
Abstract
The aim of this study was to determine the association between lifetime anabolic-androgenic steroid (AAS) use and seven indicators of sexual health behaviors among a nationally representative sample of adolescent boys in the United States. Multiple modified Poisson regression analyses were conducted to determine the associations between any lifetime AAS use and seven indicators of sexual health behaviors among 2,095 sexually active adolescent boys from the 2019 National Youth Risk Behavior Survey. Sexually active boys who reported lifetime AAS use were at greater risk of having sexual intercourse before the age of 13 years (adjusted risk ratio [aRR] = 2.73, 95% confidence interval [CI] = [1.44, 5.17]), reporting ≥4 sexual partners in their lifetime (aRR = 1.96, 95% CI = [1.34, 2.89]) and in the past 3 months (aRR = 6.77, 95% CI = [3.19, 14.37]), having been tested for HIV in their lifetime (aRR = 2.49, 95% CI = [1.13, 4.73]), and having been tested for any sexually transmitted infection in the past 12 months (aRR = 3.14, 95% CI = [1.63, 6.03]). These findings align with prior research among adult men and have implications for public health and health care prevention efforts to reduce the use of AAS, as well as support the engagement in safe sexual health behaviors among adolescent boys.
Introduction
Adolescence is a significant developmental period where the exploration of health behaviors is common, including substance use and sexual behaviors (Sawyer et al., 2012). Research within the last 2 years has shown an increase in the lifetime use of non-prescribed (i.e., illicit) anabolic-androgenic steroids (AASs), with a recent low of 1.2% in 2017 to nearly 2.0% in 2020 (Johnston et al., 2021). Generally, AAS use is more common among boys than girls (Eisenberg et al., 2012; Johnston et al., 2021; Nagata et al., 2020), in part due to the sociocultural emphasis on the muscular and lean body ideal for boys and men (Cafri et al., 2005; Nagata et al., 2020; Pope et al., 2017). Similarly, many risky sexual health behaviors, such as having sex at a young age, having sex with a greater number of individual partners, and not using a condom during sex, all occur at higher prevalence among boys than girls (Kann et al., 2018).
Although prior research has reported associations between AAS use and a number of risky sexual health behaviors among young adult and adult men (Ganson et al., 2021; Goldman et al., 2019; Ip et al., 2016, 2017, 2019), few studies have explored this relationship among adolescent boys. One study reported an association between AAS use and unprotected sex via the mediators of depression symptoms and substance use (Blashill et al., 2014), while another study identified that AAS use was associated with engagement in condomless sex and using alcohol or drugs during sexual intercourse among sexual minority (i.e., non-heterosexual) boys (Blashill et al., 2015). These studies, while informative, are limited due to the age of the data, both of which include data from more than 10 years ago, the restricted subsample of participants in one study (i.e., sexual minority boys only), thus not allowing for inferences to the wider population of boys, and the lack of comprehensive measures of sexual health behaviors (i.e., investigated few indicators of sexual health behaviors such as only condomless sex and alcohol/drug use during sex).
The aim of this study was to determine the relationships between lifetime illicit AAS use and seven indicators of sexual health behaviors among a nationally representative sample of sexually active U.S. adolescent boys. Aligning with prior research among adults (Ganson et al., 2021; Goldman et al., 2019; Ip et al., 2016, 2017, 2019), it was hypothesized that sexually active adolescent boys who report AAS use in their lifetime will also report greater engagement in risky sexual health behaviors compared with non-AAS users.
Methods
Data from the 2019 National High School Youth Risk Behavior Survey (YRBS) were analyzed for this study. The YRBS is conducted bi-annually by the Centers for Disease Control and Prevention (CDC) to monitor health risk behaviors among adolescents. The YRBS utilizes a three-stage cluster sampling method to collect a nationally representative sample of U.S. high school students. The YRBS utilizes active and passive parental consent and is approved by the CDC’s Institutional Review Board (Underwood et al., 2020). This analysis was exempt from further ethics review given the data are publicly available and anonymous. This analysis was restricted to high school–age male participants who indicated they had sex within their lifetime, comprising a sample of 2,095 boys. Listwise deletion was used to account for further missing data given low levels of missing data among the analytic sample (Allison, 2002; Parent, 2013).
Dependent Variables
Seven indicators of sexual health behaviors were analyzed in this study: (1) Sexual intercourse before age 13 years (≥13 years and <13 years); (2) Number of lifetime sexual partners (≥4 and <4); (3) Number of sexual partners in the past 3 months (≥4 and <4); (4) Use of alcohol or drugs during sex (“yes” or “no”); (5) Condom use during last sexual intercourse (“yes” or “no”); (6) Tested for HIV, lifetime (“yes” or “no”); and (7) Tested for any sexually transmitted infection (STI) in the past 12 months (“yes” or “no”). Dichotomized coding for the sexual health dependent variables was done to align with prior research (Blashill et al., 2014; Ganson et al., 2021) and CDC cut-off points (Kann et al., 2018). In addition, several variables (e.g., number of lifetime sexual partners, number of sexual partners in the past 3 months) were rare (<10% of responses) on the extreme ends, and the intent of this analysis was to determine associations based on the presence or absence of a behavior.
Independent Variables
Lifetime AAS use was assessed using the question, “During your life, how many times have you taken steroid pills or shots without a doctor’s prescription?” Responses were dichotomized to 0 times and ≥1 times in accordance with prior research (Blashill et al., 2014; Ganson et al., 2021).
Statistical Analysis
Descriptive statistics were conducted among the overall sample and stratified by AAS use. Differences between lifetime AAS use groups were determined using the adjusted F, a variant of the second-order Rao–Scott adjusted χ2 statistic. Multiple modified Poisson regression analyses with robust error variance, allowing for coefficients to be interpreted as risk ratios (Zou, 2004), were conducted to determine the association between lifetime AAS use as the independent variable and each of the seven sexual health behaviors as the dependent variables, while adjusting for age, race/ethnicity, sexual orientation, body mass index percentile, any alcohol use in the past 30 days, any marijuana use in the past 30 days, any lifetime illicit drug use, and feeling sad or hopeless for two or more weeks in the past 12 months in accordance with prior research (Blashill et al., 2014, 2015; Ganson et al., 2021; Ip et al., 2016, 2017, 2019; Nagata et al., 2020). The modified Poisson regression was used given that odds ratios may overestimate effect sizes if used to approximate a risk ratio (Tamhane et al., 2016). All analyses utilized preconstructed sample weighting and were conducted using Stata 17.
Results
Among the sample of demographically diverse, sexually active adolescent boys, all seven indicators of risky sexual health behaviors were significantly more common among those who reported any lifetime AAS use versus those who did not (Table 1). In adjusted analyses (Table 2), lifetime AAS use was significantly associated with greater risk of having sexual intercourse before the age of 13 years (adjusted risk ratio [aRR] = 2.73, 95% [confidence interval] CI = [1.44, 5.17]), reporting ≥4 sexual partners in their lifetime (aRR = 1.96, 95% CI = [1.34, 2.89]) and in the past 3 months (aRR = 6.77, 95% CI = [3.19, 14.37]), having been tested for HIV in their lifetime (aRR = 2.49, 95% CI = [1.13, 4.73]), and having been tested for any STI in the past 12 months (aRR = 3.14, 95% CI = [1.63, 6.03]), while adjusting for demographic and confounding variables.
Characteristics of 2,095 Sexually Active Adolescent Boys From the 2019 Youth Risk Behavior Survey.
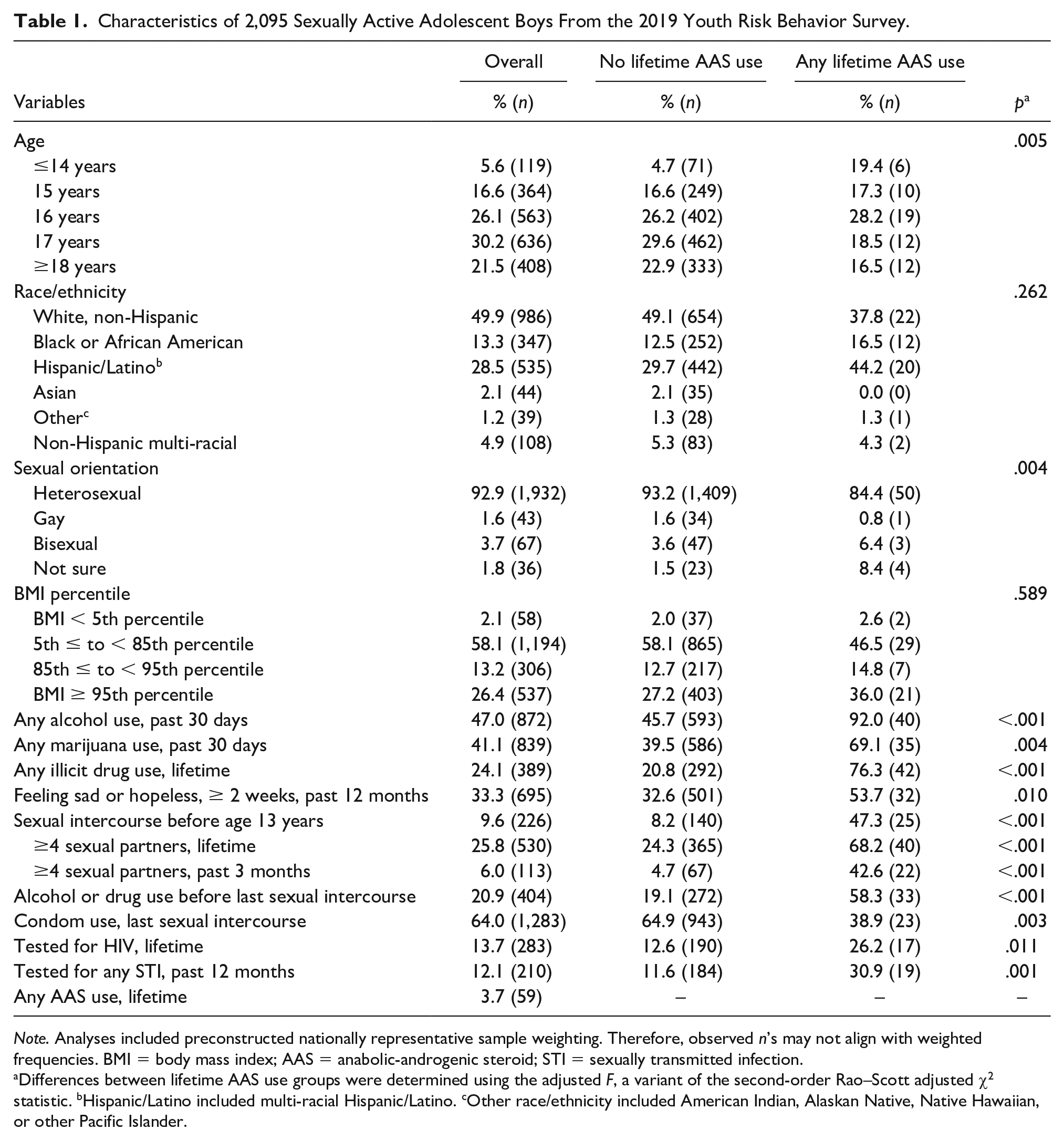
Note. Analyses included preconstructed nationally representative sample weighting. Therefore, observed n’s may not align with weighted frequencies. BMI = body mass index; AAS = anabolic-androgenic steroid; STI = sexually transmitted infection.
Differences between lifetime AAS use groups were determined using the adjusted F, a variant of the second-order Rao–Scott adjusted χ2 statistic. bHispanic/Latino included multi-racial Hispanic/Latino. cOther race/ethnicity included American Indian, Alaskan Native, Native Hawaiian, or other Pacific Islander.
Associations Between Any Lifetime Anabolic-Androgenic Steroid Use and Sexual Health Risk Behaviors.

Note. All analyses included preconstructed sample weights.
Adjusted for age, race/ethnicity, sexual orientation, body mass index percentile, alcohol use, marijuana use, illicit drug use, and feelings of sadness or hopelessness.
Discussion
In this large, nationally representative sample of sexually active high school boys, we found that those who reported illicit lifetime AAS use had significantly greater risk of engaging in several key indicators of sexual health risk behaviors. This includes nearly three times greater risk of first having sex at a young age and nearly seven times greater risk of reporting four or more sexual partners within the past 3 months. These findings are particularly salient as they are independent of several known confounding factors, including substance use and depression symptomatology. While not statistically significant in adjusted analysis, it should be noted that nearly 60% (n = 33) of sexually active boys who reported any lifetime AAS use also reported using alcohol or drugs prior to their last sexual encounter, while nearly 40% (n = 23) reported not using a condom during their last sexual encounter. These findings are cause for concern given that both may increase risk of contracting or spreading HIV and/or other STIs, and unintended pregnancy (Leftwich & Alves, 2017; Wangu & Burstein, 2017). Sexually active boys who reported any lifetime AAS use were more likely to also report being tested for HIV in their lifetime and STIs in the past 12 months. Such sexual health testing may indicate these individuals believed they were susceptible to contracting HIV or an STI, or were practicing responsible sexual health behaviors by knowing their current status (Carmine et al., 2014), despite overall low rates of lifetime HIV and STI testing among adolescents (Shannon & Klausner, 2018).
The findings from this study align with prior research that identified associations between AAS use and risky sexual health behaviors among adult men, including a greater number of sexual partners, multiple sex partners around the same time, and unprotected sex (Ganson et al., 2021; Ip et al., 2016, 2017, 2019). These findings may be explained by several factors. This includes the neurological effects of AAS use, including impaired executive functioning and emotion regulation abilities (Hauger et al., 2019, 2020). In addition, notions of hegemonic masculinity that overlap with muscularity (e.g., strength, dominance, confidence; Connell & Messerschmidt, 2005; Courtenay, 2000; Frederick et al., 2007; Luciano, 2007) may influence risk behaviors boys engage in to both display their adherence to masculine norms and achieve the muscular male body ideal. The findings from this study have important implications for social workers and public health and health care professionals. First, efforts to curtail the use of AAS among adolescent boys is warranted. Nearly 4% of this sample of sexually active boys reported use, which is double that of prior research among other national samples (Johnston et al., 2021). Health education programming in schools and sports teams, and awareness campaigns in gyms and via social media may be effective mechanism at reducing AAS use. Second, health education programming in schools promoting safe sexual health behaviors among adolescents is also warranted. Such efforts may curtail the engagement in sexual health risk behaviors. Third, health care professionals should assess for both AAS use and sexual health risk behaviors when caring for adolescent boys, particularly those who are sexually active, to provide proper guidance and intervention when appropriate.
Despite the important findings of this study, there are limitations to be noted. First, all items are based on self-report, which may increase the risk of reporting, recall, and social desirability bias. Second, this study uses cross-sectional data, precluding any causal inferences. In addition, the AAS use variable measures lifetime use, thus limiting the ability to identify at what age use occurred. Finally, despite adjusting for several known confounders, there is the potential for unmeasured confounders that may influence the relationships between the variables under study. Strengths of the study include the use of a large, diverse, and nationally representative sample of U.S. adolescent boys.
Conclusion
Lifetime use of AAS is associated with greater risk of several sexual health risk behaviors among sexually active adolescent boys, including first having sex at a young age and reporting a greater number of sexual partners. These findings warrant future research and intervention programming targeted at these behaviors to protect the health and well-being of adolescent boys.
Footnotes
Author Contributions
K.T.G.: Conceptualization; Data curation; Formal analysis; Methodology; Writing—original draft; Writing—review & editing. D.B.J., A. T., P. M. M., and J.M.N.: Conceptualization; Methodology; Writing—review & editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: J.M.N. is supported by the National Institutes of Health (K08HL159350) and the American Heart Association (CDA34760281). This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Ethical Approval
The Youth Risk Behavior Survey is approved by the CDC’s Institutional Review Board. This analysis was exempt from further ethics review given the data are publicly available and anonymous.
Consent
The Youth Risk Behavior Survey utilizes active and passive parental consent.