
Abstract
The purpose of this study was to promote the holmium laser enucleation of the prostate (HoLEP) technology for large-volume prostates (>80 ml) and compare it with the traditional method, we modified the technique and applied this technology to clinical practice. A retrospective study comprising 118 patients who underwent HoLEP surgery from February 2018 to December 2019 was conducted in our center. Group A consisted of 57 patients with large-volume prostate (>80 ml) who received modified “fenestration and tunnel method” from February 2019 till December 2019, while group B consisted of 61 patients who received the traditional trivalvular operation method from February 2018 to December 2018 for comparison. Control subjects are selected such that they match the cases concerning certain characteristics, and perioperative data, voiding outcomes, and complications were evaluated at 1- and 12-month follow-up. The international prostatic symptomatic score (IPSS), quality of life (QoL), and maximum flow rate (Qmax) at 1 month and 12 months were both significantly improved compared with the preoperative baseline, and no significant differences were found between Groups A and B. The mean enucleation time, operation time, catheter indwelling duration, and hemoglobin decrease during the operation of Group A showed superiority compared with Group B (p<.05). The modified “fenestration and tunnel method” of HoLEP was statistically superior to the traditional trivalvular method in terms of the operation time, enucleation time, catheter indwelling duration, and hemoglobin decrease. For large-volume prostates (>80 ml), modified HoLEP was suggested to be a better treatment option.
Keywords
Introduction
Benign prostatic hyperplasia (BPH) is one of the most common medical problems in aging people, occurring in about 80% of men by the 8th decade of their life (Abedi et al., 2020; Jeon et al., 2019). Holmium laser enucleation of the prostate (HoLEP) has recently become the recommended treatment for prostate in all sizes in BPH surgery (Abedi et al., 2020; Large & Krambeck, 2018; Robert et al., 2018; Vincent & Gilling, 2015). Nowadays, HoLEP is recommended by the current guidelines of the European Association of Urology (EAU) in men with substantially enlarged prostates (>80 ml) as the first choice (Zhang et al., 2020). The traditional trivalvular method of surgery has become the most popular way to undergo a HoLEP all over the world. However, HoLEP has also been criticized for its long operative time, steep learning curve, and higher cost (Tan et al., 2003). Therefore, our center modified the traditional method to increase the efficiency of the HoLEP procedure in large-volume prostate. In this study, we present the modified “fenestration and tunnel method” HoLEP, and retrospectively analyze and compare the validity and safety between the traditional trivalvular method and the modified fenestration and tunnel method.
Materials and Methods
Patients
A retrospective study consisting of 118 patients was conducted at our center. Patients with large-volume prostate (>80 ml) were stratified into two groups according to operation method; Patients of Group A received modified fenestration and tunnel methods from February 2019 to December 2019 (n = 57), and patients of Group B received the traditional trivalvular operation method from February 2018 to December 2018 (n = 61). Inclusion criteria were as follows: (1) prostate volume > 80 ml; (2) surgical history of HoLEP in our hospital; (3) followed up for at least 1 year after surgery. Patient with cancerous diseases, previous prostate surgery history, bladder calculus, neurogenic bladder dysfunction, urethral stricture, or coagulopathy was excluded from this analysis.
Primary indicators including the International Prostate Symptom Score (IPSS), quality-of-life (QoL), peak urinary flow rate (Qmax) were reassessed at 1 month and 12 months. Perioperative data including enucleation time, total operation time, serum hemoglobin decrease, catheter indwelling duration, and some relevant complications were collected according to medical history. In addition, the proportion of transient urine leakage (TUL), which referred to persistent urine leakage after catheter removal for more than 24 hr but less than 3 months (Tokatli et al., 2020), was measured to compare the safety of the two methods.
All operations were performed by the same experienced surgeon capable of both operations using a 550-μm end-firing laser fiber and an 80-W Versa pulsed holmium laser (Raykeen China). The power setting was 80 W at 2 J/s and 40 Hz. Transurethral morcellation was performed with a 26 F nephroscope (Storz, Tuttlingen, Germany) using a mechanical morcellator (VersacutMorcellation; Lumenis, Inc., USA.). An irrigating catheter was inserted after surgery. Bladder irrigation was applied if necessary until hematuria resolved. The standard for catheter removal was clear urine without gross hematuria.
Traditional Trivalvular Method (Figure 1)
Gilling’s method was applied to accomplish the traditional trivalvular group, which enucleated the median and lateral lobes independently in retrograde fashion by making three longitudinal incisions from the apex to the bladder neck (Gilling et al., 1996; Oh, 2019; Tokatli et al., 2020). The first step of this HoLEP procedure was to create bladder neck incisions at the 5- and 7-o’clock positions down to the surgical capsule. And the second step was to enucleate the median lobe. The bladder neck at the 5-o’clock position and 7-o’clock position was incised vertically to the verumontanum. The median lobe was then detached from the bladder neck and allowed to float into the bladder for later morcellation (Gilling et al., 1996). The third step was to core out the side lobes. The bladder neck incisions were lengthened laterally and circumferentially to undermine the lateral lobes below. A sweeping motion on each side was made while making an incision in the bladder neck at the 12-o’clock position. Finally, the upper part of the lateral lobe was gradually withdrawn from the capsule and gradually returns to the verumontanum to join the lower incision; hemostasis was achieved by defocusing the bundle in the bleeding vessels. The urethral morcellator was used to remove tissue after hemostasis.
Illustrations of the Traditional Trivalvular Method.
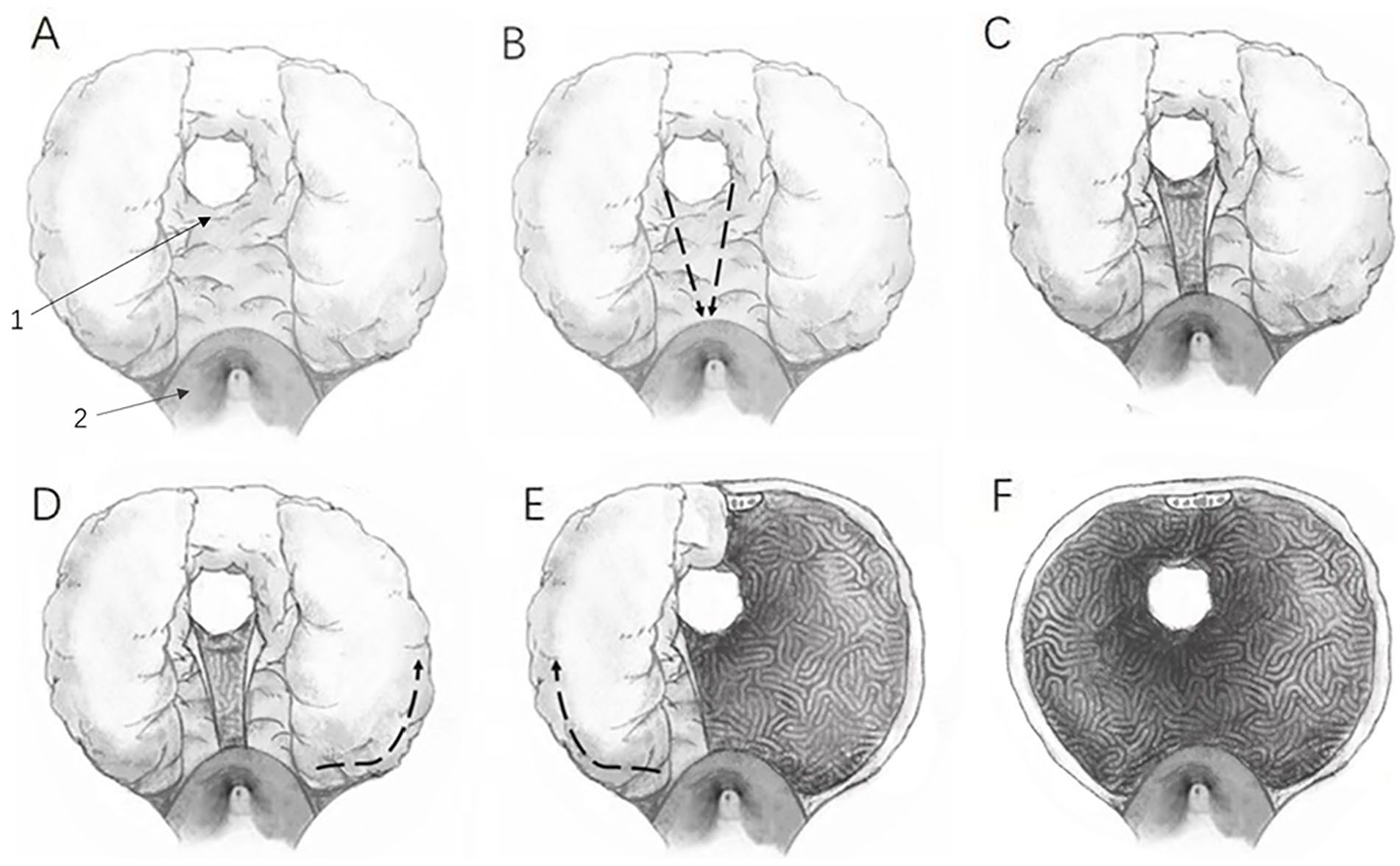
Modified Fenestration and Tunnel Method (Figure 2)
The first step of our modified HoLEP procedure was to expose the surgical capsule of the prostate before the apex. After careful observation and confirmation of the location of the verumontanum, external urethral sphincter, and the neck of the bladder, the initial incision was retrogradely made in the front of the verumontanum (at 6 o’clock) to expose the surgical capsule of the prostate at the apex. The second step was to fenestrate at the bladder neck. After confirming the position of the bladder neck, a longitudinal incision was built in the 6-o’clock direction of the anterior bladder neck deep to the surgical capsule. The third step was to dig a tunnel beneath the middle lobe from the apex to the bladder neck along with the surgical capsule. With the open incision made by prior procedures, it was potential to avoid the prolonged surgery time or injury to the bladder neck caused by the excessive volume of the prostate throughout the dug tunnel.

Illustrations of the Modified Holmium Laser Enucleation of Prostate Procedure and the Schematic of Benign Prostatic Hyperplasia.
The fourth step was to enucleate the lateral lobe. The left lateral lobe was then separated from the anterior prostate tissue. By turning the laser resectoscope, we can enucleate the left lateral lobe from 6 to 12 o’clock counterclockwise. During the operation, the laser-laser shaft resectoscope was used to blunt the left lateral lobe and detach it from the operating capsule. Notably, good exposure of the surgical capsule after the laser resectoscope sheath was depressed actually accelerates enucleation of the lateral lobe. It was dug at 6 o’clock. Because there was a non-existent median lobe left to enucleate, we could enucleate the right lateral lobe, in the same way, starting from the tunnel near the verumontanum in a clockwise direction. Pay attention to the protection of the urethral mucosa when dealing with the apex of the prostate to avoid tearing off the long segment of the mucosa.
The final step was hemostasis and morcellation. Once the entire prostate was totally mobilized and pushed into the bladder, hemostasis is achieved by defocusing the beam on bleeding vessels. Morcellator is then inserted into the bladder to morcellate the entire enucleated prostatic tissue.
Statistical Analysis
The statistical software SPSS 26.0 was used for data analysis. All measurement data were analyzed with a two-tailed Student’s t test and are shown as mean ± SD. The results with p ≤ .05 were considered as statistical significance. Odds ratios with 95% confidence intervals were used to estimate the relationship between independent and dependent variables.
Results
No significant differences were found between the two groups in terms of patients’ baseline characteristics: age, prostate volume, and prostate specific antigen level (Table 1). The IPSS, QoL, and Qmax (Table 2) were assessed before operation and at 1 month and 12 months after operation. The Qmax data of 21 patients were missing (9 in Group A; 12 in Group B) due to lack of in-hospital urinary flow rate examination because these patients were unwilling to visit hospital 12 months after operation; IPSS and QoL assessment was accomplished by telephone call. All patients had improved IPSS, QoL, and Qmax at 1 month and 12 months compared with preoperative data. However, there was no statistical difference between Groups A and B. Two patients who received conventional surgery had transient post-surgery urinary leakage. No patients had long-term urinary incontinence.
Characteristics of Patients.

Note. Values are expressed as means ± SD. PSA = prostate-specific antigen.
Follow-Up Data.

Note. N of PSA: Group A: n = 48, Group B: n = 49. Values are expressed as means ± SD. PSA = prostate specific antigen; Post-OP = postoperative; mo = month(s); IPSS = international prostate symptom score; Pre-OP = preoperative; QoL = quality of life score; Qmax = maximum urinary flow rate.
The enucleation time was 48.96 ± 5.89 min in Group A, which was significantly lower than Group B (53.00 ± 5.58 min) (Table 3, p < .001). There was no significant difference in terms of morcellation time between the two groups. The decrease of hemoglobin in Group A (0.96 ± 0.18) was significantly lower than that in Group B (1.32 ± 0.19), p < .001. The catheter duration time in Group A was shorter than that in Group B, p < .001.
Perioperative Data.
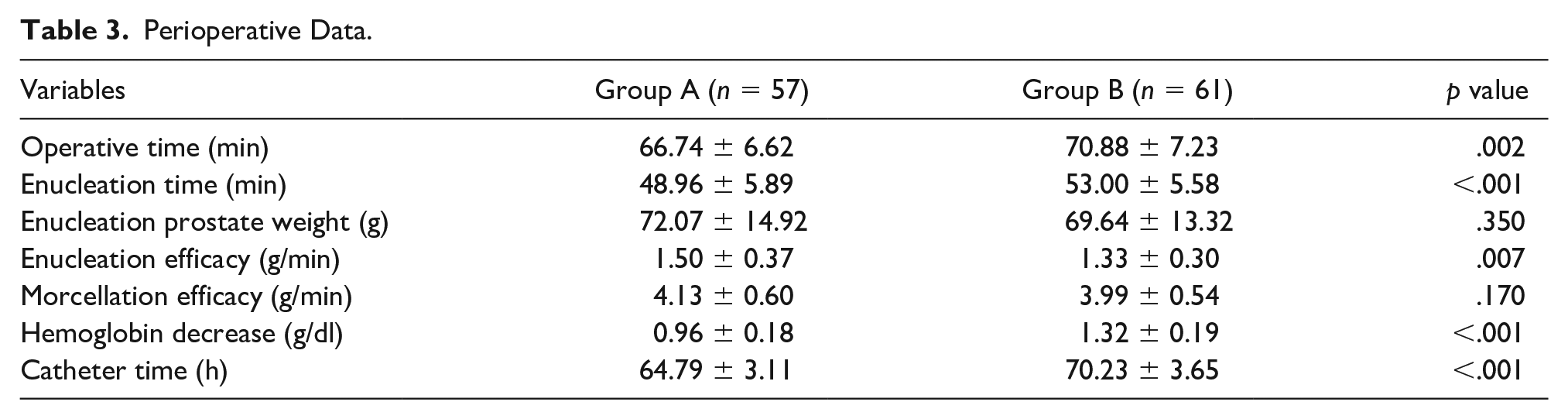
Two patients in Group B and one patient in Group A received intraoperative blood transfusion (two units of red blood cell suspension and 200 ml of plasma) due to blood pressure changes. There was no prostatic capsule perforation in both groups.
Discussion
HoLEP has been proven to be a safe and efficient therapeutic option in patients with large prostates (Kim et al., 2015; Krambeck et al., 2010). In general, compared with TURP, HoLEP is a complicated procedure, and long-term training limits its application in clinical and urological practice (Minagawa et al., 2015). Since the development of trivalvular technology, HoLEP has gained great popularity and demonstrated excellent surgical results (Large & Krambeck, 2018). However, it is concerned that the prevalence of stress urinary incontinence after HoLEP (4.9%–12.5%) was reported higher than it after open prostatectomy (3%–9%) or conventional TURP (approximately 2%) for BPH (Elmansy et al., 2011; Vavassori et al., 2008). Furthermore, if the depth of the three longitudinal incisions of the trivalvular technique does not coincide, especially if the prostate is large, a residual adenoma may remain due to the formation of multiple operating levels (Oh, 2019). Since it is difficult for a surgeon to discern the surgical capsule in a large prostate when the prostatic tissues are adherent to the surgical capsule when bleeding (Xu et al., 2016).
To solve all these problems mentioned above, our center modified a new technique called “fenestration and tunnel method.” In contrast to the trivalvular enucleation procedure, we began enucleation at the apex of the prostate by cutting a short horizontal incision going deep into the level of the surgical capsule in the front of the verumontanum with only 20 to 30 se, while it costs more than 5 min to find the right layer in the traditional way. After that, if the prostate is small (<80 ml), we usually perform a tunnel directly from the horizontal incision along the surgical capsule using the laser up to the 6-o’clock position of the bladder neck, and reduce the speed as we approach the bladder neck and upwarp the head of the cystoscope sheath appropriately. When finding something like circular fibers and the color change (the color of the water seen through the prostate tissue), it indicates the right time to go through the tunnel for the laser fiber is probably approaching the bladder neck. The possibility of peritoneal penetration and sphincter injury is likewise greatly decreased through this measure (Xu et al., 2016).
However, for giant prostates (volume >80 ml), reaching the bladder neck through an instantaneous tunnel approach faces several difficulties (Qian et al., 2017). It takes a longer distance to tunnel through and is likely to be additionally tougher to seek out the precise location of the penetration. The probability of damaging the sphincter muscle is also increased especially when the prostate protrudes into the bladder or when the intraoperative view is not clear enough with mass bleeding. Therefore, for large-volume prostate enucleation, we tend to build a longitudinal incision at the 6-o’clock position of the bladder neck deep to the surgical capsule first. Then a tunnel is made along with the surgical capsule from the incision of the prostate apex to the incision of the bladder neck. According to a previous study, the learning phase for this technique of small prostate only took 2 months (Xu et al., 2016), and in our experience so far, it takes less than 1 month for surgeons to learn the tunneling method of large-volume prostate if the tunneling method for small-volume prostate has been mastered. We excluded eight cases of large volume in January 2019 because they were used for training new surgical.
Anatomically, the prostate tissue at 6-o’clock position has much fewer blood vessels compared with that at 5- and 7-o’ clock position (Sievert et al., 2008). Starting enucleation at 6-o’clock position may probably prevent vessels from being damaged; instead, we could find vessels and stop the bleeding under direct vision.
The inner muscle layer of the urethral sphincter surrounds the urethra completely and consists of smooth muscle fibers and elastic tissue. The smooth muscle layer can be subdivided into an outer layer with a more circumferential orientation and an inner layer with a longitudinal orientation (Walz et al., 2010). The retrograde dissection of the apex in the trivalvular may stretch an inner longitudinal-oriented layer around the apical gland, while with the modified method, we could evaluate under direct vision so as to avoid damage to the urethral sphincter (Endo et al., 2010). In addition, since large-volume prostatic hyperplasia tends to project beyond the seminal colliculus toward the urethra, it is important to avoid excessive urethral mucosal damage while removing the hyperplastic gland as much as possible when dealing with the prostate apex. Also, studies indicate that shortening the enucleation time can decrease the incontinence rate by diminishing the holmium laser exerts on the sphincter (Minagawa et al., 2015).
In addition, prostate shape plays a significant role in the surgical treatment of BPH (Yalcin et al., 2019). For patients sharing a similar volume of the prostate, those with a transverse diameter of prostate greater than the longitudinal diameter have shorter enucleation times. We suppose that patients with shorter longitudinal diameters have an advantage in tunneling and removing the lateral lobe using a modified approach (Walz et al., 2010; Yu et al., 2018).
IPSS date, QoL, and Qmax at the 1 month and 12 months demonstrate no significant difference between Groups A and B, and the results of these two kinds of treatments are almost equivalent to those of previous studies (Enikeev et al., 2016; Gong et al., 2012; Large & Krambeck, 2018; Zhang et al., 2020).
There are several limitations of this study. As it is a retrospective study with a low level of evidence, a prospective study is needed to confirm the efficacy and safety of the fenestration and tunnel method. Meanwhile, special caution is required in citing the conclusion for all operations were performed by the same experienced surgeon. For inexperienced surgeons, the conclusion may differ, and the learning curve of this technique needs further evaluation.
Conclusion
HoLEP, with high efficacy and safety, could be a better treatment option for large-volume prostates (>80 ml). The modified “fenestration and tunnel method” was statistically superior to the traditional trivalvular method in terms of operation time, enucleation time, catheter indwelling duration, and hemoglobin decrease. The modified “fenestration and tunnel method” could be regarded as a safer and more efficient method of HoLEP surgery for large-volume prostate.
Footnotes
Author Contributions
Y.-C.T. and Z.-W.W. designed the research, analyzed the data, and wrote the draft manuscript. Y.-B.C., Q.C., and Y.-C.T. performed literature search, extracted, and analyzed the data. M.G. and Z.W. were responsible for reviewing the manuscript and providing critical scientific input. All authors made contribution to this article, read, and approved the final version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Ethical approval and informed consent was waived by the local Ethics Committee of Shanghai Ninth People’s Hospital in view of the retrospective nature of the study and all the procedures being performed were part of the routine care.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from the multi-center clinical research project of Shanghai Jiao Tong University School of Medicine (grant number DLY201809).