
Abstract
Web-based HIV and sexually transmitted infection (STI) prevention studies are increasingly requesting gay, bisexual, and other men who have sex with men (GBMSM) to return self-collected specimens for laboratory processing. Some studies have solicited self-collected extragenital swabs for gonorrhea and chlamydia testing, but to date, none have solicited self-collected hair samples for pre-exposure prophylaxis (PrEP) adherence testing. Project Caboodle! offered 100 racially/ethnically diverse GBMSM aged 18 to 34 years residing across the United States a choice to self-collect at home and return by mail any of the following: a finger-stick blood sample (for HIV testing), a pharyngeal swab, a rectal swab and a urine specimen (for gonorrhea and chlamydia testing), and a hair sample (to visually assess its adequacy for PrEP drug level testing). Despite not incentivizing specimen return, 51% mailed back at least one type of specimen within 6 weeks (1% returned three specimens, 11% returned four specimens and 39% returned all five specimens). The majority of returned specimens were adequate for laboratory processing. Significantly more participants without a college education (p = .0003) and those who were working full-time or part-time (p = .0070) did not return any specimens. In addition, lower levels of HIV-related knowledge (p = .0390), STI-related knowledge (p = .0162), concern about contracting HIV (p = .0484), and concern about contracting STIs (p = .0108) were observed among participants who did not return any specimens. Self-collection of specimens holds promise as a remote monitoring strategy that could supplement testing in clinical settings, but a better understanding of why some GBMSM may choose to fully, partially, or not engage in this approach is warranted.
Keywords
Introduction
Gay, bisexual and other men who have sex with men (GBMSM) represent a small proportion of the U.S. population (Grey et al., 2016; Purcell et al., 2012), but are heavily affected by HIV and bacterial sexually transmitted infections (STIs). In 2019, GBMSM accounted for 63% of the 1.2 million people living with HIV and 69% of new HIV diagnoses (Centers for Disease Control and Prevention [CDC], 2021). In 2018, the median national prevalence of pharyngeal, rectal, and urethral gonorrhea among GBMSM was estimated to be 12.9%, 14.8%, and 7.9%, respectively, and that of pharyngeal, rectal, and urethral chlamydia was estimated to be 2.7%, 16.1%, and 5.8% respectively (CDC, 2019b). Left untreated, STIs may lead to acute and chronic complications, such as epididymitis, orchitis, seminal vesiculitis, prostatitis, and proctitis (Benson et al., 2009; Read & Donovan, 2012; Workowski, 2013), and can increase the risk of HIV acquisition and its onward transmission in case of inadequate viral suppression (Bernstein et al., 2010; Buchacz et al., 2004; Galvin & Cohen, 2004; Menza et al., 2009; Ward & Rönn, 2010). Recent modeling suggests that approximately 10% of incident HIV infections are attributable to gonococcal or chlamydial infections (Jones et al., 2019).
In an effort to improve suboptimal HIV and bacterial STI screening levels among GBMSM at elevated risk (CDC, 2019a; Hoots et al., 2018), experts are increasingly advocating for the evaluation of alternative strategies to supplement testing in clinical settings such as the self-collection of specimens at home for rapid testing or their return by mail for laboratory processing (Hawk et al., 2020; Steehler & Siegler, 2019; Tenover et al., 2017). Clinic-based studies have demonstrated that self-collected specimens for HIV, gonorrhea, and chlamydia screening are equally sensitive and specific as specimens collected by health-care professionals (Dize et al., 2013, 2016; Lunny et al., 2015; van Loo et al., 2017). Prior research conducted with GBMSM in nonclinical settings involving cross-sectional surveys, in-depth interviews, and focus group discussions has found generally favorable attitudes toward specimen self-collection from different anatomical sites on account of an increased sense of privacy, convenience, and autonomy (Cushman et al., 2019; A. E. Freeman et al., 2018; Pearson et al., 2018; Sharma et al., 2014; Tobin et al., 2018). Social-distancing and stay-at-home orders during the COVID-19 pandemic have highlighted the previously known benefits of home-based HIV and bacterial STI testing options and accelerated their demand (Kersh et al., 2021). Positive reactions expressed toward this approach by GBMSM have prompted several recent Web-based studies to request the return of self-collected specimens for HIV or bacterial STI testing (Biello et al., 2021; Grov et al., 2016; Merchant et al., 2018; Mustanski et al., 2018; Salow et al., 2017; P. S. Sullivan, Stephenson, et al., 2021; S. P. Sullivan, Sullivan, & Stephenson, 2021).
One specimen that has recently sparked interest in the HIV prevention research community is hair, a nonbiohazardous, easy-to-ship specimen that remains stable at ambient temperature. Pre-exposure prophylaxis (PrEP) significantly reduces the risk of acquiring HIV from sex but relies on adequate adherence to be effective (Anderson et al., 2012; Blumenthal & Haubrich, 2013; Grant et al., 2010, 2014; Haberer, 2016). Hair samples are novel with respect to PrEP drug-level testing and can be utilized to objectively measure adherence both in daily and in event-driven users of PrEP (Baxi et al., 2015; Gandhi et al., 2015, 2017; Koss et al., 2017, 2018; Seifert et al., 2018; Spinelli et al., 2020). For example, PrEP drug concentrations in the 1.5 cm of hair closest to the scalp (i.e., at the proximal end) represent drug exposure over the preceding 6 weeks, with segmental analysis of hair samples allowing for an assessment of PrEP adherence over different time intervals (Cohen et al., 2019; Thaden et al., 2018). Self-collecting hair and returning it by mail might be a viable method to conduct remote PrEP adherence testing, especially among GBMSM who do not wish to provide a self-collected dried blood spot (DBS) specimen and could allow for the identification of GBMSM facing adherence difficulties for subsequent intervention. Some studies have reported on the practicality of using self-collected hair samples to conduct cortisol testing in diverse populations (Enge et al., 2020; Ouellet-Morin et al., 2016; Ramirez et al., 2017); however, little is known about this aspect with respect to PrEP drug-level testing.
Given the ongoing need to promote regular HIV and STI screening among GBMSM, it is important to advance research on the utility of strategies that have the potential to overcome known barriers to testing (Barbee et al., 2015; Carter et al., 2014; Heijman et al., 2017; Horridge et al., 2019; Lutz, 2015). It is also paramount to assess new methods to remotely measure PrEP adherence to help identify GBMSM in need of added assistance such as enhanced counseling or digital medication reminders (Abaasa et al., 2018; Haberer, 2016; Hannaford et al., 2021). Combining the self-collection of specimens for HIV and bacterial STI testing along with a hair sample for PrEP drug-level testing might hold promise as a remote monitoring strategy. Although the aforementioned Web-based studies conducted with GBMSM that implemented specimen self-collection have contributed to the extant knowledge base on the acceptability and feasibility of this approach (Biello et al., 2021; Grov et al., 2016; Merchant et al., 2018; Mustanski et al., 2018; Salow et al., 2017; P. S. Sullivan, Stephenson, et al., 2021; S. P. Sullivan, Sullivan, & Stephenson, 2021), none asked participants to return a hair sample.
To advance research on remote testing and adherence monitoring strategies, we conducted an exploratory study in which we offered sexually active GBMSM a choice to self-collect at home and return by mail any of the following: a finger-stick blood sample (for HIV testing), a pharyngeal swab, a rectal swab and a urine specimen (for gonorrhea and chlamydia testing), and a hair sample (to visually assess its adequacy for PrEP drug-level testing). Actual PrEP drug-level testing was not a study objective; therefore, being on PrEP was not an eligibility criterion. Specimen return was voluntary, and no monetary incentive was provided for completing this step. In this article, we present results on the proportion of each type of self-collected specimen returned by participants, their adequacy for laboratory processing and differences in characteristics between those who returned at least one specimen and those who did not return any specimens. Understanding these issues is essential for developing comprehensive public health interventions to improve screening rates for HIV and STIs and to objectively measure and support adherence to PrEP among GBMSM.
Method
Project Caboodle! sought to explore patterns of self-collecting and returning up to five specimens for HIV, bacterial STI, and potential PrEP drug-level testing among 100 HIV-negative or unknown status GBMSM aged 18 to 34 years recruited online from across the United States. Study procedures were completed between March 2019 and April 2020 and have been described in detail elsewhere (Sharma et al., 2019). Approval was obtained from the Institutional Review Board at the University of Michigan (Approval number: HUM00153673). Electronic informed consent was obtained from all individual participants included in the study.
Recruitment and Eligibility
Recruitment was conducted through advertising on Facebook and Grindr. Individuals who clicked on the advertisements were directed to the study’s landing page that included a brief overview of the protocol and a link to the informed consent document, and those who consented were asked to complete an eligibility screener. Our eligibility criteria included being assigned male sex at birth, reporting a male gender identity, being 18–34 years of age, residing in the United States or dependent areas, not known to be living with HIV, having ≥2 male sex partners in the past 3 months, and willing to receive a specimen self-collection box at a preferred mailing address. Individuals who met the eligibility criteria were asked to provide their full name, email address, mobile phone number, and mailing address. Those who did not provide consent, did not meet the eligibility criteria, or did not provide verifiable contact information were directed to the Centers for Disease Control and Prevention (CDC) website on HIV and STIs.
Web-Based Survey
GBMSM who provided verifiable contact information were emailed a link to a survey programmed in Qualtrics that collected demographic and behavioral data, including engagement in condomless anal or oral sex in the past 3 months and HIV and bacterial STI testing history. The survey asked questions on current and previous PrEP use, including reasons for discontinuing or never using PrEP. The 18-item Brief HIV Knowledge Questionnaire (Carey & Schroder, 2002) and the 27-item Sexually Transmitted Disease Knowledge Questionnaire (Jaworski & Carey, 2007) were used to assess HIV and STI-related knowledge, respectively. These scales measure an individual’s knowledge around HIV and STI transmission, prevention, and treatment and have been extensively used in studies conducted with GBMSM (Balán et al., 2019; Garofalo et al., 2015; Mimiaga et al., 2009; Newcomb & Mustanski, 2014; Wiersema et al., 2019). Levels of concern about contracting HIV and STIs were solicited by presenting separate scales ranging from 0 (not concerned at all) to 10 (very concerned) for each domain (Kahle et al., 2020). Up to three reminders to complete the survey were sent at weekly intervals, and an incentive of U.S.$40 was provided in the form of an Amazon e-gift card.
Specimen Self-Collection Box
Participants who completed the survey were shipped a box containing instructions and materials to self-collect and return five different specimens for HIV, bacterial STI, and potential PrEP drug-level testing (Figure 1). Each component was labeled with a unique participant ID to enable specimen identification upon return. The boxes were shipped from the University of Michigan School of Nursing (UMSN) in Ann Arbor in plain unmarked packaging. Step-by-step written instructions accompanied by color images were provided to assist participants in self-collecting and packaging their specimens. The boxes also included envelopes affixed with prepaid FedEx shipping labels to return a finger-stick blood sample, a pharyngeal swab, a rectal swab and a urine specimen to the Clinical Virology Research Laboratory (CVRL) at Emory University in Atlanta, and a hair sample to the Hair Analytical Laboratory (HAL) at the University of California San Francisco. Participants were given 6 weeks from receiving the box to return self-collected specimens of their choice for laboratory processing. Specimen return was voluntary, and no monetary incentive was provided for completing this step.

Specimen Self-Collection Box Used in Project Caboodle!, United States, March 2019 to April 2020.
Laboratory Processing of Specimens
Finger-stick blood samples received by the CVRL were screened for HIV with the OraQuick Advance Rapid HIV-1/2 Antibody Test (Reynolds & Muwonga, 2004), and pharyngeal swabs, rectal swabs, and urine specimens were screened for gonorrhea and chlamydia using the Abbott RealTime PCR assay (Gaydos et al., 2010). Hair samples received by the HAL were visually inspected to determine whether the quantity of hair was sufficient to potentially conduct PrEP drug-level testing (i.e., ≥20 fibers), whether the hair was affixed to the aluminum foil with an adhesive label at the distal end, and whether the hair was properly enclosed in the aluminum foil to protect it from light. No participant identifiable information was shared with personnel at either the CVRL or the HAL, and the specimens were connected to results solely based on unique participant IDs. Results were returned to study staff at UMSN through password-protected files.
Return of Test Results
HIV, gonorrhea, and chlamydia test results were delivered back to participants by a counselor with experience in the provision of HIV Counseling, Testing, and Referral over the phone or via an email containing a link to a secure Box folder created specifically for each participant. The email was only used to deliver negative test results back to those who requested this option so they could have a copy for their records. Participants who received positive test results were counseled about the importance of accessing treatment, notifying their partners, and adopting sexual risk reduction measures. Based on their ZIP code, they were emailed a list of local health care providers within 24 hr of results delivery. Participants were contacted 2 weeks after the delivery of positive test results to confirm whether they had sought treatment. Participants who received negative test results were counseled about the importance of regularly screening for HIV and STIs, engaging in safer sexual behaviors, and continuing or considering the use of prevention strategies.
Data Analysis
Statistical analyses were conducted using SAS. Descriptive statistics were used to summarize the demographic and behavioral characteristics of the sample. Participants’ HIV testing, bacterial STI testing, and PrEP use histories were tabulated. Each participant’s responses to items on the Brief HIV Knowledge Questionnaire (Cronbach’s α = .77) and the Sexually Transmitted Disease Knowledge Questionnaire (Cronbach’s α = .91) were summed to calculate overall scores ranging from 0 to 18 and 0 to 27, respectively, with higher scores indicating greater knowledge. Levels of concern about contracting HIV and STIs ranging from 0 (not concerned at all) to 10 (very concerned) were summarized.
The CVRL specimen quality and screening report were used to document the number of finger-stick blood samples, pharyngeal swabs, rectal swabs, and urine specimens returned by participants, the proportion that were adequate for HIV, gonorrhea and chlamydia testing, and the test results. Data on the delivery of test results back to participants and linkage to medical care for anyone receiving a positive test result were aggregated from case report forms. The HAL hair inspection report was used to document the number of hair samples returned by participants, the proportion that included a sufficient quantity of hair to potentially conduct PrEP drug-level testing and which part of hair was affixed to the aluminum foil with an adhesive label.
Chi-square tests were conducted to compare the characteristics of participants who returned at least one specimen with those who did not return any specimens. Wilcoxon rank sum tests were used to identify variations in HIV and STI-related knowledge between participants in each group (as these data were skewed). Independent samples t tests were conducted to identify variations in levels of concern about contracting HIV and STIs between participants in each group (as these data were normally distributed). Chi-square tests were used to assess if there were any differences in returning a finger-stick blood sample across strata of HIV testing in the past year, returning a pharyngeal swab, a rectal swab, or a urine specimen across strata of bacterial STI testing in the past year, and returning a hair sample across strata of current PrEP use.
Results
Sample Characteristics
Of the 575 individuals who completed the eligibility screener, 191 (33%) met the eligibility criteria, 156 (82%) of whom provided verifiable contact information. Of these, 100 (64%) completed the survey and were shipped a specimen self-collection box (Figure 2).

Recruitment of 100 Gay, Bisexual, and Other Men Who Have Sex With Men in Project Caboodle!, United States, March 2019 to April 2020.
The mean and median ages were 26 years, and the sample was diverse with respect to race and ethnicity with 29 (29%) identifying as Hispanic, 17 (17%) identifying as non-Hispanic Black, and 12 (12%) identifying as Asian (Table 1). The majority had a college degree or higher educational level (n = 59, 59%), worked full-time or part-time (n = 76, 76%), had health insurance coverage (n = 83, 83%), identified as gay (n = 86, 86%), and were single (n = 68, 68%). More than half (n = 54, 54%) had condomless anal sex and more than two-thirds (n = 69, 69%) had condomless oral sex with ≥2 men in the past 3 months.
Demographic and Behavioral Characteristics of 100 Gay, Bisexual, and Other Men Who Have Sex With Men Participating in Project Caboodle!, United States, March 2019 to April 2020.
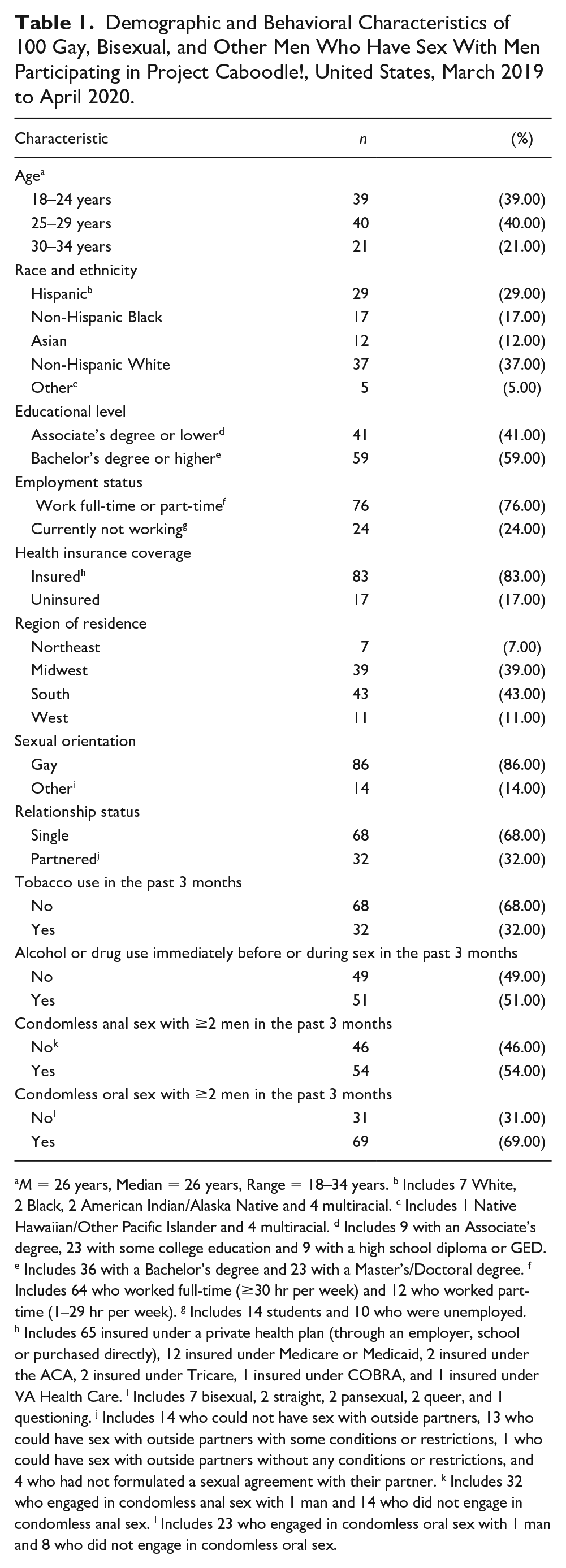
M = 26 years, Median = 26 years, Range = 18–34 years. b Includes 7 White, 2 Black, 2 American Indian/Alaska Native and 4 multiracial. c Includes 1 Native Hawaiian/Other Pacific Islander and 4 multiracial. d Includes 9 with an Associate’s degree, 23 with some college education and 9 with a high school diploma or GED. e Includes 36 with a Bachelor’s degree and 23 with a Master’s/Doctoral degree. f Includes 64 who worked full-time (≥30 hr per week) and 12 who worked part-time (1–29 hr per week). g Includes 14 students and 10 who were unemployed. h Includes 65 insured under a private health plan (through an employer, school or purchased directly), 12 insured under Medicare or Medicaid, 2 insured under the ACA, 2 insured under Tricare, 1 insured under COBRA, and 1 insured under VA Health Care. i Includes 7 bisexual, 2 straight, 2 pansexual, 2 queer, and 1 questioning. j Includes 14 who could not have sex with outside partners, 13 who could have sex with outside partners with some conditions or restrictions, 1 who could have sex with outside partners without any conditions or restrictions, and 4 who had not formulated a sexual agreement with their partner. k Includes 32 who engaged in condomless anal sex with 1 man and 14 who did not engage in condomless anal sex. l Includes 23 who engaged in condomless oral sex with 1 man and 8 who did not engage in condomless oral sex.
Three-fourths of all participants (n = 75, 75%) reported testing for HIV at least once a year (Table 2). Of the 95 who had tested for HIV at least once, the majority (n = 64, 67%) most recently tested at a private doctor’s office, public health clinic or community health center, and several (n = 55, 58%) had never used a commercially available home HIV test. More than half of all participants (n = 58, 58%) reported testing for bacterial STIs at least once a year. Of the 86 who had tested for bacterial STIs at least once, the majority (n = 68, 79%) most recently tested at a private doctor’s office, public health clinic or community health center, and almost two-thirds (n = 55, 64%) did not provide specimens for extragenital screening at their most recent test. Regarding PrEP, 32 (32%) of all participants were currently using PrEP and 10 (10%) had discontinued use as they started a committed relationship or did not like its side effects. The remaining 58 (58%) had never used PrEP primarily because they could not afford it, did not know where to access it, or were concerned about its side effects.
HIV Testing, Bacterial STI Testing and PrEP Use Histories Among 100 Gay, Bisexual and Other Men Who Have Sex With Men Participating in Project Caboodle!, United States, March 2019 to April 2020.

Note. PrEP = pre-exposure prophylaxis; STI = sexually transmitted infection.
Includes 13 who did not test regularly and 7 who tested every time they thought they might have been exposed. b Includes 4 who tested at a mobile testing unit, 2 who tested in an emergency room, 1 who tested as an inpatient, 1 who tested at a blood bank, 1 who tested in the military, and 1 who tested as part of another research study. c Includes 33 who had used the OraQuick In-Home HIV test, 1 who had used the Home Access HIV-1 Test System, and 6 who had used both types of home HIV tests. d Includes 14 who did not test regularly and 14 who tested every time they thought they might have been exposed. e Includes 2 who tested at a mobile testing unit, 3 who tested in an emergency room, 1 who tested in the military, and 1 who tested as part of another research study. f Participants provided a pharyngeal swab and a rectal swab in addition to a urine specimen or urethral swab for gonorrhea and chlamydia testing. g Participants could have indicated more than one reason for discontinuing PrEP. h Participants could have indicated more than one reason for never using PrEP.
Overall scores on the Brief HIV Knowledge Questionnaire ranged from 4 to 17, with a mean of 14 and a median of 15. Overall scores on the Sexually Transmitted Disease Knowledge Questionnaire ranged from 0 to 27, with a mean of 18 and a median of 19. The distributions for both these variables were skewed to the left, indicating generally high levels of HIV and STI-related knowledge. Levels of concern about contracting HIV ranged from 0 to 10, with a mean and median of 5. Levels of concern about contracting STIs ranged from 0 to 10, with a mean and median of 5. The distributions for both these variables were approximately symmetrical.
Specimen Return and Test Results
Overall, 51 (51%) of all participants returned at least one of five specimens (1 [2%] of whom returned three specimens, 11 [22%] of whom returned four specimens and 39 [76%] of whom returned all five specimens), and 49 (49%) did not return any specimens within 6 weeks of receiving the specimen self-collection box. The CVRL received 47 finger-stick blood samples, 51 pharyngeal swabs, 48 rectal swabs and 50 urine specimens, and the HAL received 46 hair samples. The mean time between receiving the specimen self-collection box at one’s preferred mailing address and returning self-collected specimens of one’s choice for laboratory processing was 14 days.
Of the 47 finger-stick blood samples, 42 (89%) were adequate for HIV testing and none (n = 0, 0%) tested positive. Five (11%) finger-stick blood samples could not be tested as the transport tube contained clotted blood. Of the 51 pharyngeal swabs, all (n = 51, 100%) were adequate for gonorrhea and chlamydia testing, and none (n = 0, 0%) tested positive. Of the 48 rectal swabs, all (n = 48, 100%) were adequate for gonorrhea and chlamydia testing. One (2%) tested positive for gonorrhea and 2 (4%) tested positive for chlamydia. Of the 50 urine specimens, all (n = 50, 100%) were adequate for gonorrhea and chlamydia testing. None (n = 0, 0%) tested positive for gonorrhea, but 1 (2%) tested positive for chlamydia. All (n = 196, 100%) returned specimens were packaged in the provided biohazard bag. Test results were delivered back to participants by a counselor over the phone (n = 33, 65%) or via an email containing a link to a secure Box folder created specifically for each participant (n = 18, 35%). All (n = 4, 8%) participants who received a positive test result for gonorrhea or chlamydia reported successfully obtaining treatment when they were contacted by study staff after 2 weeks of results delivery.
Of the 46 hair samples, 36 (78%) included a sufficient quantity of hair to potentially conduct PrEP drug-level testing (i.e., ≥20 fibers). Of these, 13 (36%) specimens were affixed to the aluminum foil with an adhesive label at the distal end, but 5 (14%) were affixed somewhere in the middle which made it difficult for laboratory personnel to distinguish between the proximal and distal ends. Of the 18 specimens that were not affixed to the aluminum foil, 3 (17%) were justified as the hair fibers were very short (≤1 cm) and our instructions directed participants with short haircuts to skip this step. Finally, 43 (93%) of the 46 returned hair samples were properly enclosed in the aluminum foil, and all were packaged in the provided clear plastic bag.
Variations in Specimen Return
Significantly more participants without a college education and those who were working full-time or part-time did not return any specimens (Table 3). In addition, lower levels of HIV and STI-related knowledge and lower levels of concern about contracting HIV and STIs were observed among participants who did not return any specimens. No variations in specimen return were observed across strata of age, race and ethnicity, health insurance coverage, sexual orientation, relationship status, or engagement in condomless anal or oral sex with ≥2 men in the past 3 months. Also, no differences in returning a finger-stick blood sample across strata of HIV testing in the past year, returning a pharyngeal swab, a rectal swab, or a urine specimen across strata of bacterial STI testing in the past year and returning a hair sample across strata of current PrEP use were observed.
Differences in Selected Characteristics Between Those Who Returned at Least One Specimen and Those Who Did Not Return Any Specimens Among 100 Gay, Bisexual and Other Men Who Have Sex With Men Participating in Project Caboodle!, United States, March 2019 to April 2020.

Chi-square test. b Wilcoxon rank sum test. c Independent samples t-test.
Discussion
Project Caboodle! is the only study to our knowledge to explore patterns of self-collecting and returning up to five specimens for HIV, bacterial STI, and potential PrEP drug-level testing in a racially/ethnically diverse sample of GBMSM recruited online from across the United States. At the time of enrollment, our participants reported substantial engagement in sexual risk behaviors (54% had condomless anal sex and 69% had condomless oral sex with ≥2 men in the past 3 months) but inadequate levels of annual screening for HIV (88% in the past year) or bacterial STIs (69% in the past year). Approximately a third (32%) reported using PrEP, which is comparable to current U.S. national estimates (Finlayson et al., 2019; Mansergh et al., 2020). Despite not incentivizing specimen return, slightly over half (51%) chose to mail back at least one type of specimen, and the majority of returned specimens were adequate for laboratory processing. Notably, the average proportion of specimens returned for bacterial STI testing in our study (50%) was higher than in six other studies recently conducted with GBMSM (30%) (Norelli et al., 2021). Our results delineate how some intrapersonal characteristics (e.g., educational level, and HIV and STI-related knowledge) might influence the voluntary return of specimens by GBMSM participating in research and underscore the need to provide additional support for successfully implementing this approach in future Web-based studies.
Focusing first on self-collected finger-stick blood samples, almost half (47%) of our participants returned their specimens, suggesting that this option could offer utility as a complementary HIV screening tool to rapid oral fluid HIV self-testing. In previous research, some GBMSM were reluctant to prick themselves as they feared the sight of blood or were worried about pain, leading them to skip returning their specimens (Biello et al., 2021; Hirshfield et al., 2018; Merchant et al., 2018). Participants in our study who chose not to return finger-stick blood samples may have experienced similar challenges. The majority of specimens received were of adequate quality, but 5 (11%) could not be tested as the blood inside the transport tube had clotted, likely because it had not been properly mixed with the anticoagulant as instructed. Providing assistance for the self-collection of finger-stick blood samples beyond written instructions in the form of prerecorded video instructions or real-time video conferencing may bolster the return and adequacy of this specimen in subsequent studies. Further gains might also be achieved by offering tests to supplement HIV screening (e.g., syphilis screening, hepatitis B screening) as the finger-stick appears to become more agreeable to GBMSM if it can furnish them with information on multiple STIs (Balán et al., 2017).
Offering extragenital screening for bacterial STIs as part of our study resulted in the identification of one case of rectal gonorrhea and two cases of rectal chlamydia. Although less than a third (31%) of our participants reported providing specimens for extragenital screening at their most recent test, it is encouraging that 51% returned pharyngeal swabs and 48% returned rectal swabs, all of which were adequate for gonorrhea and chlamydia testing. In light of the suboptimal rates of extragenital screening among GBMSM (Hoots et al., 2018), specimen self-collection presents an opportunity to address gaps in the identification of pharyngeal and rectal infections. Prior research participants have mentioned that their inability to clearly see the back of their throat has acted as an impediment to self-collecting a pharyngeal swab, and their uneasiness about fecal residue being present in their rectum has precluded them from self-collecting a rectal swab (S. P. Sullivan, Stephenson, et al., 2021). These issues, among others such as the potential for minor physical discomfort associated with swabbing one’s throat or rectum, could have been problematic for a subset of participants in our study. Nonetheless, our findings demonstrate that it is possible for investigators to obtain high-quality extragenital specimens from GBMSM without supervision in nonclinical settings. Half (50%) our participants also mailed back urine specimens, which resulted in the identification of one case of urethral chlamydia. Given that this is one of the easier specimens to self-collect, with the process being almost identical to what is performed in clinical settings (S. P. Sullivan, Sullivan, & Stephenson, 2021), it is unclear why more participants did not return urine specimens. Additional research to determine which attributes of each of the three self-collection methods are associated with increased specimen return could help inform the development of future interventions to improve bacterial STI screening among GBMSM.
Regarding self-collected hair samples, almost half (46%) our participants returned their specimens, suggesting that this option could offer utility as a complementary PrEP drug-level testing tool to other objective methods like the measurement of drug levels in plasma or DBS specimens (Abaasa et al., 2018; Haberer, 2016; Hannaford et al., 2021). Hair self-collection is a painless procedure that does not require sterile equipment, and hair samples do not need specialized storage or transport conditions. Despite these advantages, it is crucial to bear in mind that not all GBMSM would be able or willing to provide this specimen. Recent demonstration projects in which study staff sought to collect a hair sample for PrEP drug level testing have encountered obstacles such as participants not having enough hair or expressing apprehension about disruption of their hairstyle (Gandhi et al., 2017; Koss et al., 2018). Although most participants in our study who chose to return hair samples provided a sufficient quantity to potentially conduct PrEP drug-level testing, many skipped affixing their specimen to the aluminum foil with an adhesive label at the distal end. Supplemental support for the self-collection of hair samples such as access to prerecorded video instructions or real-time video conferencing may be helpful to improve this specimen’s return and adequacy for laboratory processing.
Turning to focus on differences in characteristics between participants who returned at least one specimen and those who did not return any specimens, greater proportions of those without a college education and those who were working full-time or part-time did not mail back any specimens. Lower educational levels have been associated with reduced engagement in HIV and STI prevention among GBMSM (Matacotta et al., 2020; Noble et al., 2017; Sharma et al., 2021), and it is possible that participants without a college education faced challenges in successfully navigating some instructions. Our finding parallels another U.S. study in which GBMSM who had not completed college failed to achieve a recruitment milestone that involved rapid oral fluid HIV self-testing at home and the return of self-collected rectal swabs and urine specimens to a laboratory for gonorrhea and chlamydia testing (Grov et al., 2016). Judgments about how long it would take to self-collect, package, and drop off their specimens at a FedEx location might have served as an impediment to undertaking these activities among our participants who were working, especially in the absence of a monetary incentive. These results illuminate the need to investigate both logistical and perceived barriers to specimen self-collection and return faced by GBMSM to offer more tailored support in future Web-based studies.
Participants who did not return any specimens had lower levels of HIV and STI-related knowledge compared with those who returned at least one specimen. Previous studies among GBMSM have documented that higher levels of knowledge around transmission, prevention, and treatment are positively associated with regular testing and negatively associated with sexual risk-taking (Adam et al., 2014; Sharma et al., 2017; Wagenaar et al., 2012). Our sample had generally high levels of HIV and STI-related knowledge but further gains in specimen return might have been achieved by including educational resources such as factsheets and brochures in the specimen self-collection box and by encouraging access to publicly available information on the CDC website. Our finding that participants who did not return any specimens also had lower levels of concern about contracting HIV and STIs compared with those who returned at least one specimen is not surprising. Higher risk perceptions of contracting HIV and STIs have been associated with increased adoption of preventive behaviors among GBMSM (Goedel et al., 2016; Golub et al., 2019; Kahle et al., 2020; Lacefield et al., 2015; McGarrity et al., 2018). To better engage participants with lower risk perceptions in specimen self-collection and return, investigators might consider highlighting the opportunity to learn about their current HIV and STI status without having to visit a health care provider and emphasizing that their data are valuable to advance public health research.
Limitations of our study include the use of a convenience sample of GBMSM that was recruited via Facebook and Grindr, subjecting our results to sampling bias. GBMSM in communities that are already disproportionately impacted by HIV and STIs may not have access to technology such as a computer, tablet, or smartphone, although almost two-thirds (63%) of our participants identified as a racial or ethnic minority. Our Web-based survey and specimen self-collection instructions were only provided in English, and the lack of Spanish versions could have posed language difficulties for some participants. Due to budget constraints, our written instructions were not supplemented with prerecorded video instructions or real-time video conferencing. We acknowledge that we were not able to validate the veracity of returned specimens (i.e., whether they belonged to a participant or someone else). However, we do not think this was an issue as participants could choose to not return some or any specimens if they preferred. Finally, we did not conduct syphilis screening on finger-stick blood samples, but analogous to actual PrEP drug-level testing, this was not an original study objective.
Conclusion
Our exploratory study lends support to the growing acceptability and feasibility of requesting self-collected specimens for HIV and bacterial STI screening from those at elevated risk (A. H. Freeman et al., 2011; Ogale et al., 2019; Paudyal et al., 2015; Rosenberger et al., 2011; Witzel et al., 2020) and provides new information on the potential for utilizing self-collected hair samples to conduct PrEP drug-level testing. In addition, we have identified subgroups of GBMSM that did not return any specimens that might benefit from the provision of additional resources and guidance in future research. Although our study sheds light on differential patterns of self-collected specimen return, a better understanding of why some GBMSM may choose to fully, partially, or not engage in this approach is warranted. Home-based options to test for HIV, bacterial STIs, and PrEP drug levels provide certain unique advantages over clinic-based options including privacy, convenience, and autonomy and could benefit GBMSM who are reluctant to frequently visit clinical settings on account of anticipated stigma, long geographic distances, or transportation issues. Designing, evaluating, and implementing innovative approaches to stem the burden of HIV and bacterial STIs among GBMSM remains crucial, and specimen self-collection is a promising strategy to achieve the desired improvements in testing and adherence.
Footnotes
Acknowledgements
The authors would like to thank laboratory personnel at the Clinical Virology Research Laboratory at Emory University in Atlanta and the Hair Analytical Laboratory at the University of California San Francisco.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in the manuscript was funded by the National Institute of Allergy and Infectious Diseases of the National Institutes of Health (R21AI136657). The University of California San Francisco Hair Analytical Laboratory infrastructure was further supported by 2R01AI098472.