
Abstract
We performed a systematic review and meta-analysis on efficacy and safety of holmium laser enucleation of prostate compared with bipolar technologies in treating benign prostatic hyperplasia. We analyzed several databases such PubMed, Embase, and Web of Science. Two reviewers independently reviewed studies for consistent criteria and extracted relevant data. Reviewers independently assessed the risk of bias and strength of the evidence for the body of the literature. Ten randomized controlled trials including 1,157 participants were included in this meta-analysis. The holmium laser group had favorable perioperative outcomes in this study. The holmium laser group identified shorter catheterization duration and shorter hospital stay duration than the bipolar technologies group. Efficiency outcomes, such as International Prostate Symptom Score, peak urinary flow rate, quality of life, postvoid residual urine volume, and international index of erectile function reported no obvious differences between the holmium laser and bipolar technologies groups at the 6 to 12 months follow-up. Bipolar technologies and holmium laser groups shared equivalent effectiveness and safety in treatments for benign prostate hyperplasia. Holmium lasers identified lower catheter times, shorter hospital stays, and lesser risk of hemorrhage than bipolar technologies.
Introduction
Benign prostate hyperplasia (BPH) has a high incidence rate and is a common disease encountered in the urology department. It can cause lower urinary tract symptoms (LUTSs), which undermine the quality of life (Gratzke et al., 2015). After the 1960s, several people have resorted to surgical operation for symptomatic relief. Treatment modalities range from watchful waiting, medication, and surgical treatment (Dörsam & Altwein, 2009; Rieken & Bachmann, 2014). Patients in whom symptoms are not relieved by medications and those who develop complications require further surgical operations.
Since the 1980s, with the rapid advancement in minimally invasive endovascular technologies, open surgical procedures are losing popularity (Oelke et al., 2013). Transurethral operation techniques comprise resection, enucleation, and vaporization. The operation tools involve monopolar energy, bipolar energy, holmium laser, greenlight laser, thulium lasers, and diode lasers (Cornu, 2016). More recently, a quantity of reviews and meta-analyses conducted on the merits and drawbacks of transurethral operations had proven that bipolar technologies and holmium laser shown advantages over reducing TURP syndrome and fitness for any prostate size (Mamoulakis et al., 2009; Rieken & Bachmann, 2014). Meanwhile, enucleation is closely related to removal of a larger volume of prostate tissue, greater decline in prostate-specific antigen (PSA), more refined peak urinary flow rate (Qmax), and greater decrease in the International Prostate Symptom Score (IPSS; Cornu, 2016; Oh & Shitara, 2020).
Since 2010, numerous systematic reviews and meta-analyses have compared individual laser technology treatments against either monopolar transurethral resection of the prostate (M-TURP) or bipolar technology against M-TURP. To our knowledge, no systematic review or meta-analysis has compared holmium laser enucleation with bipolar technology (enucleation and resection; C. Gu et al., 2020). The clinical effectiveness and safety of holmium laser enucleation of prostate (HoLEP) and those of bipolar transurethral resection of the prostate (B-TURP) have been studied in a meta-analysis; however, this study contains more randomized controlled trials (RCTs) and includes subgroup analysis between two bipolar technologies (enucleation and resection; Qian et al., 2017). To compare the clinical efficacies and differences in efficiency, perioperative outcomes, and the safety of holmium laser enucleation and bipolar technologies in patients with BPH, we conducted a meta-analysis.
Method
Research Design
We perform this meta-analysis and systematic review of RCTs in accordance with the preferred reporting items for systematic reviews and meta-analyses (PRISMA) checklist (Liberati et al., 2009).
Data Sources and Searches
PubMed, Embase and Web of Science databases were searched to compare the efficacy and safety of HoLEP versus bipolar technologies (bipolar techs) in treating patients with BPH. The searches were limited to studies in the English language. A systematic search was carried out of databases stated above in December 2020 using the search using the terms: ((Hyperplasia) OR (Hyperplasia, Prostatic) OR (Prostatic Hypertrophy) OR (Adenoma, Prostatic) OR (Adenomas, Prostatic) OR (Prostatic Adenomas) OR (Prostatic Adenoma) OR (Benign Prostatic Hyperplasia) OR (Prostatic Hyperplasia, Benign) OR (Prostatic Hypertrophy, Benign) OR (Benign Prostatic Hypertrophy) OR (Hypertrophy, Benign Prostatic)) AND ((Laser Enucleation) OR (HoLEP)) AND ((OR (Plasmakinetic Resection))). In addition, two reviewers individually conducted the review of the retrieved articles. Any disagreement was reconciled by consensus.
Inclusion Criteria and Exclusion Criteria
We defined the inclusion and exclusion criteria before the research was performed. Inclusion criteria include the following: (1) The article fell into the RCT category; (2) the article incorporated patients who suffered from symptomatic LUTS caused by BPE; (3) the article provided precise and complete data that could be analyzed, primarily comprising assessment of the effectiveness and safety of holmium laser technology compared with bipolar technology (enucleation or resection); and (4) follow-up duration is more than or equal to 6 months. Articles were excluded if they were not clinical trial, such as abstract, review, or comment; meanwhile, animal experiments or studies with incomplete data were also excluded. Study selection and elimination was performed according to the PRISMA flow diagram (Figure 1).

Preferred Reporting Items for Systematic Reviews and Meta-Analyses Flow Diagram
Data Extraction
Two reviewers individually recorded the relevant information: author; publication year; number of included patients; prostate volume; effectiveness outcomes, including Qmax, IPSS, quality of life (QoL), postvoid residual urine volume (PVR) and five-item version of the International Index of Erectile Function (IIEF-5); and perioperative outcomes, including hospital stay time, catheterization duration, hemoglobin loss and serum sodium loss and complications such as retention of urine, transient incontinence, urinary tract infection (UTI), capsule perforation, bladder neck contracture, and blood transfusion. When mean and SD data were missing, an estimated mean and SD was calculated according to the methods recommended by Luo et al. (2018) and Wan et al. (2014). Ethical issues and conflicts of interest are not required because our study is on the basis of open source data. We assess publication bias by means of a funnel plot. And we list the baseline characteristics of the selected articles in Table 2.
Quality Assessment
The quality of each included RCT was evaluated in line with the Cochrane risk of bias tool. With respect to outcome variables in the included trials, each item was classified as “low” risk, “high” risk, and “uncertainty” of bias. Quality assessment was conducted in six domains: selection bias, performance bias, detection bias, attrition bias, reporting bias, or other bias. Begg’s method was used to evaluate publication bias. Inconsistencies in the assessment of quality were evaluated by consensus among two authors. Sensitivity analysis or subgroup analysis was implemented in case of high heterogeneity. Mean difference with 95% confidence intervals was applied to describe continuous variables (Figures 2 and 3).

Risk of Bias Graph

Risk of Bias Summary
Results
We found 330 studies using the aforementioned search strategy. After reviewing titles and abstracts, 218 were excluded; 10 more studies were ruled out for random approaches and blinding experiments. A total of 10 RCTs were finally included and were used to analyze the differences in efficiency, perioperative outcomes, and the safety of patients with BPH (Bhandarkar, 2017; Y. B. Chen et al., 2013; Elshal et al., 2020; Fayad et al., 2011, 2015; M. Gu et al., 2018; Habib et al., 2020, 2021; Neill et al., 2006; Shoma et al., 2016). Patients who suffered from symptoms caused by BPH were included in each included shared similar assessment outcomes, such as hospital stay time, catheterization duration, IPSS, and Qmax. The baseline characteristics of the selected trials are displayed in Table 1.
The Details and Baseline Characteristics of Individual Study.

Note. M ± SD (range). IPSS = International Prostate Symptom Score; Qmax = maximum urine flow rate; PSA = prostate specific antigen; PVR = postvoid residual; RCT = randomized controlled trial; HoLEP = holmium laser enucleation of prostate; NA = no available; e: enucleation.
Postoperative Effectiveness Outcomes
Qmax
Six RCTs comprising 652 participants were included in the analysis of Qmax. In the postoperative 6 months to 1 year of follow-up, the bipolar technology and HoLEP groups reported comparable Qmax values (MD = −0.41; 95% CI = [−1.18, 0.36]; p = .30; Figure 4).

Qmax Between Holmium Laser Enucleation of Prostate and Bipolar Techs
IPSS
Six studies comprising 638 subjects discussed data on IPSS. We found no significant differences in the pooled data between the bipolar technology and HoLEP groups (MD = 0.16; 95% CI = [−1.41, 1.74]; p = .84) during the 6 months to 1 year postoperative follow-up phase (Figure 5).

IPSS Between HoLEP and Bipolar Techs
PVR
Four RCTs including 468 participants were analyzed for changes in PVR. We found no significant difference in PVR between the bipolar technology and HoLEP groups (MD = −0.90; 95% CI = [−4.85, 3.04; p = .65) during the 6 months to 1 year postoperative follow-up period (Figure 6).

PVR Between HoLEP and Bipolar Techs
QoL
Three RCTs comprising 666 patients were selected for analysis of the quality of life (QOL) scale. The bipolar technology and HoLEP groups had comparable QOL scores (MD = −0.06; 95% CI = [−0.14, 0.02]; p = .16) during the 6 months to 1 year postoperative follow-up period (Figure 7).

QoL Between HoLEP and Bipolar Techs
IIEF-5
Four RCTs including 468 participants were analyzed for IIEF-5. There was no significant difference in IIEF-5 (MD = 0.04; 95% CI = [−0.57, 0.65]; p = .89) in the collected data between bipolar technology and HoLEP groups during the 6 months to 1 year postoperative follow-up period (Figure 8).

IIEF-5 Between HoLEP and Bipolar Techs
Perioperative Variables
Hospital Stay
With respect to hospital stay duration, we analyzed data of five RCTs comprising 617 participants. The studies identified higher heterogeneity (p < .00001, I2 = 88%) with HoLEP group being significantly different than bipolar technology group in hospital stay duration (MD = −5.84; 95% CI= [−10.71, −0.97]; p = .02) in the perioperative variables as measured by forest plots (Figure 9).

Hospital Stay Duration Between HoLEP and Bipolar Techs
Hemoglobin Loss
Data related to change in hemoglobin levels were evaluated from three RCTs comprising 325 patients. A higher heterogeneity was indicated between studies (p < .00001, I2 = 89%). A significant difference was shown by random-effects model between the HoLEP and bipolar technology groups (MD = −0.48; 95% CI = [−1.05, 0.08]; p < .0001) in decreased hemoglobin loss (Figure 10).

Hemoglobin Loss Between HoLEP and Bipolar Techs
Serum Sodium Loss
To analyze serum sodium loss, we studied four RCTs with 389 participants. A fixed-effects model did not report significant difference in serum sodium loss between HoLEP and bipolar technology groups (MD = −0.07; 95% CI = [−0.53, 0.67]; p = .82) in perioperative variables (Figure 11).

Serum Sodium Loss Between HoLEP and Bipolar Techs
Operation Duration
An integrated data from four studies comprising eight RCTs comprising 916 participants identified no significant differences in operation duration (MD = 2.03; 95% CI= [−13.20, 17.26]; p = .79) between HoLEP group and bipolar technology group (Figure 12).

Operation Duration Between HoLEP and Bipolar Techs
Catheterization Duration
The criterion for catheter removal is that the urine color remains clear after the irrigation is stopped (Y. B. Chen et al., 2013; Habib et al., 2020, 2021; Neill et al., 2006). For study of catheterization duration, we analyzed data from four RCTs comprising 529 patients. A higher heterogeneity was pointed out among studies (p = .03, I2 = 66%). The forest plots indicated that the HoLEP group had remarkable preference as compared with the bipolar technology group (MD = −5.84; 95% CI = [−10.71, −0.97]; p = .02) in the perioperative outcomes (Figure 13).
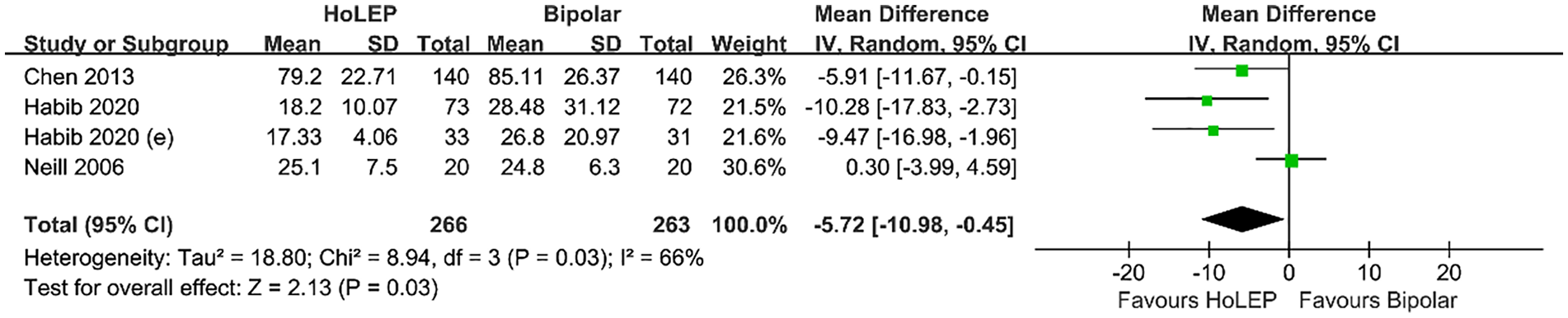
Catheterization Duration Between HoLEP and Bipolar Techs
Complications
Table 2 presents the postoperative complication events. There was no marked difference in transient incontinence, retention of urine, capsule perforation, bladder neck contracture, blood transfusion, and urinary tract infection (UTI) between the bipolar technology and HoLEP groups.
Postoperative Conditions.

Note. HoLEP = holmium laser enucleation of prostate; UTI = urinary tract infection.
Discussion
BPH is a progressive disease characterized by prostate enlargement, which consequently causes LUTS and other conditions (Gratzke et al., 2015). In 1995, Gilling et al. introduced holmium laser in urologic surgical procedures as a tool to support and enrich the treatment of BPH. They developed a new operative method using holmium laser for the treatment of prostatic adenoma. Subsequently, Gilling et al. introduced the morcellator and combined morcellation with holmium laser resection to invent a new surgical method. The superiority of this new method was that it could be used on prostate gland of any size (Gilling et al., 1995, 1996). HoLEP and bipolar technology have become popular for surgical treatment of BPH in the recent years. Compared with M-TURP, these two technologies have proven effectiveness and are safe to use. HoLEP and bipolar technology have a promising prospect for application and may in future replace M-TURP (C. Gu et al., 2020).
We performed this meta-analysis of 10 RCTs comprising 1,157 participants to compare the efficacy and safety of the HoLEP and bipolar technology (resection or enucleation) in treating BPH. The HoLEP group reported better outcomes, such as shorter hospital stays, shorter duration of catheterization, lesser loss of hemoglobin and serum sodium, and lesser possibility of blood transfusion than the bipolar technology group. Overall, HoLEP identified a more promising prospect than bipolar technologies for patients undergoing symptomatic BPH.
In this meta-analysis, HoLEP displayed superior perioperative outcomes than bipolar technologies. Shorter catheterization duration, shorter hospital stays, and lower hemoglobin loss were seen in the HoLEP group than in the bipolar technologies group. Reduced hemoglobin loss was observed in HoLEP group compared with bipolar resection group. This could be attributed to favorable hemostasis, a more concentrated and lighter resection depth, and a more efficient and targeted coagulation (Shvero et al., 2021). HoLEP is recommended in patients with high bleeding risk and prostate of any size (the larger the volume of prostate, the easier it is to bleed). Lower chance of hemoglobin loss also contributes to reduced risk of hematuria, which further affects the hospital stay and catheterization duration. The significance of hospital stay duration and catheterization duration was still meaningful in subgroup analysis when compared in HoLEP and bipolar resection group. There was no significant difference found between HoLEP and bipolar enucleation, which indicates that enucleation method also reduces bleeding risk.
Efficiency outcomes, such as IPSS, Qmax, QOL, PVRU, and IIEF-5 at the 6 to 12 months follow-up phase reported no significant difference between HoLEP and bipolar technology groups. Similarly, in the subgroup analyses, we did not notice any significant differences. The efficiency outcomes of our study concur with those of published literature that compared holmium laser enucleation with bipolar technology.
We noticed no significant differences in complications between HoLEP group and bipolar technology group with respect to rates of retention of urine, transient incontinence, urinary tract infection, capsule perforation, and bladder neck contracture (Table 2). With regard to transfusion, the p value is equal to .05. Theoretically, HoLEP is advantageous in reducing adverse events such as hematuria. Our study demonstrated reduced hemoglobin loss in the HoLEP group than in the bipolar resection group. Further studies are required to explain this observation. This meta-analysis shows that HoLEP achieved better outcomes in safety and efficiency.
Limitations
This meta-analysis and systematic review included 10 RCTs. We could not collect data of RCTs comparing HoLEP to bipolar vaporization and the outcome of our article may also be influenced by subjective factors such as selection and publication bias. J. Chen et al. (2022) mentioned in his study that for prostate volume less than 100 mL, HoLEP has advantages over monopolar technology in perioperative outcomes. We can speculate that HoLEP has certain advantages in the comparison between HoLEP and bipolar technology. We still need to include more RCTs to prove our conclusion. More high-quality RCTs with appropriate study design are required to increase the sample size and verify the efficacy and safety of HoLEP technologies compared with bipolar technologies in treating BPH.
Conclusion
Bipolar technology and HoLEP were shown to be effective and safe treatment modalities for BPH. Compared with bipolar technology, HoLEP reduces the catheterization time, hospital stay, and risk of hemorrhage that in effect reduces the need of blood transfusion. The learning curve for HoLEP has been studied in several reports. Thus, we believe that HoLEP should be proposed as a potential new gold standard surgical therapy instead of TURP for patients with BPH, especially those at high risk of bleeding.
Footnotes
Acknowledgements
Throughout the writing of this paper, I have received a great deal of support and assistance. I would first like to thank my mentor, Pro Zhang, whose expertise was invaluable in formulating the research questions and methodology. Your insightful feedback pushed me to sharpen my thinking and brought my work to a higher level. In addition, I would particularly like to acknowledge my team members, Yumeng Chai & Zhongbao Zhou, for their wonderful collaboration and patient support.
Author Contributions
Conceptualization: All authors; Methodology: All authors; Formal analysis and investigation: X.C., Z.Z., Y.Chai, Y.Cui; Writing-original draft preparation: X.C., Z.Z., Y.Chai, Y.Cui; Writing—review and editing: Z.Z., Y.Z.; Supervision: Z.Z., Y.Z.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
No ethical approval and patient consent are required.
Consent to Publish
Not applicable.
Availability of Data and Materials
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.