
Abstract
Additional characterization of patients using anabolic androgenic steroids (AAS) is needed to improve harm reduction and cessation resources for patients. Our group sought to expand upon the currently limited data regarding AAS use by performing a web-based survey assessing experiences of males using AAS. Participants included men over the age of 18 with history of AAS use within the past 5 years. Data were collected between August 2019 and April 2020. Primary outcome measures included age when starting AAS, dose of AAS, motivations for use, experiences with health-care professionals, and rate of successful cessation. The survey was accessed 3640 times, resulting in 2385 completed surveys meeting the inclusion criteria (68.93% participation rate).
Average participant age was 31.69 ± 10.09 years. Over half of respondents were from the United States (n = 1271, 53.3%). Motives to use AAS included improving appearance (n = 1959, 82.2%), strength gain (n = 1192, 50%), and self-esteem/body image issues (n = 712, 29.87%). Participants rated physicians poorly, regarding knowledge of AAS (4.08 ± 2.23). Most participants did not reveal AAS use to their health-care providers (n = 1338, 56.1%); of those that did, 55.30% (n = 579) reported feeling discriminated against for their use. Of 46.16% (n = 1101) attempting AAS cessation, 60.22% (n = 663) were unsuccessful. Challenges in the management of AAS use include early onset of use, supraphysiologic doses used, and frequently present body image disorders stress. Distrust of health-care providers, poor cessation rates, and lack of physician training further exacerbate this. These findings should serve to reinforce previous calls to action for further research on the treatment of AAS use disorder.
The widespread adoption of anabolic androgenic steroid (AAS) use has exacerbated an emerging worldwide public health epidemic. The true lifetime prevalence of AAS use is difficult to establish, but conservative estimates range from 1% to 5% worldwide and are higher in the United States (Anawalt, 2019). Increasing social acceptance of use, ease of acquisition through the internet (Fink et al., 2019), and a growing preoccupation with male appearance fueled by social media (Pope et al., 2017) are believed to be contributing factors. These drugs have multisystem effects, and often severe withdrawal symptoms can impede cessation. Men using AAS often hesitate to seek out physicians for help, viewing them as both unknowledgeable on AAS and disrespectful to those taking these substances (Pope et al., 2004; Zahnow et al., 2017). Instead, these patients default to friends, online forums, and self-proclaimed coaches or gurus for advice that is often inaccurate and dangerous (de Ronde & Smit, 2020; Fink et al., 2019). A 2019 review highlights the lack of data, guidelines, and clinical preparedness to assist these patients (Goldman et al.).
The lack of larger comprehensive studies makes the reliability of the AAS using patient profile problematic. A more complete characterization of this population is needed to design patient-centered medical protocols for harm minimization and successful cessation. Thus, we sought to assess a broad number of characteristics of AAS use via a large-scale online survey study, designed to test the reliability of prior findings while also exploring questions suggested by these and the authors’ clinical experiences.
Anabolic Androgenic Steroids: The State ofthe Art
The primary classes of AAS consist of testosterone esters, 19-nortestosterone derivatives, and dihydrotestosterone (DHT) derivatives (Kicman, 2008; Llewellyn, 2017). Direct hepatoxicity is only seen with 17-alpha alkylated oral AAS (Niedfeldt, 2018). Commonly used accessory performance enhancing drugs (PEDs) include aromatase inhibitors (AIs), selective estrogen receptor modulators (SERMs), human chorionic gonadotropin (hCG), thyroid hormone, insulin, and human growth hormone (hGH), among others (de Ronde & Smit, 2020). AIs and SERMs (particularly tamoxifen) are used to mitigate the estrogenic side effects of supraphysiologic androgen levels, while hCG is used to maintain testicular volume (Anawalt, 2019). Many men using AAS utilize the SERM clomiphene and/or hCG while temporarily stopping AAS in an attempt to normalize the hypothalamic-pituitary-testicular (HPT) axis (Anawalt, 2019; de Ronde & Smit, 2020; Smit & de Ronde, 2018; Smit et al., 2020), a practice commonly known as “post-cycle therapy” or “PCT.”
While long-term prospective harm data are lacking, strong evidence exists for the development of accelerated atherosclerosis, left ventricular hypertrophy, arrhythmias, hypertension, and HDL suppression (Achar et al., 2010; Alizade et al., 2016; Baggish et al., 2017; Santora et al., 2006; Thiblin et al., 2015). Polycythemia, infertility, tendon rupture of the upper extremity, and behavioral disorders are commonly associated with AAS use (Coviello et al., 2008; Hauger et al., 2019; Kanayama, DeLuca, et al., 2015; Rahnema et al., 2014; Tatem et al., 2019; Thiblin et al., 1999). AAS withdrawal syndrome has also been reported and is due to the sudden decline in androgen levels with resultant anabolic steroid-induced hypogonadism (ASIH) and neuropsychiatric effects (Bertozzi et al., 2019; Bhasin et al., 2018; Pope et al., 2014). Prolonged hypogonadism after AAS cessation has been well described, due to direct testicular toxicity from chronic exposure to very high dose androgen levels (Chainy et al., 1997; Kanayama, Hudson, et al., 2015; Rasmussen et al., 2016).
Approaches to transitioning men from AAS have been proposed (Anawalt, 2019; Rahnema et al., 2014), such as supervised tapering of testosterone dosage or the use of hCG or clomiphene citrate. However, no randomized control trials or prospective data exist to support these approaches. The net result is a growing population of patients using AAS with limited to no medical resources to assist with attempted cessation.
Methods
An anonymous web-based survey consisting of 160 items, intended to take 20 min to complete, was designed using REDCap electronic data capture tools (Harris et al., 2009, 2019). Questions were designed based on the authors’ clinical experience in addition to existing evidence and consisted of primarily multiple-choice questions and numeric ratings. Several questions included the option to select multiple applicable responses. All related materials and methods were reviewed by the Wake Forest University IRB and approved (IRB00057901). The survey was advertised on nine AAS use web forums, and on one of the author’s YouTube channel that focuses on patient education for AAS side effects and support for cessation (Thomas O’Connor). Upon clicking the survey link, participants were directed to a consent page where they were given the option to voluntarily participate, noting that they should only participate if they were comfortable disclosing details regarding AAS use. The potential to experience feelings of distress while discussing past experiences of abuse was noted. Inclusion criteria were male gender, over the age of 18 years old, and having used AAS in the past 5 years. Those who did not meet these criteria were re-directed to a site informing them they were ineligible to participate. Survey responses were collected from August 2019 to April 2020. Upon completion of data collection, the results were further analyzed using REDCap and Microsoft Excel. In addition to analyzing the responses of all meeting the inclusion criteria, further subgroup analysis was performed on those from the United States (USA), countries other than the United States (World), those 18–34 years old (Under 35), and those age 35 or older (Over 35).
Statistical Analysis
For questions requiring a rated response of 1–10, descriptive statistics were utilized to obtain mean values and 95% confidence intervals for each subgroup. A single-variable ANOVA test was used to compare multiple groups with continuous variables for significance. Fisher’s exact test and the χ2 test were used to compare binary data between two groups and groups larger than two, respectively. For all statistical testing, a p value of <.05 was considered significant.
Results
Demographics, Motivations, and Acquisition
The survey was accessed 3640 times, resulting in 2385 completed surveys meeting the inclusion criteria (68.93% participation rate). The average man using AAS was 31.69 ± 10.09 years old (Table 1). Men aged 22–30 represented 42.85% (n = 1022) of respondents. The most common ethnicity was Caucasian (n = 1991, 83.52%). Most respondents were from the United States (n = 1271, 53.3%). Other regions represented were Europe (n = 536, 22.47%), Canada (n = 198, 8.30%), and Australia/New Zealand (n = 134, 5.62%; Table 2).
Demographics and Motivations of Men Using AAS.
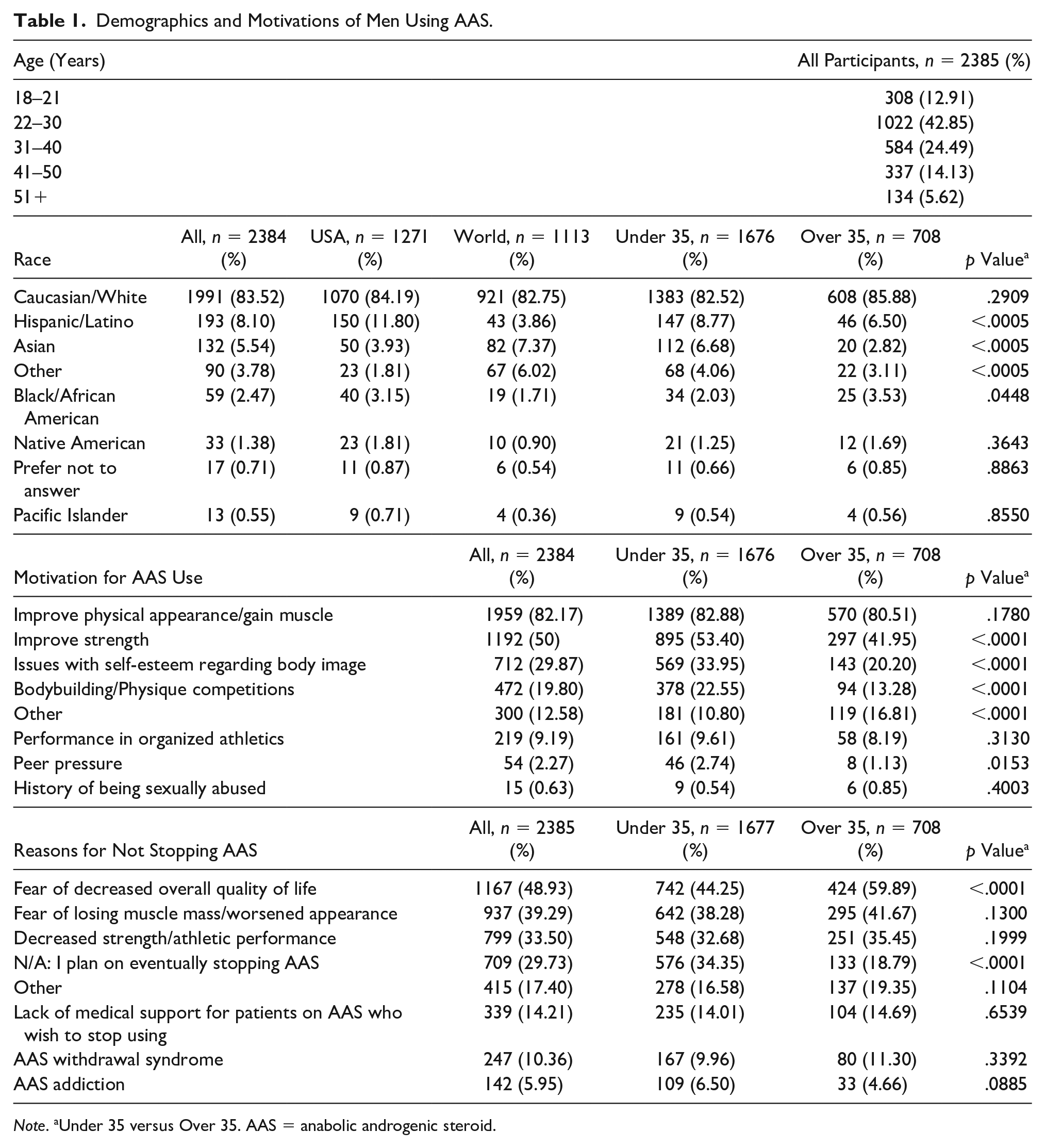
Note. aUnder 35 versus Over 35. AAS = anabolic androgenic steroid.
Countries of Respondents.

Note. aUnder 35 versus Over 35. AAS = anabolic androgenic steroid.
The primary motive in using AAS was improving appearance (n = 1959, 82.2%) and strength gain (n = 1192, 50%; Table 1). Men over 35 were less likely to use AAS for strength gain, self-esteem/body image issues, or bodybuilding/physique competitions than men under 35 (41.9% vs. 20.2%), compared to those under 35 (53.4% vs. 33.9%, respectively). Self-esteem or body image issues were strongly reported (n = 712, 29.87%) as motivation for use. Less than 10% of respondents reported using AAS for competitive athletics. These motivations were consistent when comparing sub-cohorts across regions. The most commonly reported reasons for not discontinuing AAS use were concerns over decreased quality of life (n = 1167, 48.93%), muscle loss/worsened appearance (n = 937, 39.3%), and decreased strength/athletic performance (n = 799, 33.5%). Subjects over 35 years old were significantly less likely to consider stopping AAS use than those under 35 years old (18.8% and 34.4%, respectively).
The primary source of AAS was the internet (n = 1465, 61.41%). Of the 16.82% (n = 401) who reported physicians as a source of AAS, 20.95% reported this as their only source. Moreover, 79.05% (n = 317) of respondents who listed physicians as a source of AAS reported also obtaining AAS from additional sources.
Attempted AAS Cessation
Of 46.16% (n = 1101) of participants who reported a prior attempt to stop AAS use, 39.78% (n = 438) reported success (Figure 1). Of the 60.22% (n = 663) who were unsuccessful, 297 (44.80%) had previously stopped for over 1 year, and 138 (20.81%) had previously stopped for over 3 years.
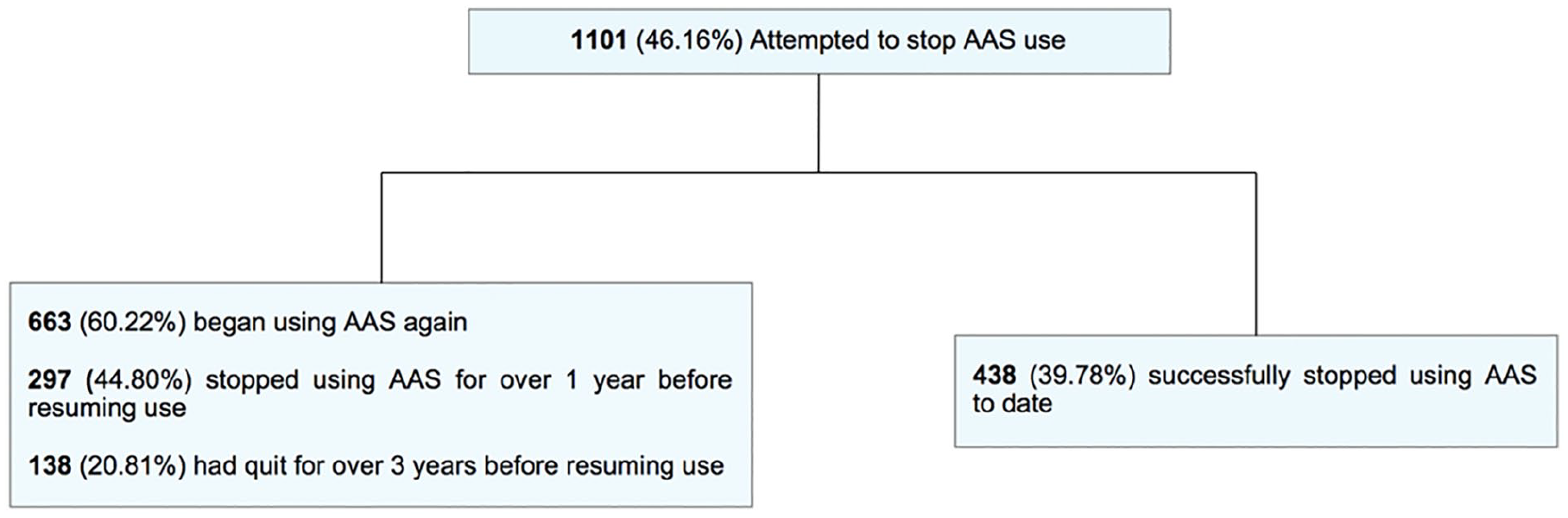
Attempted AAS cessation. AAS = anabolic androgenic steroid.
Beliefs Regarding AAS/PED safety
A majority (n = 1782, 74.7%) of respondents reported they believe AAS/PEDs can be used safely in the long term. This was consistent across regions and age groups. Further, 86.7% (n = 2073) of respondents reported they would cease AAS use if they suffered a serious health problem because of AAS use; this was consistent across analyzed sub-cohorts.
Attitudes and Experiences With Medical Professionals
Physicians were rated the lowest (4.08 ± 2.23) regarding knowledge and expertise of AAS use. Coaches/gurus (6.52 ± 2.38), bodybuilding websites (6.44 ± 2.03), and persons currently using AAS (5.92 ± 2.31) received the most favorable ratings (Figure 2). Most respondents (n = 1338, 56.1%) had never revealed their AAS use to a medical professional (Figure 3). Of those not disclosing AAS use to health-care providers, frequently reported reasons for this included concern for judgment from physicians/others who access medical records (n = 853, 63.75%), lack of confidence in their physician’s knowledge of AAS use (n = 812, 60.69%), and concern for legal repercussions (n = 611, 45.67%). Of the participants who had reported AAS use to their health-care provider (n = 1047, 43.90%), 55.30% (n = 579) reported feeling discriminated against by a physician for AAS use. The most frequently ordered diagnostic tests ordered for those who disclosed AAS use were basic metabolic panels (BMP) and/or complete blood count (CBC; n = 944, 90.16%), testosterone levels (n = 822, 78.51%), liver function tests (LFTs) (n = 726, 69.34%), thyroid stimulating hormone (TSH) (n = 522, 49.86%), and gonadotropins (n = 469, 44.79%; Table 3). Compared to those under age 35, those over age 35 were more likely to undergo prostate specific antigen (PSA) testing (52.7% vs. 19.6%), coronary artery calcium scan (11.1% vs. 4.9%), transthoracic echocardiogram (18.5% vs. 8.8%), and electrocardiogram (36.2% vs. 21.0%).

Rated knowledge of AAS use of various groups. AAS = anabolic androgenic steroid.

Reporting of AAS use to medical professionals. AAS = anabolic androgenic steroid.
Diagnostic Workup for Men Disclosing AAS Use to Medical Providers.

Note. aover 35 vs under 35. AAS = anabolic androgenic steroid, CBC = complete blood count, BMP = basic metabolic panel, TSH = thyroid stimulating hormone, LH = luteinizing hormone, FSH = follicle stimulating hormone, PSA = prostate specific antigen, ECG = electrocardiogram, TTE = transthoracic echocardiogram.
Patterns of AAS/PED Use
The most frequently reported age range for starting AAS was 22–30 years (n = 1001, 41.97%), followed by 19–21 years (n = 691, 28.97%); 7.42% (n = 177) reported beginning AAS prior to age 18. The most frequently utilized androgens were testosterone enanthate (n = 1922, 80.62%), testosterone cypionate (n = 1217, 51.05%), metandione (n = 1213, 50.88%), trenbolone (n = 1199, 50.29%), oxandrolone (n = 1110, 46.56%), and nandrolone decanoate (n = 1107, 46.43%). The most common base dose of weekly testosterone was 500–1000 mg (n = 1132, 47.46%). The most common number of AAS compounds utilized per cycle was two (n = 1126, 47.21%) or three (n = 727, 30.48%). Continuous AAS use without PCT was reported at 47.32% (n = 1128), while an “on-and-off” cycle approach with PCT was reported by 45.93% (n = 1095). Please see Table 4 for details.
Patterns of AAS/PED Use.
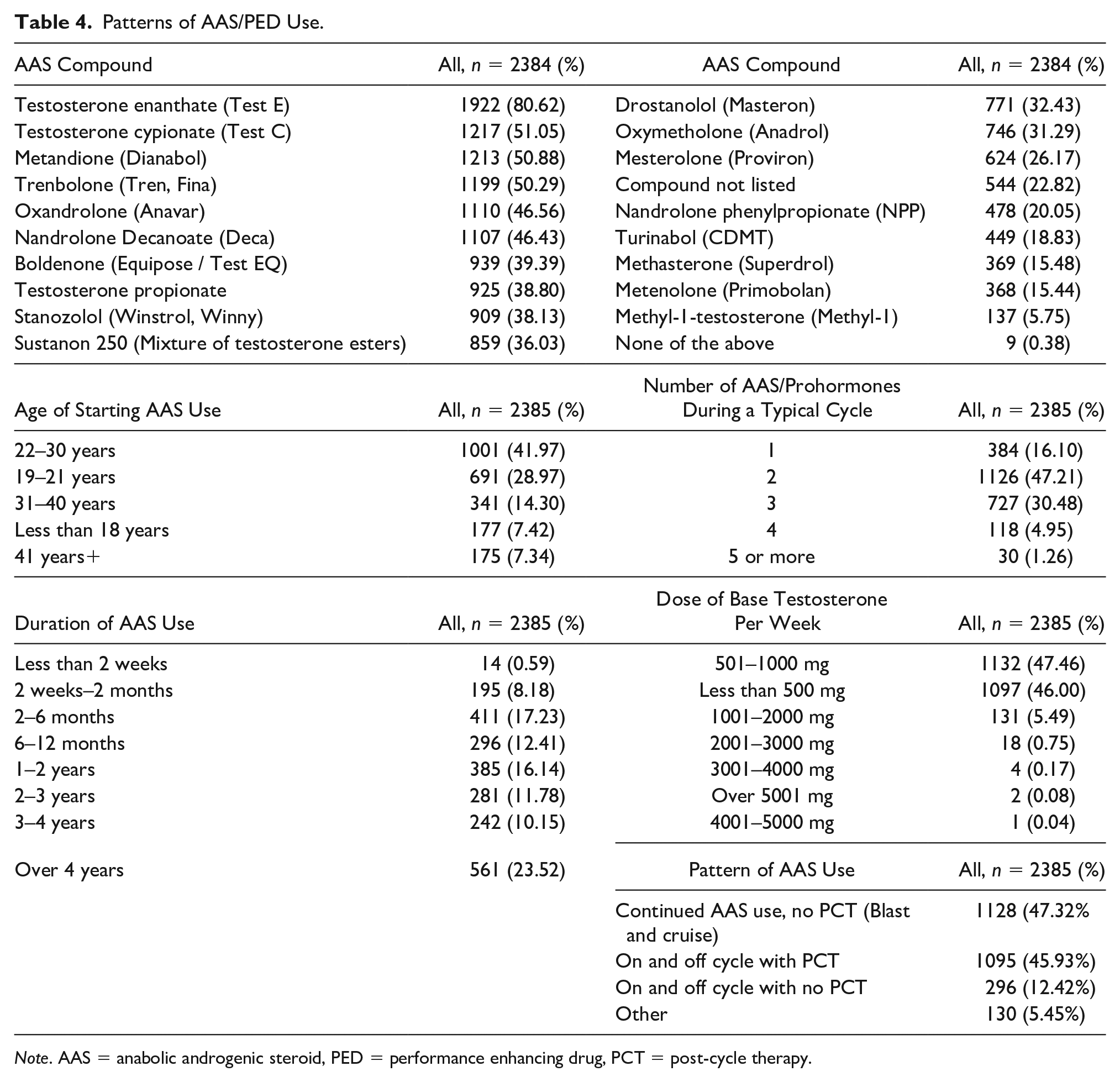
Note. AAS = anabolic androgenic steroid, PED = performance enhancing drug, PCT = post-cycle therapy.
Accessory Compounds/PED Use
While on an AAS cycle, commonly used accessory compounds were anastrozole (n = 1135, 47.61%), tamoxifen (n = 742, 31.12%), exemestane (n = 719, 30.16%), and hCG (n = 682, 28.61%). While off AAS, tamoxifen (n = 959, 40.23%), clomiphene citrate (n = 754, 31.63%), and hCG (n = 610, 25.59%) were most commonly used, and 32.84% (n = 783) reported using no additional compounds when off AAS (Table 5).
Accessory PED Use.

Note. PED = performance enhancing drug.
Of those reporting an “on/off cycle w/ PCT” approach to using AAS (n = 1095), 52.51% (n = 575) reported using both tamoxifen and clomiphene simultaneously while off AAS, while 25.02% (n = 274) reported using tamoxifen, clomiphene, and hCG simultaneously between cycles.
Additional Illicit Substance Use
While 42.49% (n = 1013) reported no such use, additional illicit substance use was reported by the majority who ranked marijuana (n = 973, 40.81%), excess alcohol (n = 697, 29.24%), and cocaine (n = 380, 15.94%) as the most commonly used. Men over age 35 were less likely to use illicit substances (56.9%) compared to men under 35 (36.4%). In the under 35 group, use of marijuana (47.2% vs. 25.7%), alcohol (33.2% vs. 19.9%), cocaine (19.2% vs. 8.3%), MDMA (14.6% vs. 4.5%), psychedelics (13.9% vs. 4.2%), and nonprescription amphetamines (12.3% vs. 4.2%) was significantly more common (Table 6).
Additional Illicit Substance Use.

Note. aUnder 35 versus Over 35.
Reported Side Effects of AAS Use
As shown in Table 7, testicular atrophy (n = 1501, 62.94%), acne (n = 1320, 55.35%), hypersexuality (n = 1209, 50.69%), hypertension (n = 1036, 43.44%), mood changes (n = 1017, 42.64%), erectile dysfunction (n = 786, 32.96%), dyslipidemia (n = 667, 27.97%), and gynecomastia (n = 622, 26.08%) were most commonly reported. Dyslipidemia (32.91% vs. 25.88%), hair loss (27.12% vs. 20.69%), tendon rupture (9.89% vs. 6.92%), left ventricular hypertrophy (6.64% vs. 2.92%), infertility (9.82% vs. 6.92%), injection site abscess (12.43% vs. 8.05%), and polycythemia (20.9% vs. 9.0%) were significantly more common in respondents over 35 years old.
Reported Side Effects of AAS Use.

Note. aUnder 35 versus Over 35. AAS = anabolic androgenic steroid, MPB = male pattern baldness, LVH = left ventricular hypertrophy, CKD = chronic kidney disease, CHF = congestive heart failure, MI = myocardial infarction, DVT = deep vein thrombosis, PE = pulmonary embolism, CAD = coronary artery disease.
Discussion
To our knowledge, this is the largest published quantitative survey of AAS use to date in the medical literature. Cohen et al. (2007) published a survey of 1955 men using AAS in the United States in 2007, while other studies such as Parkinson and Evans (2006) and Rowe et al. (2017) surveyed 496 and 605 men using AAS, respectively. The profile of males using AAS that emerged from our data resembled that presented in earlier studies, suggesting reliability of our data. Our findings expanded on this populations’ experiences with health care and attempted cessation.
We noted that AAS use often begins at a young age with markedly supraphysiologic testosterone doses of 500–1000 mg per week, which is five to 10 times of that used for treatment of male hypogonadism. Even more concerning is that 7.42% of men reported AAS use prior to age 18, indicating a significant need for improved AAS education and awareness directed toward adolescents. The prevalence of body image disorders serving as a motivation to use AAS in our data (29.5%) supports the multidisciplinary challenges noted in prior studies (de Ronde & Smit, 2020; Goldman et al., 2019; Pope et al., 2017). The combination of easily accessed AAS compounds via the internet, early onset of use with high-dose androgens, and prevalence of body image disorders has created a greater need than ever for medical resources for these patients.
Testosterone esters, nandrolone compounds, and oral alkylated AAS were the most used androgens, consistent with prior surveys and reported steroid cycles (Cohen et al., 2007; Steroids: What Pro Bodybuilders Are Really Using, 2015). Utilization of accessory PED compounds varied significantly, as expected, with whether respondents were “on” or “off” cycle. Over half of the men utilizing an “on-and-off-cycle” approach with PCT reported using both tamoxifen and clomiphene simultaneously, consistent with a popular regimen propagated on forums and underground steroid guides (Llewellyn, 2017). Discussing individual experiences with these compounds may provide valuable information for the clinician when determining an optimal strategy to treat AAS withdrawal symptoms associated with attempted cessation. For example, a man who reports prior success cycling off AAS by utilizing SERMs may be willing to try medically supervised treatment with such compounds.
Over 94% of respondents reported side effects from their use, stressing the importance of providing medical care for this population. Congruent with prior studies (Dennington et al., 2008; Grogan et al., 2006; Maycock & Howat, 2005; Pope et al., 2004), this population generally found medical professionals unknowledgeable regarding AAS and indicated fear of judgment or repercussions as a barrier to disclosing their use. These concerns are valid, as most men in our study who disclosed AAS use to their physician reported feeling discriminated against after doing so. Furthermore, the reported diagnostic workup of men disclosing AAS use to their health-care providers appeared inconsistent and at times inadequate. Coronary artery calcium (CAC) scoring was performed in only 11.1% of men over 35, and 4.9% in men under 35. Yet, a prior study of bodybuilders using AAS reported that 50% had CAC scores much higher than expected for their age (Santora et al., 2006). In our study, transthoracic echocardiograms were performed in 18.5% men over 35 and in 8.8% of younger patients. Given the increased frequency of left ventricular hypertrophy (LVH), hypertension, and atherosclerosis seen with AAS use (Alizade et al., 2016; Baggish et al., 2017; Thiblin et al., 2015), our data suggest that TTEs are likely underutilized in this population. The lack of additional indicated testing for this population supported a prior study, concluding that physicians do not have adequate knowledge of AAS (Hill & Waring, 2019).
Many patients reporting physicians as an AAS source also reported obtaining additional illicit AAS compounds in addition to prescribed therapy. In a cohort of over 6000 men with hypogonadism, it was identified that 20.9% had a history of prior AAS use (Coward et al., 2013). This potential underscore the need for clinicians to have an open and nonjudgmental discussion with patients before prescribing testosterone therapy, especially if recent or concurrent AAS use is suspected. “Physician source” may also include prescriptions from “men’s health centers” and “integrative” or “anti-aging” centers, which commonly prescribe compounds such as anabolic steroids, growth hormone, and porcine thyroid hormone in an inappropriate manner (Irwig et al., 2020).
While most respondents reported they felt AAS could be safely taken in the long term, a greater majority reported they would stop AAS use if they experienced a serious health problem. This suggests many men using AAS care about their health, but do not believe the risk of serious side effects is significant enough to consider cessation. Implementing public education regarding AAS use and ensuring easier access to appropriate health care for this population could help improve upon this.
Most men using AAS reported difficulty with prolonged cessation. While half of respondents attempted to quit, over 60% returned to using AAS. Recidivism was common even after prolonged cessation, as 44.8% of those who had ceased AAS use for over a year and 20.8% of those not using for over 3 years returned to AAS use. This reflects previous reports that nonmedically addressed AAS withdrawal symptoms present challenges to attempted cessation (Kanayama, Hudson, et al., 2015; O’Connor & Hoekstra, 2018; Rahnema et al., 2014).
The disconnect that exists between patients struggling with cessation and medical professionals inadequately prepared to care for these men continues to broaden as AAS use becomes more prevalent. Urgent efforts on behalf of the medical community are needed. Initiatives directed toward assisting patients with cessation and offering access to high yield screen tests (such as lipid profile, BMP, CBC, and cardiac screening) for harm minimization should take priority. Additional research regarding the management of AAS withdrawal symptoms will be paramount in decreasing high rates of unsuccessful cessation.
Conclusions
Our updated data on attitudes and behavior of men using AAS should serve to reinforce previous calls to action for further research on the treatment of AAS use disorder. Particularly concerning are the young age at which use begins, the extreme supraphysiologic doses utilized, distrust of the health-care professionals, and lack of harm-minimization strategies. Poor rates of sustained AAS cessation are accompanied by the absence of medical resources to assist patients in need. Randomized control trials examining pharmacologic and behavioral approaches to AAS withdrawal and HPT axis recovery would be of immense clinical benefit. Our findings suggest the broad distrust of health-care providers will make recruitment for such studies increasingly difficult. Therefore, as a first step, medical education should emphasize the importance of an informed, nonjudgmental, and harm-mitigation approach to these patients. A multidisciplinary approach that includes medical professionals, addiction support groups, and behavioral health specialists is essential to support successful harm reduction and cessation of AAS use.
Limitations
The many uncensored online AAS forums have been an underutilized setting for research (Brennan et al., 2017). However, our study may have a sampling bias, in that men using AAS who do not frequently visit these forums and YouTube channel, or those without internet access, would have been unable to participate. While responses were anonymous, the illegal nature of AAS may have discouraged some respondents from answering truthfully. Due to the demographics of our participants, results are most applicable to Caucasian men between 18 and 30 years in the United States. The exclusion of men who had not used in the past 5 years limits the ability to assess long-term cessation rates.
Footnotes
Acknowledgements
Alex K. Bonnecaze participated in study design, survey instrument design, recruitment design, data analysis, and manuscript preparation. Thomas O’Connor participated in study design, survey instrument design, recruit design, and manuscript preparation. Joseph A. Aloi participated in study design and manuscript preparation.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Alex K Bonnecaze and Joseph A Aloi have no disclosures or COI to disclose. Thomas O’ Connor owns and operates an internal medicine private practice based out of Essex, CT, and has written a book on the health consequences of androgen misuse.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.