
Abstract
Background:
Previously, we highlighted the benefits of magnified subinguinal varicocelectomy over conservative treatment on the semen of a small group of adolescents with varicoceles. In this report, we presented changes of semen parameters of 47 adolescents who underwent magnified subinguinal varicocelectomy (MSV) and followed-up for 6 months.
Methods:
The present prospective controlled study was conducted on 47 adolescents with varicocele who underwent MSV and were followed up for 6 months. In addition, age and sex-matched patients were added as control group. The primary outcome of this study was to assess the postoperative change in semen analysis parameters.
Results:
A significant increase in sperm volume from 2.5 (1.9–3) to 3.2 (2.6–4) mL at the end of the sixth month of follow-up. Likewise, the sperm count increased from 10.8 (3.51–21.6) to 20.3 (9.6–35) million. Notably, the percentage of rapid and slow sperms increased significantly from a median of 5% (0%–10%) and 15% (10 -20%) to a median of 10% (5%–15%) and 17.5% (15%–25%), respectively. The percentage of sperm with progressive movement increased from 35% (30%–40%) to 59% (45%–69%). The vitality of the sperms increased significantly as well. While the percentage of sperms with abnormal morphology decreased significantly at the end of follow-up.
Conclusion
Our findings support the safety and efficacy of MSV in patients with clinically detectable varicocele. MSV has improved the semen parameters of the included patients, including sperm motility, volume, count, and total progressive motility, which may positively impact their fertility potential.
Background
Varicocele is the most frequent urogenital defect in adolescents that can be surgically corrected (Cayan & Woodhouse, 2007). It affects 6%–8% of people aged 11–14 years and 11% to 19% of people aged 15–19 years (Higuchi et al., 2016). A meta-analysis of 20 articles found that having varicocele in adolescence had a negative impact on sperm forms, count, and motility. However, the treatment appears to result in a moderate increase in sperm concentration and a little enhancement in sperm motility (Nork et al., 2014). In addition, varicocele has an unfavorable effect on the testis function in adolescents as it has been linked to increased DNA fragmentation (Chu et al., 2017).
At adolescence, the testis is still growing; therefore, varicocele should be treated as soon as possible to preserve fertility (Jensen et al., 2017). Recent guidelines, such as the American Urological Association (AUA), recommended treatment of unilateral or bilateral varicoceles with reduced testicular size or semen abnormalities, while the European Association of Urology (EAU) has no distinct recommendations for adolescent varicoceles (Macey et al., 2018). The presence of testicular hypotrophy on the impacted side is an absolute indication for varicocele surgery. Testicular pain, solitary testis with varicocele, poor semen quality, bilateral high-grade varicocele without testicular hypotrophy, and soft testis are all relative criteria for varicocele surgery (Cayan et al., 2005). The number of well-designed studies that evaluated the different procedures or described the optimal strategy for adolescent varicocele therapy is very low. Many various methods, including radiologic, laparoscopic, and open surgical approaches, can be used to treat adolescent varicocele (Cayan et al., 2005; Lurvey et al., 2015).
The optimum treatment for adolescent varicocele is to ligate all internal and external spermatic veins while keeping the spermatic arteries and lymphatics intact. Sclerotherapy or radiologic embolization of spermatic veins looks to be a less invasive treatment (Chan, 2011). However, it has a failure rate of up to 15% and requires considerable expertise and experience. In addition, in traditional varicocelectomy without optical magnification, tiny internal spermatic veins may be missed, causing subsequent dilation and recurrence (Paduch & Skoog, 2001). On the other hand, the testicular artery, lymphatic, and tiny venous networks can all be seen at microscopic magnification. As a result, the microsurgical technique significantly reduces the risk of hydrocele development, testicular artery damage, and varicocele recurrence (Salama & Blgozah, 2014).
Previously, we highlighted the benefits of magnified subinguinal varicocelectomy over conservative treatment on the fertility outcomes of a small group of adolescents with varicoceles. In this report, we presented the 6-month fertility outcomes of 47 adolescents who underwent magnified subinguinal varicocelectomy (MSV) at our centers.
Materials and Methods
The protocol of the current trial was approved by the local ethics committee of faculty of medicine for girls Al-Azhar University, Cairo, Egypt (number not applicable). All procedures run in compliance with the standards of the Declaration of Helsinki (JAVA, 2013). Written informed consent was obtained from all patients before enrollment.
Study Design and Patients
The present prospective cohort study recruited adolescents with varicocele who were scheduled to undergo MSV at AlZahraa University Hospital through the period from December 2018 to January 2022. Patients were recruited if they aged 15–19 years and had clinically detectable varicocele (Dubin & Amelar, 1970), then confirmed diagnosis of refluxing varicocele by Doppler ultrasound with cutoff testicular volume 12 mL or more (Tanner 4 and 5), using the commonly accepted color Doppler ultrasound criterion of 3 mm or greater vein diameter for varicocele. We included adolescents who showed abnormalities in semen analysis and clinically reduced testicular size; the clinically reduced testicular size was defined as a smaller testis than the other size by visual inspection or reduced size compared with previous examinations or Doppler ultrasound. We excluded patients with delayed puberty, azoospermia patients, patients with atrophic testis (volume <12 mm), and/or patients with chromosomal abnormalities. Patients were divided into an intervention (MSV) group and a control group, which were followed for 6 months. The control group consisted of adolescents with varicocele who did not undergo MSV and signed the written informed consent to be enrolled in the study. The decision to divide patients into MSV or control groups was based on the surgeon’s discretion.
MSV
All patients were assessed preoperatively and postoperatively (after 3 and 6 months) according to the institution’s standards. Besides, all patients underwent ≥ two preoperative semen analyses, which were performed after ≥ 3 days of abstinence and 1 month from the least abnormal semen findings. Two samples of semen analysis for each patient were obtained after 3 months postoperatively in the same laboratory after 3 days of abstinence. All individuals were provided instructions on sample collection, including collection after self-stimulation into a clean container. Samples were immediately provided to the laboratory. The samples were then assessed using the World Health Organization (WHO) 5th edition, which required a cutoff of ≥4% and a strict morphometric assessment of the sperm characteristics.
The same surgeon performed all procedures. Patients underwent spinal or general anesthesia according to the surgeon’s decision. Then, a three-cm skin incision was done over the external inguinal ring transversely. The Camper’s and Scarpa’s fascias were separated to reach the spermatic cord, which was situated over Penrose drain using a Babcock forceps. An 8× to 15× microscope was employed to identify gubernacular and cremasteric veins and sparing the artery. These veins were tied by 4-0 or 5-0 vicryl sutures followed by incision of spermatic fascias; the vas deferens and its vessels were examined and suited in the posterior fascial compartment to create a window between vas and vessels using the Penrose drain or forceps. We made another window between the internal spermatic vessels and the external spermatic fascia and its structures. The internal spermatic arteries were then freed from the surrounding veins and irrigated with diluted warm papaverine; the surrounding veins were ligated by 4 or 5-0 vicryl, sparing the internal spermatic artery and lymphatic vessels. We closed the spermatic fascia, subcutaneous tissue using 3-0 or 4-0 Vicryl sutures followed by subcuticular closure of the skin using 4-0 Proline or 4-0 Vicryl. The incision was infiltrated with 0.5% Marcaine solution with epinephrine, and a dry sterile dressing was applied. All patients were followed up for 6 months after the operation.
Study’s Outcomes
The primary outcome of this study was to assess the change in semen analysis parameters (sperm volume, count, motility, vitality, and percentage of abnormal morphology) 6 months after the procedure. The secondary outcomes were to describe the incidence of postoperative complications and the changes in testicular volume and varicocele grade.
Statistical Analysis
Retrieved data were summarized and processed with IBM SPSS statistical software (version 25). Frequencies were used to describe the presentation, side, retrograde flow/reflux, and postoperative complications. However, age, testicular volume, hormonal assays findings, testicular volume, and semen analysis parameters were summarized, according to normality, into mean (±standard deviation [SD]) or median (interquartile range [IQR]). The hypothesize of significant changes in semen analysis parameters over the study period was testing using paired t-test or Wilcoxon rank test, according to data normality. p-value <.05 was regarded as statistically significant.
Results
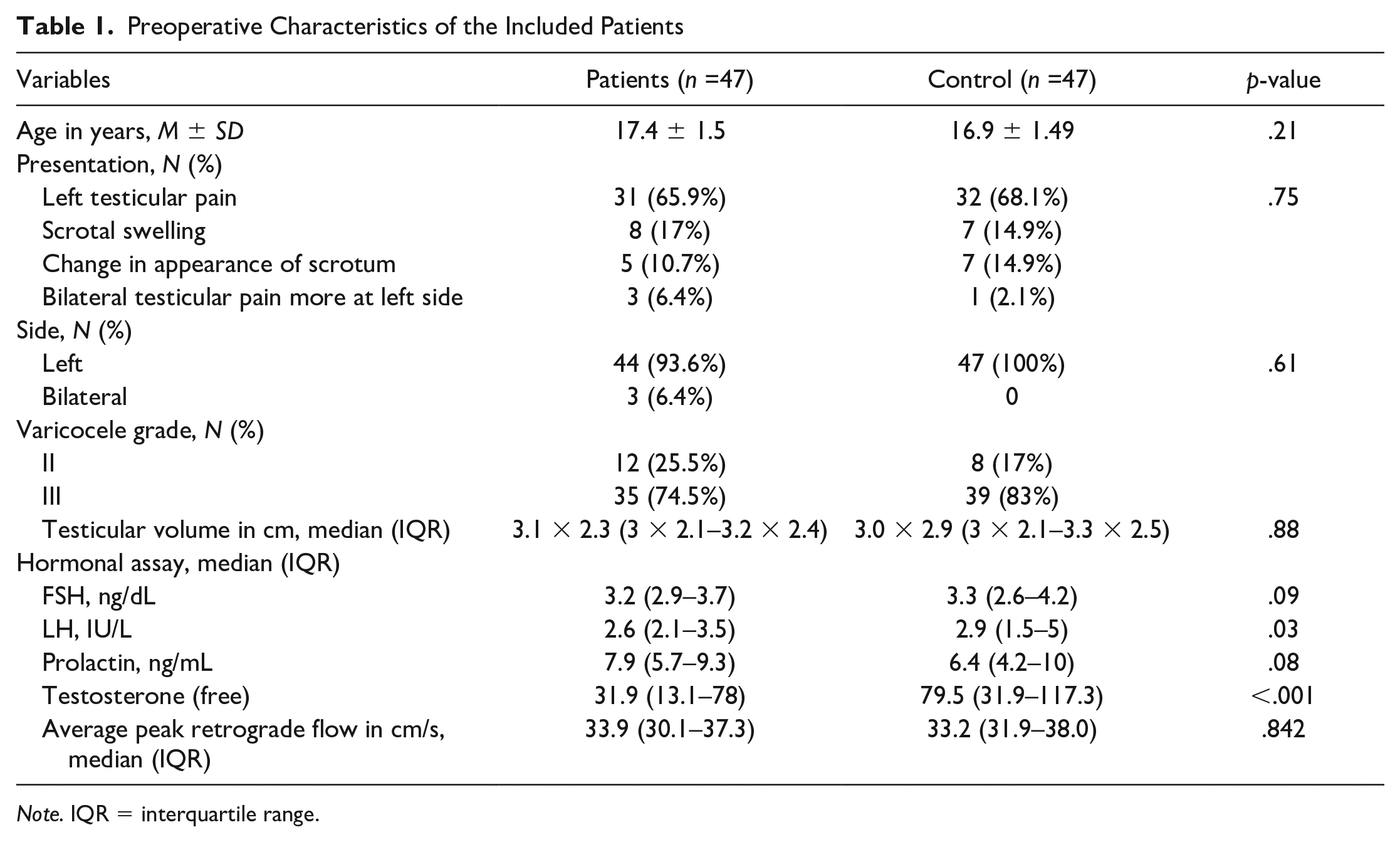
A total of 47 patients were included in each group. The mean age of the included patients in the MSV group was 17.4 ± 1.5 years. The majority of the patients had left testicular pain at presentation (65.9%), and 17% had scrotal swelling. Besides, nearly 94% of the patients had left-sided varicocele, and 74.5% of the encountered varicoceles were of grade III. The median (IQR) testicular volume was 3.1 × 2.3 (3 × 2.1–3.2 × 2.4) cm. Concerning hormonal assay, the median (IQR) FSH and LH was 3.2 (2.9–3.7) and 2.6 (2.1–3.5) ng/dL, respectively (Table 1).
Preoperative Characteristics of the Included Patients
Note. IQR = interquartile range.
Semen analysis demonstrated a significant increase in the sperm volume from 2.5 (1.9–3) to 3.2 (2.6–4) mL at the end of the sixth month of follow-up. Likewise, the sperm count increased from 10.8 (3.51–21.6) to 20.3 (9.6–35) million (Figure 1). Notably, the percentage of rapid and slow sperms increased significantly from a median of 5% (0%–10%) and 15% (10%–20%) to a median of 10% (5%–15%) and 17.5% (15%–25%), respectively. The percentage of sperm with progressive movement increased from 35% (30%–40%) to 59% (45%–69%). The vitality of the sperms increased significantly as well. While the percentage of sperms with abnormal morphology decreased significantly at the end of the follow-up (Table 2).

A Column Graph Showing the Degree of Change in Each Patient
The Change in Semen Analysis Parameters, Testicular Volume, and Peak Retrograde Flow Six Months After the Operation

Note. IQR = interquartile range.
Concerning the secondary outcomes of this study, the median (IQR) testicular volume increased significantly from 3.1 × 2.3 (3 × 2.1 – 3.2 × 2.4) cm at preoperative stage to 4.1 × 2.3 (3.1 × 2.1 – 5.1 × 2.4) cm. However, 43 patients (89.4%) had Grade 0 at the end of follow-up, and the rest of the patients had Grade I varicocele. Minimal complications were encountered postoperatively in the form of mild scrotal edema in three cases, one case of mild hydrocele unilaterally, no recurrent cases reported, or testicular atrophy.
Discussion
From the perspective of experts, the optimal treatment strategy for varicocele in the adolescent population is varied. Some surgeons believe that surgical repair is preferable to a conservative approach, whereas others disagree (Baazeem et al., 2011). The latest version of the AUA guideline varicocele repair for adolescents with detectable unilateral or bilateral varicoceles. However, the EAU guidelines state that adolescent varicoceles are less likely to lead to infertility, and it is often overtreated (Macey et al., 2018). Retroperitoneal, inguinal, and subinguinal techniques are the three surgical varicocele correction methods. The retroperitoneal operation is done laparoscopically, whereas the inguinal and subinguinal approaches are generally made using a surgical loupe or an operative microscope (Paduch & Skoog, 2001; Van Batavia et al., 2013). A randomized clinical trial on 120 patients with palpable varicoceles who underwent varicocelectomy showed that the microscopic group had no postoperative hydrocele compared with 20% in the laparoscopic group. Furthermore, only one patient in the microscopic group had a recurrence, compared with seven patients in the open group and nine in the laparoscopic group (Al-Kandari et al., 2007).
The effectiveness and safety of laparoscopy versus microsurgery in the surgical treatment of varicocele were compared in a meta-analysis involving 554 patients. The microsurgery group had a reduced postoperative frequency of hydrocele and a lower rate of recurrence, but a longer operation duration (Wu et al., 2017). Compared with laparoscopic surgery, another meta-analysis of 1178 patients found that microscopic surgery reduced complication, hospital stay, and recurrence rate while increasing sperm density (Wang & Ji, 2020). In addition, pediatric urologists were issued a questionnaire on the best strategy for treating pediatric varicocele. According to the responses, the subinguinal microsurgical technique was the most popular (51%), followed by inguinal (24%) and laparoscopic (14%) approaches (Lee et al., 2016). The MSV approach, according to experts, should be the standard gold technique for varicocelectomy since it properly analyzes the complete anatomical vasculature of the spermatic cord, resulting in improved surgical results (Al-Kandari et al., 2018).
Our findings demonstrated that MSV significantly improved sperm volume, count, motility, progressive movement, and vitality in this study. On the other hand, the abnormal morphology has been significantly reduced six months postoperative. Our findings were similar to those of Sallam and his team, who compared the conservative method and the MSV in 40 patients with refluxing varicocele. They reported that varicocele grade, sperm count, volume, motility, vitality, and progressive movement have significantly improved in the MSV group compared with the conservative method group. Thus, they concluded that MSV is a superior conservative method in treating patients with symptomatic varicocele (Sallam et al., 2021).
Paduch and Niedzielski studied children aged 10 to 20 years in prospective research. The surgical group had a substantial rise in terms of testicular volume (from 15.7 to 17.5 mL), but the conservative group had no significant change (from 14.7 to 15.9 mL). Paduch and Niedzielski also found that in the surgical group, the width of the pampiniform vein decreased from 2.8 to 2 mm (p0.0001), whereas in the conservative group, the diameter decreased from 2.9 to 2.8, with no significant difference (Paduch & Niedzielski, 1997). Spinelli et al. observed that surgical intervention improved outcomes significantly when compared with a conservative strategy. After 6 months of follow-up, they found that 77.2% of patients in the surgical group had a higher than 20% change in testicular volume than 37.1% in the conservative group (Spinelli et al., 2010). In contrast, 173 adolescents with varicocele were monitored by Moursy et al. The conservative group and the surgical group had similar mean testicular volumes; however, the surgical group had a greater percentage of testicular catch-up growth (Moursy et al., 2013).
MSV with testicular delivery (TD) was linked with a greater postoperative complication rate but a lower recurrence rate and postoperative serum testosterone level than MSV without TD, according to a recent meta-analysis of seven studies. However, they did not find any significant difference between both techniques in terms of pregnancy rate, sperm motility and concentration, operation time, and preoperative serum testosterone level (Liao et al., 2019). Tian et al. conducted a retrospective study to evaluate the role of MSV with TD and vein stripping. Their findings demonstrated that this technique is safe and effective in reducing varicocele recurrence and scrotal pain. In addition, they observed a substantial improvement in the progressive sperm counts (Tian et al., 2020). To explore the factors associated with varicocele recurrence after MSV, Alkhamees and his colleagues conducted a retrospective study on 34 married male patients with varicocele. They observed a significant association between advanced grade on the left side and large vein diameter before and after surgery with an increased recurrence rate (Alkhamees et al., 2020).
This study is one of few reports that evaluated the benefits of MSV over conservative treatment on the fertility outcomes of adolescents with varicoceles. However, we acknowledge that this study has certain limitations. Data regarding postoperative testicular size and average peak retrograde flow were unavailable for the control group; hence, we could not compare them between the study’s groups. Another limitation is that the study was based on a single-center experience only, which limits the generalizability of our findings. Finally, the limited number of patients evaluated reduced the strength of our results.
In conclusion, our findings support the safety and efficacy of MSV in patients with varicocele. Furthermore, MSV has improved the semen parameters of the included patients, including sperm motility, volume, count, and total progressive motility, which may positively impact their fertility potential.
Footnotes
Author Contributions
S.E.S. developed the study concept, development, and data collection, performed the statistical analysis, and performed manuscript writing. K.S. performed data interpretation, provided critical revision for important intellectual content, and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
The protocol of the current trial was approved by the local ethics committee of faculty of medicine for girls Al-Azhar University, Cairo, Egypt (No applicable number). All procedures run in compliance with the standards of the Declaration of Helsinki (JAVA, 2013). Written informed consent was obtained from all patients before enrollment.
Consent for Publication
Not applicable.
Availability of Supporting Data
The data set used or analyzed during the current study is available from the corresponding author upon reasonable request
Availability of Data and Materials
Data available on request.