
Abstract
Transurethral resection of the prostate (TURP) is the gold-standard classical method for the treatment of benign prostatic hyperplasia (BPH). In minimally invasive surgery, holmium laser enucleation of the prostate (HoLEP) is considered an alternative option. In this systematic review and meta-analysis, we aimed to comprehensively evaluate the advantages and disadvantages of TURP and HoLEP the treating BPH. We comprehensively searched PubMed, Cochrane Library, EMBASE, and Web of Science databases for all randomized controlled trials published before 1 December 2022 comparing HoLEP and TURP. The study protocol is registered on INPLASY (DOI: 10.37766/inplasy2023.5.0065). Compared with TURP, HoLEP required longer operation time but shorter catheter duration, hospital stay, and bladder irrigation time, as well as less postoperative irrigation. With HoLEP, maximum urinary flow rate at 12 and 24 months after surgery; post-void residual volume at 1, 6, and 12 months; and International Prostate Symptom Score at 12 months after surgery were superior to those with TURP. HoLEP was associated with significantly lower risk of hyponatremia, blood transfusion, and urethral stricture but greater risk of postoperative dysuria. Compared with TURP, HoLEP had better curative efficacy at 6, 12, and 24 months after operation and lower incidence of adverse events in patients with BPH.
Keywords
Introduction
A considerable number of older male patients develop benign prostatic hyperplasia (BPH), which can cause obvious lower urinary tract symptoms and seriously affect the patient’s life. 1 , 2 In clinical work, transurethral incision of the prostate and transurethral resection of the prostate (TURP) are widely used to relieve the patients’ symptoms, with good curative efficacy. 3 In view of its efficacy and safety, TURP has become the gold standard for the treatment of BPH. 4 , 5 However, new minimally invasive surgical procedures have been developed and applied in the clinic to reduce the possible harm to patients caused by TURP, such as postoperative bleeding and transurethral resection syndrome. Among these new surgical procedures, holmium laser enucleation of the prostate (HoLEP), proposed by Gilling et al. 6 is considered an attractive alternative for TURP owing to its shallow penetration and excellent hemostatic properties.
Previous studies have compared HoLEP with TURP but these have failed to reach a unanimous conclusion. Some studies suggest that HoLEP has better long-term curative efficacy and a lower incidence of complications. 7 , 8 However, the results obtained by Jhanwar et al. do not support this view. 9 Zhong et al. 10 conducted a systematic review to comprehensively analyze the advantages and disadvantages of HoLEP and TURP. Their results showed that HoLEP offered safer clinical outcomes with less bleeding and potentially better long-term relief of bladder outlet obstruction in patients with small to mid-sized prostates. However, none of the randomized controlled trials (RCTs) included in that systematic review compared the outcomes among patients with a large prostate and those taking anticoagulant or antiplatelet drugs. Cornu et al. 11 also compared several transurethral procedures for benign prostatic obstruction. However, in comparing the curative efficacy and postoperative adverse events of different surgical procedures, their findings were relatively limited and failed to reflect comprehensive and dynamic changes in the patient's condition.
In view of the above limitations, we conducted the present systematic review and meta-analysis with additional RCTs included, aiming to provide a detailed evaluation of HoLEP and TURP and obtain more comprehensive and robust conclusions.
Methods
We conducted this systematic review and meta-analysis according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). 12 PRISMA is an evidence-based minimum set of items for reporting systematic reviews and meta-analyses that can be used as a basis for reporting reviews of different types of research. We registered our study protocol on INPLASY (DOI: 10.37766/inplasy2023.5.0065). Owing to the nature of this systematic review and meta-analysis, the study protocol did not require ethics approval or the consent of participants.
Search strategy
We comprehensively searched the PubMed, Cochrane Library, EMBASE, and Web of Science databases for RCTs published before 1 December 2022 that compared HOLEP and TURP. The search was performed with the following Medical Subject Headings: “holmium laser enucleation of the prostate” (or “HoLEP”), “transurethral resection of the prostate” (or “TURP”), “benign prostatic hyperplasia” (or “BPH”), and “prostate.” The reference lists of all included studies were also checked for any additional relevant publications. The detailed search strategy is presented in Supplementary Table 1.
Inclusion and exclusion criteria
The inclusion criteria were as follows: (1) research participants were patients with BPH; (2) intervention measures included TURP and HoLEP; (3) research results were related to curative efficacy and safety of TURP and HoLEP; (4) the study was an RCT.
The exclusion criteria were as follows: (1) duplicate publications, reviews, editorials, abstracts, comments, case reports, animal studies, or an expert consensus or guidance; (2) studies involving prostate cancer.
Data extraction
Two reviewers independently screened the identified publications according to the titles and abstracts and selected relevant studies that met the eligibility criteria. Data were extracted and collated independently by the same two reviewers, with any disagreement settled by a third reviewer. An e-mail was sent to the original investigators to request data that were lacking in the publications.
The following items were extracted: (1) basic information: name of the first author, publication date, sample size, demographic data of participants; (2) perioperative results: operation time, mean resected prostatic weight, catheter duration, hospital stay, bladder irrigation time, intraoperative irrigation, postoperative irrigation; (3) primary outcome data related to curative efficacy: maximum urinary flow rate (Qmax), post-void residual volume (PVR), International Prostate Symptom Score (IPSS); (4) secondary outcomes: American Urological Association (AUA) symptom score, a quality of life (QoL) score to reflect the patient’s subjective feelings regarding their QoL, International Index of Erectile Function 5 (IIEF-5), postoperative transrectal ultrasound (TRUS) measurement of the prostate volume, level of prostate specific antigen (PSA), detrusor pressure at maximum flow (PdetQmax), Schäfer grade; (5) occurrence of adverse events: incidence of hyponatremia, blood transfusion, recatheterization, urinary incontinence, urinary retention, urethral stricture, urinary tract infection, reoperation, transurethral resection syndrome, postoperative fever, and dysuria.
Statistical analysis
The present meta-analysis was conducted using Review Manager software (RevMan 5.4; Cochrane Collaboration, Oxford, United Kingdom). Continuous data are expressed as weighted mean difference (WMD) and 95% confidence interval (CI). For means that were too different or inconsistent units of measurement, the data are expressed as standardized mean difference and 95% CI. For dichotomous variable data, we used the Mantel–Haenszel method. Cochran’s Q test and Higgins’ I2 statistical test were used to assess statistical heterogeneity. With results showing low heterogeneity (I2 < 50%), a fixed-effects model was used. For results with significant heterogeneity (I2 ≥ 50%), sensitivity analysis and subgroup analysis were conducted to find the source of heterogeneity. If the heterogeneity could not be eliminated, a random-effects model that estimated the uncertainty of results with sampling error and between-studies variance was used. Descriptive analysis was used for data that could not be merged.
Risk of bias in the included studies was assessed by two authors using RevMan 5.4. The following seven domains of the included studies were assessed as “high risk,” “unclear risk,” or “low risk”: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other biases. Finally, a funnel plot was used to visually assess potential publication bias.
Results
Search results and study characteristics
We retrieved a total of 1224 articles; of these, 464 remained after excluding duplicate articles. After reading the title and abstract, 363 articles were eliminated, leaving 101 publications. Of these, 83 articles were discarded for various reasons (retrospective study, review article, case report, expert consensus or guidance) in a full-text review during further screening. Finally, 18 studies7–9,13–27 met the inclusion criteria (Figure 1). The characteristics of the 18 studies involving 2150 participants are summarized in Table 1. The included study participants were from different countries and regions and were mainly in their 60s and 70s.
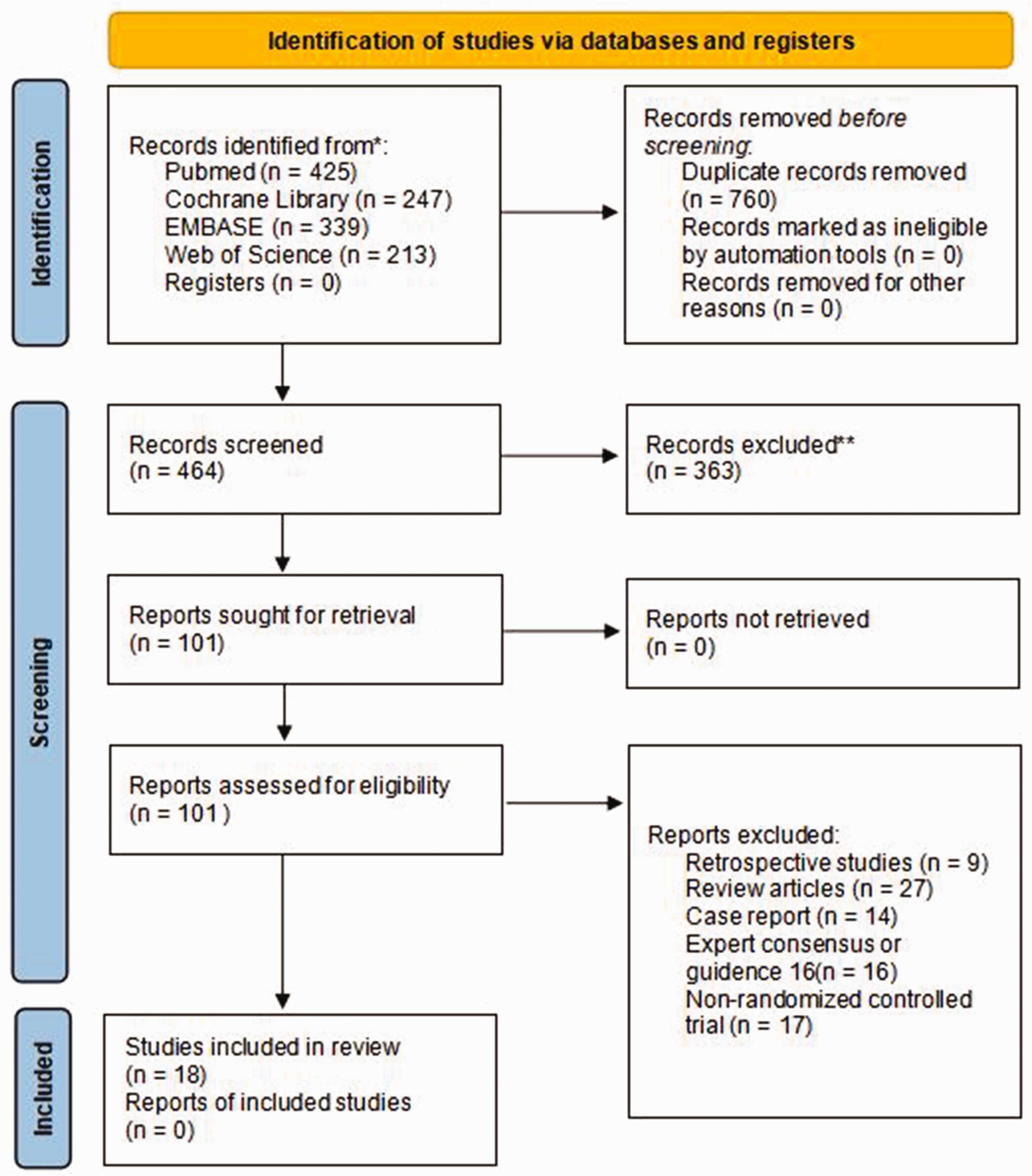
Flow chart of study selection.
Characteristics of the included studies.
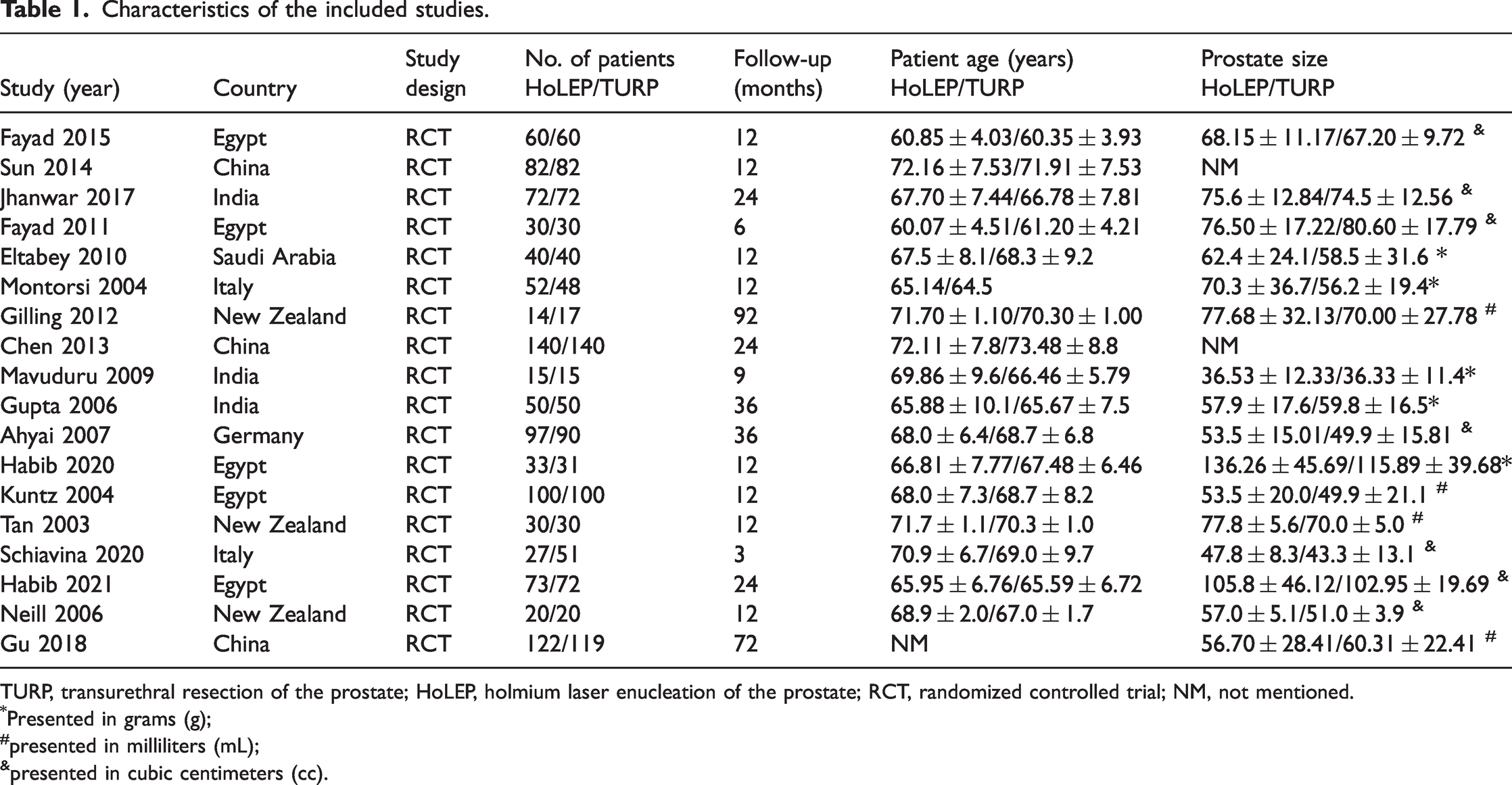
TURP, transurethral resection of the prostate; HoLEP, holmium laser enucleation of the prostate; RCT, randomized controlled trial; NM, not mentioned.
Presented in grams (g);
presented in milliliters (mL);
presented in cubic centimeters (cc).
Perioperative results
The results showed that HoLEP was significantly associated with longer operation time (WMD: 11.02; 95% CI: 1.18 to 20.85; p = 0.03; I2 = 98%), shorter catheter duration (WMD: −15.73; 95% CI: −21.37 to −10.08; p < 0.0001; I2 = 91%), shorter hospital stay (WMD: −15.50; 95% CI: −21.95 to −9.04; p < 0.0001; I2 = 96%), shorter bladder irrigation time (WMD: −13.13; 95% CI: −21.93 to −4.33; p = 0.003; I2 = 97%), and less postoperative irrigation (WMD: −7.18; 95% CI: −10.69 to −3.67; p < 0.0001; I2 = 80%). There was no significant difference in mean resected prostatic weight and intraoperative irrigation (Figure 2).

Forest plot of the perioperative results.
Primary outcomes
Qmax
In the HoLEP group, higher Qmax was detected at 12 (WMD: 0.88; 95% CI: 0.12 to 1.65; p = 0.02; I2 = 75%) and 24 (WMD: 0.99; 95% CI: 0.42 to 1.57; p = 0.0007; I2 = 0%) months after surgery, but there was no significant difference in Qmax at 1, 3, 6, and 36 months after operation (Figure 3).
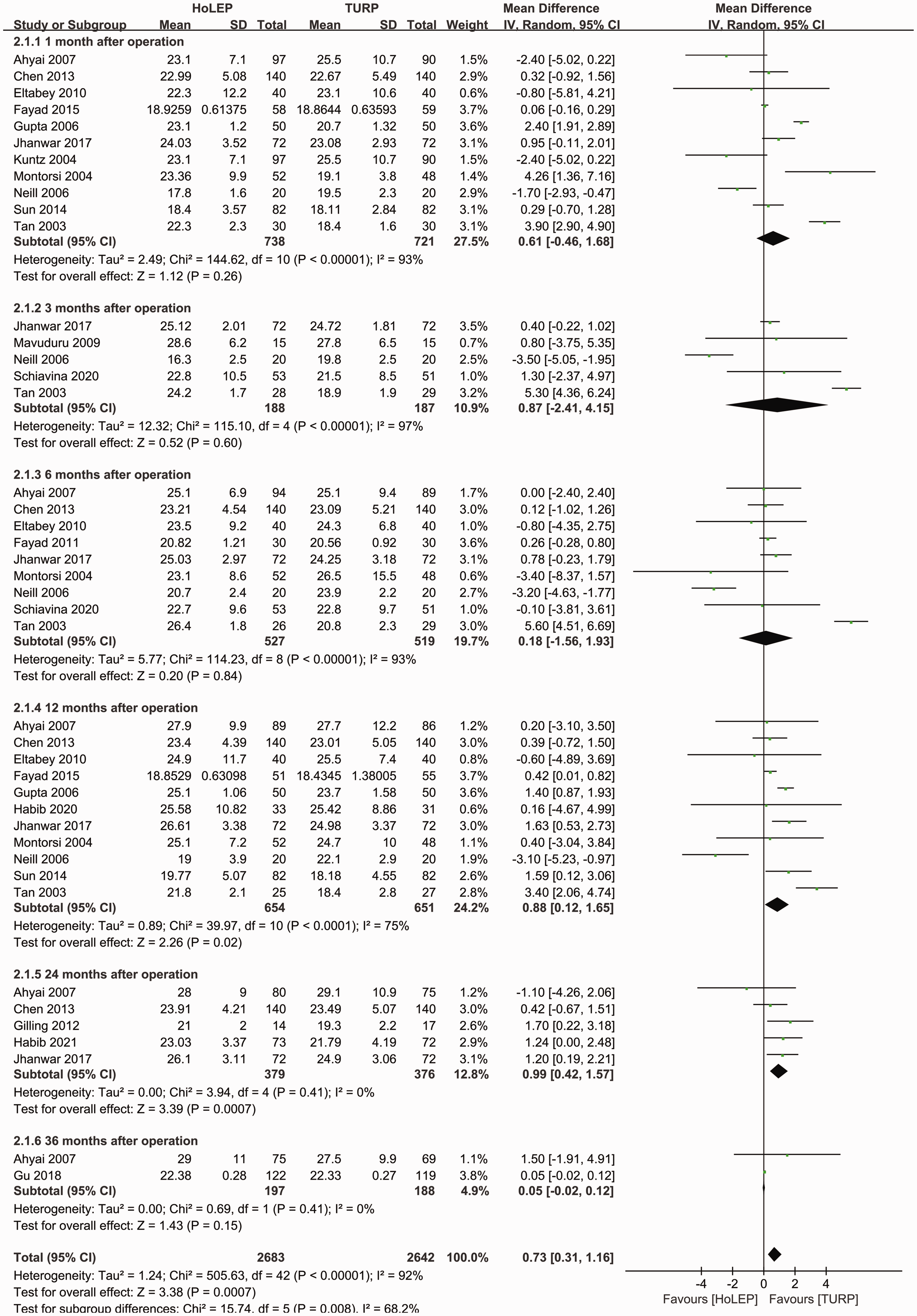
Forest plot of maximum urinary flow rate.
PVR
Statistically significant differences indicated a benefit of HoLEP over TURP in terms of PVR at 1 (WMD: −2.60; 95% CI: −4.76 to −0.44; p = 0.02; I2 = 0%), 6 (WMD: −4.49; 95% CI: −8.27 to −0.71; p = 0.02; I2 = 91%), and 12 (WMD: −8.55; 95% CI: −15.56 to −1.54; p = 0.02; I2 = 90%) months after surgery. No significant difference was found at 3 and 24 months after operation (Figure 4).

Forest plot of post-void residual volume.
IPSS
HoLEP showed a superior outcome in terms of IPSS at 12 months (WMD: −0.60; 95% CI: −1.03 to −0.17; p = 0.006; I2 = 86%) after surgery. On the contrary, there was no significant difference at 1, 3, 6, and 24 months postoperatively (Figure 5).
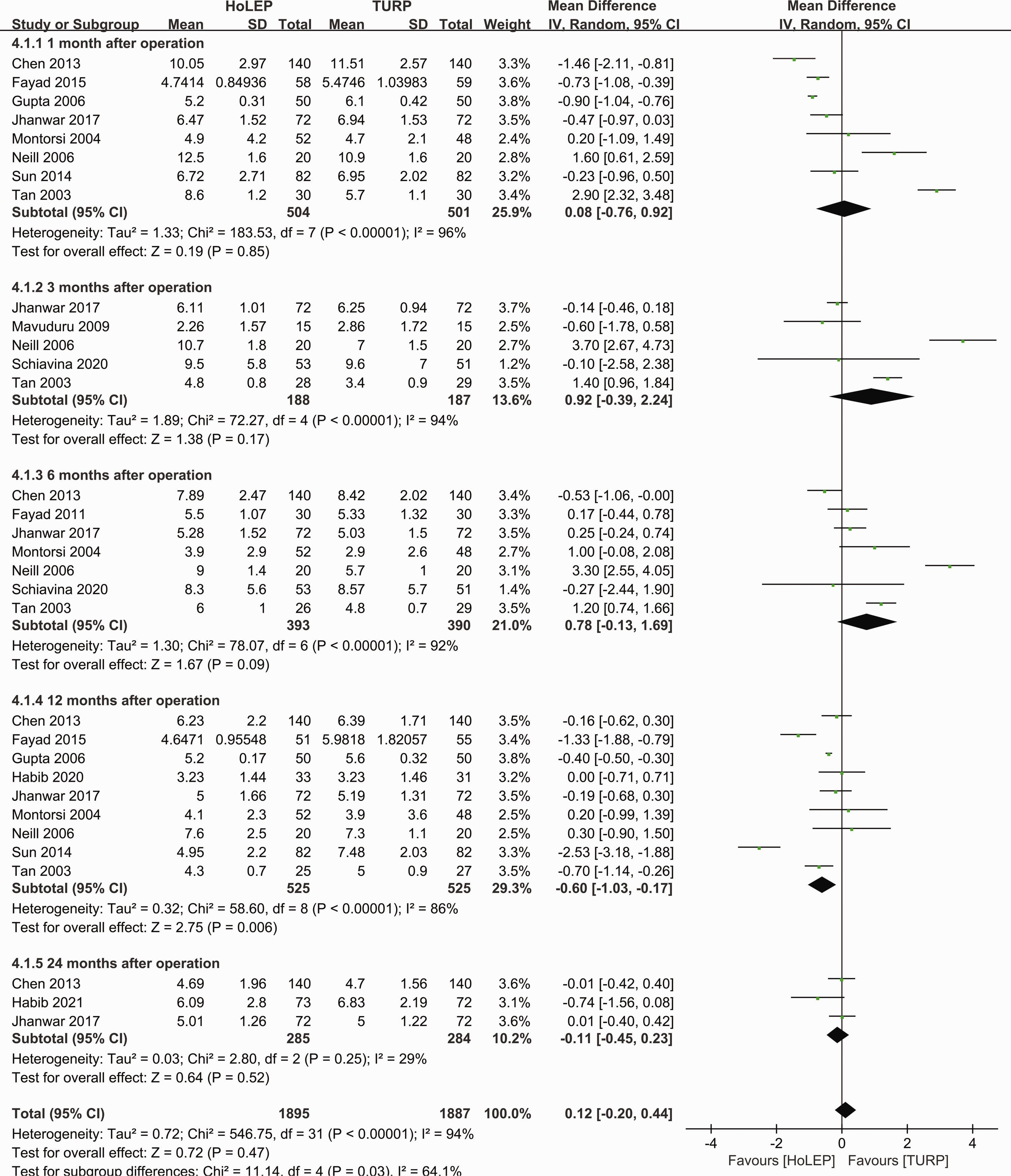
Forest plot of International Prostate Symptom Score.
Secondary outcomes
AUA symptom score, QoL score, and IIEF-5
The analysis results showed no significant difference between the groups in terms of AUA symptom score at 1, 6, 12, and 24 months after surgery; QoL score at 1, 3, 6, 12, and 24 months after operation; and IIEF-5 at 6, 12, and 24 months after surgery.
TRUS volume and PSA
No statistically significant differences were observed between the two groups in TRUS volume of the prostate at 6 months postoperatively and in the level of PSA at 24 months postoperatively.
PdetQmax and Schäfer grade
The results indicated that HoLEP was associated with superior outcomes in terms of PdetQmax (WMD: −13.72; 95% CI: −25.87 to −1.56; p = 0.03; I2 = 99%) and Schäfer grade (WMD: −0.88; 95% CI: −0.95 to −0.81; p < 0.00001; I2 = 96%) at 6 months after surgery.
Occurrence of adverse events
The results showed that compared with TURP, HoLEP was associated with a significantly lower risk of hyponatremia (relative risk [RR]: 0.26; 95% CI: 0.10 to 0.67; p = 0.006), blood transfusion (RR: 0.17; 95% CI: 0.07 to 0.42; p < 0.0001), and urethral stricture (RR: 0.48; 95% CI: 0.24 to 0.95; p = 0.03) but a higher risk of postoperative dysuria (RR: 2.63; 95% CI: 1.55 to 4.46; p = 0.0004). There was no significant difference in the incidence of recatheterization, urinary incontinence, urinary retention, urinary tract infection, reoperation, transurethral resection syndrome, and postoperative fever between the two groups.
Bias assessment
As seen in the risk of bias graph (Figure 6), three studies 7 , 17 , 23 had high bias risk for blinding of participants and personnel, one study 17 had high risk for blinding of outcome assessment, and two studies 7 , 13 had high bias risk for incomplete outcome data. Moreover, most included studies did not mention blinding of participants and personnel and blinding of outcome assessment during the trials. As for publication bias, a slight degree of asymmetry can be seen in the funnel plot, so we concluded that there was a possibility of publication bias. As an example, the funnel plot of Qmax is presented in Figure 7.
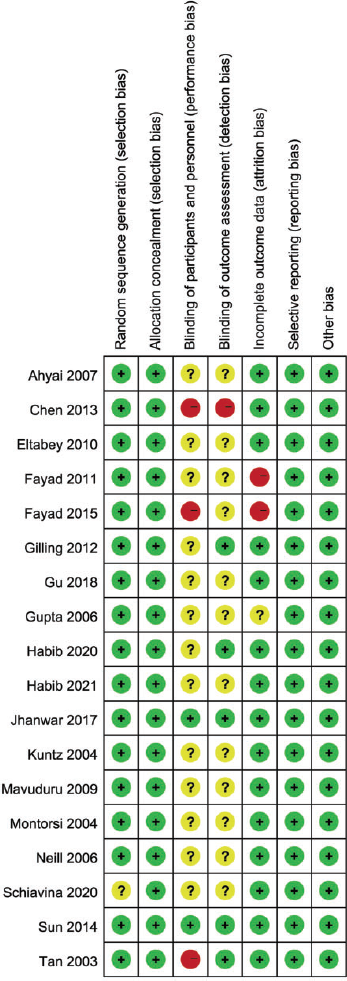
Risk of bias summary graph for randomized controlled trials.
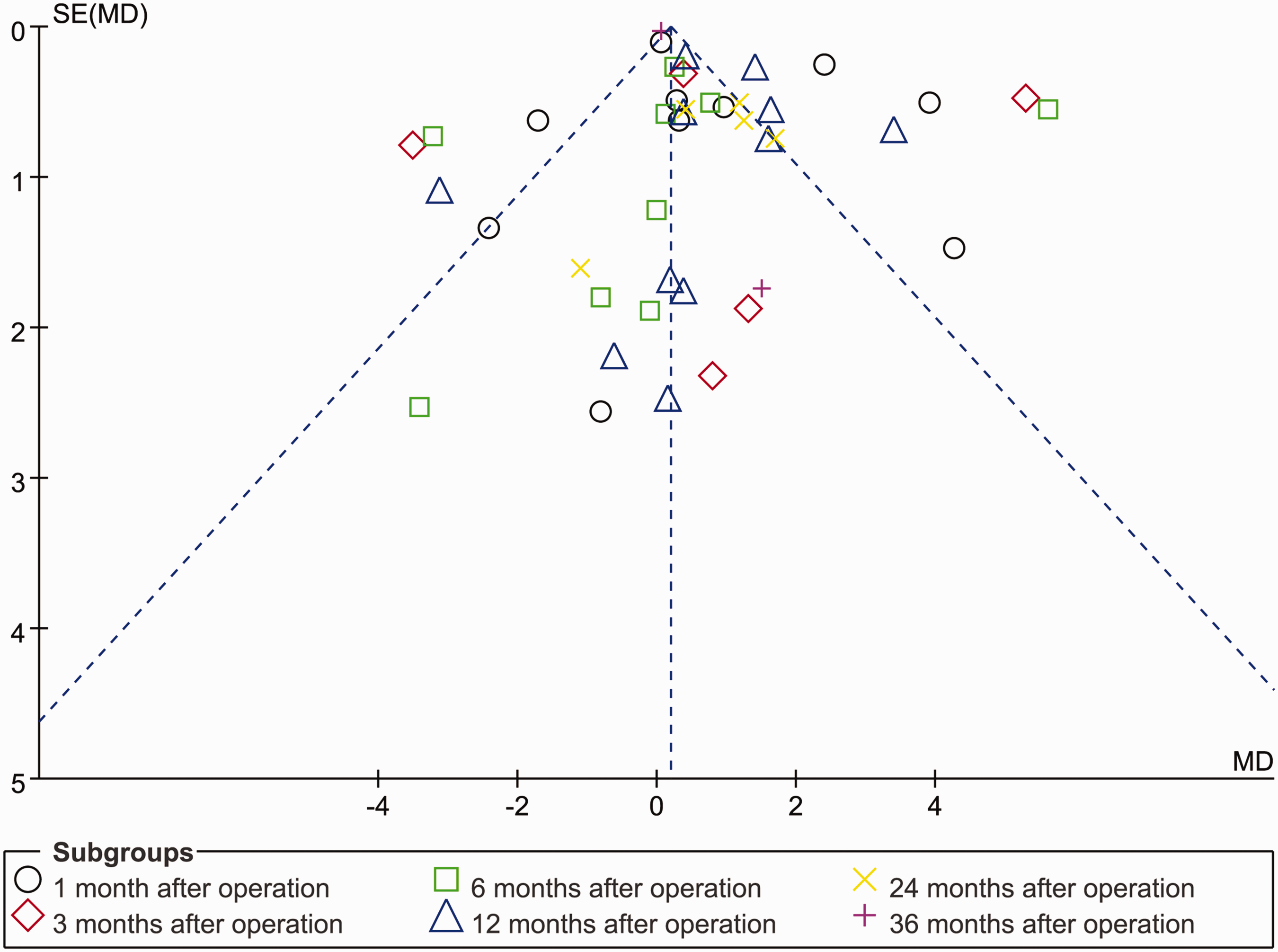
Funnel plot.
Discussion
BPH seriously affects the physical and mental health of patients owing to severe lower urinary tract symptoms, which cause great distress in patients' lives. Because of the limited effect of drug therapy, TURP has long been the main method used in the treatment of BPH. TURP can effectively relieve patients’ symptoms and is regarded as the gold standard for the treatment of BPH. 28 , 29 However, related adverse reactions, such as bleeding and transurethral resection syndrome, are of concern in its clinical application. Therefore, new treatment methods that are safer and more effective are urgently needed. 4 HoLEP is now accepted and recommended internationally as a minimally invasive alternative to TURP. 30 In this meta-analysis, we included RCTs comparing TURP and HoLEP with the aim to provide insight for clinical decision making.
According to our findings, HoLEP requires a longer operation time; the additional morcellation time associated with HoLEP may be an important reason for this. This may also be related to the long, steep learning curve and rich surgical experience required for HoLEP. 31 As for mean resected prostatic weight, there was no significant difference between HoLEP and TURP, which was confirmed by the results of TRUS volume for the two groups at 6 months after surgery. HoLEP was superior to TURP in terms of catheter duration, hospital stay, bladder irrigation time, and postoperative irrigation. Although there was no significant difference in intraoperative irrigation between the two groups, the operation time of HoLEP was longer than that of TURP, which also reflected in that the former required less irrigation per unit of time. The above result may be related to less trauma, less bleeding, and faster recovery with HoLEP. From the practical viewpoint of surgery, TURP repeatedly forms new wounds, leading to more bleeding whereas HoLEP only damages the prostate vessels once at the capsule level, resulting in less bleeding and a clearer surgical vision. 7 , 17 The results of this meta-analysis also showed that the incidence of blood transfusion required in the perioperative period was lower with HoLEP, which supports this viewpoint.
Importantly, this meta-analysis involved data relevant to postoperative sexual function change for the first time. The results suggest that the effects of the two surgical procedures on patients' sexual function are comparable. Although our results showed that AUA symptom score, QoL score, and IIEF-5 of the two groups were roughly equivalent at various time points after surgery, the change trends for postoperative Qmax, PVR, IPSS, PdetQmax, and Schäfer grade all suggested that HoLEP has better curative efficacy. This may be related to the fact that more prostate tissue can be resected in HoLEP. Although our study results showed no significant difference in mean resected prostatic weight between the two groups, this may be because HoLEP can cause partial tissue evaporation and disappearance during the operation, which cannot be effectively measured. 32 However, Qmax at 36 months postoperatively and PVR, IPSS, and PSA level at 24 months postoperatively showed no significant differences between the two groups. Such changes may be associated with re-hyperplasia in residual prostate tissue. A related study similarly observed an increase in TRUS volume of the prostate during follow-up. 27 Although the studies included in this meta-analysis only involved patients with BPH undergoing primary surgery, it is interesting that related studies have shown that salvage HoLEP is still a feasible and effective method for treating residual benign prostatic hyperplasia. 33
In all relevant studies, only one case of transurethral resection syndrome occurred in TURP, and no significant difference was found between the two groups; however, the incidence of hyponatremia in HoLEP was significantly lower. This result may be related to the less invasive nature of HoLEP and the availability of normal saline as a perfusion fluid in HoLEP. 34 We also observed postoperative dysuria more often in the HoLEP group. This might be owing to transient mild thermal injury of the external urinary sphincter. The incidence of urethral stricture after TURP was significantly higher than that of HoLEP. At present, there is no confirmed evidence regarding the cause of this. Avoiding any use of electrical current may decrease the risk of iatrogenic stricture formation. In addition to the above results, there was no significant difference between the two groups regarding the incidence of recatheterization, urinary incontinence (including stress urinary incontinence and urgent urinary incontinence), urinary retention, urinary tract infection, reoperation, and postoperative fever. Currently, only one RCT 21 involving the application of HoLEP in patients on anticoagulants has been conducted; we could not include this RCT in the present meta-analysis. Another two studies on the use of HoLEP found that it did not increase blood transfusion rates in patients taking anticoagulants compared with those who were not on anticoagulants. 35 , 36 Thus, HoLEP has an acceptable safety profile for such patients.
Although all studies involved in this meta-analysis were RCTs, the overall sample size was small. Additional study limitations include a short follow-up period (<12 months), a risk of random error in the cumulative meta-analysis of RCTs, and failure to use trial sequential analysis.
Conclusions
Compared with TURP, HoLEP for BPH was associated with longer operation time but shorter catheter duration, hospital stay, and bladder irrigation time. According to the results for Qmax, PVR, and IPSS, HoLEP showed better curative efficacy at 6, 12, and 24 months after operation. The incidence of adverse events such as perioperative hyponatremia, blood transfusion, and urethral stricture was also significantly decreased.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231190763 - Supplemental material for Comparison of holmium laser enucleation and transurethral resection of prostate in benign prostatic hyperplasia: a systematic review and meta-analysis
Supplemental material, sj-pdf-1-imr-10.1177_03000605231190763 for Comparison of holmium laser enucleation and transurethral resection of prostate in benign prostatic hyperplasia: a systematic review and meta-analysis by Feng Chen, Yijin Chen, Yongsheng Zou, Yunxiao Wang, Xiaogang Wu and Milian Chen in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605231190763 - Supplemental material for Comparison of holmium laser enucleation and transurethral resection of prostate in benign prostatic hyperplasia: a systematic review and meta-analysis
Supplemental material, sj-pdf-2-imr-10.1177_03000605231190763 for Comparison of holmium laser enucleation and transurethral resection of prostate in benign prostatic hyperplasia: a systematic review and meta-analysis by Feng Chen, Yijin Chen, Yongsheng Zou, Yunxiao Wang, Xiaogang Wu and Milian Chen in Journal of International Medical Research
Footnotes
Authors' contributions
Feng Chen and Yijin Chen contributed to the article screening and data collection. Yongsheng Zou and Yunxiao Wang contributed to the data synthesis. Xiaogang Wu and Milian Chen contributed to the study design and preparation of the primary manuscript. Milian Chen contributed to the editing of this article.
Data availability statement
All the relevant data, including analysis results, have been supplied within the manuscript. Any further required data are available upon request.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.