
Abstract
The human papillomavirus (HPV) vaccine was recently approved for use in males. Certain groups, such as men who have sex with men (MSM), are at increased risk of HPV infection. The purpose of the study was to understand perceptions of HPV and the vaccine among adolescent and young adult males, both heterosexual and MSM. Seventy-six males (45 heterosexual, 31 MSM) completed a questionnaire and participated in a focus group. Overall, 42% had heard of HPV and 39% had heard of the HPV vaccine. Males had moderate to favorable attitudes toward vaccination, although intentions to vaccinate were more neutral. MSM were more knowledgeable, aware, and in control of the decision to vaccinate than heterosexual males. Increasing awareness and knowledge about HPV and the vaccine may be necessary to encourage vaccination; certain subgroups of males may be more receptive to HPV vaccination than others.
Keywords
Background
HPV and the HPV vaccine
The human papillomavirus (HPV) is the most common sexually transmitted infection (STI) in the United States and worldwide (Dunne & Markowitz, 2006). HPV Types 6 and 11 cause approximately 90% of the more than 500,000 cases of genital warts that occur each year in the United States among sexually active men and women (Hoy, Singhal, Willey, & Insinga, 2009; Hu & Goldie, 2008). Direct medical costs related to genital warts are estimated at $200 million per year (Hu & Goldie, 2008). In addition, genital warts can have an adverse impact on quality of life (Woodhall et al., 2009). HPV-associated cancers in males include certain anal, penile, oropharyngeal, and oral cavity cancers caused primarily by HPV 16 (Parkin & Bray, 2006). Men who have sex with men (MSM) are at higher risk for HPV infection than heterosexual males because of risky sexual practices, such as unprotected anal sex (Jin et al., 2007; Joseph et al., 2008). This leads to an increased risk of anal HPV transmission and higher rates of anal and penile cancers among MSM (Dietz & Nyberg, 2011; Guilano et al., 2008). Additionally, MSM with HIV are at even higher risk of developing anal cancer than MSM who are not HIV positive (Shiels et al., 2011).
In 2009, the U.S. Food and Drug Administration (FDA) licensed a quadrivalent HPV vaccine, previously licensed for females in 2006, for use in males aged 9 to 26 years, in an effort to reduce the incidence of genital warts (FDA, 2009). In December 2010, the FDA added prevention of anal cancer in males and females as an indication for vaccine use. Data from vaccination trials has shown reductions in persistent HPV infections and genital warts among vaccinated males (Centers for Disease Control and Prevention [CDC], 2010). As with females, HPV vaccination likely offers the greatest benefit when administered before the onset of sexual activity and HPV exposure, hence why it was licensed for males as young as age 9 years (Hildesheim & Herrero, 2007). The vaccine was recently endorsed by the Advisory Committee on Immunization Practices, who recommended routine use for males aged 11 and 12 years, as well as for males aged 13 to 21 years who had not already received the vaccine (CDC, 2011a).
A growing number of studies have been conducted with males to assess their awareness, attitudes, and intentions to receive the HPV vaccine (Allen, Fantasia, Fontenot, Flaherty, & Santana, 2009; Ferris et al., 2009; Gerend & Barley, 2009; Gilbert, Brewer, Reiter, Ng, & Smith, 2011; Jones & Cook, 2008; Petrovic, Burney, & Fletcher, 2011; Reiter, Brewer, McRee, Gilbert, & Smith, 2010; Reiter, Brewer, & Smith, 2010). The studies have generally reported low levels of knowledge and awareness about HPV and the vaccine among adult males. Some males are aware of the vaccine’s existence, although many are not aware that it is available to males (Katz, Krieger, & Roberto, 2011). Knowledge and awareness of the virus and the vaccine appear to be higher among MSM than among males with female sex partners (Gilbert et al., 2011; Reiter, Brewer, McRee, et al., 2010). Across all male populations, interest in vaccination is relatively favorable, although not as high as it is for females, possibly because of lower levels of knowledge and awareness. Predictors of vaccine acceptability for males are similar to those that influence intention to vaccinate among females and include perceived susceptibility to HPV infection, sexual activity, perceived benefits of the vaccine, and perceived norms for vaccination (Liddon, Hood, Wynn, & Markowitz, 2010). However, self-reported estimates among males of vaccine uptake, albeit less than 1 year postlicensure, were quite low, roughly 2% (Reiter, McRee, Kadis, & Brewer, 2011).
Few studies involving males have included adolescent males, both heterosexual and MSM, exactly at the age when they are now encouraged to make a decision, either independently or with a parent, about vaccination. This study specifically targeted African American, urban males living in low-income, low-resource environments, in part, because of the increased prevalence of STIs and risky health behaviors among this population (CDC, 2011b). Exploring awareness of and attitudes toward HPV vaccination among adolescent males is necessary if the goal is to increase HPV vaccination among this age group and ultimately reduce the burden of genital warts and HPV-related cancers in males. While the adolescent male may not be making the decision to vaccinate, their understanding and awareness of the vaccine may trigger discussions with a parent or provider, which could have a positive influence on the decision maker.
Theoretical Framework
The theory of planned behavior (TPB) posits that an individual’s intention to perform a given behavior, in this case one’s intention to get an HPV vaccine, is based on one’s attitudes toward the behavior (positive or negative evaluation of performing the behavior), subjective norms (perception of the social pressures to perform or not perform the behavior), and one’s perceived behavioral control (perception of the ability to perform the behavior; Ajzen, 1991). Behavioral beliefs produce a favorable or unfavorable attitude toward the behavior; normative beliefs result in perceived social pressure or subjective norm; and control beliefs give rise to perceived behavioral control. The TPB is a useful model for predicting a wide range of behaviors and behavioral intentions (Montaño & Kasprzyk, 2008). Educational and public health initiatives designed to increase awareness and intention to vaccinate should be based on the identification of factors linked to the intention to receive the HPV vaccine (Kahn et al., 2008).
Study Purpose and Design
The purpose of the study was to understand knowledge, attitudes, and intentions toward vaccination in a sample of adolescent males, both heterosexual and MSM. The study used a multimethod, exploratory study design to assess factors that could potentially influence young males when deciding about HPV vaccination. Factors were modeled after constructs in the TPB. Self-administered questionnaires and focus group discussions were used to quantitatively and qualitatively explore factors most associated with intent to vaccinate. Although other studies have assessed males’ perspective of the HPV vaccine, none, to our knowledge, have included the voices of a young minority population at elevated risk of HPV infection.
Method
Study Population
Five neighborhoods in Philadelphia were preselected because they had predominately low-income populations. Median household incomes in these five neighborhoods ranged from $13,906 to $37,714, and the percentage of African American adults living in each neighborhood was greater than 75% (U.S. Census Bureau, 2000). We recruited a convenience sample of males aged 13 to 21 years within these neighborhoods during the summer and fall of 2010. Participation in the study was not limited by HPV vaccination status, but none of the males self-reported HPV vaccination. Males self-identified as being primarily heterosexual or MSM and were invited to a particular focus group based on this information. Study sessions were held in the neighborhoods where the males were recruited, at places they were familiar with such as recreation centers, public libraries, nonprofit organizations, and the local community college. All participants gave written consent after research staff read and explained the informed consent document. Because this study was considered low risk and anonymous, parental consent was not warranted. The study was approved by the Institutional Review Board at Thomas Jefferson University.
Self-Administered Questionnaire
At the beginning of each study session, participants completed a self-administered questionnaire about HPV knowledge and awareness, as well as attitudes, subjective norms, perceptions of behavioral control, and intentions regarding the HPV vaccine. The questionnaire included a brief description of the HPV vaccine so that participants who had no prior knowledge of the vaccine were able to answer some questions related to attitudes and intention to vaccinate (“The vaccine is a series of three shots that can protect against human papillomavirus, or HPV. HPV is known to cause almost all cases of genital warts in males, as well as certain cancers like those of the anus and penis”). Awareness of HPV and the vaccine was measured with two items: “Have you ever heard of HPV?” and “Have you ever heard of the HPV vaccine?” We included five items to assess knowledge of HPV and the vaccine (listed in a table in the Results: Questionnaire Data section). Intentions to vaccinate were measured with a single item: “How likely are you to get the HPV vaccine in the next 12 months?” Items consistent with the TPB that measured attitudes, subjective norms, perceived behavioral control, and intentions are listed in a table in the Results: Questionnaire Data section. These items were measured on a 5-point Likert-type scale with “1” representing the most negative response, “3” representing a neutral response, and “5” representing the most positive response.
Focus Group Discussions
Focus groups were moderated by males who had extensive public health training or were graduate students in public health at the time of the study. The moderators were African American, Asian American, or Mexican American and represented the demographic and cultural backgrounds of the adolescent male population. This was intended to increase feelings of familiarity between the moderator and participants, which would foster an environment where an honest discussion on sensitive sexual health topics was possible. Moderators were trained by the principal investigators and the investigator’s team in all aspects of the study protocol, such as obtaining informed consent, administering the questionnaire, and moderating focus groups.
The research team developed the focus group script to elicit discussion around HPV and HPV vaccination, guided by the constructs of the TPB. This included topics such as susceptibility to HPV infection, behavioral, normative, and perceived control beliefs about getting vaccines (in general, and specifically about the HPV vaccine), and decision making about health care in general and HPV vaccination specifically (who makes decisions about your health; where does one look for information when making decisions). If participants were unclear of HPV and the vaccine, the moderators had information that they could read to participants, so that the group could have an informed discussion about the topic. Four of the focus groups consisted exclusively of MSM aged 13 to 21 years, while 6 focus groups consisted of heterosexual males aged 13 to 18 years. Participants were grouped into younger or older males to foster equal participation and avoid domination by older males during the discussions. The same general script was used for all focus groups; slight modifications were made to scripts for each group to make them relevant and culturally appropriate. All focus group discussions lasted roughly 2 hours and were audio recorded. Participants were compensated $20 in cash and two tokens for public transportation.
Data Analysis
For survey items, means, frequencies, and distributions were calculated when appropriate. Bivariate analyses were used to evaluate differences between the two groups of males. A knowledge summary score was calculated for each participant by summing the number of items (out of 5) that were correct; each correct item was worth 1 point and total scores ranged from 0 to 5. Questionnaire items were analyzed using SPSS Version 19.
For focus groups, word document transcripts from the audio-recorded focus groups were produced verbatim by a professional transcription service and verified for accuracy by a moderator that attended the focus groups. Any discrepancy in transcribing was corrected by the moderator so that accurate transcription files were used in analysis. Transcripts were then analyzed by iterative rounds of coding by at least two members of the research team, where specific themes and trends were identified within each transcript and discussed by the research team until final consensus was reached. Themes were identified as topics that consistently occurred across transcripts as well as similarities and differences between transcripts (Ryan & Bernard, 2003). Quotes that appear in this article were selected based on their ability to represent typical responses during the discussion and/or provide insight into the thought process of the adolescents. They do not represent the flow of discussion within one group but are compiled of the most representative responses to the same question across all groups.
Results: Questionnaire Data
Demographics
Seventy-six males completed a baseline questionnaire and participated in 1 of 10 focus groups. The mean number of participants in a focus group was 7. Participants were predominantly African American (84%), with 15% identifying as Hispanic. The median age of participants was 17 years. Fifty-nine percent of males identified as heterosexual whereas 41% identified as MSM. Among all males, 88% reported ever having sex, with a median age of first sexual experience at 14 years of age. There were no significant demographic differences between the heterosexual males and MSM. Data can be found in Table 1.
Participant Characteristics

Awareness and Knowledge of HPV and the Vaccine
From the questionnaire, 42% of all participants had heard of HPV, and 39% had heard about the HPV vaccine. There were significant differences in awareness of HPV and knowing someone who had been vaccinated between the two subpopulations of males. For example, only 18% of heterosexual males had heard of HPV compared with 77% of MSM (χ2 = 27.0, df = 2, p < .001). Only 22% of heterosexual males had heard of the vaccine compared with 61% of MSM (χ2 = 11.4, df = 2, p < .01). Close to 20% of MSM knew someone (either male or female) who had been vaccinated compared with 5% of heterosexual males (χ2 = 4.0, df = 1, p < .05). In terms of knowledge, the mean number of correct items (out of 5) among all participants was 1.66 (SD = 1.4). Among the full sample, 26% percent got all 5 knowledge questions wrong; only 5% of males got all 5 items correct. Males were most likely to know that getting the HPV vaccine would not protect you from other infections such as HIV and were least likely to know that getting the HPV vaccine would not cure you if you already had HPV. Heterosexual males were significantly less knowledgeable about HPV and the vaccine than MSM (t = 4.1, p < .001). These data are presented in Table 2.
Knowledge and Awareness of HPV and the HPV Vaccine
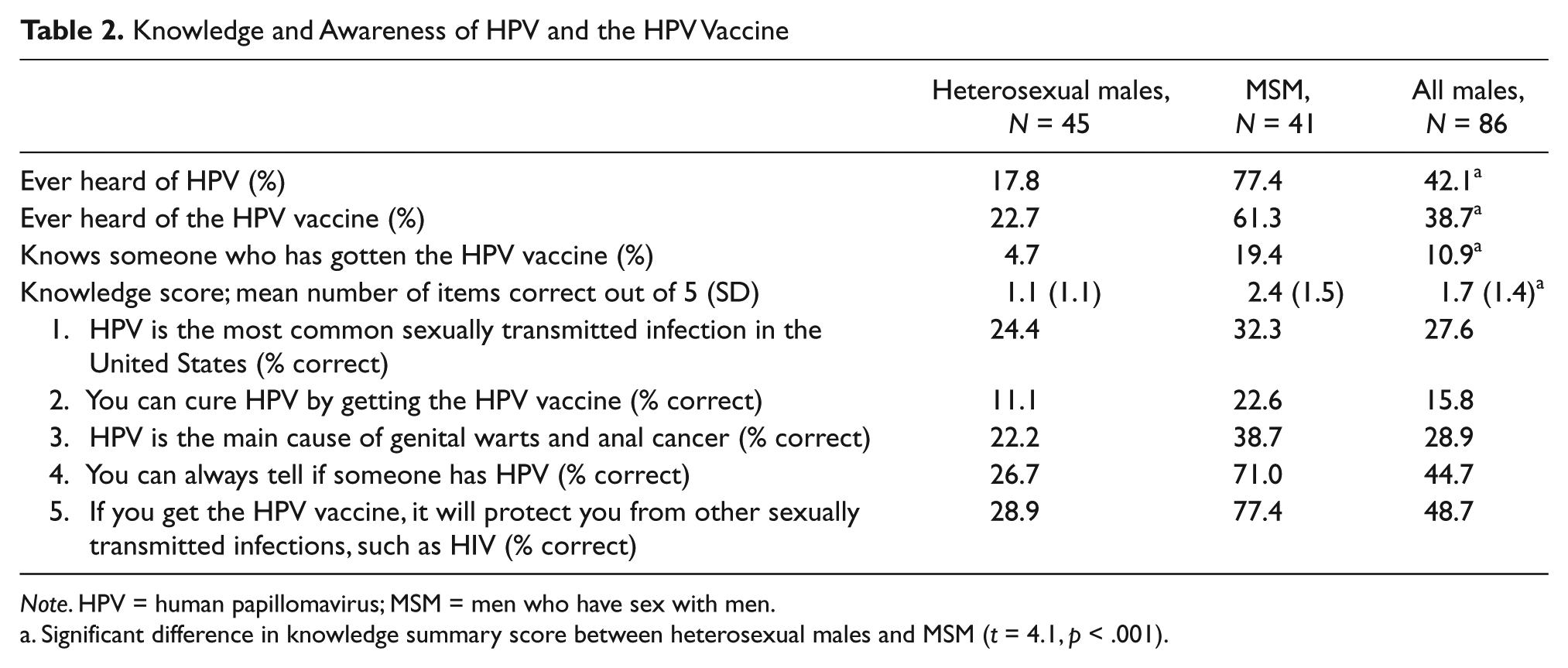
Note. HPV = human papillomavirus; MSM = men who have sex with men.
Significant difference in knowledge summary score between heterosexual males and MSM (t = 4.1, p < .001).
Attitudes, Norms, and Intention to Vaccinate
Mean scores for TPB items identified that participants had moderately favorable attitudes toward HPV vaccination. Participants generally agreed with the statement that getting the vaccine was a “smart” thing to do (M = 3.6, SD = 1.2) but were less likely to agree with the statement relating to subjective norms (“people who are important to me think I should get the HPV vaccine”; M = 3.07, SD = 0.9). Males generally agreed with the statement related to perceived control (“getting the HPV vaccine is completely up to me”; M = 3.8, SD = 1.1). Significant differences were observed between the two subpopulations for the perceived behavioral control items; MSM were more likely to agree that the decision to vaccinate was under their control than heterosexual males. Intentions to vaccinate were lower than attitudes toward vaccination. The mean score for intention to vaccinate was 2.5 (SD = 1.2) among heterosexual males and 2.6 (SD = 1.2) among MSM. There were no significant differences between the two subgroups of males. Mean scores for the TPB items are displayed in Table 3.
Mean Scores (Standard Deviations) of Theory of Planned Behavior Variables a

Note. HPV = human papillomavirus; MSM = men who have sex with men.
All items were measured on a 5-point scale, as 1 = weak, 3 = neutral, 5 = strong.
Significant differences were observed between heterosexual males and MSM by t test (p < .05).
Results: Focus Group Discussions
Awareness and Knowledge of HPV and the Vaccine
Although half of all males had reported awareness of HPV during the questionnaire, discussions in the focus groups revealed that a thorough understanding of the virus and the vaccine was rare. Males in the MSM focus groups were more likely to know that HPV was an STI and that a vaccine was available. Fewer heterosexual males had heard of HPV; some had heard of it by name but were unsure of its meaning or that a vaccine was available to them. For some males who had heard of HPV, it was evident that their exposure had been through vaccine pharmaceutical advertising for females. Therefore, some males thought that the vaccine was strictly available for females. There were frequent misunderstandings about the purpose of vaccines in general, with many males believing that vaccines cure, rather than prevent, disease. Below is a sample of discussion from focus groups illustrating the points mentioned above.
Heterosexual Focus Group
Has anybody heard of HPV?
No, we ain’t never really heard about it.
This is my first time hearing about it. It sounds like a disease, but I don’t know.
Has anyone heard of the HPV vaccine?
Yeah, my sister got that one. It’s for cancer, or something like that.
MSM Focus Group
Has anybody heard of HPV?
I’ve seen the commercials.
From what I noticed from most of the commercials, the commercials generally focus on females and girls because they get some type of cancer or something.
What I’ve heard about HPV is it’s kind of connected to genital warts and herpes. I know some of the side effects are sterility, and I’ve seen images of it, and it looks nasty.
Risky Health Behaviors and HPV Risk Perception
When moderators explained that the HPV vaccine was a form of protection against an STI, participants reported that almost all young adults in their neighborhoods were sexually active. When asked to name STIs that came to mind, males recalled more commonly known STIs such as HIV, chlamydia, and herpes but rarely mentioned HPV. Group discussions with the heterosexual males frequently centered on young men having multiple sexual partners and making poor decisions, such as trusting their partner’s sexual fidelity or apparent lack of disease and agreeing to unprotected sex. MSM also reported risky behaviors among their peers, such as unprotected or improperly protected sex, but seemed to be more aware of the implications of their behavior, possibly because of the history of HIV and prevention efforts in their community. When asked whether they felt that young males are at risk for HPV infection, the general consensus was that they were highly at risk, mostly because of their unprotected sexual behavior. Some males did not feel that they, personally, were at risk because they felt that they were cautious when choosing a sexual partner or had limited experiences for which to be exposed to HPV. The following represents dialogue during the focus groups about risk and perceptions of STI’s in general and HPV specifically.
Heterosexual Focus Group
What do males do that put themselves at risk for STIs?
A lot of people are a lot more sexually active than in the past and they’re not really aware of the risk as opposed to the act itself.
I think young men should be worried about diseases because young males, nowdays, are so fast to get in bed with a female, you know what I’m saying. You don’t know this girl from a can of paint, and she might have everything under the sun.
Do you think that young males are at risk of getting HPV?
Absolutely. They don’t know what it is and they don’t always protect themselves. There are probably a lot of guys who have it [HPV] right now and don’t know it.
MSM Focus Group
Do you think gay males are at increased risk for STIs?
Yeah, but I also think we know more about them, because of HIV.
Too many people don’t know what proper condom use is. They take it out of the wrapper, stick it on, and if it looks right, go right ahead.
The risk is always going to be in the back of your head because you’re wondering if this guys’ infected or is this guy not infected? Like, you don’t know what to do. And he’s so sexy.
Do you think that young gay males are at risk for getting HPV?
Yeah. If you’re at risk for HIV than you’re at risk for HPV. It’s almost like one and the same.
Attitudes, Norms, and Intentions to Vaccinate
In almost all focus groups, regardless of sexual orientation, males presented a similar mix of positive and negative attitudes toward HPV vaccination. In terms of positive reasons to be vaccinated, participants primarily cited issues of protection against a disease that has no cure. Some males considered risk to be an important factor when thinking about intentions to vaccinate. They suggested that males who were at increased risk of contracting HPV, primarily from risky sexual behavior, should more strongly consider vaccination than males who were at lower risk. In terms of negative attitudes toward HPV vaccination, the possibility of side effects was the most common response to why a male might not want to get the vaccine.
Heterosexual Focus Group
What would be good or bad about getting the HPV vaccine?
Any shot that’s helpful, you should get it . . . reduces your risk.
It’s a disease I’ve never heard of, and now I know about it, I want to protect myself against it.
Some of the (vaccines) could be dangerous . . . what if somebody’s system is not strong enough to take the vaccine?
MSM Focus Group
What would be good or bad about getting the HPV vaccine?
You can’t get rid of it [HPV] once you got it, so it’s better to be safe than sorry.
It depends on what kind of a person you are. If you’re, like, free-spirited and want to go sleep with everybody, then maybe it’s a good idea for you to get the vaccination. But, if you’re more introverted, a “to yourself” kind of a person, or a Christian, then maybe not.
Decision Making About HPV Vaccination
During the focus groups, participants frequently cited parents or guardians as people who would be influential in their decision to get vaccinated. A few participants mentioned that some parents, notably fathers, would be less aware of their intentions of getting vaccinated because they felt that fathers were less informed about the purpose of the vaccine. Moreover, for MSM, fathers may be less willing to support their decision to be vaccinated because some do not approve of their sexual identity. Health care providers were also mentioned as an influential source, but to a lesser extent than parents or guardians. Some males felt that they could make the decision about vaccination on their own. This belief was more salient among MSM, who may have made their own health care decisions in the past, particularly related to sexual health. However, other participants noted that in order to make a decision about something, they wanted to be informed about it, and many did not feel sufficiently informed about HPV vaccination to make a decision on their own.
Heterosexual Focus Group
Who would you turn to, if anyone, if you were deciding whether or not to get the HPV vaccine?
It’s really up to you . . . because (the doctors) can’t give you a shot if you don’t want it.
Most people won’t consent to something that they don’t know about. So, I mean, you need to go ahead, ask the right questions, do the homework that you need to do, and then, eventually, decide whether you feel that it’s safe or not.
My grandmother had a problem with this vaccine. In her mind, why would I want to go out and get this [vaccine], when I could just like stay home and try to avoid it [HPV]?
MSM Focus Group
Who would you turn to, if anyone, if you were deciding to get the HPV vaccine?
Well, I know my uncle wouldn’t be helpful because he’s kind of homophobic. This is one of those things that he’d really like to chalk up to being gay. And not so much as protecting yourself.
Me, personally, I wouldn’t ask somebody. I would just go do it [get the vaccine] on my own. I don’t think that me talking to someone would change my mindset of something that I really want to do.
The focus group moderator also enquired about how participants would feel if their sexual partner (either male or female) had received the HPV vaccine. Among the heterosexual males, knowing that a female had received the HPV vaccine generated different types of conclusions. For some, knowing that their female partner had received the vaccine elicited a positive response that she was taking care of her own health. In addition, males saw a benefit to her being vaccinated because it alleviated the possibility that he could infect her with HPV or vice versa. However, some males had a negative reaction to hearing that their partner was vaccinated. Some concluded that if a girl had received the HPV vaccine, it must be because she is sexually promiscuous, or “dirty.” The MSM participants generally concluded that if their partner had gotten vaccinated, that it was a positive benefit to them, in terms of protection from infection. One participant summed up the general consensus of the MSM participants: “Well if he’s getting vaccinated, then I don’t have to worry about it because he’s protecting me as well.”
Discussion
This is one of the first multimethod studies to involve young adult males, both heterosexual and MSM, from low-income, low-resource neighborhoods to better understand their thoughts about HPV and the vaccine. The study used both quantitative and qualitative data to provide insight into cognitions that might influence intent to receive the HPV vaccine. Our exploratory research questions were firmly guided by behavioral theory, in this case the TPB, which is a strength of the study. Additionally, the study went beyond the constructs of the theory to include additional elements of knowledge, awareness, and key influencers of decision making. Few studies, to our knowledge, have provided such in-depth insight into the decision-making process about HPV vaccination among underserved adolescent males who are eligible to receive the vaccine.
The study revealed that many adolescent males, particularly those who were heterosexual, had never heard of HPV or the HPV vaccine prior to being involved in the research study, which is similar to what has been reported with adult males (Gilbert et al., 2011; Reiter, Brewer, McRee, et al., 2010). MSM participants were significantly more aware and knowledgeable about HPV and the vaccine, possibly from their more frequent exposure to messages about HIV and other STIs or more frequent discussions about health issues among their friends and peers. A higher level of awareness and knowledge about the vaccine among gay/bisexual males has been reported in other studies (Reiter, Brewer, McRee, et al., 2010; Simatherai et al., 2009); however, not with males as young as those who participated in our study. Additionally, MSM participants were significantly more likely to feel in control of the decision to vaccinate than heterosexual males, but this may because MSM participants may have more experience in taking care of their sexual health or being tested for HIV.
It is important to note that although knowledge of HPV and the vaccine was quite low, this did not appear to affect vaccine acceptance. Once males were educated about the high prevalence of HPV and the health consequences of infection, attitudes toward vaccination and intentions to vaccinate were moderate to favorable. This has been reported in other studies, although the males were significantly older (Ferris et al., 2009; Gerend & Barley, 2009). This suggests that public health campaigns to educate males about the vaccine are warranted and may cement their interest in wanting to protect their health by vaccination. However, a better understanding of how to increase intentions, the precursor to behavior and the hallmark of the TPB, is necessary, even when attitudes are favorable.
Because HPV vaccination likely offers the greatest benefit if administered before sexual activity, in early adolescence, it is important to understand the attitudes and influences of males who may actually be facing the decision about vaccination. Knowing who the males would involve in the decision-making process, and who influences their normative beliefs about vaccination, is an important first step in creating an educational intervention. The majority of heterosexual males agreed that close relatives, especially females, would influence their decision making about HPV vaccination. The influence of female caregivers over male caregivers in the health care decisions of adolescent males has been documented in the past (Blum, 2002). To a lesser extent, a doctor’s or their partner’s recommendation would also influence their decision making. In other studies involving older adult males, a physician recommendation was a strong influencing factor in decision making (Jones & Cook, 2008; Lenselink et al., 2008). It may be that younger males have easier access to family members than health care providers, and the shift to involving a provider in decisions comes with older age. This may be what occurred, as the heterosexual males, who tended to be younger in age, were more likely to report that a female caregiver would be influential whereas the MSM participants, who tended to be older in age, were more likely to report that their health care provider would be an active decision maker.
Despite the numerous strengths of the study, it is not without limitations. While the study was deliberately designed to hear the voices of young urban males who are at increased risk of infectious diseases, this unique sample may limit the generalizability of the findings. Furthermore, the study was cross-sectional in nature, so it was not possible to determine if intentions among the nonvaccinated lead to actual behavior. Last, the sample size was too small to distinguish which constructs of the TPB were most likely to influence the males’ intent to be vaccinated. However, this study serves as a starting point for documenting how urban adolescent males, both heterosexual and MSM, are thinking, learning, and deciding about HPV vaccination.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by an American Cancer Society Institutional Research Grant at Thomas Jefferson University.