of T2D require consideration of cultural factors.
One exception to the empirical studies of men’s experiences is the article by Jack et al. (2010), who develop a conceptual approach labeled “a gender-centered ecological framework” to address Black men’s specific experiences with T2D, with an integrated approach to how socio-demographic factors, knowledge of diabetes, family, community, psychological and biological health, and masculinity all affect Black men’s experiences with T2D. This ecological approach calls for an examination of the social norms of masculinity across individual, familial, and societal contexts in order to improve understanding of how gender roles conflict, such as how the expectations of staying strong and hesitation to ask for help affect Black men’s management of T2D.
A general finding in the publications is the lack of emphasis on masculinity. The studies indicate the need of developing differentiated interventions targeting men, not only focusing on gendered practices or race/ethnicity but also on how men’s experiences with T2D are determined by sociodemographic factors, community, social network, family status, and knowledge of diabetes.
The findings point to a need to engage further with research on the intersections between practices of race, gender, class, and regional affiliation to enhance the understanding of men’s practices of managing T2D. Following Hawkins (2019) and Jack et al. (2010), the empirical research also indicates how men’s management of T2D is a complex field requiring fluid conceptualizations of masculinity, as men’s experiences also become affected by social support, access to health care, community, socioeconomic status, and knowledge of T2D.
Men’s Experiences of Encounters With Health Professionals and of Treatment of T2D
A less developed theme in research on T2D involves men’s encounters with HPs (Ahlmark & Dindler, 2017; Hurt et al., 2015, 2020; Jack, 2005). Two publications address a study of African American men’s preferences regarding interventions, involving the influence of masculinity to further men’s self-management of T2D (Hurt et al., 2015, 2020). Another study evaluates a male peer-to-peer program targeting vulnerable men at risk of T2D in Denmark to determine men’s experiences with the program (Ahlmark & Dindler, 2017). One publication addresses men’s sexual problems following T2D, particularly how norms of masculinity and the emphasis on control affect men’s sexuality (Jack, 2005). Men with T2D face complications in their sexual lives to a greater degree than women, which necessitates the capability of HPs to address this issue in consultations (Jack, 2005; see also Arnskov & Diabetesforeningen, 2019).
Several publications call for differentiated interventions to support the different needs of men and women (Cherrington et al., 2011; Hurt et al., 2020; Jack, 2005; Mansyur et al., 2016), although without explaining how gendered dynamics actually influence encounters between male patients and female HPs. A theme common to several publications involves the effect of gendered preferences on the content of encounters with HPs. In these publications, a gendered dynamic is emphasized, where men prefer a practical approach to managing T2D focusing on instrumental aspects and self-education, while women prefer social support and participation in support groups (Mathew et al., 2012). Apart from the need for interventions to take account of gendered preferences, several studies point out the importance of developing culturally sensitive programs (Hurt et al., 2020; Hurt et al., 2015; Sherman & Fawole, 2016).
For programs to be effective, interventions should also take account of gendered role conflicts such as the obligation of men to perform as breadwinners and the difficulties this poses for effective management of T2D. Based on a study of African American men, Hurt et al. (2020) propose the inclusion of men’s families in interventions, as African American men benefit from an inclusion of their spouses.
Apart from the intersections between gendered and cultural practices, studies from the United States report how African American and non-White Hispanic men prefer community-based services and emphasize affordable access to health care for further participation (see Hawkins, 2019), which suggests the importance of regional affiliation.
A gendered pattern emerges in relation to men’s experiences with health care provision in a study from Denmark, as men reported greater satisfaction than women with help from HPs to achieve glycemic control. This included help from their doctor and specialized diabetes nurses at Danish outpatient clinics (Arnskov & Diabetesforeningen, 2019). This is rather interesting as men have poorer health outcomes than women.
A final point is the lack of focus in research on HPs’ experiences of treating men with T2D. None of the selected publications brought up this subtheme, which is interesting given the fact that men with T2D are likely to meet female HPs, calling for attention to how gendered practices unfold in these encounters. 1
Men’s Experiences With Social Support to Self-Manage T2D
Publications addressing men’s experiences with T2D in relation to social support particularly identified spousal support to improve medication adherence and the lifestyle changes required to self-manage T2D. They specifically focused on whether support is perceived as constructive or as criticism and nagging behavior (August & Sorkin, 2010; Sandberg et al., 2006) or whether experiences of social support are equally distributed between men and women (August et al., 2021). Men experience much greater support from their spouse and other forms of network than women do (Cherrington et al., 2011) and also find the support more helpful than women (August & Sorkin, 2010; Sandberg et al., 2006). In a study of needs and barriers of immigrant women and men with a Latino background, Mansyur et al. (2016) present a gendered dynamic where women face social barriers to T2D through poor family support whereas men face barriers related to work (see also Cherrington et al., 2011). Married men receive the most support whereas unmarried men report receiving the least support (August & Sorkin, 2010). Helgeson et al. (2020) suggest the role of socialization as an explanation for why men in general tend to benefit more from spousal support than women, although the same study also shows how men derive greater benefit from their own communal coping than women, as men tend to be less affected by their spouses. The study also indicates a racial difference; the patients were divided into Black and White participants and men from Black families generally experienced less support from their spouses (Helgeson et al., 2020).
Spousal support is often related to diet, planning meals, buying food, and cooking, reflecting a gendered division of labor, as men trust their wives’ ability to select and cook appropriate dishes (Broom & Lenagh-Maguire, 2010; Ponzo et al., 2006). A general finding is that men irrespective of their ethnicity or race look to their wives for help with managing T2D, and wives willingly assume this responsibility, which reflects a gendered dynamic of giving and receiving care (August & Sorkin, 2010; Helgeson et al., 2020). However, exceptions to these norms are found in men with T2D who identify as homosexuals, calling for a greater focus on the intersections between gendered health practices and sexuality (Broom & Lenagh-Maguire, 2010).
All the publications focus on the gendered dynamics of heterosexual couples, reflecting masculinity and femininity norms in providing and receiving care. Fekete (2007) further unfolds the dynamics through a study of couples in which congruent relationships, where men are patients and women are caregivers, thrive better psychologically than couples defined by the opposite dynamics of women as patients and men as caregivers.
Discussion
Considerations for Future Research on Men's Experiences of Managing T2D
This scoping review indicates a lack of sustained debate in research on men’s experiences with T2D and these men’s encounters with HPs, as the selected studies have been published in a variety of journals. While gendered differences are included in research on T2D, the studies often reflect a concern with women’s experiences of managing T2D (see for instance Legato et al., 2006).
The publications that focus on men’s experiences of managing T2D often involve an intersectional approach with a specific emphasis on men from a minority background or ethnic group. Very few studies include encounters between men with T2D and HPs and their respective experiences of these encounters. Research on T2D thus reveals little focus on the gendered dynamics of encounters, although men with T2D commonly encounter female HPs. This review thus indicates a gap in research on men’s experiences with T2D and their encounters with health professionals.
The findings suggest a need for further research on how men’s performative masculinity practices across varying settings intersect with men’s experiences with managing T2D. Of interest in this respect is the extent to which men have similar experiences with the difficulties of managing T2D across racial and ethnic groups. The study by Morgan et al. (2016) includes a similar finding between the health practices associated with the masculinities of rural White men and Hawkins’ study of African American and Latino men in the United States (Hawkins, 2019; Hawkins et al., 2015). These findings indicate a need to explore how masculinity practices intersect with work and regional affiliation.
The gap in research on diabetes also involves men’s encounters with HPs, and the experiences of these professionals; such encounters are even less researched than men’s experiences with managing T2D. However, research including gendered preferences has been conducted in relation to the design of interventions (instrumental vs. emotional) and general satisfaction with health care (see for instance Arnskov & Diabetesforeningen, 2019), but research is required to enhance our understanding of how gendered dynamics shape the actual encounters between men with T2D and HPs. This aspect of diabetes care is important, as men with T2D are likely to encounter female HPs. Research on HPs’ experience of interactions with male patients is required to highlight their knowledge of gendered barriers to men’s management of the disease.
Social support constitutes an important theme in the publications focusing on men’s experiences with T2D. Overall, men’s experiences of social support reflect a gendered dynamic with men receiving support from spouses and their social network to manage T2D. Several publications focus on the experiences of men and women with social support as reflecting a gendered dynamic, as men who identify as living in a heterosexual relationship report receiving more spousal support than women do. This demonstrates the relevance of professional attention to men’s social networks, specifically men without a partner or adult children, and continuing research on how men with inadequate social support experience management of T2D.
Most publications are based on qualitative empirical studies involving a limited number of individual or focus group interviews to deepen knowledge of men’s subjective experiences. However, none of the studies apply ethnographic methods such as participant observation, which could improve knowledge of how gendered practices in various contexts (work, inpatient and outpatient care, home, and community) intersect with practices of doing T2D.
Another important finding is the very limited use of theoretical frameworks in studies of men’s experiences with T2D and their encounters with HPs. While the publications provide a range of empirical data, the research rarely involves the use or development of theoretical concepts that could enhance our understanding of how practices of masculinity intersect with the practices involved in chronic diseases in gendered enactments. Following Hawkins (2019) in her plea to adopt a fluid conception of masculinities, we argue for the need to continue conceptual development within the field.
Building on Connell and Messerschmidt’s argument that masculinities are “configurations of practice that are constructed, unfold and change through time” (Connell & Messerschmidt, 2005, p. 852), future research of men’s experiences with T2D should involve an equal focus on practices related to gender, race, class, and regional affiliation. Future research should also identify the heterogeneous experiences of men with T2D who might share the same ethnicity, socioeconomic status, and community but differ in their experiences with T2D. Knowledge of how diabetes intersects with heterogeneous gendered and racial performances is required to enable a fluid understanding of masculinity to counter universalizing approaches to men. This knowledge would enable the continuing development of differentiated diabetes education and interventions to improve the treatment of all patients.
Limitations of the Study
This study is limited by the criterion to include only publications from countries with health care comparable to that of Denmark or the United States. Another limitation is the criterion to include only publications in English, Danish, Swedish, and Norwegian, which emphasizes the need for further research including a more global perspective.
In the process of full-text reading, some studies were excluded because of the criterion to focus exclusively on men’s experiences with managing T2D even if these experiences might resemble those of managing other forms of chronic diseases.
Conclusion
Men’s experiences with T2D and the experiences of men with T2D of encounters with HPs are underexplored topics in current diabetes research. While several of the identified studies emphasize men’s experiences with managing T2D in relation to specifically ethnicity and race, we found that knowledge is still needed on the experiences of men of different ethnicities and socioeconomic status, and men without spousal or social support.
Research on encounters between men and HPs is required to understand their respective experiences of these encounters and collaborations to improve the treatment of T2D. Several studies include a call for differentiated interventions and patient education to help men with T2D. Research on men’s experiences of social support has a particular focus on the role of spousal support, reflecting a gendered pattern involving married men in heterosexual relationships receiving support from their wives to self-manage T2D. This finding calls for greater awareness by HPs of men with T2D who do not have a spouse or lack a close social network.
While this scoping review is based on extensive research literature on T2D, future reviews could explore men’s experiences with managing other chronic diseases, as findings from such studies could be relevant to future studies of men’s experiences with T2D. Future research could include a relational approach to enhance understanding of diabetes as shaped by gendered enactments and could also explore how gendered dynamics affect collaboration in encounters between HPs and men with T2D.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883231178753 – Supplemental material for Men’s Experiences With Managing Type 2 Diabetes and Their Encounters With Health Professionals: A Scoping Review
Supplemental material, sj-docx-1-jmh-10.1177_15579883231178753 for Men’s Experiences With Managing Type 2 Diabetes and Their Encounters With Health Professionals: A Scoping Review by Eva Vibeke Kofoed Pihl, Louise Søgaard Hansen, Anne-Louise Bjerregaard, Peter Bindslev Iversen and Nicole Thualagant in American Journal of Men's Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Steno Diabetes Center Zealand, Denmark.
Ethical Approval
A scoping review is a secondary analysis of published literature and does not require ethics approval.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.